1. Introduction
Traumatic dental injuries have emerged as a major public health concern worldwide. These injuries commonly occur due to fighting, falls due to playing, road accidents, falling from a bus, medical problem, hitting a wall, being hit with a desk (school), as well as due to physical activities [
1]. Children and young adults are at high risk of suffering traumatic dental injuries (TDIs), affecting their maxillary anterior teeth [
2]. The prevalence ranges from 14–22% globally [
3,
4,
5,
6,
7].
It has been established that the anterior teeth, particularly maxillary central incisors and, to a lesser extent, mandibular central incisors and maxillary lateral incisors, are commonly affected teeth [
8,
9]. These teeth consist of three important structural parts, i.e., the structure of the enamel, dentin, and cementum, as well as the surrounding periodontal ligaments and bone. Several studies reported different values of elastic modulus and yield stresses, depending on the testing method [
10,
11,
12,
13]. Previous studies [
10,
11] have reported the modulus of elasticity of enamel and dentin to be within the range of approximately 10 GPa to 63 GPa and 11 GPa to 17 GPa, respectively. The ultimate yield stress of the enamel and dentin was reported to be maximum 53 GPa and 29 GPa, respectively [
14].
Depending on the varied amounts of loads applied on the teeth, different types of tooth fractures were observed. A commonly observed fractured tooth involves either the breakage of the crown part or the breakage of both the crown and root parts. If the fracture line spans through the surface of tooth, then those fractures are known as uncomplicated tooth fractures. Additionally, if the fracture line spans throughout the whole tooth, involving the pulp, then it is categorized as a complicated tooth fracture. Crown, crown–root, and root fractures are the common type of injuries to the hard dental tissues and the pulp [
15].
The International Association of Dental Traumatology [
16] has recommended fragment reattachment as the treatment of choice for complicated and uncomplicated crown fractures and as an intermediatory procedure in crown–root fractures. Tooth fragment reattachment treatment is not only the most conservative alternative, but it also has several advantages over several conventional treatments. Multiple reports have shown that reattachment of broken fragments to the leftover tooth structure using various adhesive materials (restorative materials) and procedures is a viable option anytime the fractured fragment is recommended [
17,
18,
19,
20,
21,
22,
23,
24].
In previous research by Ausiello et al. [
25], four 3D models of teeth were computationally restored with different filling materials. Highest stress distributions were observed on the filling lining applied on the teeth surfaces. This particular modelling strategy was found to significantly calculate adverse stresses, distributions, and displacements accurately. In addition to this, the indirect lithium disilicate showed reduced stress values when replaced with lost enamel or dentin. In another work by Ausiello et al. [
26], the influence of a specific ferrule design on the mechanical response of a restored teeth was studied computationally. Micro-CT of a canine tooth was performed to develop a high-fidelic 3D model. The study reported high stresses for the model without a ferrule, whereas the stress was found to be equally distributed with ferrule. The finite element (FE) approach using in silico modeling has quantified dental fractures and reattached teeth that included various adhesive materials [
27,
28,
29,
30,
31]. Recent advancements in finite element model production, such as greater computed tomography image quality, improved segmentation methods, and faster computers, have substantially enhanced the efficiency of finite element modeling [
32]. Finite element analysis (FEA) studies also provide the extra benefits of being cost-effective and accurate [
33]. Thus, using a computer simulation has become a practical and acceptable approach for assessing the stresses and strains produced in complicated structures under variable loading situations. This is crucial for researching inaccessible anatomical locations in vivo and traumas that cannot be examined in situ, therefore forecasting the possible areas of structural collapse [
34,
35]. Although several studies have analyzed the effect of adhesive materials across custom crown–root fractures, no previous research has quantified the effect of these materials across realistic fracture geometries of reattached tooth fragments. Hence, this study aimed to quantify the performance of three different adhesive materials in crown and crown–root fractures using the 3D modelling techniques of FEA. The null hypothesis of this study states that there is no change in the stress and deformation values when the crown and crown–root fractures were reattached using various adhesive materials under masticatory and traumatic loading.
2. Materials and Methods
2.1. Geometrical Modeling
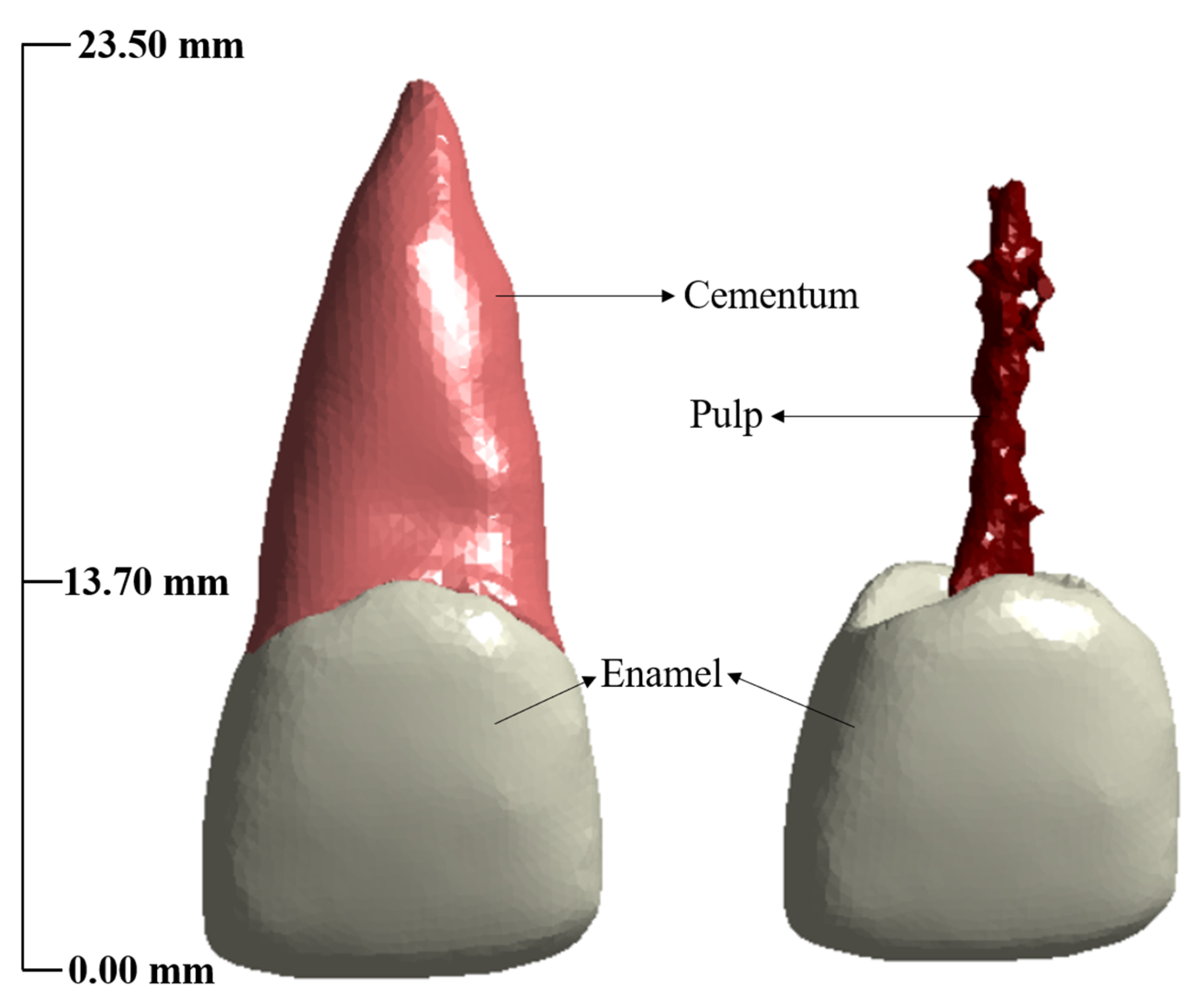
The geometrical 3D model of the permanent maxillary anterior tooth (PMAT) was acquired through cone beam computed tomography (CBCT) scans [
19,
20] from a 25-year-old healthy subject. The CBCT data were then transferred to software (Mimics 24.0, Materialise, Belgium) that employs the DICOM file format, so that the pulp, enamel, and root may be segmented precisely. After segmentation, the permanent maxillary incisor teeth’s 3D triangle-based surfaces were generated using stereo lithography (STL) format. Several constituents used in this study have been shown in
Figure 1. The measurements were consistent with those of the permanent maxillary central incisor tooth, i.e., the distance from the incisal boundary to root was 23.50 mm, and root length from cementoenamel junction to root apex was 13.70 mm [
21].
Two commonly observed crown and crown–root fracture models were applied for the reattached tooth model using a 3D CAD modelling software (Solidworks 2017, Dassault Systèmes, France). To model the fractures, a 25-micron [
22] gap was implemented, which mimicked the fracture line, and was applied with a filler material depicting the luting material. The first realistic fracture model used in this study was a crown fracture based on the previous literature [
23,
24]. Another fracture model was the crown–root fracture, which was generated by modeling a fracture line of 60° from the axis of the tooth and traversed both enamel and root [
25,
26,
27].
Figure 2 represents all the fractures considered in this study.
2.2. Material Model
In the current study, three commonly available adhesive materials, i.e., flowable composite, resin cement, and resin adhesive, were used. The flowable composite consists of a mixture of resin matrix and filler material [
36]. Examples of some commonly used resin matrices involves combination of materials such as Bis-GMA (Bisphenol A dimethacrylate) adduct, Bis-EMA (Bisphenol A polyetheylene glycol diether dimethacrylate) adduct, TEGDMA (Triethyleneglycol dimethacrylate), EBPADMA (ethoxylated Bisphenol A dimethacrylate), and UDMA (urethane dimethacrylate), and filler material includes Ba–F–Al–B–Si–glass nanofiller silica [
36]. Resin cement, along with resin and filler material, also consists of setting accelerators, such as camphor quinone or ethyl 4-dimethylaminobenzoate. Resin adhesives are different in that they are made up of a mixture of resin and a solvent, rather than filler particles [
37]. Examples of commonly used solvent in preparation of resin adhesives include water, ethanol, acetone, or tert-Butanol [
37].
In this analysis, linear and isotropic elastic models were assumed for the healthy and reattached tooth. The values of elastic modulus for the enamel, root, and pulp were considered to be 77.90 GPa, 16.60 GPa, and 6.89E-3 GPa, respectively, based on a previous study [
38]. The corresponding Poisson’s ratio values were 0.3 for enamel and root and 0.45 for the pulp. Similarly, flowable composite, resin cement, and resin adhesive were assumed to have Young’s modulus of 19.70 GPa, 4.92 GPa, and 1 GPa and a Poisson’s ratio of 0.32, 0.27, and 0.24, respectively [
38]. According to the ISO requirements for luting cement, the thickness of the adhesive system was standardized at 25 microns [
39].
2.3. Finite Element (FE) Model
2.3.1. Mesh Convergence Study
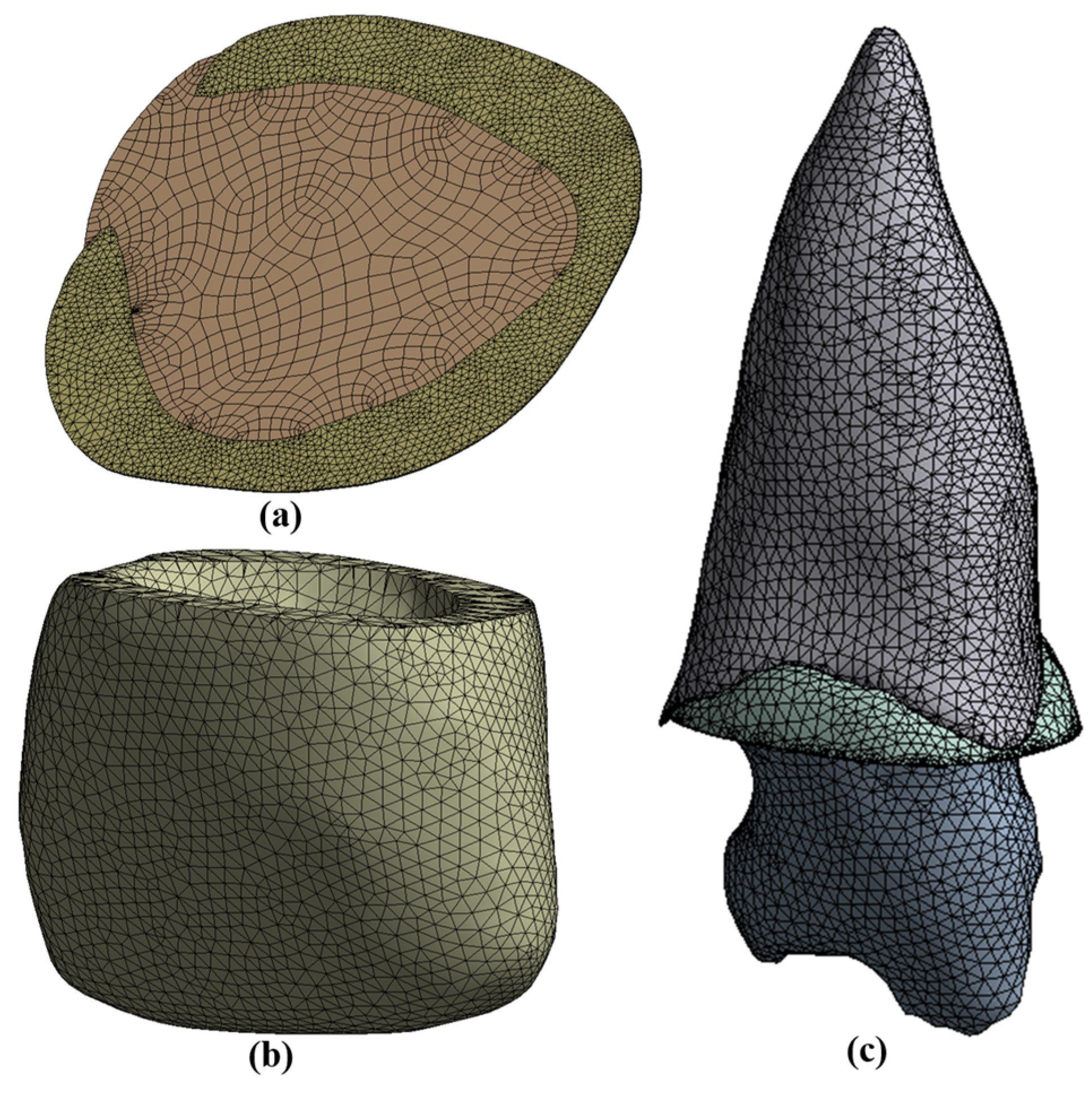
A detailed mesh convergence study was conducted across the healthy tooth model to establish the FE model’s accuracy. Stress and displacement analyses of the healthy and fractured tooth models was performed by using FE software (Ansys 19.0, Ansys Inc., Beltsville, MD, USA). Material properties were applied to the enamel, root, and pulp across three different adhesive materials. The models were meshed with a 20-node Solid 186 element. A contact pair with the characteristics were ‘permanently bonded’, without considering minimal sliding, and a trim tolerance of 0.0016 mm was used between enamel, root, and pulp for the tooth models. Face sizing of enamel and root with sizes ranging from 0.2 mm to 0.6 mm was used to limit the number of meshes. Four different meshes were generated, and the stresses across these models were evaluated. Mesh with a difference in stress values of less than 5% was considered as the optimal mesh. As a result of this mesh convergence exercise, an optimal mesh consisting of 87,471 elements was selected as shown in
Figure 3.
2.3.2. Loads and Constraints
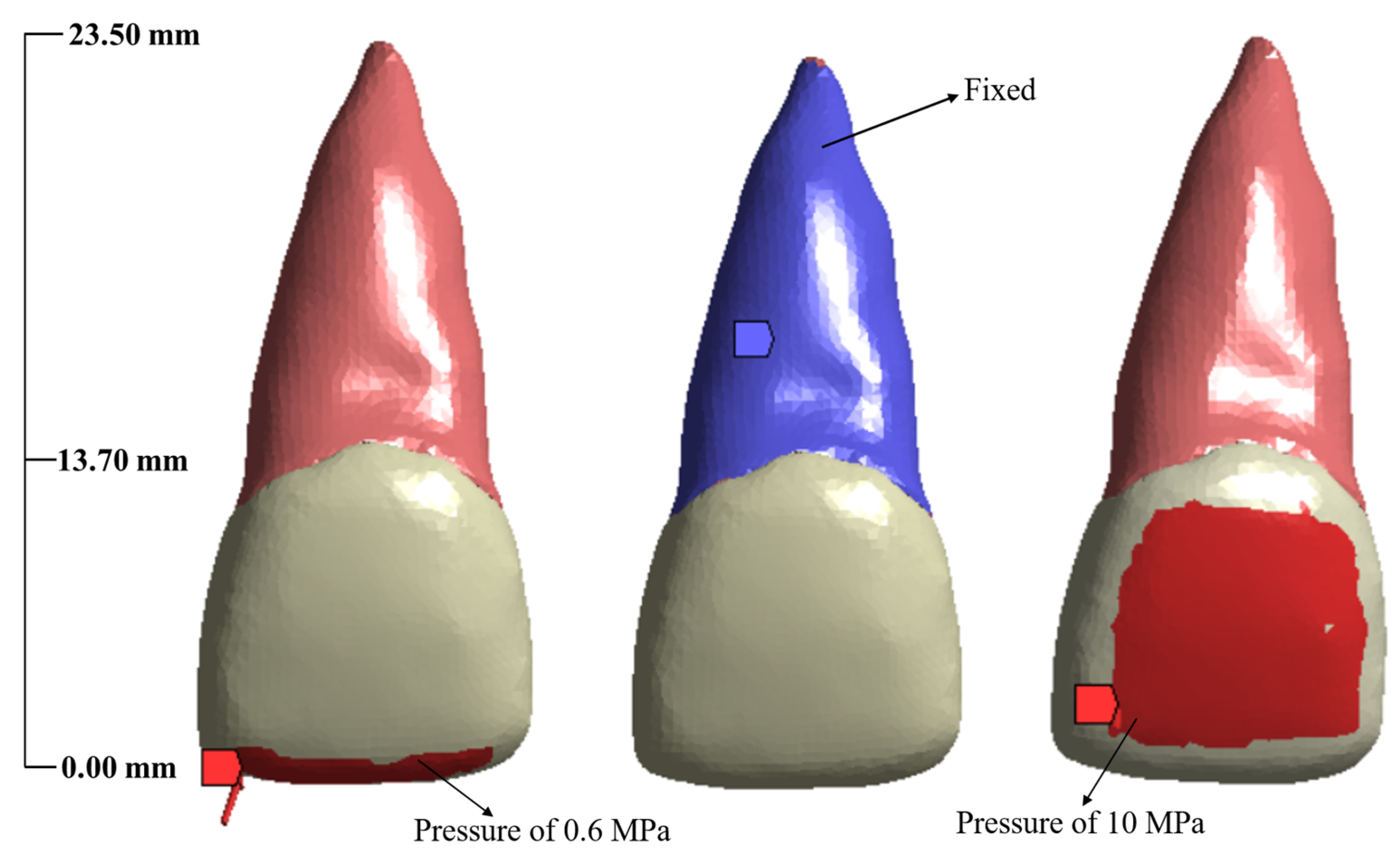
Figure 4 represents all the loads and boundary conditions that is being applied in this study. Due to the prevalence of frontal and incisal injuries [
40], two common types of loads and boundary conditions were implemented (represented in red color). The tooth roots are encased in the periodontium; therefore, the root surface, as a whole, was constrained in all axes (represented in blue color). A load of 0.6 MPa was applied at the incisal edge of both the healthy and reattached tooth to replicate the normal masticatory or incisive load [
41]. In order to simulate the effects of a traumatic load (impact force due to a ball hitting the tooth surface), a 10 MPa of pressure was applied to the centre of the crown of healthy and re-attached tooth models [
41].
2.4. Data Analysis
A detailed statistical analysis was carried out to test the significance of each adhesive material under considered fracture models. A confidence value of 95% was used for the statistical tests. In our work, paired t-test was implemented to ascertain the significant differences amongst the test combinations. Sample size of five observations per class was considered, with total of 12 groups having three variables each summing up to 180 data values. Total of 12 test combinations were tested within 12 groups. These 12 groups were as follows:
- (i)
Displacement, stress, and shear stress values for reattachment of crown fracture using flowable composite under masticatory loading.
- (ii)
Displacement, stress, and shear stress values for reattachment of crown fracture using resin cement under masticatory loading.
- (iii)
Displacement, stress, and shear stress values for reattachment of crown fracture using resin adhesive under masticatory loading.
- (iv)
Displacement, stress, and shear stress values for reattachment of crown fracture using flowable composite under traumatic loading.
- (v)
Displacement, stress, and shear stress values for reattachment of crown fracture using resin Cement under traumatic loading.
- (vi)
Displacement, stress, and shear stress values for reattachment of crown fracture using resin adhesive under traumatic loading.
- (vii)
Displacement, stress, and shear stress values for reattachment of crown–root fracture using flowable composite under masticatory loading.
- (viii)
Displacement, stress, and shear stress values for reattachment of crown–root fracture using resin cement under masticatory loading.
- (ix)
Displacement, stress, and shear stress values for reattachment of crown–root fracture using resin adhesive under masticatory loading.
- (x)
Displacement, stress, and shear stress values for reattachment of crown–root fracture using flowable composite under traumatic loading.
- (xi)
Displacement, stress, and shear stress values for reattachment of crown–root fracture using resin cement under traumatic loading.
- (xii)
Displacement, stress, and shear stress values for reattachment of crown–root fracture using resin adhesive under traumatic loading.
3. Results
3.1. Displacement and Stresses on the Normal Tooth
3.1.1. Masticatory Load
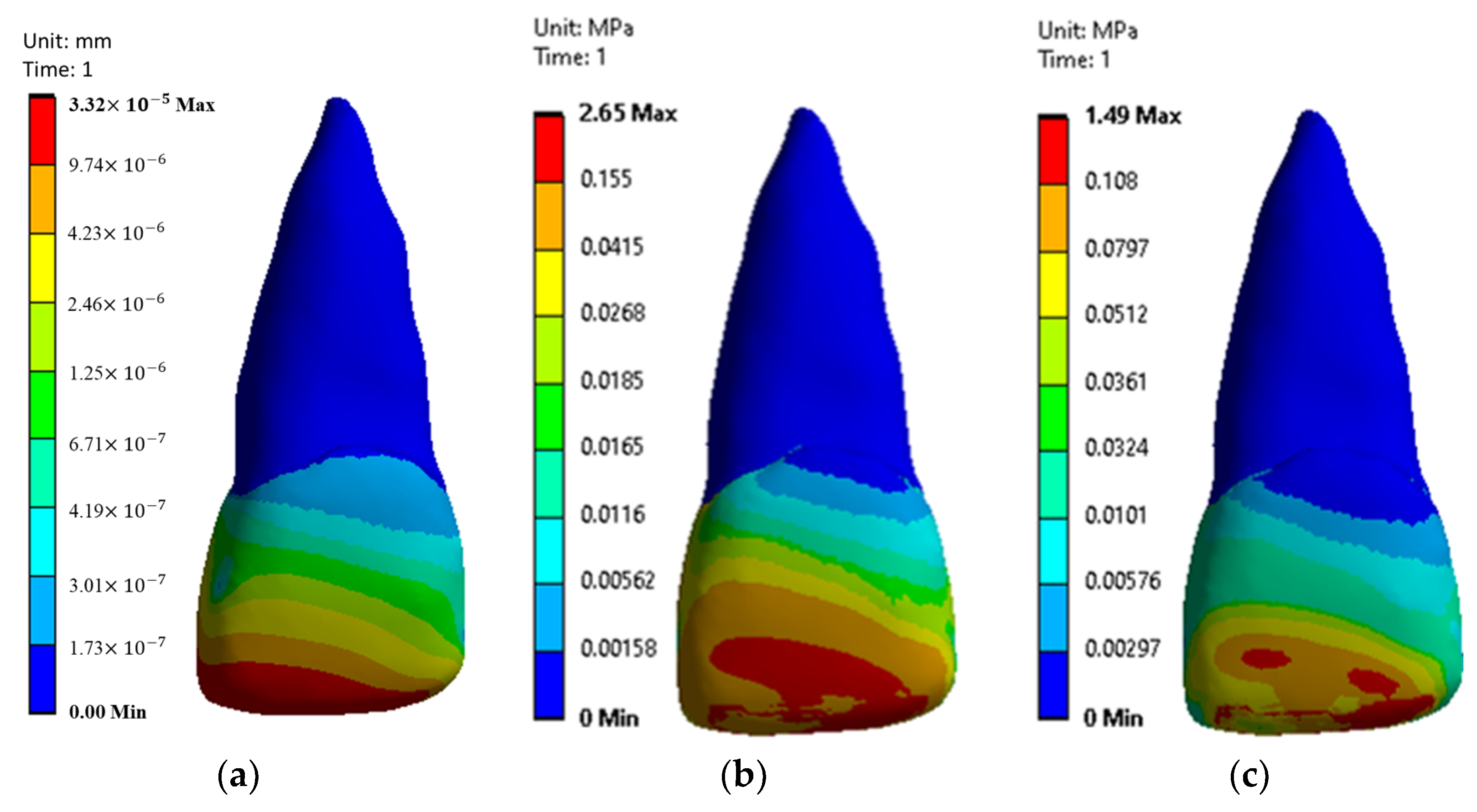
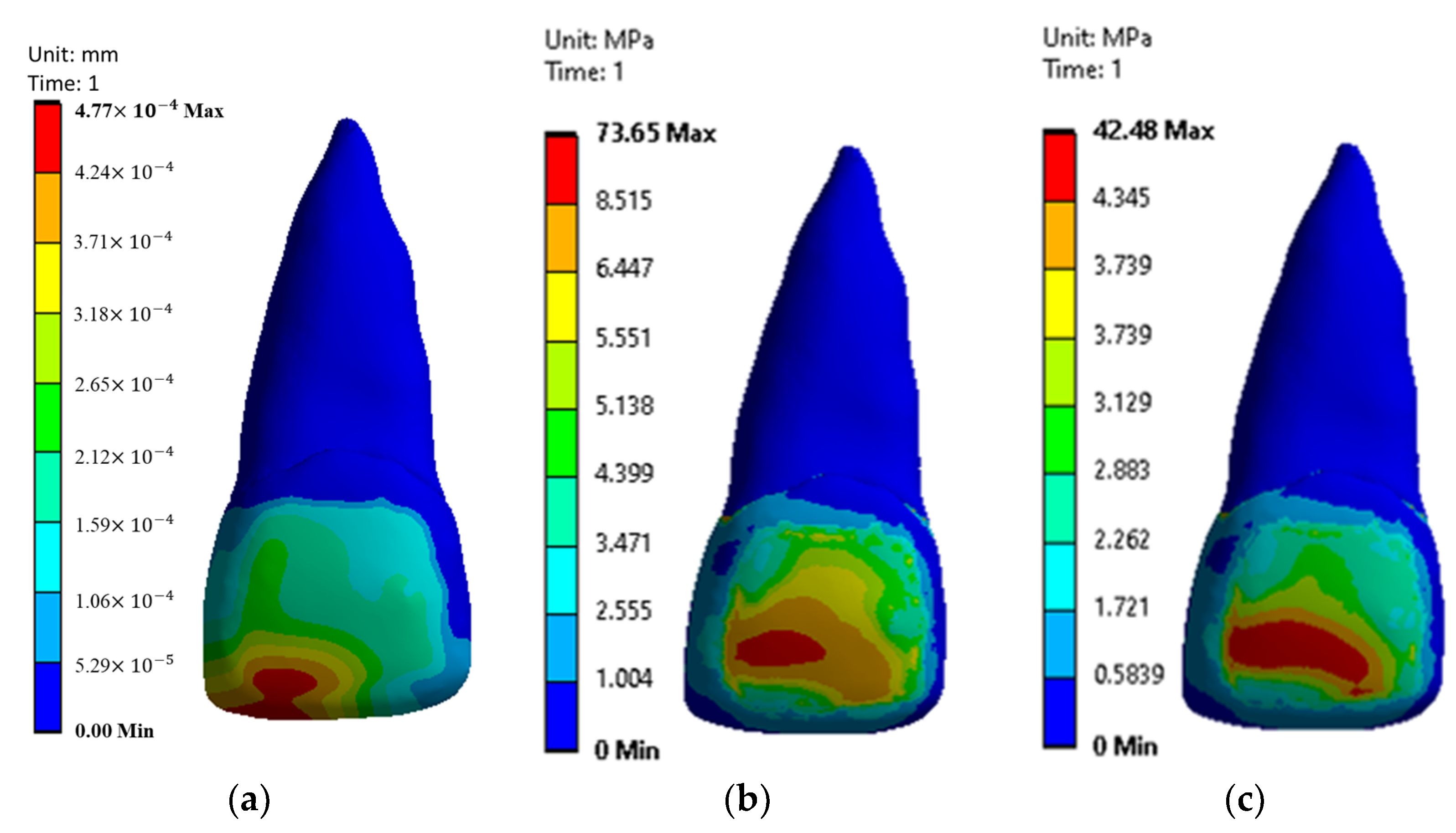
Under masticatory load, the maximum displacement induced in a normal tooth has been represented in
Figure 5a. The maximum displacement was observed at the incisal edge (i.e., under the enamel), which was estimated as 0.0000332
1.66 × 10
−5 mm. The maximum displacement across the enamel started at the incisal edge and decreased as it progressed towards the junction of crown and root. In the case of the root, no significant displacements were observed.
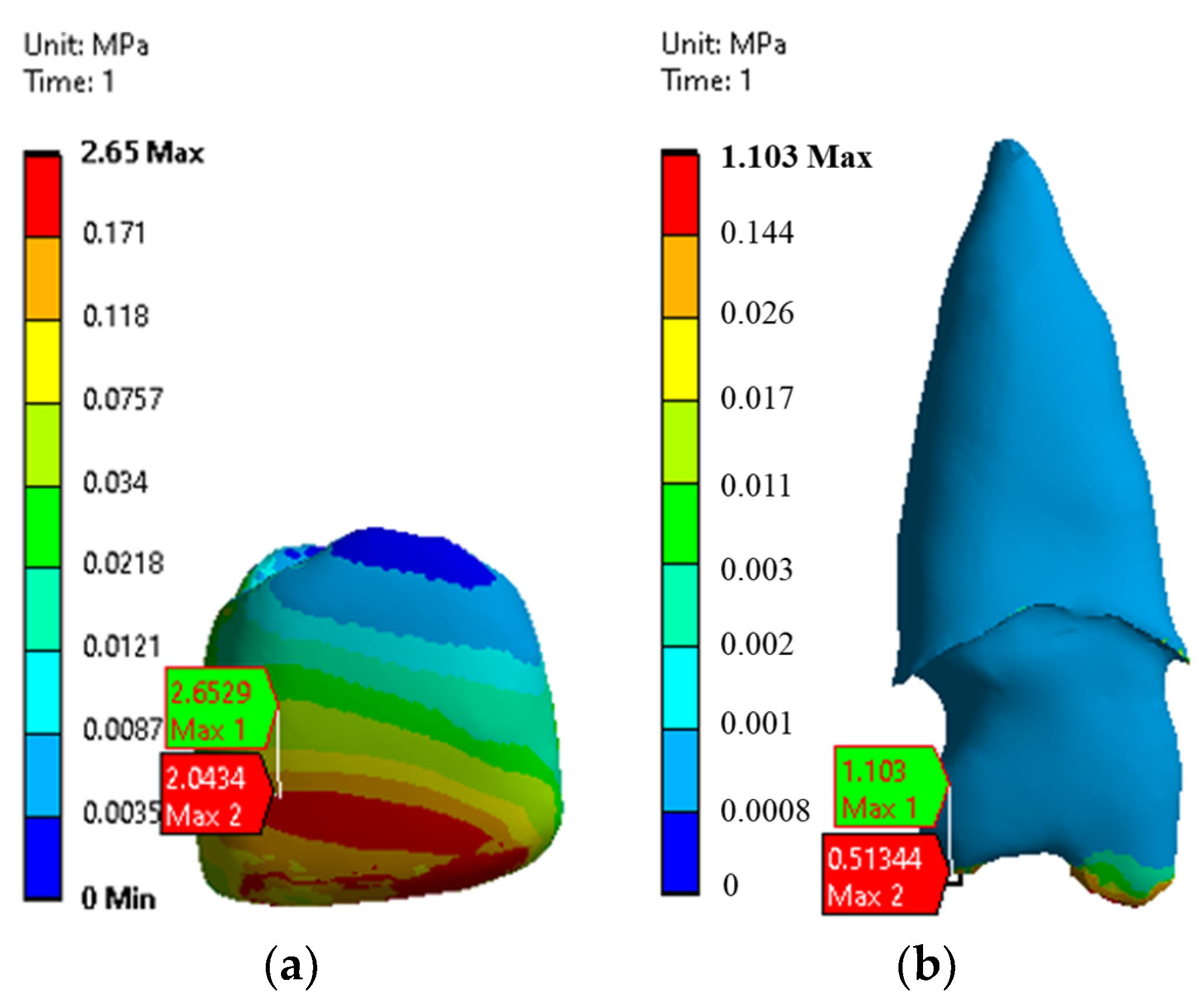
Figure 5b represents the von Mises stress across the healthy tooth. The maximum von-Misses stress observed was 2.65
0.13 MPa (
Figure 6a) at the surface of the enamel. Apart from enamel, the maximum von Mises stress observed was 1.10
0.05 MPa (
Figure 6b) at the base surface of root in contact with the inner part of the cingulum. The second most maximum von Mises stress value observed was 0.51
0.02 MPa at the same location.
Across the enamel geometry, maximum stress was reported at the incisal edge of the crown and minimum was reported near the junction of crown and root. Shear stresses across the healthy tooth with the value of 1.49 0.07 MPa were observed at the lower surface of enamel and root, respectively. Maximum shear stress was observed at the incisal and frontal surfaces of the enamel.
3.1.2. Traumatic Load
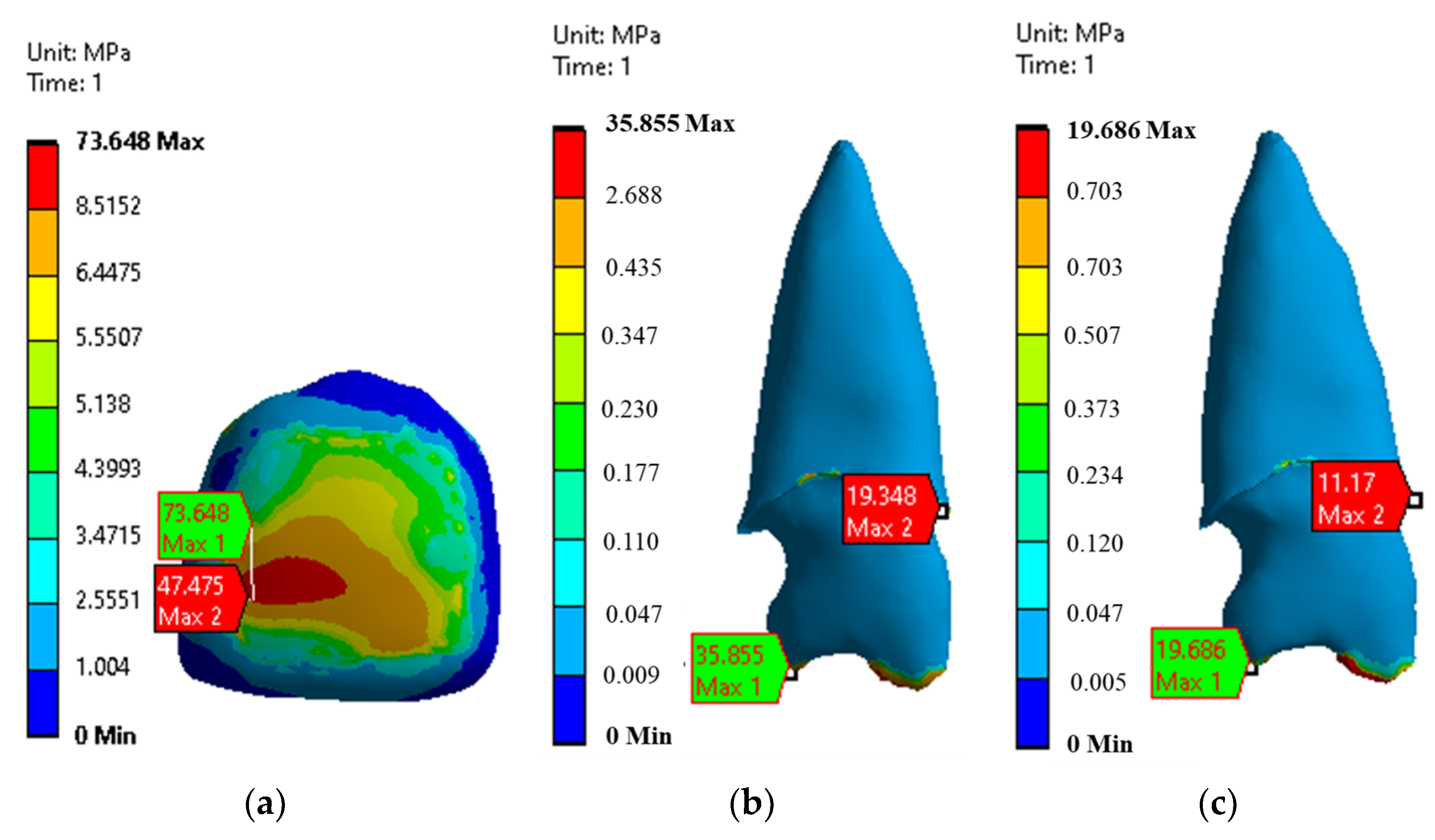
Figure 7a represents the maximum displacement in a healthy central incisor tooth due to traumatic loading. In this case, the maximum displacement was 0.00047
2.35 × 10
−5 mm at the incisal edge of the crown. Significant displacement was not observed at the root surface. Large displacement was observed in the frontal portion of enamel, while little to no changes were observed in the root.
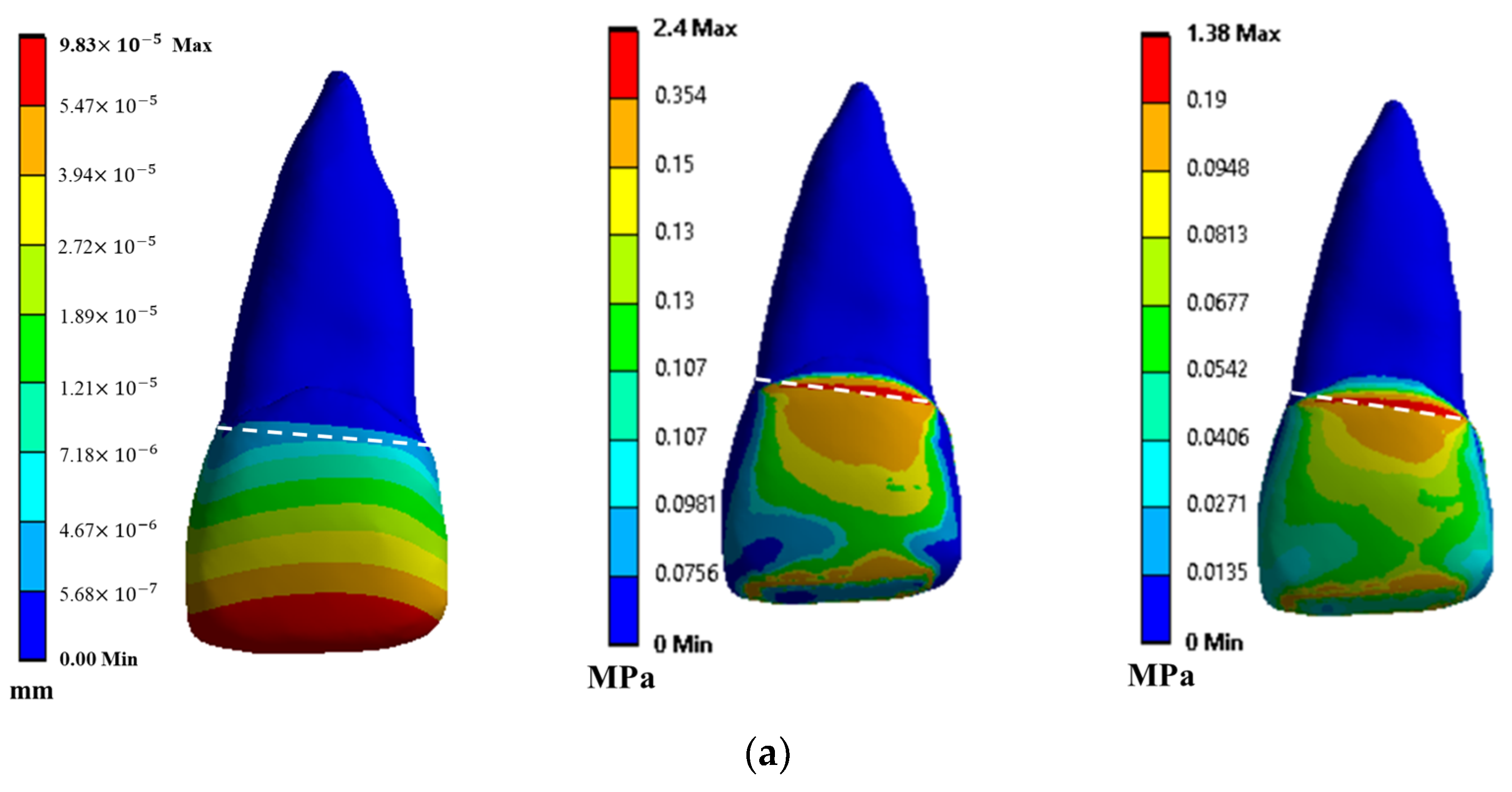
Figure 7b represents the distribution of induced von Mises stress across the tooth geometry in healthy conditions under traumatic loading. Maximum stress was observed at the palatal surface of the tooth in the enamel and the apical portion on the root. The maximum values reported were 35.85
1.79 MPa and 73.648
3.68 MPa for root and enamel, respectively (
Figure 8a,b). In case of dentin, maximum von Mises stress value was observed at the base surface area of dentin, which is in contact with inner surface of cingulum, and the second most maximum von Mises stress value was observed at the cemento–enamel junction with the reduction of almost 48% (
Figure 8b). Maximum shear stress contours across the healthy tooth under traumatic loading are presented in
Figure 7c. For dentin, high shear stress with the value of 19.686
0.98 MPa and 11.17
0.55 MPa was observed on the base of dentin that is covered inside of enamel and cemento–enamel junction, respectively (
Figure 8c).
3.2. Displacement and Stresses on Reattached Tooth with Different Fractures
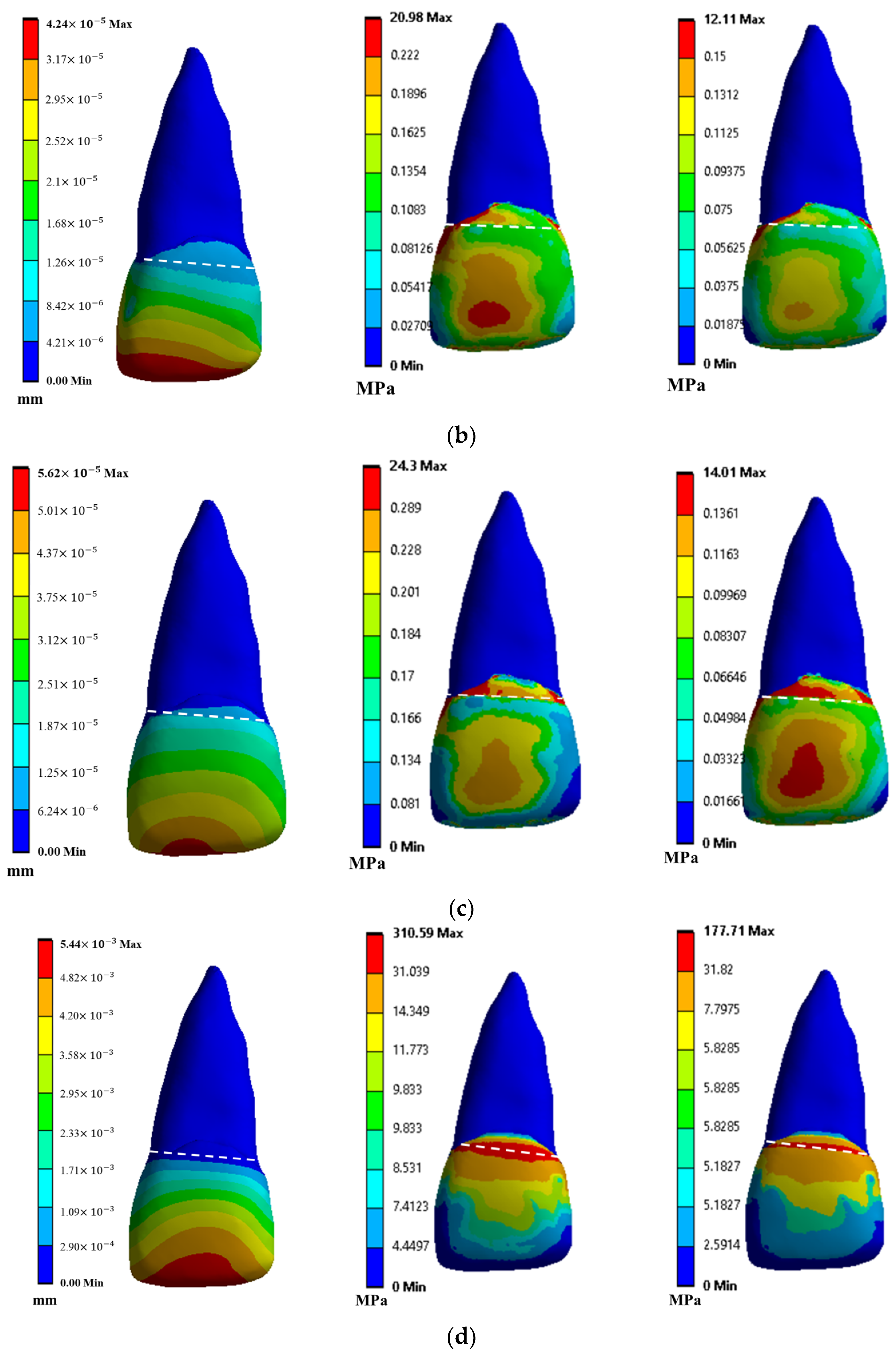
3.2.1. Crown Fracture
In each simulation, the maximum displacement was observed at the incisal edges, as compared to the fracture lines, whereas for stresses, varied locations (i.e., dento-enamel junction and fracture line) were reported. Under masticatory loading, the fragment of crown fracture reattached with flowable composite reported a maximum displacement, maximum stress, and maximum shear stress of 9.83 × 10
−5 0.4925 × 10
−5 mm, 2.4
0.12 MPa, and 1.38
0.069 MPa, respectively (
Figure 9a). The ones reattached with resin cement exhibited a maximum displacement of 4.24 × 10
−5 0.21 × 10
−5 mm, maximum stress of 20.98
1.04 MPa, and the maximum shear stress of 12.11
0.60 MPa (
Figure 9b). The fragments reattached with resin adhesive showed a maximum displacement of 5.62 × 10
−5 0.28 × 10
−5 mm, the maximum stress of 24.3
1.21 MPa, and maximum shear stress of 14.01
0.70 MPa under masticatory load (
Figure 9c).
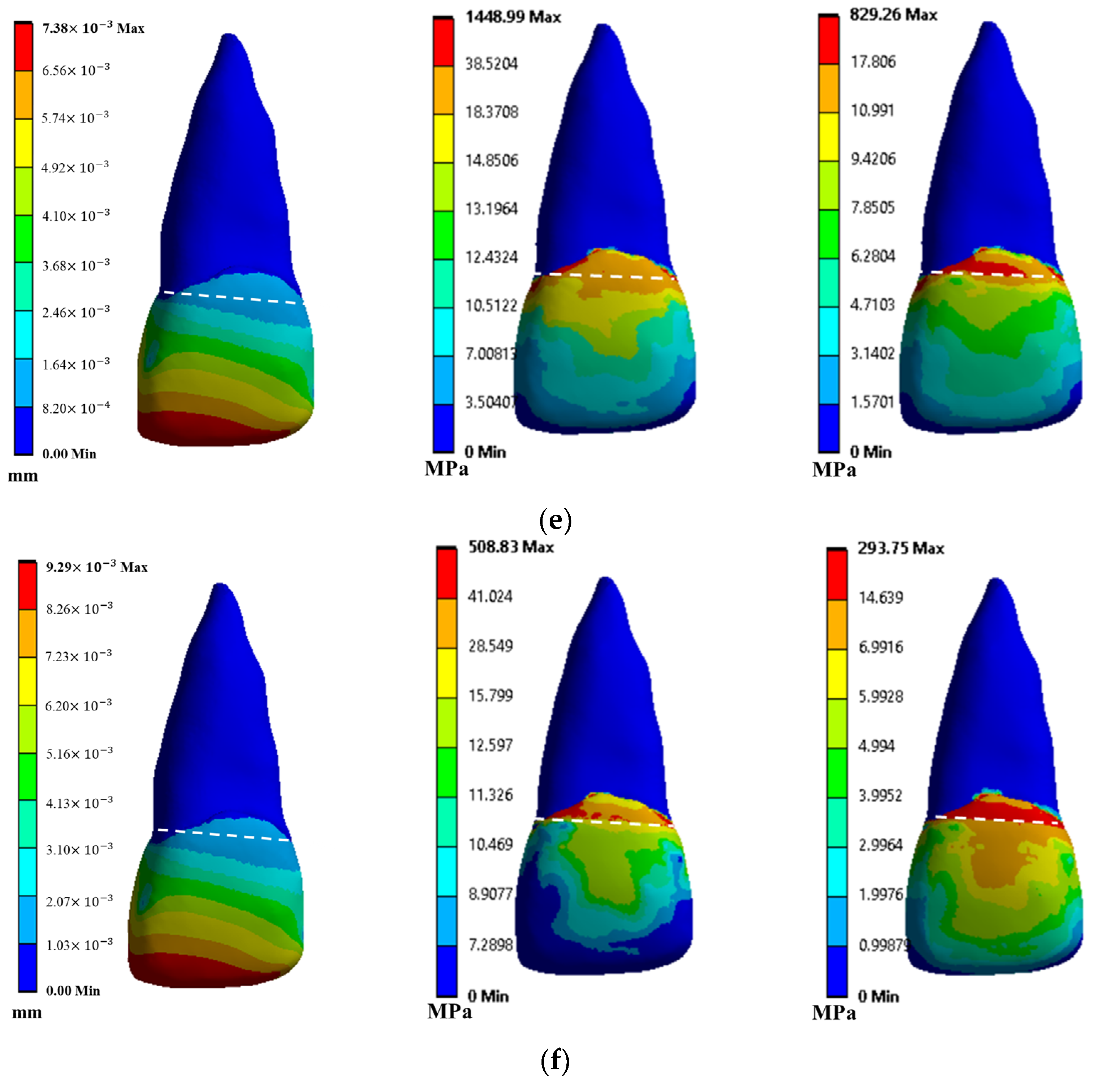
Under traumatic loading, the fragments reattached with flowable composite demonstrated maximum displacement, von Mises stress and shear stress values of 5.44 × 10
−3 0.27 × 10
−3 mm, 310.59
15.52 MPa, and 177.71
8.88 MPa respectively (
Figure 9d). In the fragments reattached with resin cement, maximum displacement, von Mises stress, and shear stress were found to be 7.38 × 10
−4 0.36 × 10
−4 mm, 1448.99
72.44 MPa, and 829.26
41.46 MPa, respectively (
Figure 9e). While the fragments reattached with resin adhesive showed maximum displacement, von Mises stress, and shear stress values of 9.29 × 10
−3 0.46 × 10
−3 mm, 509
25.45 MPa, and 293.75
14.68 MPa, respectively (
Figure 9f).
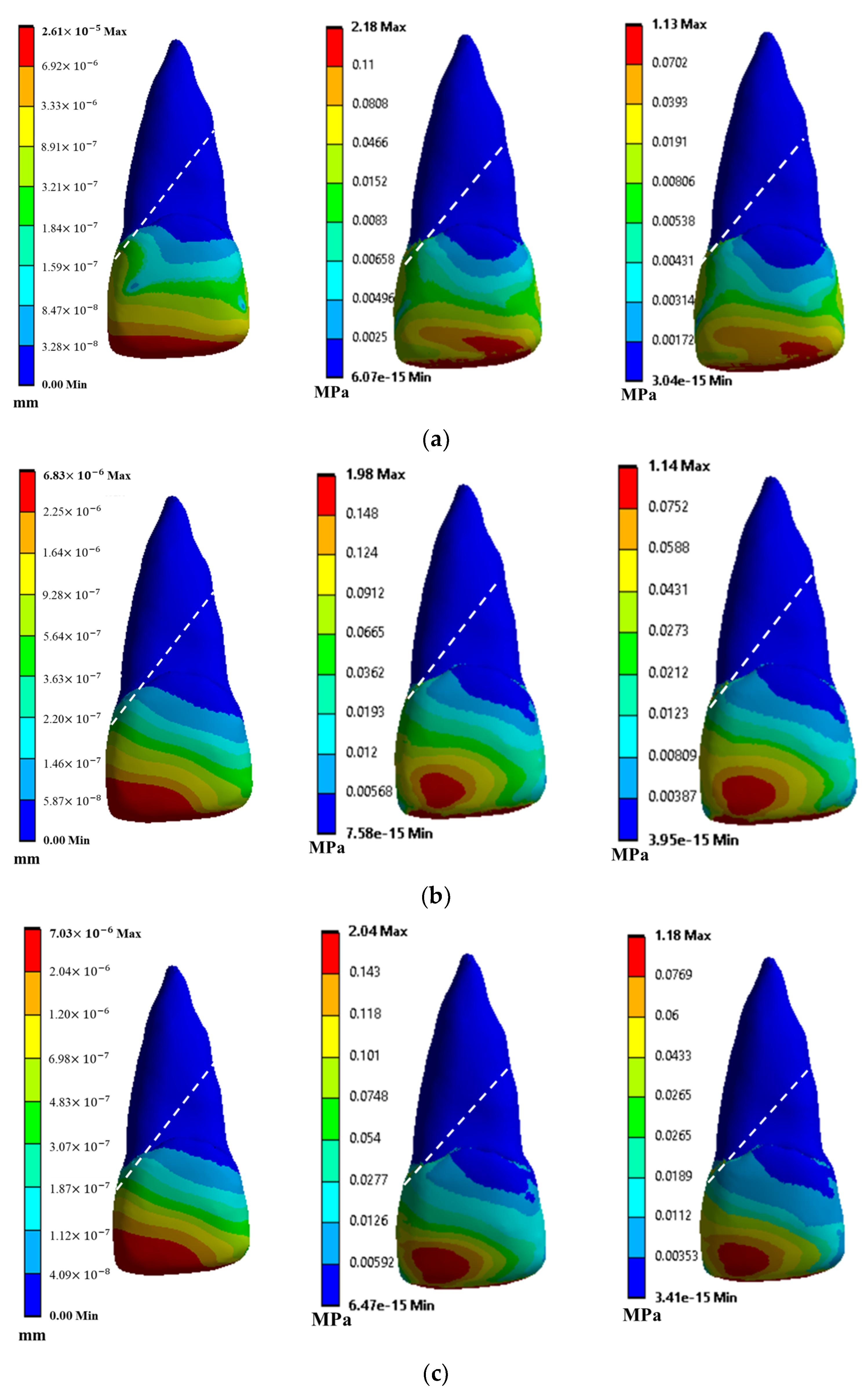
3.2.2. Crown–Root Fracture
Fragments of tooth with crown–root fracture, reattached with a flowable composite, displayed the maximum displacement of 2.61 × 10
−5 0.13 × 10
−5 mm, maximum stress of 2.18
0.10 MPa, and maximum shear stress of 1.13
0.05 MPa (
Figure 10a), under the masticatory loading. Similar fracture model reattached with the resin cement reported the maximum displacement of 6.83 × 10
−6 0.34 × 10
−6 mm, maximum stress of 1.98
0.09 MPa, and maximum shear stress of 1.14
0.05 MPa (
Figure 10b). The fracture model reattached with resin adhesive material displayed a maximum displacement of 7.03 × 10
−5 0.35 × 10
−5 mm, a maximum von Mises stress of 2.04
0.10 MPa, and a maximum shear stress of 1.18
0.05 MPa (
Figure 10c).
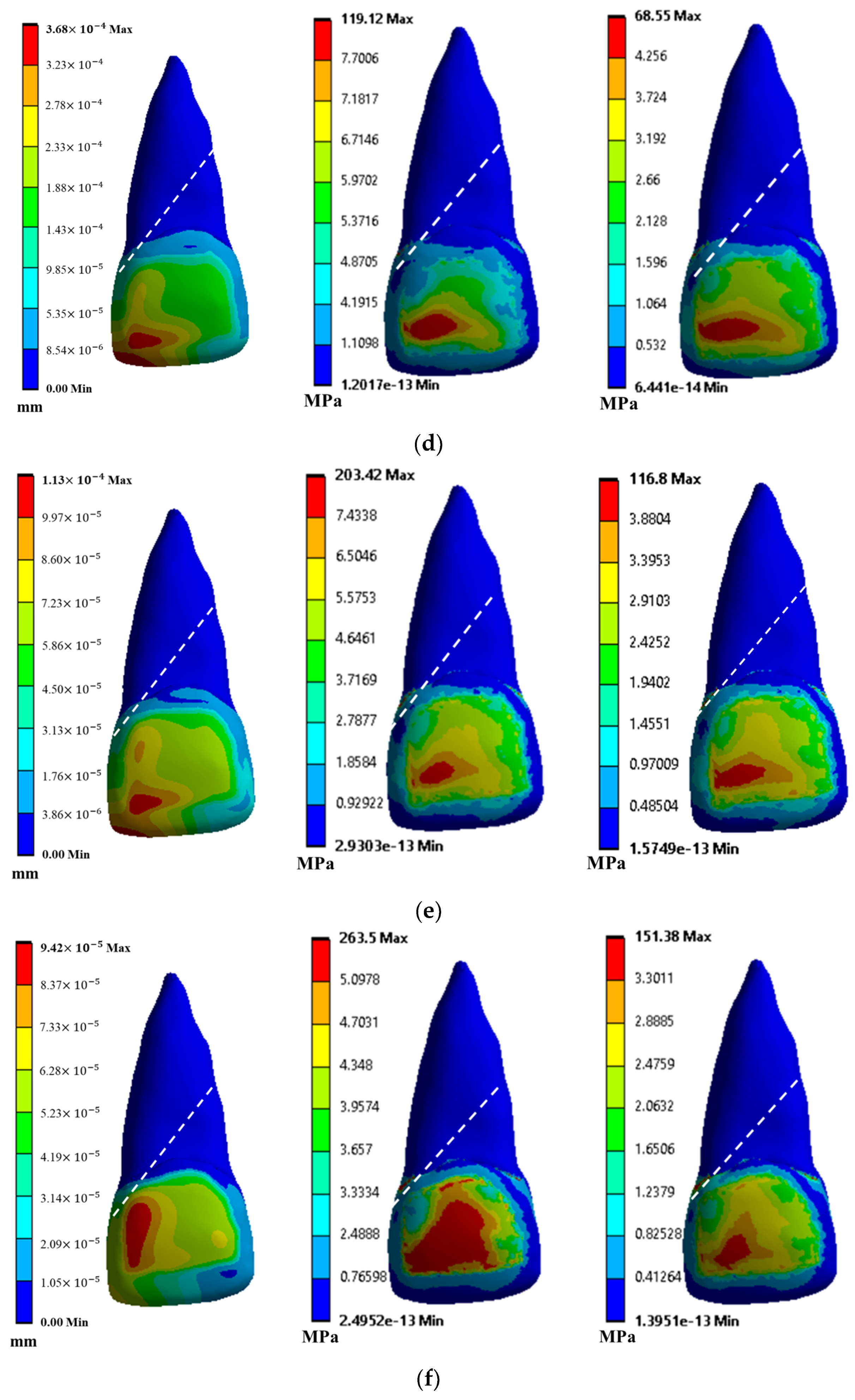
Under the traumatic loading after the application of flowable composite as an adhesive material, the displacement, induced von Mises stresses, and the shear stress were found to be 3.68 × 10
−4 0.18 × 10
−4 mm, 119.12
5.95 MPa, and 68.55
3.42 MPa, respectively (
Figure 10d). Application of resin cement as a filler material resulted in the maximum displacement, maximum stress, and maximum shear stress of 1.13 × 10
−4 0.05 × 10
−4 mm, 203.42
10.17 MPa, and 116.8
5.84 MPa, respectively (
Figure 10e). Further, the stress value of such fragments was significantly higher when reattached with resin cement than its shear modulus. Additionally, the models with resin adhesive as a filler material reported the maximum displacement of 9.42 × 10
−5 0.47 × 10
−5 mm, maximum von Mises stress of 264
13.20 MPa, and maximum shear stress of 151.38
7.56 MPa, mostly at the labio-incisal edge (
Figure 10f).
3.3. Effect of Adhesive Materials and Varying Loads on the Reattached Tooth
3.3.1. Statistical Comparison
All the statistical analysis was carried out with three test combinations across the crown fracture and crown–root fracture under both types of loading. These test combinations were as follows:
- (i)
Flowable composite with resin cement;
- (ii)
Resin cement with resin adhesive;
- (iii)
Resin adhesive with flowable composite.
Therefore, twelve test combinations were created to test the statistical significance of this study.
Effect of Adhesive Material across Crown Fracture under Masticatory Loading
For the crown fracture under masticatory loading, the comparison between the displacements of tooth reattached with flowable composite and resin cement showed no significant difference and were found to be statistically similar (i.e., p < 0.5). Comparing resin cement and resin adhesive, as well as the resin adhesive with flowable composite, also showed no significant differences, with p-values of less than 0.09 and 0.1, respectively. On the other hand, the comparison between the von Mises stresses of teeth reattached with flowable composite, resin cement, and resin adhesive, a significant difference (i.e., p < 0.01) was reported. In these test combinations, flowable composite showed low stress values. Similar observations were reported for shear stress values.
Effect of Adhesive Material across Crown–Root Fracture under Masticatory Loading
For crown–root fracture under masticatory loading, the comparison between the displacements of tooth reattached with flowable composite and resin cement showed no significant difference, and they were found to be statistically similar (i.e., p < 0.1). Comparing resin cement and resin adhesive, as well as resin adhesive with flowable composite, also showed no significant differences, with similar p-values. On the other hand, the comparison between the von Mises stresses of teeth reattached with flowable composite, resin cement, and resin adhesive, a significant difference (i.e., p < 0.001) was reported. In these test combinations, resin cement showed low stress values. Similar to previous case, similar observations were reported for shear stress values.
Effect of Adhesive Material across Crown Fracture under Traumatic Loading
For the crown–root fracture under masticatory loading, the comparison between the displacements of tooth reattached with flowable composite and resin cement showed no significant differences and were found to be statistically similar (i.e., p < 0.1). Comparing the resin cement and resin adhesive, as well as the resin adhesive with flowable composite, also showed no significant differences, with similar p-values. On the other hand, comparison between the von Mises stresses of tooth reattached with flowable composite, resin cement, and resin adhesive, significant difference (i.e., p < 0.001) was reported. In these test combinations resin cement showed low stress values. Similar to previous case, similar observations were reported for shear stress values.
Effect of Adhesive Material across Crown–Root Fracture under Traumatic Loading
For the crown fracture under traumatic loading, the comparison between the displacements of the teeth reattached with flowable composite and resin cement showed significant differences, and they were found to be statistically different (i.e., p < 0.02). Flowable composite was found to produce the lowest displacement amongst all the test cases. On the other hand, the comparison between the von Mises and shear stresses of teeth reattached with flowable composite, resin cement, and resin adhesive were similar, as compared to masticatory loading, where resin cement showed low stress values.
3.3.2. Summary of Comparison between Each Group
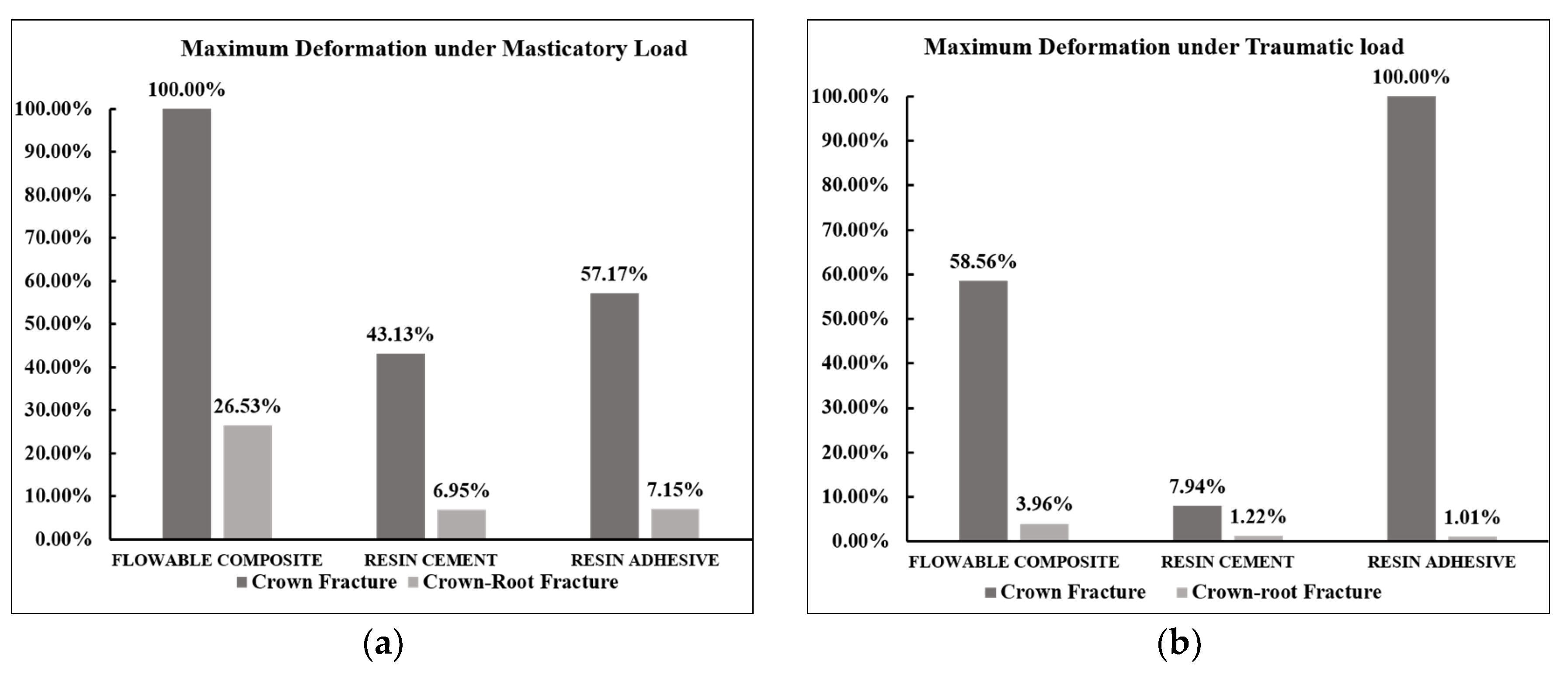
Figure 11 represents the comparison between displacement, von Mises stress, and shear stress values across reattached fragments of tooth with crown and crown–root fractures using different restorative material. It was found that fragments of crown-fractured teeth reattached using flowable composite shows maximum displacement across all adhesive material under masticatory load (
Figure 11a). Fragments of crown–root fractured tooth shows very low values of displacement when reattached using resin cement, resin adhesive which was 6.9% and 7.2% respectively as compared to maximum displacement value across reattached crown-fractured tooth (
Figure 11a). In case of masticatory loading, fragments with crown fracture and crown–root fracture reattached using flowable composite shows maximum displacement followed by resin adhesive and resin cement. Minimum displacement was observed when fragments of fractured tooth reattached using resin adhesive under masticatory load in both cases. Fragments with crown fracture and reattached with resin adhesive shows displacement value of 57.2% and 7.2% respectively as compared displacement value of crown-fractured tooth reattached using flowable composite under masticatory load.
As contrary to masticatory load,
Figure 11b depicts the maximum displacement value when fragments with crown fracture reattached using resin adhesive and crown–root-fractured tooth reattached using flowable composite under traumatic load. In case of fragments with crown fracture, maximum displacement was observed when reattached using resin adhesive, followed by flowable composite which is 58.6% of maxi-mum displacement value under traumatic load. As compared to crown fracture, fragments with crown–root fracture reattached using resin adhesive and resin cement shows much lower displacement value which was 1% and 1.2% respectively as compared to maximum displacement value which was observed in case crown fracture reattached using resin adhesive under traumatic load (
Figure 11b).
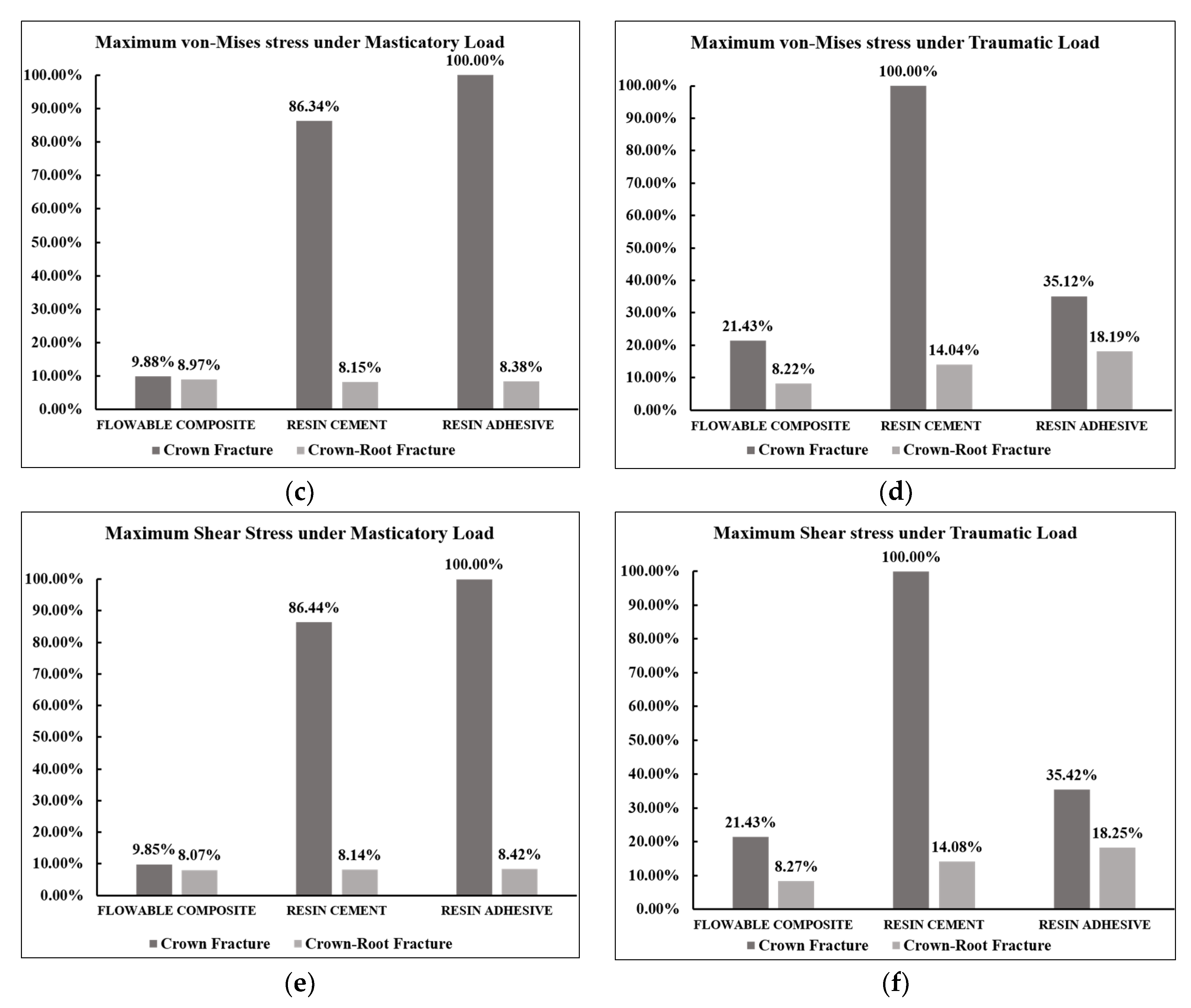
Figure 11c,e shows similar trend values for von Mises stress and shear stress for both fractured tooth models under masticatory load. A similar trend in values was observed under traumatic load (
Figure 11d,e). Maximum von Mises and shear stress values were observed when fragments with crown fracture reattached using resin adhesive, followed by resin cement and flowable composite, which were 86.3% and 9.9%, respectively, of the maximum value under masticatory load. In the case of fragments with crown–root fracture, the same reattached with resin adhesive, resin cement, shows much lower von Mises stress and shear stress values, which was about 8.4% and 8.1%, respectively, as compared to the maximum stress value observed when the crown-fractured tooth was reattached using resin adhesive.
4. Discussion
This research employs computational modelling to examine the strength of three different adhesive materials used for reattaching frequently encountered crown and crown–root dental fractures. The CBCT imaging data were utilized, a full-scale model of the maxillary central incisor was created, and three different adhesive material fillings were simulated for commonly occurring fractures through novel numerical cutting and filling operations and were subjected to masticatory and traumatic loadings. The observed results showed significant variations in the stress values of the fragments reattached with these materials. It was observed that no material can be universally employed for reattachment of the frequently encountered teeth with crown and crown–root fractures.
Studies have shown that the type of restorative material used for fragment reattachment will influence fracture strength [
42,
43,
44]. In a flowable composite, resin is a type of polymer that provides adhesive properties to the material, whereas the filler material provides strength and durability to the composite [
36]. Resin cement consists of both resin and filler material, along with that, it also consists of setting accelerator that helps the material to set quickly [
45]. Resin adhesives are different in that they are made up of a mixture of resin and a solvent, rather than filler particles [
37].
It was observed that the maximum stress value of 2.65 MPa, due to masticatory load, was less than the compressive stress limits of the enamel (38 MPa) and root (163 MPa). Thus, the masticatory stresses are easily handled by a healthy maxillary central incisor. Likewise, the maximum shear stress of 1.49 MPa suggests that a healthy maxillary central incisor tooth can withstand the biting pressures, as well [
30]. It was observed that the fracture line close to the cemento–dentin junction must be handled with caution, since larger stresses were recorded at this location. Analyzing the significant and insignificant differences amongst all the test combinations, certain adhesive materials showed enhanced performances, as compared to others. For crown fracture, under masticatory loading, the application of adhesive materials showed an insignificant difference, where all the materials showed statistically similar displacements. Hence, no conclusion can be drawn to ascertain the best performing material for minimal displacements.
On the other hand, under masticatory loading, flowable composite showed statistically significant differences, along with the lowest induced stresses. For crown–root fractures re-attached with adhesive materials and subjected to masticatory loading, resin cement showed significantly lower stress values. Under traumatic loading, across both the fractures, resin cement showed significantly lower displacements and stress values. Additionally, for crown–root fractures, high stresses were not observed at the fracture line, and instead, they were observed on the enamel. This could be due to the complex tooth geometries, which consisted of several areas where high stress concentration could be anticipated.
Concerning their shear strength, the crown–root-fractured teeth exhibited low stress values, with all the materials under masticatory load and significantly high stress values during traumatic load. The shear stress values in reattached crown–root fractures subjected to masticatory loading with all adhesive materials did not vary significantly. However, the stress value for the same material under a traumatic load varies significantly amongst the three materials. Actual experiments were not performed in our work, but our consideration of CBCT for the tooth scanning, finite element model, replication of actual fracture geometries, and statistical analysis tried to ensure accurate outcomes, so that the best material could be selected for a certain type of fracture.
5. Conclusions
The novelty of the current work was to evaluate the performances of commonly available adhesive materials, while considering the actual fracture path line on a scanned tooth. This modelling procedure, along with the testing framework, has never been explored in the past, as per the best of our knowledge.
In conclusion, this kind of detailed research on how different adhesive materials affect reattached fractured teeth has not been conducted to date, as per the best of our knowledge. Flowable composite showed the lowest induced stresses for crown fracture under masticatory loading. Under the same loading conditions, crown–root fracture re-attached using resin cement showed significantly lower stress values. While, across both the fractures, resin cement showed significantly lower displacements and stress values under traumatic loading. Therefore, the null hypothesis was rejected. These novel findings can help dentists select an appropriate kind of adhesive material for their patients. The modelling techniques presented in this research could also help researchers or scientists to test newer adhesive materials for the re-attachment of teeth to protect them from further trauma.
Author Contributions
Conceptualization, S.G., N.T. and A.C.; methodology, A.G., S.G., S.S., N.T. and A.C.; software, A.G., S.G. and A.C.; validation, A.G., S.G., S.S., N.T. and A.C.; formal analysis, S.S., N.T. and A.C.; investigation, S.G., S.S., N.T. and A.C.; data curation, A.G., S.G. and A.C.; writing—original draft preparation, A.G. and S.G.; writing—review and editing, A.G., S.G., N.T. and A.C.; supervision, A.C. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by IITD-AIIMS MFIRP Grant, 2022.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available, due to the large dataset, but are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dua, R.; Sharma, S. Prevalence, causes, and correlates of traumatic dental injuries among seven-to-twelve-year-old school children in Dera Bassi. Contemp. Clin. Dent. 2012, 3, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O. Etiology and pathogenesis of traumatic dental injuries A clinical study of 1,298 cases. Eur. J. Oral Sci. 1970, 78, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Andreasen, F.M.; Andersson, L. Textbook and Color Atlas of Traumatic Injuries to the Teeth. Stomatol. EDU J. 2019, 6, 279. [Google Scholar] [CrossRef]
- Sanaei-Rad, P.; Hajihassani, N.; Jamshidi, D. Management of a complex traumatic dental injury: Crown, crown-root, and root fracture. Clin. Case Rep. 2020, 8, 2504–2509. [Google Scholar] [CrossRef]
- Agouropoulos, A.; Pavlou, N.; Kotsanti, M.; Gourtsogianni, S.; Tzanetakis, G.; Gizani, S. A 5-year data report of traumatic dental injuries in children and adolescents from a major dental trauma center in Greece. Dent. Traumatol. 2021, 37, 631–638. [Google Scholar] [CrossRef]
- Petti, S.; Glendor, U.; Andersson, L. World traumatic dental injury prevalence and incidence, a meta-analysis-One billion living people have had traumatic dental injuries. Dent. Traumatol. 2018, 34, 71–86. [Google Scholar] [CrossRef] [Green Version]
- Patnana, A.K.; Vanga, N.R.V.; Vabbalareddy, R.; Chandrabhatla, S.K. Evaluating the fracture resistance of fiber reinforced composite restorations—An in vitro analysis. Indian J. Dent. Res. 2020, 31, 138–144. [Google Scholar] [CrossRef]
- Tewari, N.; Bansal, K.; Mathur, V.P. Dental Trauma in Children: A Quick Overview on Management. Indian J. Pediatr. 2019, 86, 1043–1047. [Google Scholar] [CrossRef]
- Sun, L.; Wu, X.; Li, Y.; Lin, Z.; Xu, D.; Lin, X.; Gao, Y. Comparative analysis of the stress distribution in five anatomical types of maxillary central incisor. Technol. Health Care 2017, 25, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Stanford, J.W.; Weigel, K.V.; Paffenbarger, G.C.; Sweeney, W. Compressive properties of hard tooth tissues and some restorative materials. J. Am. Dent. Assoc. 1960, 60, 746–756. [Google Scholar] [CrossRef]
- Craig, R.G.; Peyton, F.A.; Johnson, D.W. Compressive Properties of Enamel, Dental Cements, and Gold. J. Dent. Res. 1961, 40, 936–945. [Google Scholar] [CrossRef]
- He, L.H.; Fujisawa, N.; Swain, M.V. Elastic modulus and stress–strain response of human enamel by nano-indentation. Biomaterials 2006, 27, 4388–4398. [Google Scholar] [CrossRef]
- Roy, S.; Basu, B. Mechanical and tribological characterization of human tooth. Mater. Charact. 2008, 59, 747–756. [Google Scholar] [CrossRef]
- Ziskind, D.; Hasday, M.; Cohen, S.R.; Wagner, H.D. Young’s modulus of peritubular and intertubular human dentin by nano-indentation tests. J. Struct. Biol. 2011, 174, 23–30. [Google Scholar] [CrossRef]
- Bhanderi, S. Facts About Cracks in Teeth. Prim. Dent. J. 2021, 10, 20–27. [Google Scholar] [CrossRef]
- DiAngelis, A.J.; Andreasen, J.O.; Ebeleseder, K.A.; Kenny, D.J.; Trope, M.; Sigurdsson, A.; Andersson, L.; Bourguignon, C.; Flores, M.T.; Hicks, M.L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent. Traumatol. 2012, 28, 2–12. [Google Scholar] [CrossRef]
- Badami, A.A.; Dunne, S.M.; Scheer, B. An in vitro investigation into the shear bond strengths of two dentine-bonding agents used in the reattachment of incisal edge fragments. Endod. Dent. Traumatol. 1995, 11, 129–135. [Google Scholar] [CrossRef]
- Demarco, F.; Fay, R.-M.; Pinzon, L.M.; Powers, J.M. Fracture resistance of re-attached coronal fragments—Influence of different adhesive materials and bevel preparation. Dent. Traumatol. 2004, 20, 157–163. [Google Scholar] [CrossRef]
- Andreasen, F.M.; Norén, J.G.; Andreasen, J.O.; Engelhardtsen, S.; Lindh-Strömberg, U. Long-term survival of fragment bonding in the treatment of fractured crowns: A multicenter clinical study. Quintessence Int. 1995, 26, 669–681. [Google Scholar]
- Andreasen, F.M.; Steinhardt, U.; Bllle, M.; Munksgaard, E.C. Bonding of enamel-dentin crown fragments after crown fracture. An experimental study using bonding agents. Endod. Dent. Traumatol. 1993, 9, 111–114. [Google Scholar] [CrossRef]
- Bruschi-Alonso, R.C.; Alonso, R.C.B.; Correr, G.M.; Alves, M.C.; Lewgoy, H.R.; Sinhoreti, M.A.C.; Puppin-Rontani, R.M.; Correr-Sobrinho, L. Reattachment of anterior fractured teeth: Effect of materials and techniques on impact strength. Dent. Traumatol. 2010, 26, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, P.; Srinivasan, S.; Arul, B.; Natanasabapathy, V. Fragment reattachment after complicated crown-root fractures of anterior teeth: A systematic review. Dent. Traumatol. 2020, 37, 37–52. [Google Scholar] [CrossRef] [PubMed]
- de Las Casas, E.B.; Cornacchia, T.P.M.; Gouvêa, P.H.; Cimini, C.A. Abfraction and Anisotropy--Effects of Prism Orientation on Stress Distribution. Comput. Methods Biomech. Biomed. Eng. 2003, 6, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Garcia, F.C.P.; Poubel, D.L.N.; Almeida, J.C.F.; Toledo, I.P.; Poi, W.R.; Guerra, E.N.S.; Rezende, L.V.M.L. Tooth fragment reattachment techniques-A systematic review. Dent. Traumatol. 2018, 34, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ausiello, P.; Ciaramella, S.; Martorelli, M.; Lanzotti, A.; Gloria, A.; Watts, D.C. CAD-FE modeling and analysis of class II restorations incorporating resin-composite, glass ionomer and glass ceramic materials. Dent. Mater. 2017, 33, 1456–1465. [Google Scholar] [CrossRef] [Green Version]
- Ausiello, P.; Ciaramella, S.; Martorelli, M.; Lanzotti, A.; Zarone, F.; Watts, D.C.; Gloria, A. Mechanical behavior of endodontically restored canine teeth: Effects of ferrule, post material and shape. Dent. Mater. 2017, 33, 1466–1472. [Google Scholar] [CrossRef] [Green Version]
- Oladapo, B.; Zahedi, S.A.; Vahidnia, F.; Ikumapayi, O.; Farooq, M.U. Three-dimensional finite element analysis of a porcelain crowned tooth. Beni-Suef Univ. J. Basic Appl. Sci. 2018, 7, 461–464. [Google Scholar] [CrossRef]
- Chanda, A.; Ruchti, T.; Unnikrishnan, V. Computational Modeling of Wound Suture: A Review. IEEE Rev. Biomed. Eng. 2018, 11, 165–176. [Google Scholar] [CrossRef]
- Murakami, N.; Wakabayashi, N. Finite element contact analysis as a critical technique in dental biomechanics: A review. J. Prosthodont. Res. 2014, 58, 92–101. [Google Scholar] [CrossRef]
- Peskersoy, C.; Sahan, H.M. Finite element analysis and nanomechanical properties of composite and ceramic dental onlays. Comput. Methods Biomech. Biomed. Eng. 2022, 25, 1649–1661. [Google Scholar] [CrossRef]
- Hu, S.; Wan, J.; Duan, L.; Chen, J. Influence of pontic design on speech with an anterior fixed dental prosthesis: A clinical study and finite element analysis. J. Prosthet. Dent. 2021, 126, e1–e9. [Google Scholar] [CrossRef]
- Jiang, J.; Yao, L.; Zhang, Y.; Ma, X.; Guo, Y.; Liu, Y. Establishment, FEM analysis and experimental validation of tooth movement prediction model of orthodontic archwire T-loop. BMC Oral Health 2022, 22, 406. [Google Scholar] [CrossRef]
- Poiate, I.A.V.P.; De Vasconcellos, A.B.; Santana, R.; Poiate, E. Three-Dimensional Stress Distribution in the Human Periodontal Ligament in Masticatory, Parafunctional, and Trauma Loads: Finite Element Analysis. J. Periodontol. 2009, 80, 1859–1867. [Google Scholar] [CrossRef]
- Zarone, F.; Sorrentino, R.; Apicella, D.; Valentino, B.; Ferrari, M.; Aversa, R.; Apicella, A. Evaluation of the biomechanical behavior of maxillary central incisors restored by means of endocrowns compared to a natural tooth: A 3D static linear finite elements analysis. Dent. Mater. 2006, 22, 1035–1044. [Google Scholar] [CrossRef]
- Rodrigues, M.D.P.; Soares, P.B.F.; Valdivia, A.D.C.M.; Pessoa, R.S.; Veríssimo, C.; Versluis, A.; Soares, C.J. Patient-specific Finite Element Analysis of Fiber Post and Ferrule Design. J. Endod. 2017, 43, 1539–1544. [Google Scholar] [CrossRef]
- Ilie, N.; Hickel, R. Investigations on a methacrylate-based flowable composite based on the SDR™ technology. Dent. Mater. 2011, 27, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Dressano, D.; Salvador, M.V.; Oliveira, M.T.; Marchi, G.M.; Fronza, B.M.; Hadis, M.; Palin, W.M.; Lima, A.F. Chemistry of novel and contemporary resin-based dental adhesives. J. Mech. Behav. Biomed. Mater. 2020, 110, 103875. [Google Scholar] [CrossRef]
- Huang, H.-M.; Tsai, C.-Y.; Lee, H.-F.; Lin, C.-T.; Yao, W.-C.; Chiu, W.-T.; Lee, S.-Y. Damping effects on the response of maxillary incisor subjected to a traumatic impact force: A nonlinear finite element analysis. J. Dent. 2006, 34, 261–268. [Google Scholar] [CrossRef]
- ISO 4049:2019; Dentistry—Polymer-Based Restorative Material. 2019. Available online: https://www.iso.org/standard/67596.html (accessed on 9 August 2022).
- Nyashin, Y.; Biomechanical Modelling of Periodontal Ligament Behaviour under Various Mechanical Loads. Acta of Bioengineering and Biomechanics. 2000. Available online: https://www.semanticscholar.org/paper/Biomechanical-modelling-of-periodontal-ligament-Nyashin-Nyashin/5776b0c7c69a2de5f6eee2826962c710e36ebaeb (accessed on 11 August 2022).
- Koc, D.; Dogan, A.; Bek, B. Bite Force and Influential Factors on Bite Force Measurements: A Literature Review. Eur. J. Dent. 2010, 4, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, H.; Finger, W.J.; Wegner, K.; Utterodt, A.; Komatsu, M.; Wöstmann, B.; Balkenhol, M. Factors influencing marginal cavity adaptation of nanofiller containing resin composite restorations. Dent. Mater. 2010, 26, 1166–1175. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Burrow, M.F.; Tagami, J. A light curing method for improving marginal sealing and cavity wall adaptation of resin composite restorations. Dent. Mater. 2001, 17, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Boaro, L.C.; Gonçalves, F.; Guimarães, T.C.; Ferracane, J.L.; Pfeifer, C.S.; Braga, R.R. Sorption, solubility, shrinkage and mechanical properties of “low-shrinkage” commercial resin composites. Dent. Mater. 2013, 29, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Ferracane, J.L.; Stansbury, J.W.; Burke, F.J.T. Self-adhesive resin cements—Chemistry, properties and clinical considerations. J. Oral Rehabil. 2010, 38, 295–314. [Google Scholar] [CrossRef]
Figure 1.
Constituents of tooth showing root, enamel, and pulp.
Figure 1.
Constituents of tooth showing root, enamel, and pulp.
Figure 2.
Fracture models: (a) Crown, (b) Crown fracture with adhesive material, and (c) crown–root.
Figure 2.
Fracture models: (a) Crown, (b) Crown fracture with adhesive material, and (c) crown–root.
Figure 3.
Meshes: (a) Adhesive material, (b) lower part of crown fracture, and (c) upper part of crown fracture.
Figure 3.
Meshes: (a) Adhesive material, (b) lower part of crown fracture, and (c) upper part of crown fracture.
Figure 4.
Loads and boundary conditions.
Figure 4.
Loads and boundary conditions.
Figure 5.
Contours under masticatory loading: (a) Displacement, (b) von Mises Stress, and (c) Shear Stress.
Figure 5.
Contours under masticatory loading: (a) Displacement, (b) von Mises Stress, and (c) Shear Stress.
Figure 6.
Contours depicting location of maximum von Mises stress under masticatory load at (a) Enamel, and (b) Dentin.
Figure 6.
Contours depicting location of maximum von Mises stress under masticatory load at (a) Enamel, and (b) Dentin.
Figure 7.
Contours under traumatic loading: (a) Displacement, (b) von Mises Stress, and (c) Shear Stress.
Figure 7.
Contours under traumatic loading: (a) Displacement, (b) von Mises Stress, and (c) Shear Stress.
Figure 8.
Countours depicting location of maximum values under traumatic load at (a) von Mises stress at Enamel, (b) von Mises stress at Dentin, and (c) shear stress at Dentin.
Figure 8.
Countours depicting location of maximum values under traumatic load at (a) von Mises stress at Enamel, (b) von Mises stress at Dentin, and (c) shear stress at Dentin.
Figure 9.
Displacement, stresses, and shear stresses across crown fracture: (a) masticatory loading in case of flowable composite, (b) masticatory loading in case of resin cement, (c) masticatory loading in case of resin adhesive, (d) traumatic loading in case of flowable composite, (e) traumatic loading in case of resin cement, and (f) traumatic loading in case of resin adhesive. The white dashed line in the figure represents the fracture line.
Figure 9.
Displacement, stresses, and shear stresses across crown fracture: (a) masticatory loading in case of flowable composite, (b) masticatory loading in case of resin cement, (c) masticatory loading in case of resin adhesive, (d) traumatic loading in case of flowable composite, (e) traumatic loading in case of resin cement, and (f) traumatic loading in case of resin adhesive. The white dashed line in the figure represents the fracture line.
Figure 10.
Displacement, stresses, and shear stresses across crown–root fracture: (a) masticatory loading in case of flowable composite, (b) masticatory loading in case of resin cement, (c) masticatory loading in case of resin adhesive, (d) traumatic loading in case of flowable composite, (e) traumatic loading in case of resin cement, and (f) traumatic loading in case of resin adhesive. The white dashed line in the figure represents the fracture line.
Figure 10.
Displacement, stresses, and shear stresses across crown–root fracture: (a) masticatory loading in case of flowable composite, (b) masticatory loading in case of resin cement, (c) masticatory loading in case of resin adhesive, (d) traumatic loading in case of flowable composite, (e) traumatic loading in case of resin cement, and (f) traumatic loading in case of resin adhesive. The white dashed line in the figure represents the fracture line.
Figure 11.
Effect of adhesive materials and varying loads on the reattached tooth. Maximum displacement under (a) masticatory load (b) traumatic load, von Mises stress under (c) masticatory load, (d) traumatic load, shear stress across (e) masticatory load, (f) traumatic load across both crown fracture and crown–root fracture.
Figure 11.
Effect of adhesive materials and varying loads on the reattached tooth. Maximum displacement under (a) masticatory load (b) traumatic load, von Mises stress under (c) masticatory load, (d) traumatic load, shear stress across (e) masticatory load, (f) traumatic load across both crown fracture and crown–root fracture.
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}














