
Green Automated Solid Phase Extraction to Measure Levofloxacin in Human Serum via Liquid Chromatography with Fluorescence Detection for Pharmacokinetic Study

 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Mobile Phases
2.3. Instrumentation
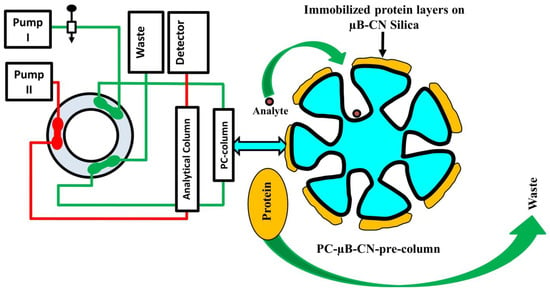
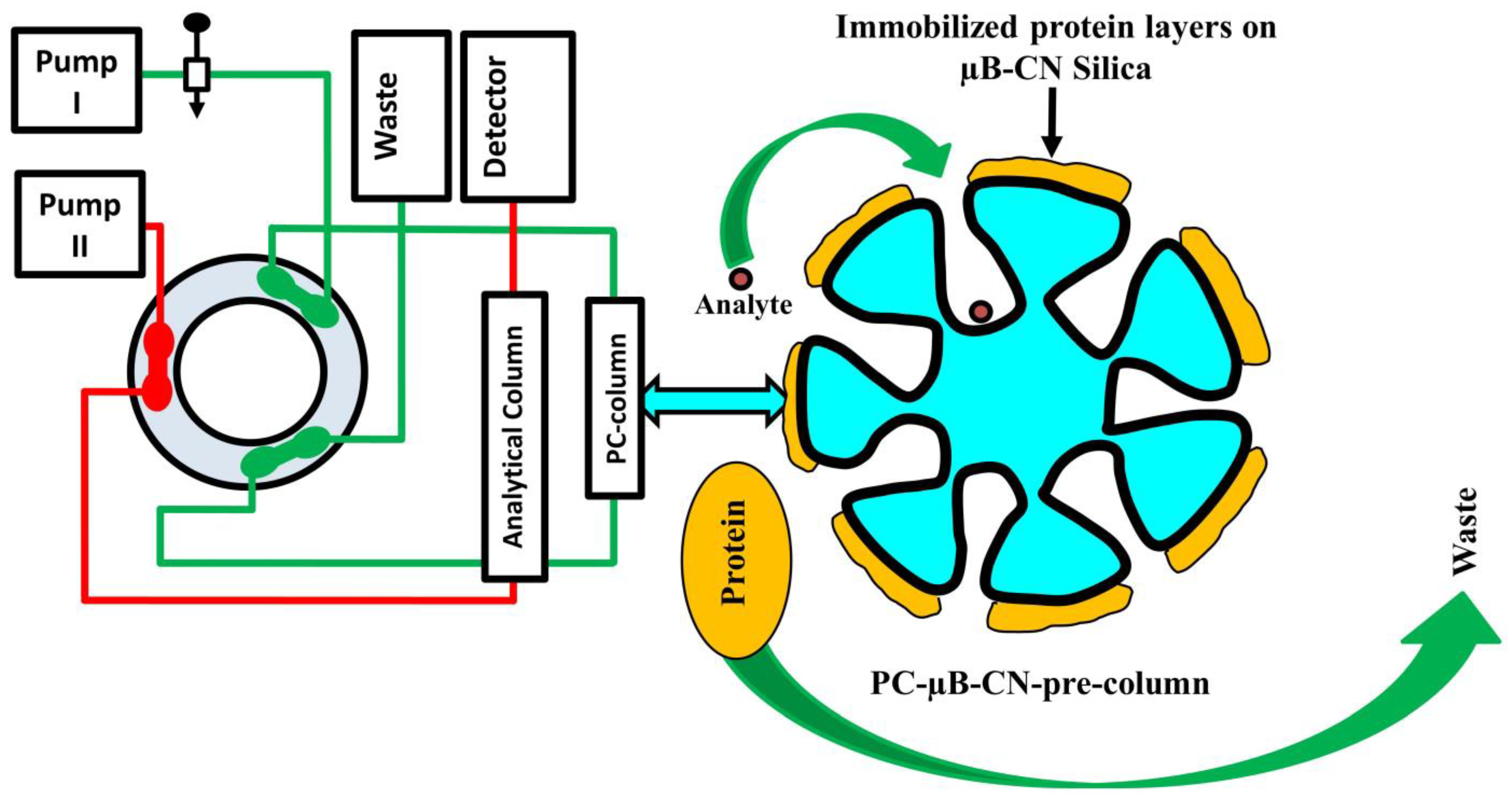
2.4. Aut-SPE-BA-HPLC-FL
2.5. Standard Solutions and Quality Control Samples
2.6. Recovery and Precision
2.7. Application
3. Results
3.1. Chromatographic Conditions
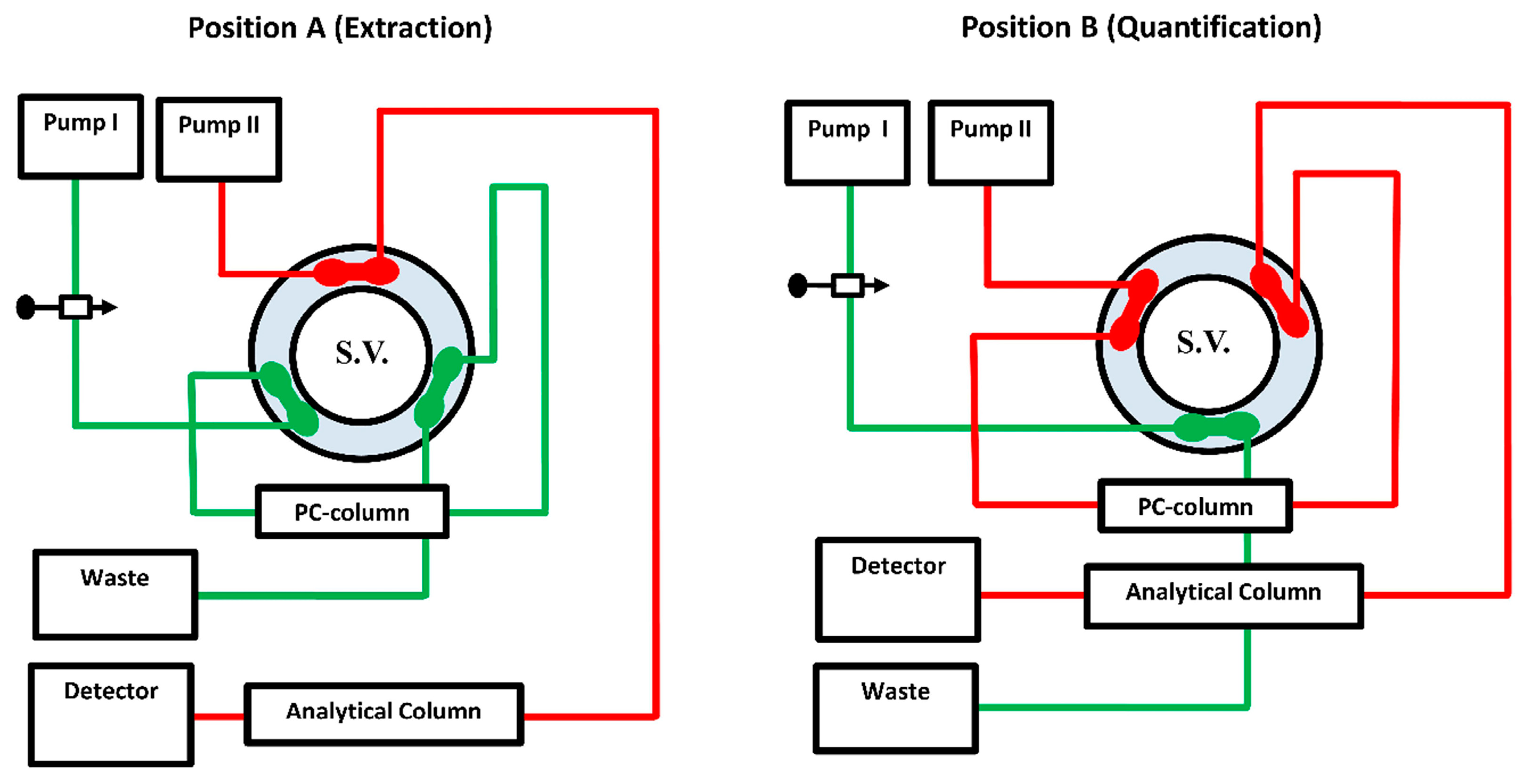
3.2. Properties of Columns and Switching Valve Timing
3.3. On-Through Elution Mode
3.4. Breakthrough Study of PC-µBCN-Pre-Column
3.5. PC-µBCN-Pre-Column Lifespan
3.6. Greenness Assessment of the Developed On-Line SPE Protocol
3.7. Method Validation
3.7.1. Linearity, Limit of Detection and Limit of Quantification
3.7.2. Method of Absolute Recovery
3.7.3. Precision
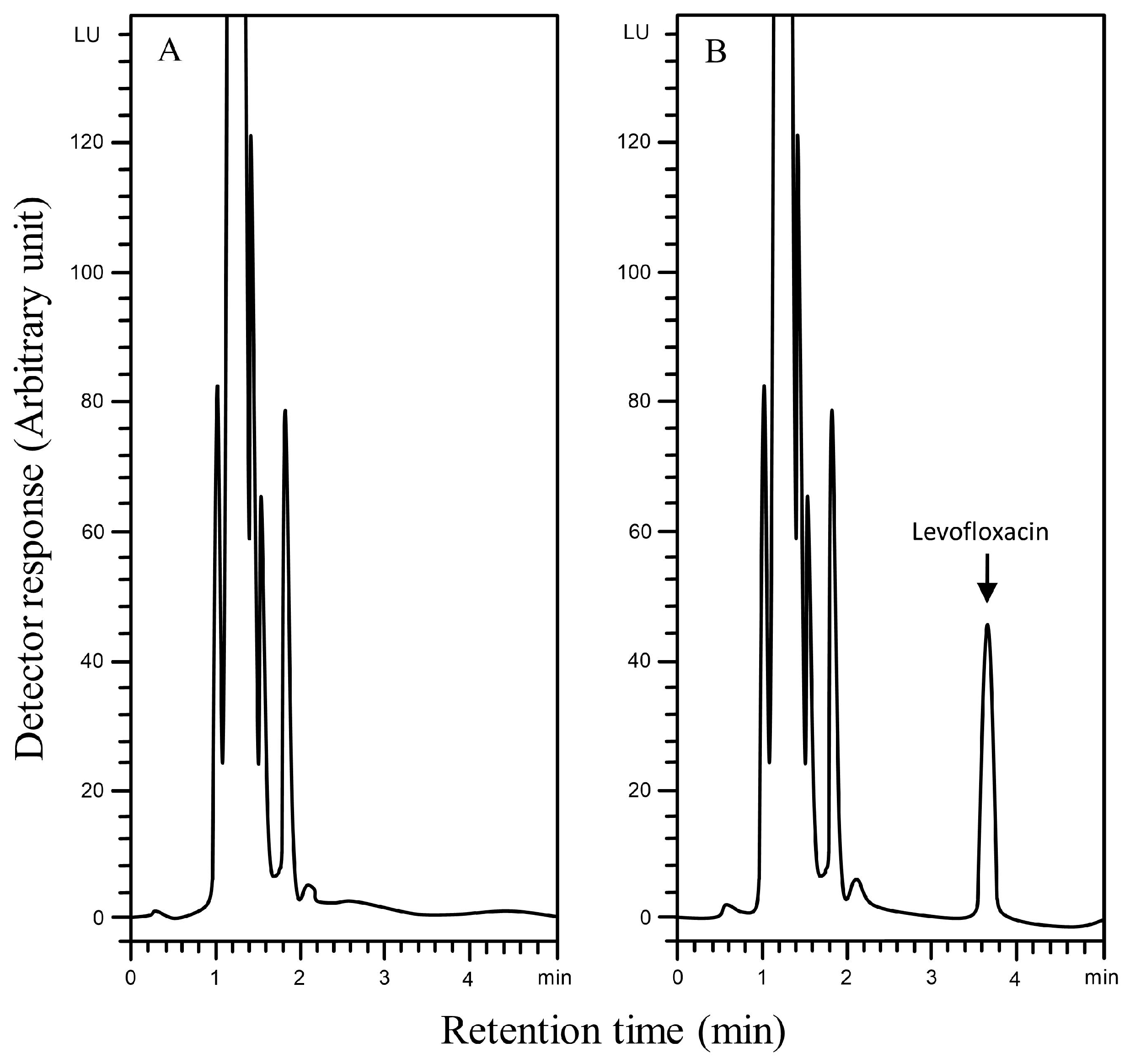
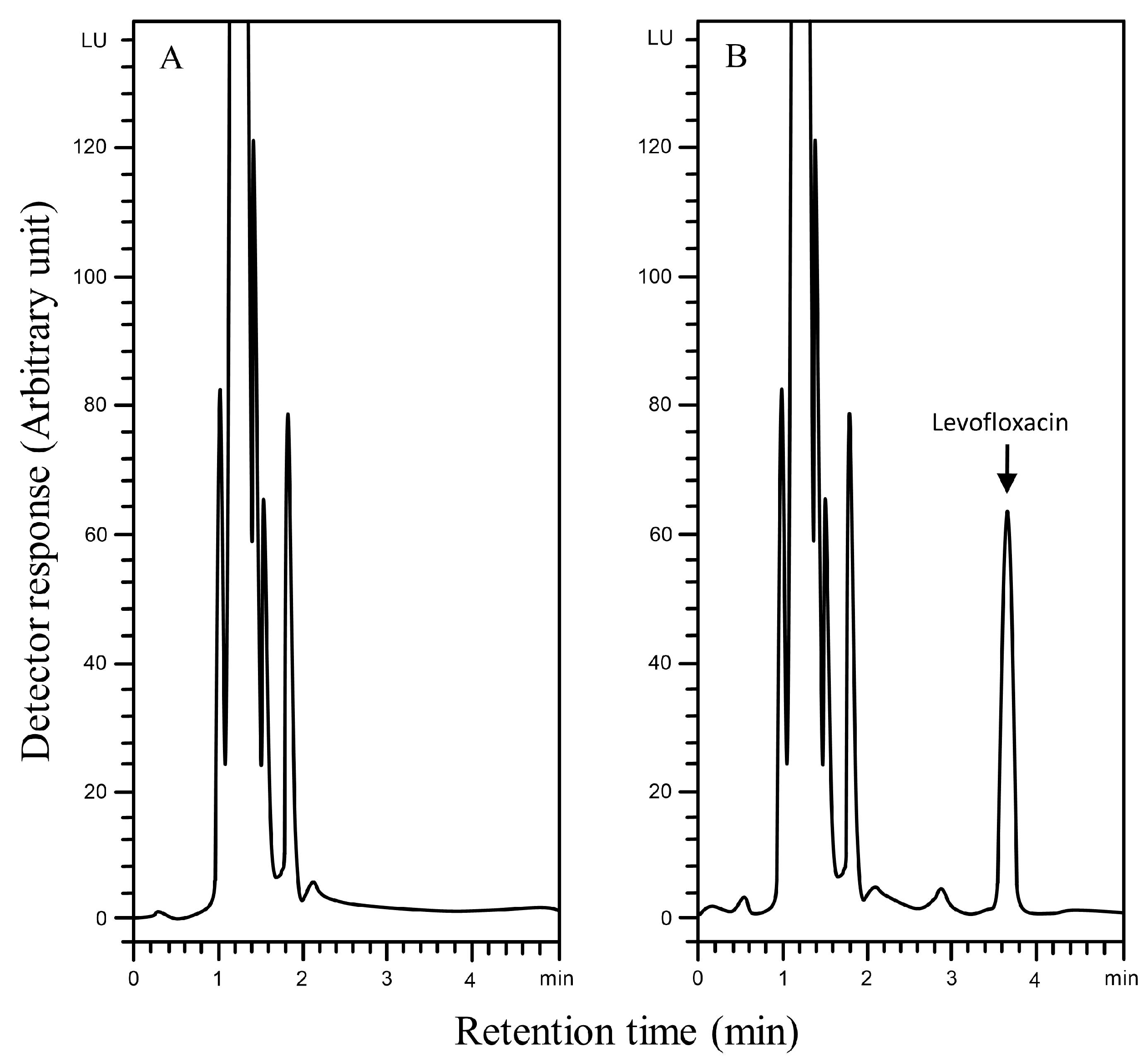
3.7.4. Selectivity
3.7.5. Stability Studies
3.7.6. Robustness
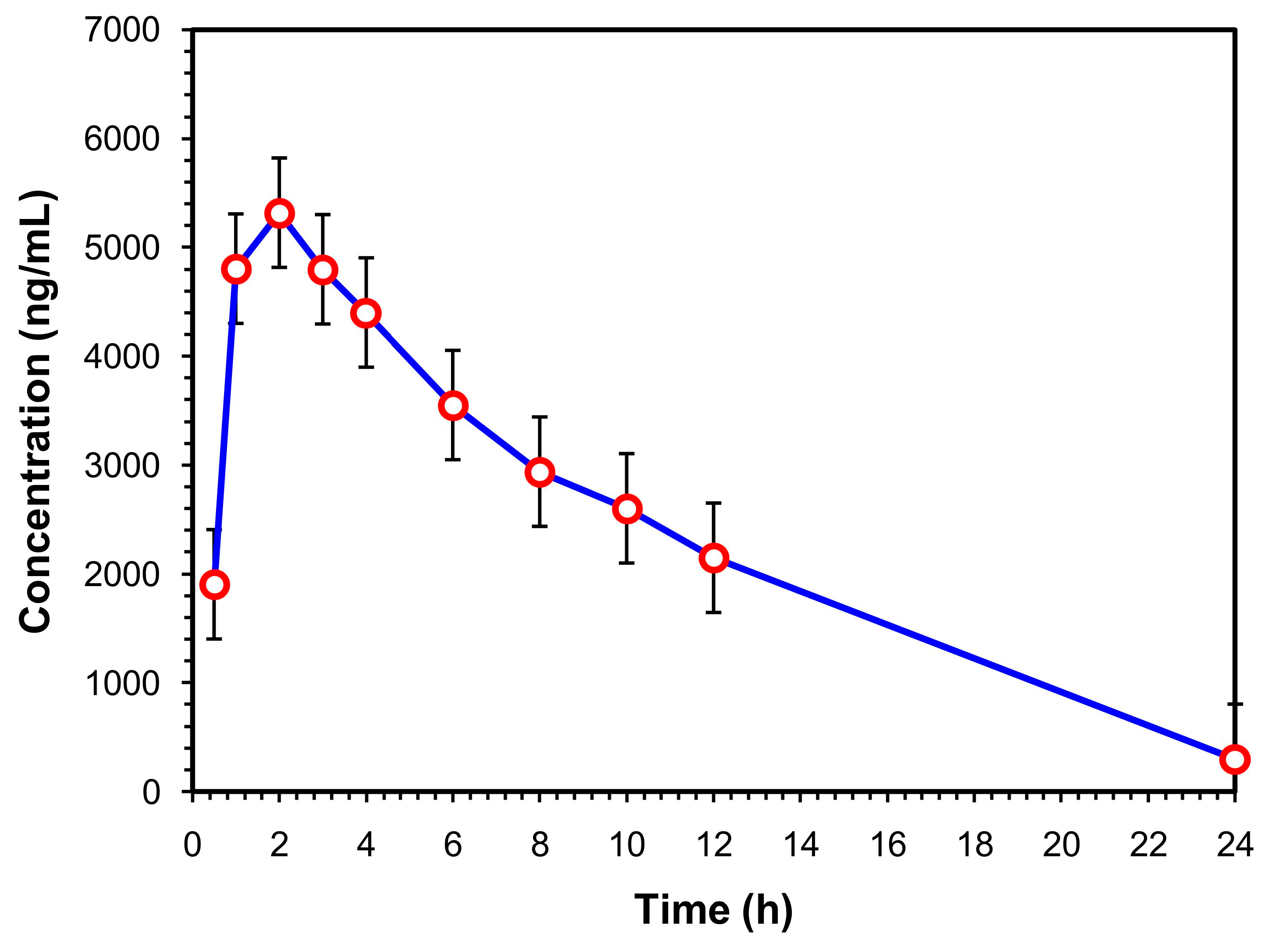
3.8. Application of the Aut-SPE-BA-HPLC-FL Technique
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Gindy, A.; Emara, S.; Mostafa, A. UV partial least-squares calibration and liquid chromatographic methods for direct quantitation of levofloxacin in urine. J. AOAC Int. 2007, 90, 1258–1265. [Google Scholar] [PubMed]
- Czyrskia, A.; Szałekb, E. An HPLC method for levofloxacin determination and its application in biomedical analysis. J. Anal. Chem. 2016, 71, 840–843. [Google Scholar] [CrossRef]
- Schulte, S.; Ackermann, T.; Bertram, N.; Sauerbruch, T.; Paar, W.D. Determination of the newer quinolones levofloxacin and moxifloxacin in plasma by high-performance liquid chromatography with fluorescence detection. J. Chromatogr. Sci. 2006, 44, 205–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghimire, S.; Hateren, K.V.; Vrubleuskaya, N.; Koster, R.; Touw, D.; Alffenaar, J.C. Determination of levofloxacin in human serum using liquid chromatography tandem mass spectrometry. J. Appl. Bioanal. 2018, 4, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Emara, S.; Morita, I.; Tamura, K.; Razee, S.; Masujima, T.; Mohamed, H.; Gizawy, S.; Rabbat, N. Utility of ion-pair chromatography for analysis of some anthracyclines in plasma and urine. J. Liq. Chromatogr. Relat. Technol. 1998, 21, 681–692. [Google Scholar] [CrossRef]
- Hadad, G.; Salam, R.A.; Emara, S. Validated and optimized high-performance liquid chromatographic determination of tizoxanide, the main active metabolite of nitazoxanide in human urine, plasma and breast milk. J. Chromatogr. Sci. 2012, 50, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Emara, S.; Razee, S.; Khedr, A.; Masujima, T. On-line precolumn derivatization for HPLC determination of methotrexate using a column packed oxidant. Biomed. Chromatogr. 1997, 11, 42–46. [Google Scholar] [CrossRef]
- Kumar, T.M.; Srikanth, G.; Rao, J.V.; Rao, K.S. Development and validation of HPLC-UV method for the estimation of levofloxacin in human plasma. Int. J. Pharm. Pharm. Sci. 2011, 3, 247–250. [Google Scholar]
- Wong, F.A.; Juzwin, S.J.; Flor, S.C. Rapid stereospecific high-performance liquid chromatographic determination of levofloxacin in human plasma and urine. J. Pharm. Biomed. Anal. 1997, 15, 765–771. [Google Scholar] [CrossRef]
- Srinivas, N.; Narasu, L.; Shankar, B.P.; Mullangi, R. Development and validation of a HPLC method for simultaneous quantitation of gatifloxacin, sparfloxacin and moxifloxacin using levofloxacin as internal standard in human plasma: Application to a clinical pharmacokinetic study. Biomed. Chromatogr. 2008, 22, 1288–1295. [Google Scholar] [CrossRef]
- Pea, F.; Di Qual, E.; Cusenza, A.; Brollo, L.; Baldassarre, M.; Furlanut, M. Pharmacokinetics and pharmacodynamics of intravenous levofloxacin in patients with early-onset ventilator-associated pneumonia. Clin. Pharmacokinet. 2003, 42, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Manousi, N.; Tzanavaras, P.D.; Zacharis, C.K. Bioanalytical HPLC applications of in-tube solid phase microextraction: A two-decade overview. Molecules 2020, 25, 2096. [Google Scholar] [CrossRef] [PubMed]
- Toi, P.V.; Pouplin, T.; Tho, N.D.K.; Phuong, P.N.; Chau, T.T.H.; Thuong, N.T.; Heemskerk, D.; Hien, T.T.; Thwaites, G.E. High-performance liquid chromatography with time-programmed fluorescence detection for the quantification of levofloxacin in human plasma and cerebrospinal fluid in adults with tuberculous meningitis. J. Chromatogr. B 2017, 1061, 256–262. [Google Scholar]
- Nemutlu, E.; Kır, S.; Özyüncü, Ö.; Beksaç, M.S. Simultaneous separation and determination of seven quinolones using HPLC: Analysis of levofloxacin and moxifloxacin in plasma and amniotic fluid. Chromatographia 2007, 66, 15–24. [Google Scholar] [CrossRef]
- Djabarouti, S.; Boselli, E.; Allaouchiche, B.; Ba, B.; Nguyen, A.T.; Gordien, J.B.; Bernadou, J.M.; Saux, M.C.; Breilh, D. Determination of levofloxacin in plasma, bronchoalveolar lavage and bone tissues by high-performance liquid chromatography with ultraviolet detection using a fully automated extraction method. J. Chromatogr. B 2004, 799, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Ebers, A.; Stroup, S.; Mpagama, S.; Kisonga, R.; Lekule, I.; Liu, J.; Heysell, S. Determination of plasma concentrations of levofloxacin by high performance liquid chromatography for use at a multidrug-resistant tuberculosis hospital in Tanzania. PLoS ONE 2017, 12, e0170663. [Google Scholar] [CrossRef] [Green Version]
- Caufield, W.V.; Stewart, J.T. Determination of zidovudine and levofloxacin in human plasma by reversed phase and solid phase extraction. J. Liq. Chromatogr. Relat. Technol. 2002, 25, 1791–1805. [Google Scholar] [CrossRef]
- Böttcher, S.; von Baum, H.; Hoppe-Tichy, T.; Benz, C.; Sonntag, H.G. An HPLC assay and a microbiological assay to determine levofloxacin in soft tissue, bone, bile and serum. J. Pharm. Biomed. Anal. 2001, 25, 197–203. [Google Scholar] [CrossRef]
- Aguilar-Carrasco, J.C.; Hernández-Pineda, J.; Jiménez-Andrade, J.M.; Flores-Murrieta, F.J.; Carrasco-Portugal, M.D.C.; López-Canales, J.S. Rapid and sensitive determination of levofloxacin in microsamples of human plasma by high-performance liquid chromatography and its application in a pharmacokinetic study. Biomed. Chromatogr. 2015, 29, 341–345. [Google Scholar] [CrossRef]
- Szerkus, O.; Jacyna, J.; Wiczling, P.; Gibas, A.; Sieczkowski, M.; Siluk, D.; Matuszewski, M.; Kaliszan, R.; Markuszewski, M.J. Ultra-high performance liquid chromatographic determination of levofloxacin in human plasma and prostate tissue with use of experimental design optimization procedures. J. Chromatogr. B 2016, 1029, 48–59. [Google Scholar] [CrossRef]
- Notario, D.; Martono, S.; Ikawati, Z.; Hakim, A.R.; Jannah, F.; Lukitaningsih, E. A rapid and simple high-performance liquid chromatographic method for determination of levofloxacin in human plasma. Indones. J. Chem. 2017, 17, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Siewert, S. Validation of a levofloxacin HPLC assay in plasma and dialysate for pharmacokinetic studies. J. Pharm. Biomed. Anal. 2006, 41, 1360–1362. [Google Scholar] [CrossRef] [PubMed]
- Ansari, M.J.; Aldawsari, M.F.; Iqbal, Z.; Khuroo, A. Determination of levofloxacin in human plasma by HPLC: Method development, validation, stability evaluation and application to pharmacokinetics. Lat. Am. J. Pharm. 2020, 39, 1149–1158. [Google Scholar]
- Neckel, U.; Joukhadar, C.; Frossard, M.; Jäger, W.; Müller, M.; Mayer, B.X. Simultaneous determination of levofloxacin and ciprofloxacin in microdialysates and plasma by high-performance liquid chromatography. Anal. Chim. Acta 2002, 463, 199–206. [Google Scholar] [CrossRef]
- Sousa, J.; Alves, G.; Campos, G.; Fortuna, A.; Falcão, A. First liquid chromatography method for the simultaneous determination of levofloxacin, pazufloxacin, gatifloxacin, moxifloxacin and trovafloxacin in human plasma. J. Chromatogr. B 2013, 930, 104–111. [Google Scholar] [CrossRef]
- Watabe, S.; Yokoyama, Y.; Nakazawa, K.; Shinozaki, K.; Hiraoka, R.; Takeshita, K.; Suzuki, Y. Simultaneous measurement of pazufloxacin, ciprofloxacin, and levofloxacin in human serum by high-performance liquid chromatography with fluorescence detection. J. Chromatogr. B 2010, 878, 1555–1561. [Google Scholar] [CrossRef]
- Nguyen, H.A.; Grellet, J.; Ba, B.B.; Quentin, C.; Saux, M.C. Simultaneous determination of levofloxacin, gatifloxacin and moxifloxacin in serum by liquid chromatography with column switching. J. Chromatogr. B 2004, 810, 77–83. [Google Scholar] [CrossRef]
- Martin, P.D.; Jones, G.R.; Stringer, F.; Wilson, I.D. Comparison of normal and reversed-phase solid phase extraction methods for extraction of β-blockers from plasma using molecularly imprinted polymers. Analyst 2003, 128, 345–350. [Google Scholar] [CrossRef]
- Liang, Y.; Zhou, I. Recent advances of online coupling of sample preparation techniques with ultrahigh performance liquid chromatography and supercritical fluid chromatography. J. Sep. Sci. 2019, 42, 226–242. [Google Scholar] [CrossRef]
- Emara, S.; Kamal, M.; Hadad, G.; Zaazaa, H.; Kawi, M.A. Back-flush column-switching technique for on-line sample cleanup and enrichment to determine guaiphenesin in human serum. J. Liq. Chromatogr. Relat. Technol. 2012, 35, 15–27. [Google Scholar] [CrossRef]
- Emara, S.; Khedr, A.; Askal, H. Rapid and specific precolumn extraction high-performance liquid chromatographic assay for bupivacaine in human serum. Biomed. Chromatogr. 1996, 10, 131–134. [Google Scholar] [CrossRef]
- Emara, S. Simultaneous determination of caffeine, theophylline and theobromine in human plasma by on-line solid-phase extraction coupled to reversed-phase chromatography. Biomed. Chromatogr. 2004, 18, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Sonbol, H.; Ebrahim, H.; Malak, M.; Ali, A.; Aboulella, Y.; Hadad, G.; Emara, S.; Shawky, A. Application of a small protein-coated column to trap, extract and enrich carbamazepine directly from human serum for direct chromatographic analysis. Separations 2023, 10, 71. [Google Scholar] [CrossRef]
- Szerkus, O.; Jacyna, J.; Gibas, A.; Sieczkowski, M.; Siluk, D.; Matuszewski, M.; Kaliszan, R.; Markuszewski, M.J. Robust HPLC-MS/MS method for levofloxacin and ciprofloxacin determination in human prostate tissue. J. Pharm. Biomed. Anal. 2017, 132, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Song, X.; Liu, Z.; Zhao, X.; Geng, L.; Bi, K.; Chen, X. Development of an LC-MS method for determination of three active constituents of Shuang-huang-lian injection in rat plasma and its application to the drug interaction study of Shuang-huang-lian freeze-dried powder combined with levofloxacin injection. J. Chromatogr. B 2012, 898, 130–135. [Google Scholar] [CrossRef]
- Rossmann, J.; Schubert, S.; Gurke, R.; Oertel, R.; Kirch, W. Simultaneous determination of most prescribed antibiotics in multiple urban wastewater by SPE-LC-MS/MS. J. Chromatogr. B 2014, 969, 162–170. [Google Scholar] [CrossRef]
- Xu, H.; Chen, L.; Sun, L.; Sun, X.; Du, X.; Wang, J.; Wang, T.; Zeng, Q.; Wang, H.; Xu, Y.; et al. Microwave-assisted extraction and in situ clean-up for the determination of fluoroquinolone antibiotics in chicken breast muscle by LC-MS/MS. J. Sep. Sci. 2011, 34, 142–149. [Google Scholar] [CrossRef]
- Bao, D.; Truong, T.T.; Renick, P.J.; Pulse, M.E.; Weiss, W.J. Simultaneous determination of rifampicin and levofloxacin concentrations in catheter segments from a mouse model of a device-related infection by liquid chromatography/electrospray ionization tandem mass spectrometry. J. Pharm. Biomed. Anal. 2008, 46, 723–727. [Google Scholar] [CrossRef]
- Ziarrusta, H.; Val, N.; Dominguez, H.; Mijangos, L.; Prieto, A.; Usobiaga, A.; Etxebarria, N.; Zuloaga, O.; Olivares, M. Determination of fluoroquinolones in fish tissues, biological fluids, and environmental waters by liquid chromatography tandem mass spectrometry. Anal. Bioanal. Chem. 2017, 409, 6359–6370. [Google Scholar] [CrossRef]
- Cao, G.; Zhu, Y.; Xie, X.; Chen, Y.; Yu, J.; Zhang, J.; Chen, Z.; Pang, L.; Zhang, Y.; Shi, Y. Pharmacokinetics and pharmacodynamics of levofloxacin in bronchial mucosa and lung tissue of patients undergoing pulmonary operation. Exp. Ther. Med. 2020, 20, 607–616. [Google Scholar] [CrossRef]
- Gałuszka, A.; Migaszewski, Z.M.; Konieczka, P.; Namieśnik, J. Analytical Eco-Scale for assessing the greenness of analytical procedures. TrAC Ternds Anal. Chem. 2012, 37, 61–72. [Google Scholar] [CrossRef]
- Tilea, B.; Vlase, L.; Popa, D.-S.; Primejdie, D.; Muntean, D.L.; Tilea, I. Therapeutic monitoring of levofloxacin: A new LC-MS/MS method for quantification of levofloxacin in human plasma. Stud. Univ. Babes Bolyai Chem. 2013, 58, 105–115. [Google Scholar]
- Chien, S.C.; Chow, A.T.; Rogge, M.C.; Williams, R.R.; Hendrix, C.W. Pharmacokinetics and safety of oral levofloxacin in human immunodeficiency virus-infected individuals receiving concomitant zidovudine. Antimicrob. Agents Chemother. 1997, 41, 1765–1769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emara, S.; El-Gindy, A.; Mesbah, M.K.; Hadad, G.M. Direct injection liquid chromatographic technique for simultaneous determination of two antihistaminic drugs and their main metabolites in serum. J. AOAC. Int. 2007, 90, 384–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emara, S.; Masujima, T.; Zarad, W.; Kamal, M.; Fouad, M.; El-Bagary, R. An Eco-friendly direct injection HPLC method for methyldopa determination in serum by mixed-mode chromatography using a single protein-coated column. J. Chromatogr. Sci. 2015, 53, 1353–1360. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Levofloxacin |
|---|---|
| Calibration range (ng/mL) | 10–10,000 |
| LOD (ng/mL) | 2.5 |
| LOQ (ng/mL) | 8.5 |
| Regression equation (Y) a: | |
| Slope (b) | 0.0166 |
| Intercept (a) | 0.5799 |
| Correlation coefficient (r2) | 0.9992 |
| Nominal Concentration (ng/mL). | Recovery (%) a ± SD | CV (%) | |
|---|---|---|---|
| Intra-assay | 40 | 87.12 ± 7.83 | 8.98 |
| 400 | 92.06 ± 5.91 | 6.41 | |
| 4000 | 97.36 ± 4.17 | 4.28 | |
| 8000 | 97.55 ± 3.63 | 3.72 | |
| Inter-assay | 40 | 86.44 ± 8.25 | 9.54 |
| 400 | 91.52 ± 6.36 | 6.94 | |
| 4000 | 96.71 ± 4.48 | 4.63 | |
| 8000 | 97.04 ± 4.07 | 4.19 | |
| Parameter | Value | Unit |
|---|---|---|
| Lambda-z | 0.16 ± 0.02 | 1/h |
| Cmax | 5453.20 ± 398.98 | ng/mL |
| Tmax | 2.20 ± 0.45 | h |
| T1/2 | 4.33 ± 0.48 | h |
| AUC 0-t | 57,757.00 ± 2463.44 | ng/mL·h |
| AUC 0-inff | 59,601.40 ± 2093.06 | ng/mL·h |
| MRT 0-inf | 8.19 ± 0.33 | h |
| Vz/F | 0.05 ± 0.01 | (mg)/(ng/mL) |
| Cl/F | 0.008 ± 0.00 | (mg)/(ng/mL)/h |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebrahim, H.; Sonbol, H.; Malak, M.; Ali, A.; Aboulella, Y.; Hadad, G.; Zarad, W.; Emara, S.; Bazan, L. Green Automated Solid Phase Extraction to Measure Levofloxacin in Human Serum via Liquid Chromatography with Fluorescence Detection for Pharmacokinetic Study. Separations 2023, 10, 136. https://doi.org/10.3390/separations10020136
Ebrahim H, Sonbol H, Malak M, Ali A, Aboulella Y, Hadad G, Zarad W, Emara S, Bazan L. Green Automated Solid Phase Extraction to Measure Levofloxacin in Human Serum via Liquid Chromatography with Fluorescence Detection for Pharmacokinetic Study. Separations. 2023; 10(2):136. https://doi.org/10.3390/separations10020136
Chicago/Turabian StyleEbrahim, Hager, Heba Sonbol, Monika Malak, Ahmed Ali, Yasmine Aboulella, Ghada Hadad, Walaa Zarad, Samy Emara, and Lamyaa Bazan. 2023. "Green Automated Solid Phase Extraction to Measure Levofloxacin in Human Serum via Liquid Chromatography with Fluorescence Detection for Pharmacokinetic Study" Separations 10, no. 2: 136. https://doi.org/10.3390/separations10020136