Effects of Photobiomodulation Using Low-Level Laser Therapy on Alveolar Bone Repair


 , and
, and 
Abstract
:1. Introduction
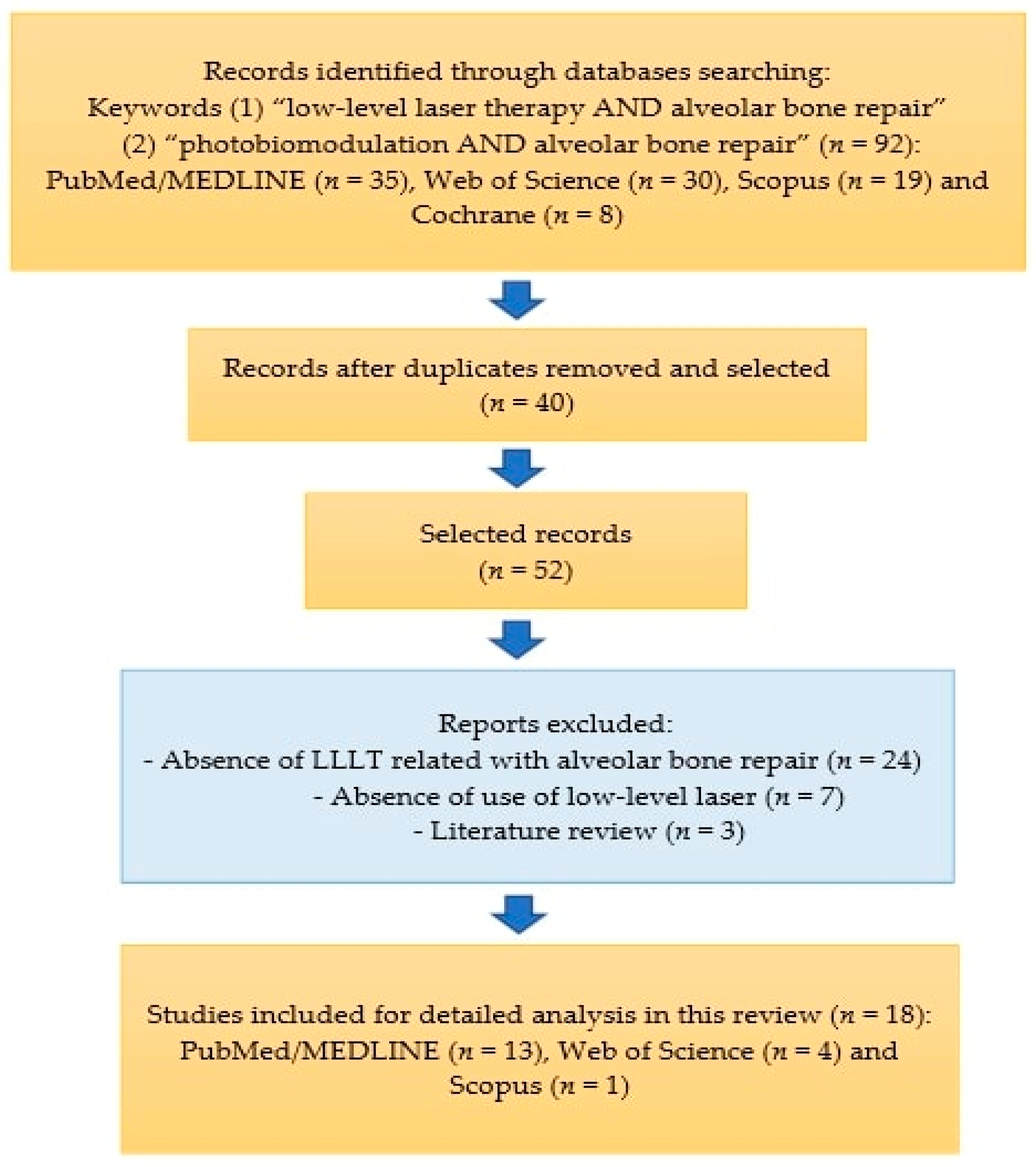
2. Materials and Methods
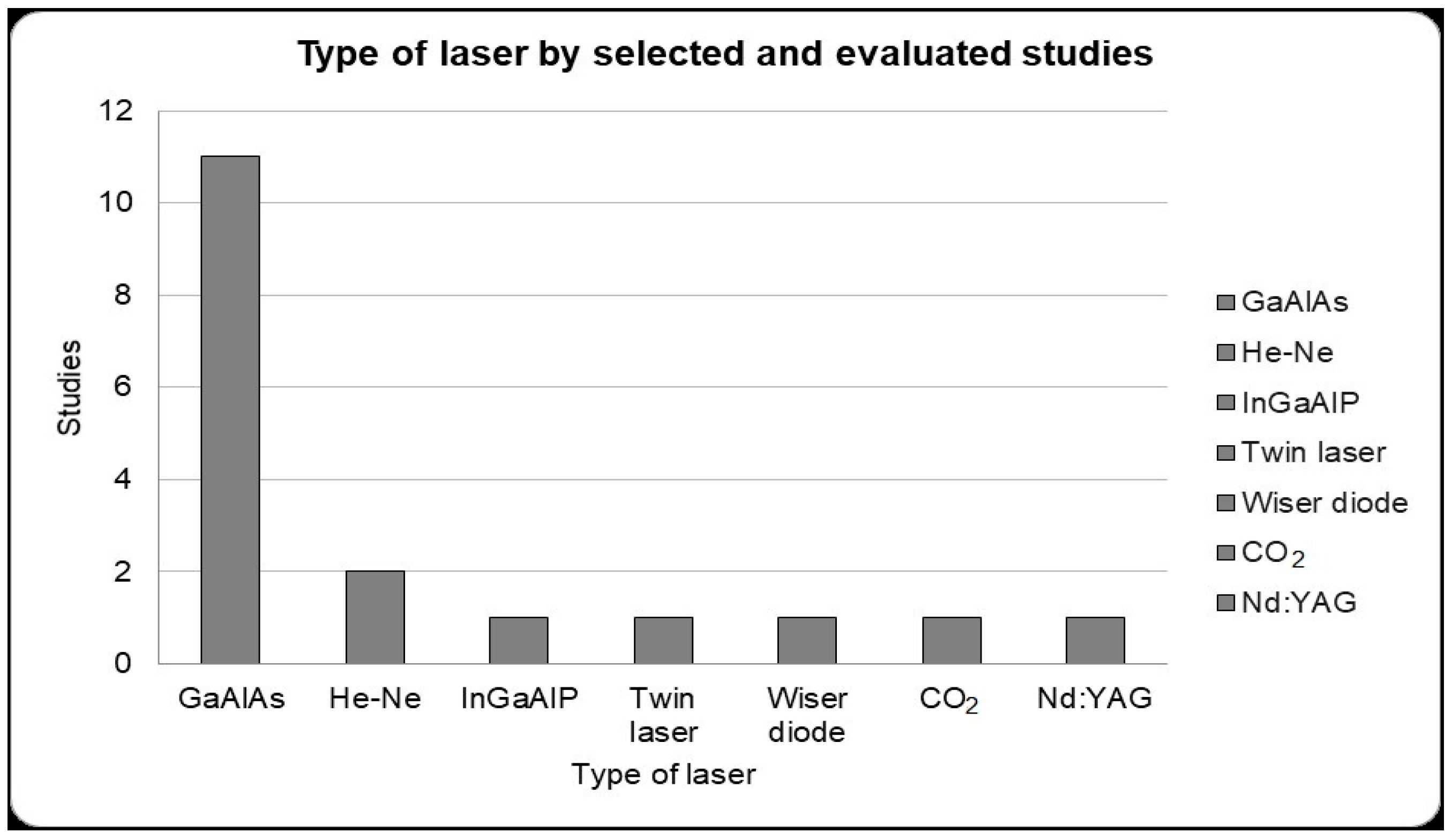
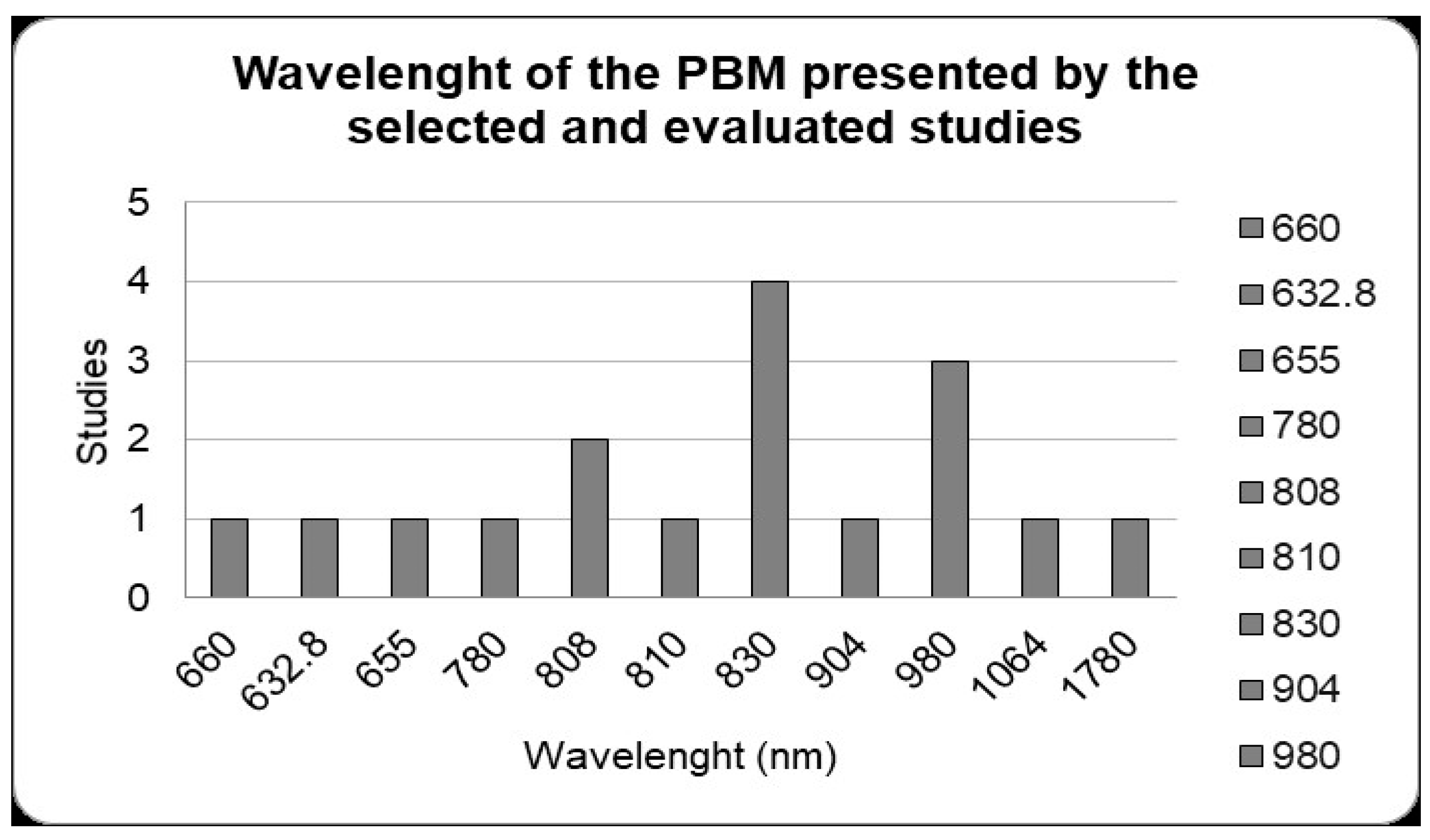
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tatullo, M.; Gentile, S.; Paduano, F.; Santacroce, L.; Marrelli, M. Crosstalk between oral and general health status in e-smokers. Medicine 2016, 95, e5589. [Google Scholar] [CrossRef] [PubMed]
- Penoni, D.C.; Leão, A.T.T.; Fernandes, T.M.; Torres, S.R. Possible links between osteoporosis and periodontal disease. Rev. Bras. Reumatol. (Engl. Ed.) 2017, 57, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Inchingolo, A.M.; Dipalma, G. Non-Hodgkin lymphoma affecting the tongue: Unusual intra-oral location. Head Neck Oncol. 2011, 3, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawinska, M.; Kondrat, A.; Jamiolkowski, J.; Paszynska, E. Dental Status and Oral Health Behaviors of Selected 45–74-Year-Old Men from Northeastern Poland. Int. J. Environ. Res. Public Health 2023, 20, 6005. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, M.; Anliker, N.; Sabatini, G.P.; De Paula, M.S.; Weber, A.R.; Molinero-mourelle, P. Assessment and Improvement of Masticatory Performance in Frail Older People: A Narrative Review. J. Clin. Med. 2023, 12, 3760. [Google Scholar] [CrossRef] [PubMed]
- Kalu, D.N. The ovariectomized rat model of postmenopa bone loss. Bone Miner. 1991, 15, 175–192. [Google Scholar] [CrossRef]
- Daigo, Y.; Daigo, E.; Hasegawa, A.; Fukuoka, H.; Ishikawa, M.; Takahashi, K. Utility of High-Intensity Laser Therapy Combined with Photobiomodulation Therapy for Socket Preservation after Tooth Extraction. Photobiomodulation Photomed. Laser Surg. 2020, 38, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Kawasaki, K.; Shimizu, N. Effects of Low-Energy Laser Irradiation on Bone Remodeling during Experimental Tooth Movement in Rats. Lasers Surg. Med. Off. J. Am. Soc. Laser Med. Surg. 2000, 26, 282–291. [Google Scholar] [CrossRef]
- Vieira, A.E.; Repeke, C.E.; De Barros Ferreira, S.; Colavite, P.M.; Biguetti, C.C.; Oliveira, R.C.; Assis, G.F.; Taga, R.; Trombone, A.P.F.; Garlet, G.P. Intramembranous bone healing process subsequent to tooth extraction in mice: Micro-computed tomography, histomorphometric and molecular characterization. PLoS ONE 2015, 10, e0128021. [Google Scholar] [CrossRef] [Green Version]
- Salhotra, A.; Shah, H.N.; Levi, B.; Longaker, M.T. Mechanisms of bone development and repair. Nat. Rev. Mol. Cell Biol. 2020, 21, 696–711. [Google Scholar] [CrossRef]
- Rosero, K.A.V.; Sampaio, R.M.F.; Deboni, M.C.Z.; Corrêa, L.; Marques, M.M.; Ferraz, E.P.; da Graça Naclério-Homem, M. Photobiomodulation as an adjunctive therapy for alveolar socket preservation: A preliminary study in humans. Lasers Med. Sci. 2020, 35, 1711–1720. [Google Scholar] [CrossRef]
- Horowitz, R.; Holtzclaw, D.; Rosen, P.S. A review on alveolar ridge preservation following tooth extraction. J. Evid. Based. Dent. Pract. 2012, 12, 149–160. [Google Scholar] [CrossRef]
- Stumbras, A.; Kuliesius, P.; Januzis, G.; Juodzbalys, G. Alveolar Ridge Preservation after Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet Concentrates: A Systematic Review. J. Oral Maxillofac. Res. 2019, 10, e2. [Google Scholar] [CrossRef]
- Pan, J.; Xu, Q.; Hou, J.; Wu, Y.; Liu, Y.; Li, R.; Pan, Y.; Zhang, D. Effect of platelet-rich fibrin on alveolar ridge preservation: A systematic review. J. Am. Dent. Assoc. 2019, 150, 766–778. [Google Scholar] [CrossRef]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: A review. Biomater. Res. 2017, 21, 9. [Google Scholar] [CrossRef] [Green Version]
- Sun, T.; Liu, M.; Yao, S.; Ji, Y.; Xiong, Z.; Tang, K.; Chen, K.; Yang, H.; Guo, X. Biomimetic composite scaffold containing small intestinal submucosa and mesoporous bioactive glass exhibits high osteogenic and angiogenic capacity. Tissue Eng.-Part A 2018, 24, 1044–1056. [Google Scholar] [CrossRef]
- Reis, C.H.B.; Buchaim, D.V.; Ortiz, A.d.C.; Fideles, S.O.M.; Dias, J.A.; Miglino, M.A.; Teixeira, D.d.B.; Pereira, E.d.S.B.M.; da Cunha, M.R.; Buchaim, R.L. Application of Fibrin Associated with Photobiomodulation as a Promising Strategy to Improve Regeneration in Tissue Engineering: A Systematic Review. Polymers 2022, 14, 2022. [Google Scholar] [CrossRef]
- Buchaim, R.L.; Goissis, G.; Andreo, J.C.; Roque, D.D.; Roque, J.S.; Buchaim, D.V.; Rodrigues, A.d.C. Biocompatibility of anionic collagen matrices and its influence on the orientation of cellular growth. Braz. Dent. Sci. 2007, 10, 12–20. [Google Scholar] [CrossRef]
- Pires Oliveira, D.A.A.; De Oliveira, R.F.; Zangaro, R.A.; Soares, C.P. Evaluation of low-level laser therapy of osteoblastic cells. Photomed. Laser Surg. 2008, 26, 401–404. [Google Scholar] [CrossRef]
- Razzaghi, M.R.; Ghazimoradi, M.H.; Afzali, S.; Kamani, E.; Mohajerani, E.; Shirkavand, A.; Farivar, S. Effect of a Low-Level Laser on Liposomal Doxorubicin Efficacy in a Melanoma Cell Line. J. Lasers Med. Sci. 2021, 12, e28. [Google Scholar] [CrossRef]
- Pogrel, M.A.; Chen, J.W.; Zhang, K. Effects of Low-Energy Gallium-Aluminum-Arsenide Laser Irradiation on Cultured Fibroblasts and Keratinocytes. Lasers Surg. Med. 1997, 20, 426–432. [Google Scholar] [CrossRef]
- Fiório, F.B.; Albertini, R.; Leal-Junior, E.C.P.; De Carvalho, P.D.T.C. Effect of low-level laser therapy on types i and III collagen and inflammatory cells in rats with induced third-degree burns. Lasers Med. Sci. 2014, 29, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Andrade, F.D.S.D.S.D.; Clark, R.M.D.O.; Ferreira, M.L. Efeitos da laserterapia de baixa potência na cicatrização de feridas cutâneas. Rev. Col. Bras. Cir. 2014, 41, 129–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatefi, K.; Hatefi, S.; Alizargar, J.; Abou-El-Hossein, K. Design of laser-assisted automatic continuous distraction osteogenesis device for oral and maxillofacial reconstruction applications. Majlesi J. Electr. Eng. 2019, 13, 135–145. [Google Scholar]
- Hatefi, S.; Etemadi Sh, M.; Alizargar, J.; Behdadipour, V.; Abou-El-Hossein, K. Two-Axis Continuous Distractor for Mandibular Reconstruction. Bioengineering 2022, 9, 371. [Google Scholar] [CrossRef]
- Jafarpour, T.; Smith, F. Low-level Laser Therapy Device for Assisting Distraction Osteogenesis in Maxillofacial Reconstruction Applications. Majlesi J. Electr. Eng. 2023, 17, 97–108. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Venugopal, A.; Marya, A.; Scribante, A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare 2022, 10, 886. [Google Scholar] [CrossRef]
- Scribante, A.; Gallo, S.; Pascadopoli, M.; Soleo, R.; Di Fonso, F.; Politi, L.; Venugopal, A.; Marya, A.; Butera, A. Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial. Photonics 2022, 9, 138. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized water administration in peri-implant mucositis sites: A randomized clinical trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Scribante, A.; Ghizzoni, M.; Pellegrini, M.; Pulicari, F.; Spadari, F. Laser Devices and Autologous Platelet Concentrates in Prevention and Treatment of Medication-Related Osteonecrosis of the Jaws: A Systematic Review. Medicine 2023, 59, 972. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Natoli, V.; Bruni, A.; Coscione, C.; Magliano, G.; Giacobbo, G.; Morelli, A.; Moressa, S.; Scribante, A. Bio-inspired systems in nonsurgical periodontal therapy to reduce contaminated aerosol during COVID-19: A comprehensive and bibliometric review. J. Clin. Med. 2020, 9, 3914. [Google Scholar] [CrossRef]
- Ibrahim, M.M.; Patwardhan, A.; Gilbraith, K.B.; Moutal, A.; Yang, X.; Chew, L.A.; Largent-Milnes, T.; Malan, T.P.; Vanderah, T.W.; Porreca, F.; et al. Long-lasting antinociceptive effects of green light in acute and chronic pain in rats. Pain 2017, 158, 347–360. [Google Scholar] [CrossRef] [Green Version]
- Almpani, K.; Kantarci, A. Nonsurgical Methods for the Acceleration of the Orthodontic Tooth Movement. Front. Oral Biol. 2015, 18, 80–91. [Google Scholar] [CrossRef]
- Pomini, K.T.; Andreo, J.C.; De Rodrigues, A.C.; De Gonçalves, J.B.O.; Daré, L.R.; German, I.J.S.; Rosa, G.M.; Buchaim, R.L. Effect of low-intensity pulsed ultrasound on bone regeneration biochemical and radiologic analyses. J. Ultrasound Med. 2014, 33, 713–717. [Google Scholar] [CrossRef] [Green Version]
- Saito, S.; Shimizu, N. Stimulatory effects of low-power laser irradiation on bone regeneration in midpalatal suture during expansion in the rat. Am. J. Orthod. Dentofac. Orthop. 1997, 111, 525–532. [Google Scholar] [CrossRef]
- Facchin, F.; Canaider, S.; Tassinari, R.; Zannini, C.; Bianconi, E.; Taglioli, V.; Olivi, E.; Cavallini, C.; Tausel, M.; Ventura, C. Physical energies to the rescue of damaged tissues. World J. Stem Cells 2019, 11, 297–321. [Google Scholar] [CrossRef]
- Farzan, A.; Khaleghi, K.; Pirayesh, Z. Effect of Low-Level Laser Therapy on Bone Formation in Rapid Palatal Expansion: A Systematic Review. J. Lasers Med. Sci. 2022, 13, e13. [Google Scholar] [CrossRef]
- Berni, M.; Brancato, A.M.; Torriani, C.; Bina, V.; Annunziata, S.; Cornella, E.; Trucchi, M.; Jannelli, E.; Mosconi, M.; Gastaldi, G.; et al. The Role of Low-Level Laser Therapy in Bone Healing: Systematic Review. Int. J. Mol. Sci. 2023, 24, 7094. [Google Scholar] [CrossRef]
- Santos, C.M.d.C.; Pimenta, C.A.d.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Özyurt, A.; Elmas, Ç.; Seymen, C.M.; Peker, V.T.; Altunkaynak, B.; Güngör, M.N. Effects of Low-Level Laser Therapy With a Herbal Extract on Alveolar Bone Healing. J. Oral Maxillofac. Surg. 2018, 76, 287.e1–287.e10. [Google Scholar] [CrossRef]
- Ribeiro, L.N.S.; Monteiro, P.M.; Barretto, G.D.; Luiz, K.G.; Alves, S.Y.F.; Stuani, M.B.S. The effect of cigarette smoking and low-level laser irradiation in RANK/RANKL/OPG expression. Braz. Dent. J. 2020, 31, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, L.N.S.; de Figueiredo, F.A.T.; da Silva Mira, P.C.; Arnez, M.F.M.; Matsumoto, M.A.N.; de Menezes, L.M.; Küchler, E.C.; Stuani, M.B.S. Low-level laser therapy (LLLT) improves alveolar bone healing in rats. Lasers Med. Sci. 2022, 37, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Çırak, E.; Özyurt, A.; Peker, T.; Ömeroğlu, S.; Güngör, M.N. Comparative evaluation of various low-level laser therapies on bone healing following tooth extraction: An experimental animal study. J. Cranio-Maxillofac. Surg. 2018, 46, 1147–1152. [Google Scholar] [CrossRef] [PubMed]
- Park, J.J.; Kang, K.L. Effect of 980-nm GaAlAs diode laser irradiation on healing of extraction sockets in streptozotocin-induced diabetic rats: A pilot study. Lasers Med. Sci. 2012, 27, 223–230. [Google Scholar] [CrossRef]
- Oliveira, E.A.; de Oliveira, V.G.M.; Pires, J.A.; Barreto, A.L.S.; Ribeiro, M.A.G.; Pinheiro, A.L.B.; Marques, A.M.C.; de Melo, C.M.; de Albuquerque, R.L.C. Effect of low-level laser therapy and mineral trioxide aggregate on alveolar bone repair. Braz. J. Oral Sci. 2008, 7, 1657–1661. [Google Scholar]
- Pretel, H.; Lizarelli, R.F.Z.; Ramalho, L.T.O. Effect of low-level laser therapy on bone repair: Histological study in rats. Lasers Surg. Med. 2007, 39, 788–796. [Google Scholar] [CrossRef]
- Park, J.B.; Ahn, S.J.; Kang, Y.G.; Kim, E.C.; Heo, J.S.; Kang, K.L. Effects of increased low-level diode laser irradiation time on extraction socket healing in rats. Lasers Med. Sci. 2015, 30, 719–726. [Google Scholar] [CrossRef]
- Abdel Hamid, M.A.; Zaied, A.A.; Zayet, M.K.; Abdelmageed, H.; Hassan, E.A.; Amaroli, A. Efficacy of Flat-Top Hand-Piece Using 980 nm Diode Laser Photobiomodulation on Socket Healing after Extraction: Split-Mouth Experimental Model in Dogs. Photochem. Photobiol. 2021, 97, 627–633. [Google Scholar] [CrossRef]
- Fukuoka, H.; Daigo, Y.; Enoki, N.; Taniguchi, K.; Sato, H. Influence of carbon dioxide laser irradiation on the healing process of extraction sockets. Acta Odontol. Scand. 2010, 69, 33–40. [Google Scholar] [CrossRef]
- Rochkind, S.; Kogan, G.; Luger, E.G.; Salame, K.; Karp, E.; Graif, M.; Weiss, J. Molecular Structure of the Bony Tissue after Experimental Trauma to the Mandibular Region followed by Laser Therapy. Photomed. Laser Surg. 2004, 22, 249–253. [Google Scholar] [CrossRef]
- Luca, R.E.; Giuliani, A.; Mănescu, A.; Heredea, R.; Hoinoiu, B.; Constantin, G.D.; Duma, V.F.; Todea, C.D. Osteogenic potential of bovine bone graft in combination with laser photobiomodulation: An ex vivo demonstrative study in wistar rats by cross-linked studies based on synchrotron microtomography and histology. Int. J. Mol. Sci. 2020, 21, 778. [Google Scholar] [CrossRef] [Green Version]
- Forte, C.P.F.; Matos, A.P.; Mendes, F.H.; Dias, C.C.; Ferreira, A.E.C.; Bezerra, T.P.; Sousa, F.B.; Barros Silva, P.G. De Photobiomodulation Therapy Reduces the Inflammatory Process without Inhibiting Bone Deposition in Rats in an Extraction Model. Photobiomodulation Photomed. Laser Surg. 2020, 38, 673–678. [Google Scholar] [CrossRef]
- Statkievicz, C.; Toro, L.F.; de Mello-Neto, J.M.; de Sá, D.P.; Casatti, C.A.; Issa, J.P.M.; Cintra, L.T.A.; de Almeida, J.M.; Nagata, M.J.H.; Garcia, V.G.; et al. Photomodulation multiple sessions as a promising preventive therapy for medication-related osteonecrosis of the jaws after tooth extraction in rats. J. Photochem. Photobiol. B Biol. 2018, 184, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Mergoni, G.; Vescovi, P.; Sala, R.; Merigo, E.; Passerini, P.; Maestri, R.; Corradi, D.; Govoni, P.; Nammour, S.; Bianchi, M.G. The effect of laser therapy on the expression of osteocalcin and osteopontin after tooth extraction in rats treated with zoledronate and dexamethasone. Support. Care Cancer 2016, 24, 807–813. [Google Scholar] [CrossRef]
- Romão, M.M.A.; Marques, M.M.; Cortes, A.R.G.; Horliana, A.C.R.T.; Moreira, M.S.; Lascala, C.A. Micro-computed tomography and histomorphometric analysis of human alveolar bone repair induced by laser phototherapy: A pilot study. Int. J. Oral Maxillofac. Surg. 2015, 44, 1521–1528. [Google Scholar] [CrossRef]
- Mozzati, M.; Martinasso, G.; Cocero, N.; Pol, R.; Maggiora, M.; Muzi, G.; Canuto, R.A. Superpulsed laser therapy on healing process after tooth extraction in patients waiting for liver transplantation. Lasers Med. Sci. 2012, 27, 353–359. [Google Scholar] [CrossRef]
- Araújo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Euler, H. Die Heilung von Extraktionswunden. Dtsch. Monatschr. Zahnh 1923, 41, 655. [Google Scholar]
- Carvalho, T.L.; Bombonato, K.F.B.L. Histometric analysis of rat alveolar wound healing. Braz Dent J. 1997, 8, 9–12. [Google Scholar]
- Zhao, Y.; Gong, Y.; Liu, X.; He, J.; Zheng, B.; Liu, Y. The Experimental Study of Periodontal Ligament Stem Cells Derived Exosomes with Hydrogel Accelerating Bone Regeneration on Alveolar Bone Defect. Pharmaceutics 2022, 14, 2189. [Google Scholar] [CrossRef]
- Pitol-Palin, L.; Batista, F.R.d.S.; Gomes-Ferreira, P.H.S.; Mulinari-Santos, G.; Ervolino, E.; Souza, F.Á.; Matsushita, D.H.; Okamoto, R. Different stages of alveolar bone repair process are compromised in the type 2 diabetes condition: An experimental study in rats. Biology 2020, 9, 471. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.F.; Wang, C.Y.; Wan, P.; Wang, S.G.; Wang, X.M. Comparison of bone regeneration in alveolar bone of dogs on mineralized collagen grafts with two composition ratios of nanohydroxyapatite and collagen. Regen. Biomater. 2016, 3, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamal, M.; Andersson, L.; Tolba, R.; Al-Asfour, A.; Bartella, A.K.; Gremse, F.; Rosenhain, S.; Hölzle, F.; Kessler, P.; Lethaus, B. Bone regeneration using composite non-demineralized xenogenic dentin with beta-tricalcium phosphate in experimental alveolar cleft repair in a rabbit model. J. Transl. Med. 2017, 15, 263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.C.; Wang, H.; Li, J.; Zhang, D.; Yin, L.Q.; Yan, Y.F.; Ma, X. Repair of alveolar cleft bone defects by bone collagen particles combined with human umbilical cord mesenchymal stem cells in rabbit. BioMed. Eng. OnLine 2020, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- Torres, H.; Mauricio, F.; Mendoza, R.; Alvítez-Temoche, D.; Medina, J.; Mayta-Tovalino, F. Histological Comparison of Post-extraction Alveolar Bone Repair Treated with Melatonin and Calcium Sulfate: An In Vivo Study in Cavia porcellus. J.Contemp. Dent. Pract. 2021, 22, 739–744. [Google Scholar] [CrossRef]
- Mandarino, D.; Luz, D.; Moraschini, V.; Rodrigues, D.M.; Alveolar, E.S.P.B. Alveolar ridge preservation using a non-resorbable membrane: Randomized clinical trial with biomolecular analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 1465–1473. [Google Scholar] [CrossRef]
- Bigham-sadegh, A.; Oryan, A. Selection of animal models for pre-clinical strategies in evaluating the fracture healing, bone graft substitutes and bone tissue regeneration and engineering fracture healing, bone graft substitutes and bone tissue regeneration. Connect. Tissue Res. 2015, 56, 175–194. [Google Scholar] [CrossRef]
- Al-obaidi, M.M.J.; Al-bayaty, F.H.; Al, R.; Hassandarvish, P.; Rouhollahi, E. ScienceDirect Protective effect of ellagic acid on healing alveolar bone after tooth extraction in rat—A histological and immunohistochemical study. Arch. Oral Biol. 2014, 59, 987–999. [Google Scholar] [CrossRef]
- Ervolino, E.; Statkievicz, C.; Felipe, L.; De Mello-Neto, J.M.; Priscila, T.; Paulo, J.; Issa, M.; Cássia, R.; Dornelles, M.; Milanezi, J.; et al. Antimicrobial photodynamic therapy improves the alveolar repair process and prevents the occurrence of osteonecrosis of the jaws after tooth extraction in senile rats treated with zoledronate. Bone 2019, 120, 101–113. [Google Scholar] [CrossRef]
- Panzarini, R.; Sonoda, C.K.; Tomiko, C.; Hamata, M. Histological and immunohistochemical analyses of the chronology of healing process after immediate tooth replantation in incisor rat teeth. Dent. Traumatol. 2013, 29, 15–22. [Google Scholar] [CrossRef]
- Van der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef]
- Farivar, S.; Malekshahabi, T.; Shiari, R. Biological Effects of Low Level Laser Therapy. J. Lasers Med. Sci. 2014, 5, 58–62. [Google Scholar]
- Jaeger, F.; Chiavaioli, G.M.d.O.; de Toledo, G.L.; Freire-Maia, B.; Amaral, M.B.F.; de Abreu, M.H.N.G.; de Arruda, J.A.A.; Mesquita, R.A. Efficacy and safety of diode laser during circumvestibular incision for Le Fort I osteotomy in orthognathic surgery: A triple-blind randomized clinical trial. Lasers Med. Sci. 2020, 35, 395–402. [Google Scholar] [CrossRef]
- Basso, F.G.; Oliveira, C.F.; Kurachi, C.; Hebling, J.; Costa, C.A.D.S. Biostimulatory effect of low-level laser therapy on keratinocytes in vitro. Lasers Med. Sci. 2013, 28, 367–374. [Google Scholar] [CrossRef]
- Cavalcanti, T.M.; Quirino De Almeida-Barros, R.; Chaves De Vasconcelos Catão, M.H.; Patrícia, A.; Feitosa, A.; Diógenes, R.; Lins, A.U. Knowledge of the physical properties and interaction of laser with biological tissue in dentistry. An. Bras. De Dermatol. 2011, 86, 955–960. [Google Scholar] [CrossRef] [Green Version]
- Amitha, K.; Paramashivaiah, R.; Laxmaiah, M.; Prabhuji, V.; Subramanya, A.P.; Assiry, A.A.; Peeran, S.W.; Fageeh, H.; Bhavikatti, S.K.; Scardina, G.A. Clinical Assessment of the Effects of Low-Level Laser Therapy on Coronally Advanced Flap Procedure in the Management of Isolated Gingival Recession. Photonics 2022, 9, 932. [Google Scholar] [CrossRef]
- Pasquale, C.; Utyuzh, A.; Mikhailova, M.V.; Colombo, E.; Amaroli, A. Recovery from Idiopathic Facial Paralysis (Bell’ s Palsy) Using Photobiomodulation in Patients Non-Responsive to Standard Treatment: A Case Series Study. Photonics 2021, 8, 341. [Google Scholar] [CrossRef]
- Poiani, G.d.C.R.; Zaninotto, A.L.; Carneiro, A.M.C.; Zangaro, R.A.; Salgado, A.S.I.; Parreira, R.B.; de Andrade, A.F.; Teixeira, M.J.; Paiva, W.S. Photobiomodulation using low-level laser therapy (LLLT) for patients with chronic traumatic brain injury: A randomized controlled trial study protocol. Trials 2018, 19, 17. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, C.; Bueno, D.S.; Clara, M.; Tonin, C.; Buchaim, D.V.; Barraviera, B.; Seabra, R.; Junior, F.; Paulo, S.; Santos, S.; et al. Morphofunctional Improvement of the Facial Nerve and Muscles with Repair Using Heterologous Fibrin Biopolymer and Photobiomodulation. Pharmaceuticals 2023, 16, 653. [Google Scholar] [CrossRef]
- Buchaim, D.V.; Rodrigues, A.C.; Buchaim, R.L.; Barraviera, B.; Junior, R.S.F.; Junior, G.M.R.; Bueno, C.R.S.; Roque, D.D.; Dias, D.V.; Dare, L.R.; et al. The new heterologous fibrin sealant in combination with low-level laser therapy (LLLT) in the repair of the buccal branch of the facial nerve. Lasers Med. Sci. 2016, 31, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Buchaim, R.L.; Andreo, J.C.; Barraviera, B.; Ferreira Junior, R.S.; Buchaim, D.V.; Rosa Junior, G.M.; De Oliveira, A.L.R.; De Castro Rodrigues, A. Effect of low-level laser therapy (LLLT) on peripheral nerve regeneration using fibrin glue derived from snake venom. Injury 2015, 46, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Lovisetto, R.; Malavazzi, T.C.D.S.; Andreo, L.; Rodrigues, M.F.S.D.; Bussadori, S.K.; Fernandes, K.P.S.; Mesquita-Ferrari, R.A. Photobiomodulation Using Different Infrared Light Sources Promotes Muscle Precursor Cells Migration and Proliferation. Photonics 2022, 9, 469. [Google Scholar] [CrossRef]
- Pomini, K.T.; Buchaim, D.V.; Bighetti, A.C.C.; Hamzé, A.L.; Reis, C.H.B.; Duarte, M.A.H.; Alcalde, M.P.; Barraviera, B.; Júnior, R.S.F.; de Souza, A.T.; et al. Tissue Bioengineering with Fibrin Scaffolds and Deproteinized Bone Matrix Associated or Not with the Transoperative Laser Photobiomodulation Protocol. Molecules 2023, 28, 407. [Google Scholar] [CrossRef] [PubMed]
- Reis, C.H.B.; Buchaim, R.L.; Pomini, K.T.; Hamzé, A.L.; Zattiti, I.V.; Duarte, M.A.H.; Alcalde, M.P.; Barraviera, B.; Ferreira Júnior, R.S.; Pontes, F.M.L.; et al. Effects of a Biocomplex Formed by Two Scaffold Biomaterials, Hydroxyapatite/Tricalcium Phosphate Ceramic and Fibrin Biopolymer, with Photobiomodulation, on Bone Repair. Polymers 2022, 14, 2075. [Google Scholar] [CrossRef]
- Angeletti, P.; Pereira, M.D.; Gomes, H.C.; Hino, C.T.; Ferreira, L.M. Effect of low-level laser therapy (GaAlAs) on bone regeneration in midpalatal anterior suture after surgically assisted rapid maxillary expansion. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, e38–e46. [Google Scholar] [CrossRef]
- Neto, F.C.J.; Martimbianco, A.L.C.; de Andrade, R.P.; Bussadori, S.K.; Mesquita-Ferrari, R.A.; Fernandes, K.P.S. Effects of photobiomodulation in the treatment of fractures: A systematic review and meta-analysis of randomized clinical trials. Lasers Med. Sci. 2020, 35, 513–522. [Google Scholar] [CrossRef]
- De Souza, G.H.M.; Ferraresi, C.; Moreno, M.A.; Pessoa, B.V.; Damiani, A.P.M.; Filho, V.G.; dos Santos, G.V.; Zamunér, A.R. Acute effects of photobiomodulation therapy applied to respiratory muscles of chronic obstructive pulmonary disease patients: A double-blind, randomized, placebo-controlled crossover trial. Lasers Med. Sci. 2020, 35, 1055–1063. [Google Scholar] [CrossRef]
- Alsharnoubi, J.; Shoukry, K.E.S.; Fawzy, M.W.; Mohamed, O. Evaluation of scars in children after treatment with low-level laser. Lasers Med. Sci. 2018, 33, 1991–1995. [Google Scholar] [CrossRef]
- Guncay, T.; Oyanedel, M.; Lemus, M.; Weinstein, A.; Ardiles, Á.O.; Marcos, J.; Fernandes, A.; Renato, Z.; Muñoz, P. The Transcranial Light Therapy Improves Synaptic Plasticity in the Alzheimer ’ s Disease Mouse Model. Brain Sci. 2022, 12, 1272. [Google Scholar] [CrossRef]
- Metin, R.; Tatli, U.; Evlice, B. Effects of low-level laser therapy on soft and hard tissue healing after endodontic surgery. Lasers Med. Sci. 2018, 33, 1699–1706. [Google Scholar] [CrossRef]
- De Oliveira Rosso, M.P.; Buchaim, D.V.; Pomini, K.T.; Della Coletta, B.B.; Bertoni Reis, C.H.; Galletti Pilon, J.P.; Duarte Júnior, G.; Buchaim, R.L. Photobiomodulation therapy (PBMT) applied in bone reconstructive surgery using bovine bone grafts: A systematic review. Materials 2019, 12, 4051. [Google Scholar] [CrossRef] [Green Version]
- Rosso, M.; Buchaim, D.; Kawano, N.; Furlanette, G.; Pomini, K.; Buchaim, R. Photobiomodulation Therapy (PBMT) in Peripheral Nerve Regeneration: A Systematic Review. Bioengineering 2018, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Bosco, A.F.; Faleiros, P.L.; Carmona, L.R.; Garcia, V.G.; Theodoro, L.H.; de Araujo, N.J.; Nagata, M.J.H.; de Almeida, J.M. Effects of low-level laser therapy on bone healing of critical-size defects treated with bovine bone graft. J. Photochem. Photobiol. B 2016, 163, 303–310. [Google Scholar] [CrossRef] [Green Version]
- He, W.L.; Yu, F.Y.; Li, C.J.; Pan, J.; Zhuang, R.; Duan, P.J. A systematic review and meta-analysis on the efficacy of low-level laser therapy in the management of complication after mandibular third molar surgery. Lasers Med. Sci. 2015, 30, 1779–1788. [Google Scholar] [CrossRef]
- Fallahnezhad, S.; Piryaei, A.; Tabeie, F.; Nazarian, H.; Darbandi, H.; Amini, A.; Mostafavinia, A.; Ghorishi, S.K.; Jalalifirouzkouhi, A.; Bayat, M. Low-level laser therapy with helium–neon laser improved viability of osteoporotic bone marrow-derived mesenchymal stem cells from ovariectomy-induced osteoporotic rats. J. Biomed. Opt. 2016, 21, 098002. [Google Scholar] [CrossRef]
- Sterczała, B.; Grzech-Lésniak, K.; Michel, O.; Trzeciakowski, W.; Dominiak, M.; Jurczyszyn, K. Assessment of human gingival fibroblast proliferation after laser stimulation in vitro using different laser types and wavelengths (1064, 980, 635, 450, and 405 nm)—Preliminary report. J. Pers. Med. 2021, 11, 98. [Google Scholar] [CrossRef]
- Ebrahimi, T.; Moslemi, N.; Rokn, A.; Heidari, M.; Nokhbatolfoghahaie, H.; Fekrazad, R. The influence of low-intensity laser therapy on bone healing. J. Dent. 2012, 9, 238–248. [Google Scholar]
- Palczewska-Komsa, M.; Kaczor-Wiankowska, K.; Nowicka, A. New bioactive calcium silicate cement mineral trioxide aggregate repair high plasticity (Mta hp)— a systematic review. Materials 2021, 14, 4573. [Google Scholar] [CrossRef]
- Mild, K.H.; Lundström, R.; Wilén, J. Non-ionizing radiation in swedish health care—Exposure and safety aspects. Int. J. Environ. Res. Public Health 2019, 16, 1186. [Google Scholar] [CrossRef] [Green Version]
- Del Vecchio, A.; Tenore, G.; Luzi, M.C.; Palaia, G.; Mohsen, A.; Pergolini, D.; Romeo, U. Laser photobiomodulation (Pbm)—A possible new frontier for the treatment of oral cancer: A review of in vitro and in vivo studies. Healthcare 2021, 9, 134. [Google Scholar] [CrossRef]
- Luchian, I.; Budală, D.G.; Baciu, E.R.; Ursu, R.G.; Diaconu-Popa, D.; Butnaru, O.; Tatarciuc, M. The Involvement of Photobiology in Contemporary Dentistry—A Narrative Review. Int. J. Mol. Sci. 2023, 24, 3985. [Google Scholar] [CrossRef] [PubMed]
- Luk, K.; Zhao, I.S.; Gutknecht, N.; Chu, C.H. Use of carbon dioxide lasers in dentistry. Lasers Dent. Sci. 2019, 3, 1–9. [Google Scholar] [CrossRef]
- De Oliveira Rosso, M.P.; Oyadomari, A.T.; Pomini, K.T.; Della Coletta, B.B.; Shindo, J.V.T.C.; Júnior, R.S.F.; Barraviera, B.; Cassaro, C.V.; Buchaim, D.V.; Teixeira, D.D.B.; et al. Photobiomodulation therapy associated with heterologous fibrin biopolymer and bovine bone matrix helps to reconstruct long bones. Biomolecules 2020, 10, 383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.S.; Wu, J.; Xu, H.; Wang, Z. Emerging Light-Emitting Materials for Photonic Integration. Adv. Mater. 2021, 33, 2003733. [Google Scholar] [CrossRef] [PubMed]
- Pou-Álvarez, P.; Riveiro, A.; Nóvoa, X.R.; Fernández-Arias, M.; del Val, J.; Comesaña, R.; Boutinguiza, M.; Lusquiños, F.; Pou, J. Nanosecond, picosecond and femtosecond laser surface treatment of magnesium alloy: Role of pulse length. Surf. Coat. Technol. 2021, 427, 127802. [Google Scholar] [CrossRef]
- Hamad, A.; Li, L.; Liu, Z. A comparison of the characteristics of nanosecond, picosecond and femtosecond lasers generated Ag, TiO2 and Au nanoparticles in deionised water. Appl. Phys. A Mater. Sci. Process. 2015, 120, 1247–1260. [Google Scholar] [CrossRef]
- Serbin, J.; Bauer, T.; Fallnich, C.; Kasenbacher, A.; Arnold, W.H. Femtosecond lasers as novel tool in dental surgery. Appl. Surf. Sci. 2002, 197–198, 737–740. [Google Scholar] [CrossRef]
- Saito, C.T.M.H.; Gulinelli, J.L.; Panzarini, S.R.; Garcia, V.G.; Okamoto, R.; Okamoto, T.; Sonoda, C.K.; Poi, W.R. Effect of low-level laser therapy on the healing process after tooth replantation: A histomorphometrical and immunohistochemical analysis. Dent. Traumatol. 2011, 27, 30–39. [Google Scholar] [CrossRef]
- Freitas, N.R.; Guerrini, L.B.; Esper, L.A.; Sbrana, M.C.; Dalben, G.D.S.; Soares, S.; Almeida, A.L.P.F. Evaluation of photobiomodulation therapy associated with guided bone regeneration in critical size defects. In vivo study. J. Appl. Oral Sci. 2018, 26, e20170244. [Google Scholar] [CrossRef]
- Colombo, M.; Gallo, S.; Garofoli, A.; Poggio, C.; Arciola, C.R.; Scribante, A. Ozone gel in chronic periodontal disease: A randomized clinical trial on the anti-inflammatory effects of ozone application. Biology 2021, 10, 625. [Google Scholar] [CrossRef]
- Hatefi, S.; Alizargar, J.; Le Roux, F.; Hatefi, K.; Etemadi Sh, M.; Davids, H.; Hsieh, N.C.; Smith, F.; Abou-El-Hossein, K. Review of physical stimulation techniques for assisting distraction osteogenesis in maxillofacial reconstruction applications. Med. Eng. Phys. 2021, 91, 28–38. [Google Scholar] [CrossRef]
- Huang, X.; Das, R.; Patel, A.; Duc Nguyen, T. Physical Stimulations for Bone and Cartilage Regeneration. Regen. Eng. Transl. Med. 2018, 4, 216–237. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Objective | Type of Laser (Manufacturer) | Wavelength (nm) | Output Power (mW) | Power Density | Energy Density (J/cm2) | Therapeutic Variables | Intervention | Laser Application | Outcome/ Results | Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Özyurt et al., 2018 [40] | Investigate the effect of GaAlAs diode laser used in LLLT with the application of Mecsina herbal hemostopper on mandibular alveolar bone healing | GaAlAs Diode Laser (BLT®, Brno, Czech Republic) | 830 | 50 | -/- | 10 | Mecsina | Defects were created on the left mandibular diastema sites of 32 rats that were allocated to four groups: CG (A), Laser Group (B), Mecsina Group (C) and Laser–Mecsina Group (D) | Once every 24 h for 7 days | There were more osteoblastic cells in the laser and laser-Mecsina groups then the others. Moreover, the laser–Mecsina combination group showed more bone tissue formed | Laser treatment, Mecsina application and the combination of both were more effective treatments on alveolar bone healing than the others |
| Ribeiro et al., 2020 [41] | Evaluate osteoclastogenesis in tooth treated with LLLT and exposure to cigarette smoke, after tooth extraction in rats, at different times of healing | GaAlAs Diode Laser (Photon Laser®, DMC Equipaments, São Carlos, Brazil) | 830 | 30 | -/- | 54 | -/- | Four groups of 15 Wistar rats were divided in CG (with right maxillary extraction-ME); Exp I (with ME and LLLT); Exp II (with ME and cigarette smoke) and Exp III (with ME, LLLT and cigarette smoke) | Immediately after extraction and once per day for 3 days | Exp III group expression of RANK, RANKL and OPG genes was higher than Exp II, but lower than CG and Exp I groups. Moreover, Exp I showed up regulation of these genes over all time compared to the CG | The results concluded that LLLT had positive effect, whereas cigarette smoke had negative effect on RANK, RANKL and OPG gene expression in bone remodelling process |
| Ribeiro et al., 2022 [42] | Evaluate the effect of LLLT in enhancing bone healing in irradiation alveolus post-tooth extraction | GaAlAs Diode Laser (Photon Laser®, DMC Equipaments, São Carlos, Brazil) | 830 | 30 | -/- | 54 | -/- | Two groups of 30 Wistar rats were divided into CG (with left maxillary molar extraction) and EG (with tooth extraction and LLLT). These groups were subdivided in six groups according to the observation time point: 1, 2, 3, 5, 7 and 10 days post-extraction | Immediately after extraction and once per day for 3 days | Histomorphometric analysis revealed an increase of osteoblast (RUNX-2) and osteoclast (TRAP) activity in the area percentage of cancellous bone in the EG compared to CG | The experiment concluded that the application of LLLT enhanced healing and mineralization on alveolar region |
| Çırak et al., 2018 [43] | To evaluate the effects of He-Ne and GaAlAs lasers with various doses on bone healing following tooth extraction | He-Ne laser (LABpen MED 30; Therapilaser, Graz, Austria) and GaAlAs laser (BTL Laser 2000; BTL Industries Ltd., Hertfordshire, UK) | Group B: 655 Group C: 830 | Group B: 30 Group C: 100 | -/- | B1(6); B2 (10); C1 (6); C2 (10) | -/- | Five groups were divided: four groups with He-Ne (B), GaAlAs (C) lasers and CG (A). | Once per day for 7 days; 6 J/cm2 (B1/C1) and 10 J/cm2 (B2/C2) | Both laser groups showed faster bone healing and the GaAlAs laser increased vascular immunoreactivity. The most increasing in bone formation was observed in the B2 | LLLT was effective on alveolar bone healing and that energy dose of 10 J/cm2 did not have inhibition effect on bone regeneration |
| Park et al., 2012 [44] | To evaluate the effect of LLLT on the healing of extraction sockets in diabetic and healthy rats | GaAlAs diode laser (Diobeauty-30®, Diotech, Busan, Korea) | 980 | 10 | -/- | 13.95 | -/- | A total of 48 rats were divided into normal (n = 24) and diabetic (n = 24) rats. Then, after a tooth extraction, these were subdivided in groups submitted to LLLT and not irradiated | Every day after tooth extraction for 3, 5, 7 or 14 days | Both groups that were submitted to LLLT showed faster initial healing and more new alveolar bone formation than the groups without laser therapy | LLLT is beneficial for the initial stages of alveolar bone healing and for further calcification |
| Oliveira et al., 2008 [45] | To evaluate the effect of LLLT associated to mineral trioxide aggregate (MTA) on the alveolar bone repair process | Twin Laser (MMOptics®, São Carlos, Brazil) | 1780 | 40 | -/- | 16 | Mineral trioxide aggregate (Angelus®; Londrina, Brazil) | Forty Wistar rats were divided into four groups after tooth extraction: G1 (control group); G2 (MTA); G3 (LLLT) and G4 (LLLT and MTA) | Four sessions every 48 h after extraction | In G2, was observed intense vascular hyperemia and chronic inflammation while in G4 it was quite distinguishable and there was intense deposition of thin bone trabeculae | It was observed that LLLT was the most successful treatment to improve alveolar bone repair |
| Pretel et al., 2007 [46] | To evaluate the bone repair in defects created in rat lower jaws after stimulation with infrared LLLT directly on the injured tissue | GaAlAs diode laser (Laser Beam Multi Laser DR 500 device®; Laser Beam Ind. Tecn. Ltd., Niterói, Brazil) | 780 | 50 | -/- | 178 | -/- | Thirty Holtzman rats that had defects prepared in their mandibles were divide in two groups: Control Group, CG and Laser group, LG (n = 15), which were subdivided in three evaluation period (15, 45 and 60 days) | A single application after tooth extraction | The LG exhibited an advanced tissue response compared to the CG, decreasing the initial inflammatory reaction and promoting rapid new bone matrix formation | LLLT showed to be a good method by stimulating the modulation of inflammatory response and anticipating the resolution to normal conditions |
| Park et al., 2015 [47] | To investigate the effects of irradiation time on the healing of extraction sockets by evaluating the expressions of genes and proteins related to bone healing | GaAlAs diode laser (Diobeauty- 30®; Diotech, Busan, Korea) | 980 | 10 | -/- | 13.95 | - | Twenty-four rats were submitted to a tooth extraction and then were divided into four groups according to the time that the wound received LLLT | For 0, 1, 2 or 5 min each day for 3 or 7 days | LLLT increased the expressions of all tested genes related to bone healing and vascular endothelial growth factor. The highest levels of gene expressions were in the 5 min group after 7 days | LLLT had positive effects on the early stages of bone healing of extraction sockets in rats, which were irradiation time-dependent |
| Abdel Hamid et al., 2021 [48] | To evaluate the effect of PBM on socket healing in the maxilla and mandible | Wiser wireless diode laser (Doctor Smile—LAMBDA Spa Vicenza, Italy) | 980 | 600 | 770 mW/ cm2 | 46 | -/- | It was a split-mouth experimental where six dogs had the 3rd premolar tooth extracted from both sides of maxilla and mandible, then the right side was treated with laser and the left side was kept as control | Immediately after tooth extraction and at 48 h interval for 14 days | Maxillary sockets in the PBM group had higher bone density compared to control one at 3, 4 and 5 weeks | The experiment concluded that PBM using a flat-top hand-piece of 980 nm improved the bone density of extraction sockets |
| Fukuoka et al., 2010 [49] | To clarify the healing promoting effects of carbon dioxide laser irradiation in high and low reactive-level laser therapies (HLLT and LLLT, respectively) on extraction sockets | CO2 laser (Panalas CO5∑; Panasonic Shikoku Electronics Co., Ltd., Osaka, Japan) | -/- | LLLT and HLLT: 1000 | -/- | LLLT- 40 J/cm2 HLLT- 152 J/cm2 | HLLT | Forty-two Wistar rats were divided into two groups: Laser group (LG), which underwent HLLT immediately after tooth extraction and LLLT 1 day post-extraction. Tissue was excised 6 h, 3, 7 or 21 days after extraction | A single application one day after tooth extraction | On day 3, almost no α-SMA-positive myofibroblasts were present in the irradiation group while many of these were present in the CG. On day 21, the alveolar bone height was significantly higher in the irradiation group | The ppearance of fewer α-SMA-positive myofibroblasts and the higher alveolar bone formed in the LG suggest that laser therapy improves the healing of alveolar bone |
| Rochkind et al., 2004 [50] | To investigate the therapeutic efficiency of laser irradiation and Bio-Oss® on the post-traumatic regeneration of bone tissue in rats | He-Ne laser | 632.8 | 35 | -/- | -/- | Bio-Oss® | Twenty-nine Wistar rats were submitted to a bone defect in the right alveolar process, then were divided into four groups: G1 (n = 5, control); G2 (n = 8, filled with Bio-Oss), G3 (n = 8, treated by laser), G4 (n = 8, Bio-Oss + laser) | For 20 min daily for the following 14 consecutive days | The G3 showed the process of absorption of inorganic component increased compared to the CG. The groups G3 and G4 showed the mineralization index significantly increased | The results suggest that the use of LLLT irradiation for the repair of bone defect can significantly improve the quality and velocity of recovery |
| Luca et al., 2020 [51] | Evaluation of the effect of PBM on the bone regeneration process, using rat calvarial defects of filled with xenograft | GaAlAs laser (IRRADIA Mid-Laser® Stockholm, Sweden) | 808 | 450 | 450 mW/ cm2 | 24.075 | Bovine bone graft (NuOss® natural cancellous and cortical bone matrix, ACE Surgical Supply, Brockton, MA, USA) and collagen membrane (ACE RCM6® Resorbable Collagen Membrane, ACE Surgical Supply, Brockton, MA, USA) | Twenty-four Wistar rats had a circular defect created in the calvaria, then were divided into three groups: NC group (spontaneous healing), PC group (filled with bone graft and covered with collagen membrane) and +LLLT group (bone graft + membrane + laser) | Surgery day and every 48 h for 14, 21 and 30 days | The +LLLT group on the 14-day fragments revealed well-represented fibrous (young) connective tissue and low inflammatory infiltration compared to other groups. Moreover, the thickness of newly-formed bone on the defect borders is higher in the +LLLT group than in the PC group from the same period | The results concluded that PBM is significantly effective in short periods as it increases the bone volume with respect to the exclusive use of the xenograft |
| Forte et al., 2020 [52] | To evaluate the influence of photobiomodulation therapy (PBMT) application during bone healing post exodontia in rats | GaAlAs active-mode diode infrared laser (Therapy EC®; DMC Equipments, São Carlos, Brazil) | 810 | 100 | -/- | 70 | -/- | Eighty-four Wistar rats were submitted to tooth extraction and then were divided into two groups: control group (CG) and test group (TG) with LLLT | Immediately after extraction and every 72 h (day 1, 3, 6, 9, 12, 15, 18, 21, 24 and 27 after extraction | There was no difference in body variation and bone neoformation between the groups, but TG presented inflammatory decrease and higher blood vessels count throughout the repair process | PBMT attenuated the inflammatory process after exodontia without interfering with bone neoformation |
| Statkievicz et al., 2018 [53] | To evaluate effects of PBM on the alveolar repair process of rats with major risk factors for medication-related osteonecrosis of the jaws (MRONJ) | InGaAlP laser device (Thera Lase®, DMC Equipaments Ltd., São Carlos, Brazil) | 660 | 35 | 1.23 W/cm2 | 74.2 | -/- | Twenty-eight Wistar rats were divided into four groups: VEH (n = 7, treated with vehicle); VEH-PMB (n = 7, vehicle and PBM); ZOL (n = 7, treated with zoledronate); and ZOL-PBM (n = 7, zoledronate and PBM) | For 0, 2 and 4 days after extraction | ZOL-PBM showed significant improvement compared to ZOL, such as greater amount of mature collagen fibres, positive repair tissue and decrease of inflammatory molecules | PBM in multiple sessions can improve the alveolar repair process, constituting a promising preventive therapy to avoid the onset |
| Mergoni et al., 2016 [54] | To investigate the action of laser therapy on extraction socket healing in rats in conditions at risk for MRONJ | Nd:YAG laser therapy (Fidelis®, Fotona, Slovenia) | 1064 | 1250 | 268.8 W/cm2 | 14.37 | Zoledonate and dexamethasone | Thirty Sprague-Dawley rats were divided into four groups: control group (CG); laser group (L); treatment group (T) and laser + treatment group (T+L). | After tooth extraction and the following 2, 4 and 6 days | The groups L and T+L revealed significant higher expression of neoformation bone (OCN) than groups CG and T. However, the expression of OPN did not present significant differences among the groups | The results demonstrated that laser therapy after tooth extraction can promote increase in bone healing, even in conditions at risk for MRONJ |
| Reference | Objective | Type of Laser (Manufacturer) | Wavelength (nm) | Output Power (mW) | Power Density | Energy Density (J/cm2) | Therapeutic Variables | Intervention | Laser Application | Outcome/Results | Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Romão et al., 2015 [55] | To evaluate the human alveolar bone repair 40 days after molar extraction in patients submitted to LPT (Laser phototherapy) | GaAlAs diode laser device (Twin Flex®; MMOptics Ltd., São Carlos, Brazil) | 808 | 100 | -/- | 75 | -/- | Twenty patients were divided into Control Group, CG (n = 10) and Laser Group, LG (n = 10) that were submitted to LPT; then 40 days later, samples of the tissue formed were analysed | During the surgical procedure, immediately after the procedure, and at 24 h, 48 h, 72 h, 96 h, 7 days and 14 days after the procedure | The analysis showed that the LG presented higher relative bone volume than the CG. Moreover, the LG showed a significant negative correlation between the thickness and separation of trabeculae, while the CG showed positive correlation between these parameters | LPT is able to accelerate alveolar bone repair after molar extraction, leading to a more homogeneous trabecular configuration represented by large number of trabeculae with a small thickness |
| Mozzati et al., 2012 [56] | To study the effect of laser therapy on alveolar healing process in patients waiting for liver transplantation | GaAlAs laser (Fisioline s.n.c., Verduno, Cuneo, Italy) | 904–910 | 200 | 200 mW/ cm2 | 180 | -/- | Twelve patients waiting for liver transplantation were submitted to a split-mouth study where, after bilateral tooth extraction, one post-extractive defect was treated with laser while the other was left without treatment | Immediately after molar extraction and at days 3 and 5 after the procedure | IL-1β increase and induced IL-6, IL-10, and collagen III was observed in the laser-treated side; in the other side, the parameters were unmodified. Epithelial regeneration evidenced a positive result of laser therapy. Patients reported less pain in the site treated with laser | The results concluded that laser therapy appears to be the treatment of choice for patients due to its clinical efficacy, safety, good tolerance and its ability to prevent inflammation |
| Rosero et al., 2020 [11] | Aimed to evaluate the effects of PBM therapy on alveolar bone repair | GaAIAs diode laser (Photon III®, DMC, São Carlos, Brazil) | 808 | 100 | 3.6 W/cm2 | 89 | -/- | Twenty patients were enrolled in a split-mouth clinical trial where were submitted to bilateral extraction of lower molars. Then one side was treated by the laser, and the other was the control side | Immediate postoperative and after 1, 2, 3, 4, 7 and 15 days | Samples from the PBMT group exhibited a higher number of spatially organized and connected bone trabeculae, as well the higher density of blood vessels when compared with the control group | The results indicated that the PBM therapy improved the new bone trabeculae formation and their connectivity which increased bone surface |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rando, R.G.; Buchaim, D.V.; Cola, P.C.; Buchaim, R.L. Effects of Photobiomodulation Using Low-Level Laser Therapy on Alveolar Bone Repair. Photonics 2023, 10, 734. https://doi.org/10.3390/photonics10070734
Rando RG, Buchaim DV, Cola PC, Buchaim RL. Effects of Photobiomodulation Using Low-Level Laser Therapy on Alveolar Bone Repair. Photonics. 2023; 10(7):734. https://doi.org/10.3390/photonics10070734
Chicago/Turabian StyleRando, Renata Gonçalves, Daniela Vieira Buchaim, Paula Cristina Cola, and Rogerio Leone Buchaim. 2023. "Effects of Photobiomodulation Using Low-Level Laser Therapy on Alveolar Bone Repair" Photonics 10, no. 7: 734. https://doi.org/10.3390/photonics10070734