
Perforating Gout: Expanding the Differential for Transepidermal Elimination

Abstract
:1. Introduction
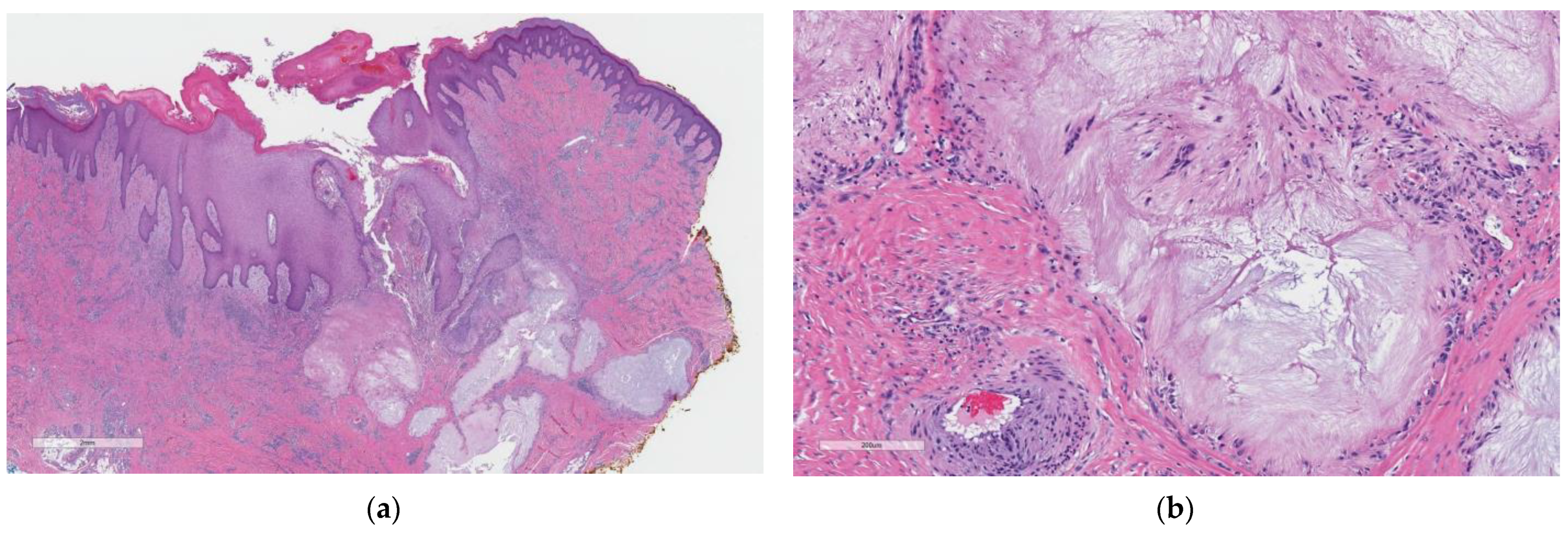
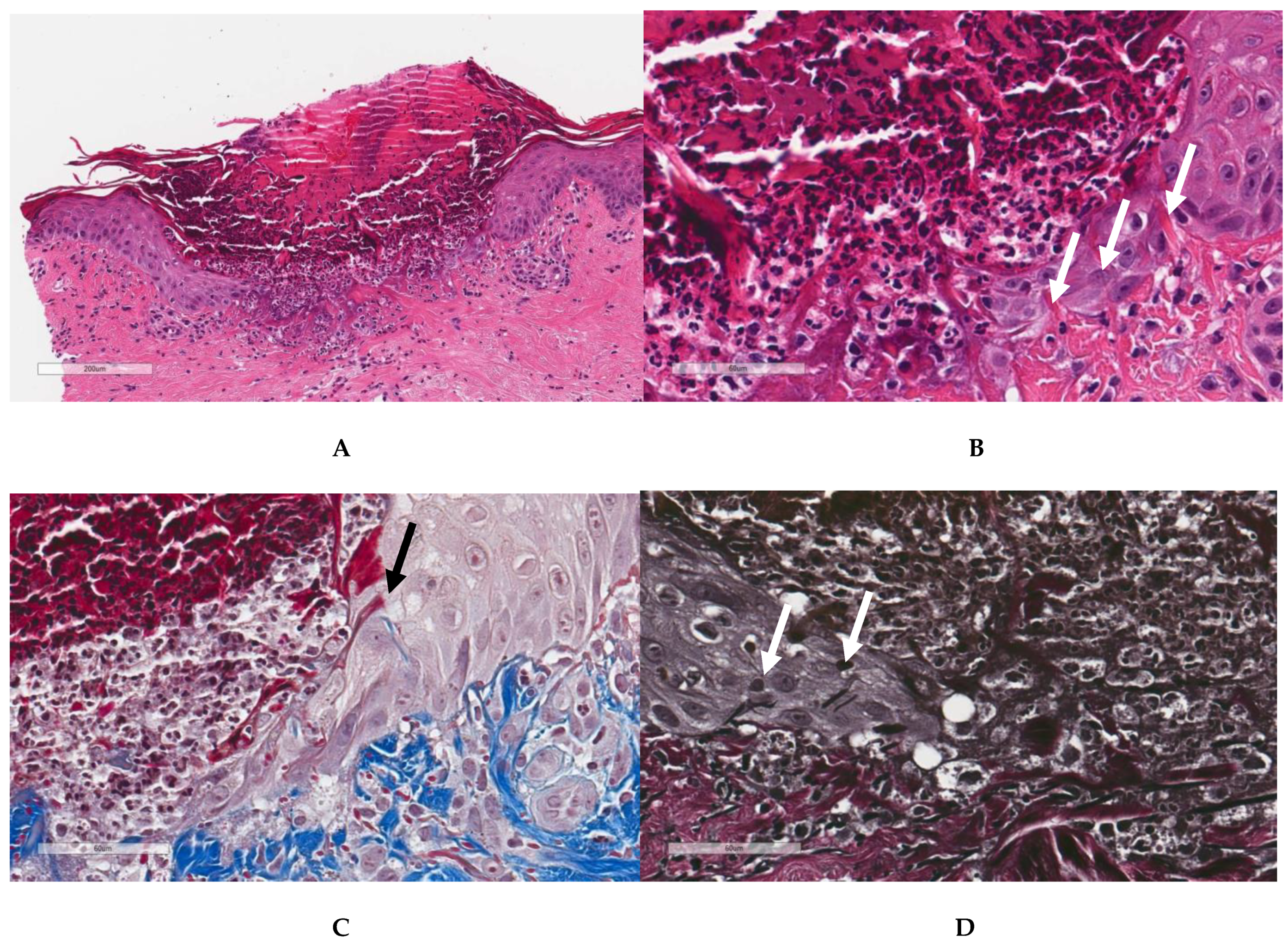
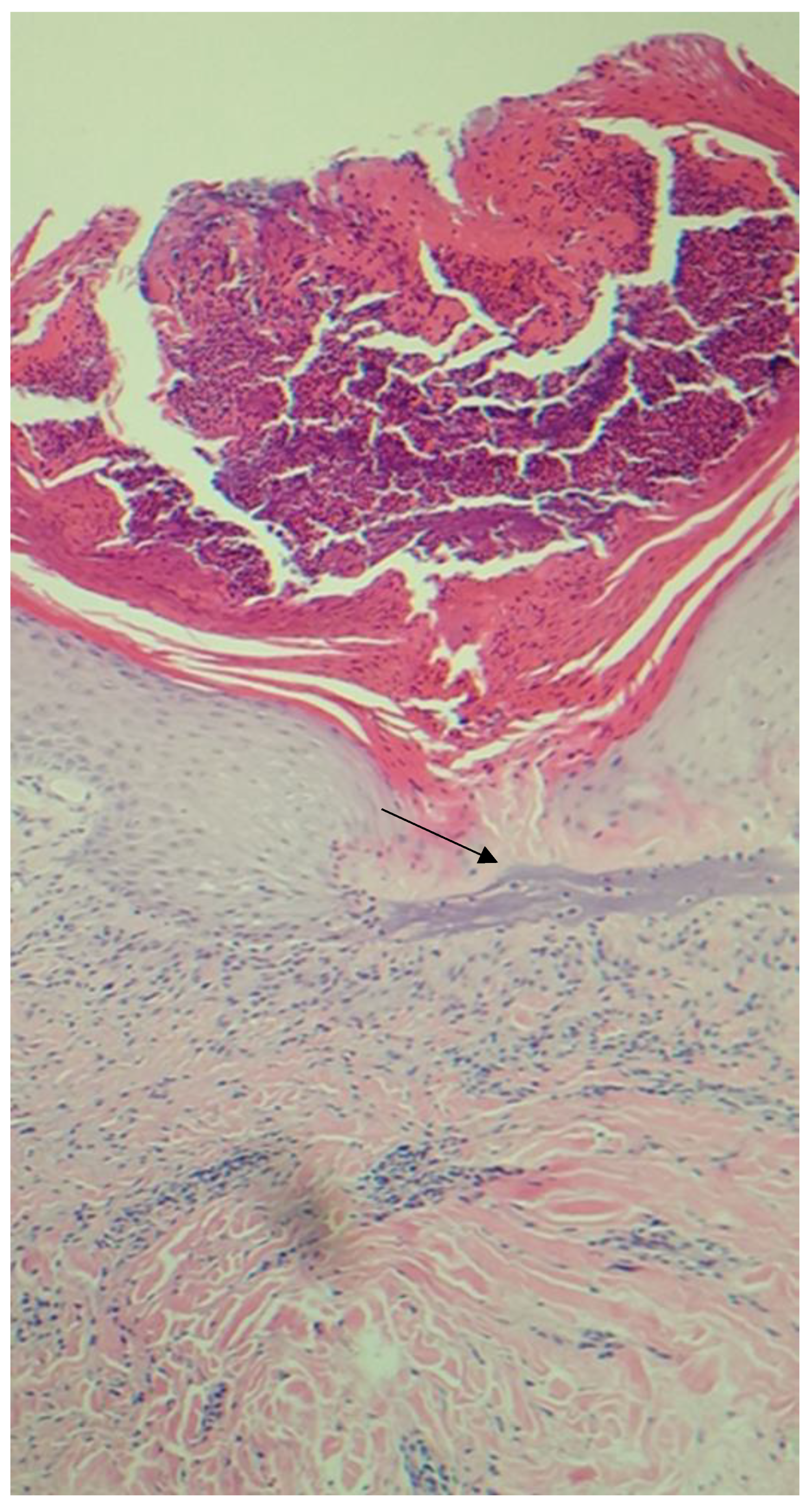
2. Case Report
3. Discussion
3.1. Approach to Perforating Dermatoses
- Endogenous substances (e.g., collagen, elastin)
- Abnormal deposits (e.g., calcium, mucin)
- Granulomatous disorders (e.g., sarcoid)
- Cellular elimination (e.g., nevus)
3.2. Review of Recent Literature
4. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


References
- Woo, T.Y.; Rasmussen, J.E. Disorders of Transepidermal Elimination. Int. J. Dermatol. 1985, 24, 337–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngan, V.; Tai, A. Peter MacCallum Sarah Smithson. (2022, April). Kyrle Disease. Available online: https://dermnetnz.org/topics/kyrle-disease (accessed on 20 May 2022).
- Rapini, R.P.; Hebert, A.A.; Drucker, C.R. Acquired perforating dermatosis: Evidence for combined transepidermal elimination of both collagen and elastic fibers. Arch. Dermatol. 1989, 125, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Sutton, L.; Parekh, P. Perforating gout of the ear. Dermatol. Online J. 2016, 22, 13030. [Google Scholar] [CrossRef]
- Lucke, T.W.; Fallowfield, M.E.; Evans, A.; Lowe, J.G.; MacKie, R.M. Transepidermal elimination of urate-like crystals: A new perforating disorder? Br. J. Dermatol. 1999, 141, 310–314. [Google Scholar] [CrossRef]
- Park, J.; Kang, C.; Kim, S.; Park, J. A Case of Transepidermal Elimination in Gouty Tophus. Korean J. Dermatol. 1990, 28, 85–89. [Google Scholar]
- Cohen, P.R.; Schmidt, W.A.; Rapini, R.P. Chronic tophaceous gout with severely deforming arthritis: A case report with emphasis on histopathologic considerations. Cutis 1991, 48, 445–451. [Google Scholar]
- Gontijo, J.R.V.; Fernandes Júnior, F.; Pereira, L.B.; Pedrosa, M.S. Trauma-induced acquired reactive perforating collagenosis. An. Bras. Dermatol. 2021, 96, 392–393. [Google Scholar] [CrossRef]
- Quaade, A.S.; Zachariae, C.; Jørgensen, M.E.; Simonsen, A.B. Perforating Baker’s cyst mimicking cutaneous malignancy. JEADV Clin. Pract. 2022, 1, 436–437. [Google Scholar] [CrossRef]
- Gunawan, H.; Nursjamsi, N.C.D.; Achdiat, P.A.; Suwarsa, O. Reactive perforating leprosy: A rare case report of type 2 leprosy reaction. Int. J. Mycobacteriology 2020, 9, 451–453. [Google Scholar] [CrossRef]
- Garrido, P.M.; Queirós, C.; Borges-Costa, J.; Soares-Almeida, L.; Filipe, P. Acquired perforating dermatosis: Clinicopathologic study of a 10-year period at a tertiary teaching hospital. Int. J. Dermatol. 2020, 59, 445–450. [Google Scholar] [CrossRef]
- Gore Karaali, M.; Erdil, D.; Erdemir, V.A.; Gurel, M.S.; Koku Aksu, A.E.; Leblebici, C. Evaluation of clinicopathological and treatment characteristics of 80 patients with acquired perforating dermatosis. Dermatol. Ther. 2020, 33, e14465. [Google Scholar] [CrossRef]
- Zhang, H.; Chang, J.M. Reactive perforating collagenosis. Int. J. Dermatol. Venereol. 2019, 2, 62–64. [Google Scholar]
- Shah, H.; Tiwary, A.K.; Kumar, P. Transepidermal elimination: Historical evolution, pathogenesis and nosology. Indian J. Dermatol. Venereol. Leprol. 2018, 84, 753. [Google Scholar] [PubMed]
- Singhania, N.; Singhania, G.; Al-Rabadi, L. Acquired Reactive Perforating Collagenosis. Clin. Exp. Nephrol. 2020, 24, 1086–1087. [Google Scholar] [CrossRef]
- Wang, W.; Liao, Y.; Fu, L.; Kan, B.; Peng, X.; Lu, Y. Dermoscopy Features of Acquired Perforating Dermatosis Among 39 Patients. Front. Med. 2021, 8, 631642. [Google Scholar] [CrossRef] [PubMed]
- Sawant, S.; Gaikwad, N.; Hajirnis, K.; Vasani, R. Acquired perforating collagenosis: A clinico-pathological study of ten. Indian J. Pathol. Oncol. 2019, 6, 677–681. [Google Scholar] [CrossRef]
- Kochen, D.; Sohal, R.J.; Nat, A. Reactive Perforating Collagenosis; An Uncontrolled Pruritus That Left You Scratching Your Head. Cureus 2020, 12, e9175. [Google Scholar] [CrossRef]
- Catolico, G.A.I.C.; Ang-Tiu, C. Clinical and Histopathologic Features of Acquired Perforating Collagenosis: A Case Report. Acta Medica Philipp. 2020. [Google Scholar] [CrossRef]
- Elmas, Ö.F.; Kilitci, A.; Uyar, B. Dermoscopic patterns of acquired reactive perforating collagenosis. Dermatol. Pract. Concept. 2021, 11, e2020085. [Google Scholar] [CrossRef]
- Barit, J.V.J.G.; Lizarondo, F.P.J.; Cubillan, E.L.A. Clinicopathologic and Dermoscopic Features of Acquired Perforating Dermatosis: A Case Report. Acta Medica Philipp. 2019, 53. [Google Scholar] [CrossRef]
- Kollipara, H.; Satya, R.S.; Rao, G.R.; Attili, S.K. Acquired Reactive Perforating Collagenosis: Case Series. Indian Dermatol. Online J. 2023, 14, 72–76. [Google Scholar] [PubMed]
- Wang, C.; Liu, Y.H.; Wang, Y.X.; Zhang, J.Z.; Jin, J. Acquired reactive perforating collagenosis. Chin. Med. J. 2020, 133, 2119–2120. [Google Scholar] [CrossRef] [PubMed]
- Wilson, B.N.; Joseph, N.K.; Alhatem, A.; Karanfilian, K.M.; Behbahani, S.; Lambert, W.C. Dermatopathologic Signs of Systemic Disease I: Acquired Perforating Dermatosis and Kyrle Disease. Bettertogether 2020, 18, 301–303. [Google Scholar]
- Vaivadaitė, U.; Janonytė, U. A case report of acquired perforating dermatosis. In Proceedings of the Rīga Stradiņš University International Student Conference 2023 “Health and Social Sciences”(RSU-ISC), Riga, Latvia, 27–28 March 2023. [Google Scholar]
- Khan, A.A.; Javed, M.; Asif, M. Reactive Perforating Collagenosis; Dermatological Manifestation in a Patient with ESRD. Available online: https://pjmhsonline.com/2019/july_sep/pdf/713.pdf (accessed on 24 May 2023).
- Villela-Segura, U.; Miranda-Aguirre, A.I.; Estrada-Aguilar, L. Crateriform plaques in a patient with end-stage renal disease. The case of an acquired reactive perforating collagenosis. Nefrología (Engl. Ed.) 2020, 40, 358–360. [Google Scholar] [CrossRef]
- Akagun, T.; Oguz, I.D.; Usta, S.; Kabaday, H.O. Acquired Reactive Perforating Collagenosis in Patient with Diabetic Chronic Kidney Disease: A Case Report. Clin. Case Rep. Int. 2022, 6, 1312. [Google Scholar]
- Bejjanki, H.; Siroy, A.E.; Koratala, A. Reactive perforating collagenosis in end-stage renal disease: Not all that itches is uremic pruritis! Am. J. Med. 2019, 132, e658–e660. [Google Scholar] [CrossRef]
- Domingos, A.; Calças, R.; Carias, E.; Vidinha, J.; Guedes, A.M.; Santos, V.; Agostini, P.; Mendonça, F.I.; Neves, P.L. Acquired perforating dermatosis with associated complicated cellulitis and amputation in a hemodialysis patient. Clin. Nephrol. Case Stud. 2021, 9, 33. [Google Scholar] [CrossRef]
- Sari, A.R.P.; Puspitasari, M.; Soebono, H.; Trisnowati, N. Acquired Perforating Disorder: A Case with Multiple Underlying Diseases. Case Rep. Dermatol. 2022, 14, 107–111. [Google Scholar] [CrossRef]
- Khalidi, M.; Frikh, R.; Hjira, N.; Boui, M. Acquired perforating dermatosis in renal dialysis and diabetic patient: A case report. Our Dermatol Online 2021, 12, e40. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, Y.; Shao, S. Acquired reactive perforating collagenosis: A case report and review of the literature. Medicine 2020, 99, e20391. [Google Scholar] [CrossRef]
- Özçelik, S.; Doğan, Y.; Kılıç, A.; Lebe, B. Giant variant of acquired perforating dermatosis in a patient with diabetes mellitus. TURKDERM-Turk. Arch. Dermatol. Venereol. 2020, 54, 25–28. [Google Scholar] [CrossRef]
- Razmi, T.M.; Chatterjee, D.; Parsad, D. Giant variant of acquired reactive perforating collagenosis in diabetic nephropathy. Postgrad. Med. J. 2019, 95, 52–53. [Google Scholar] [CrossRef]
- Ambalathinkal, J.J.; Phiske, M.M.; Someshwar, S.J. Acquired reactive perforating collagenosis, a rare entity at an uncommon site. Indian J. Pathol. Microbiol. 2022, 65, 895. [Google Scholar]
- Ladouce, F.; Beltzung, F.; Soubrier, M. Perforating dermatosis in rheumatoid arthritis. Rheumatology 2022, 61, 468. [Google Scholar] [CrossRef]
- Deb, S.; Srirangan, S. P38 A rare case of rheumatoid arthritis with perforating collagenosis. Rheumatology 2020, 59 (Suppl. 2), keaa111-037. [Google Scholar] [CrossRef]
- Ikeda, T.; Mikita, N.; Furukawa, F.; Iwahashi, Y. A case of rheumatoid vasculitis with acquired reactive perforating collagenosis. Mod. Rheumatol. 2019, 29, 547–550. [Google Scholar] [CrossRef]
- Gan, T.S.; Voo, S.Y.M. Acquired reactive perforating collagenosis—A rare cutaneous manifestation of anti-MDA5 dermatomyositis. Indian J. Dermatol. 2022, 67, 207. [Google Scholar]
- Alenzi, F. Reactive perforating collagenosis and systemic lupus erythematosus: A rare case report. Medicine 2022, 101, e32138. [Google Scholar] [CrossRef] [PubMed]
- Andrade, M.N.; Alfaro, M.F.; Van Caester, L.; Rossello, V.E.; Gallerano, V.; Herrero, M.; Pereyra, S.B. Dermatosis perforante adquirida, presentación de casos en pacientes con neoplasias malignas Acquired perforating dermatosis, a report of cases in patients with malignant neoplasms. Vol. 49 Supl. 1 Septiembre 2021, 49, 1–5. [Google Scholar]
- Cestari, S.; Dehó, I.Z.; Tovo, R.; Marques, G.; Lírio, I.D.; Macedo, M. Acquired perforating dermatosis in the setting of hepatocellular carcinoma. JAAD Case Rep. 2021, 18, 89–93. [Google Scholar]
- Huseynova, L.; Akdogan, N.; Gököz, Ö.; Evans, S.E. Acquired reactive perforating collagenosis in association with prostate adenocarcinoma, chronic lymphocytic leukemia, and Graves’ disease. An. Bras. Dermatol. 2020, 95, 336–339. [Google Scholar] [CrossRef] [PubMed]
- Malajian, D.; Husain, S.; Gallitano, S. Perforating Papules in a Patient With Acute Myeloid Leukemia. JAMA Dermatol. 2019, 155, 846–847. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, I.; Wlodek, C.; Lamont, D. Interferon therapy causing perforating dermatosis. Clin. Exp. Dermatol. 2020, 45, 349–350. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, K.; Masunaga, T.; Tohyama, M.; Sayama, K. A case of perforating folliculitis induced by vemurafenib. Acta Derm.-Venereol. 2019, 99, 230–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Song, T.T.; Hao, F. Erlotinib-induced reactive perforating collagenosis in a case of lung adenocarcinoma. Indian J. Dermatol. Venereol. Leprol. 2021, 87, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, H.; Wan, Y.; Guo, Y.; Shan, S.J. Acquired Perforating Dermatosis Induced by PD-1 Inhibitor: A Case Report. Am. J. Dermatopathol. 2021, 43, 942–944. [Google Scholar] [CrossRef]
- Tan, Q.; Liu, L.; Zhang, J.; Ni, S.L. Acquired Reactive Perforating Collagenosis Associated with Linear Immunoglobulin A Bullous Disease. Acta Derm.-Venereol. 2020, 100, adv00268. [Google Scholar] [CrossRef]
- Schauer, F.; Kern, J.S.; Virtic, O.; Technau-Hafsi, K.; Meiss, F.; Thoma, K.; Athanasiou, I.; Sitaru, C.; Di Zenzo, G.; Izumi, K.; et al. A new clinical variant of acquired reactive perforating dermatosis-like bullous pemphigoid. Br. J. Dermatol. 2019, 180, 231–232. [Google Scholar] [CrossRef]
- Oka, M. Localized Bullous Pemphigoid in a Patient with Acquired Reactive Perforating Collagenosis. Case Rep. Dermatol. 2023, 15, 1–4. [Google Scholar] [CrossRef]
- Lo, Y.P.; Snehal, D.; Deng, L.H.; Chang, C.H.; Shih, C.J. Successful treatment of acquired reactive perforating collagenosis induced by pregnancy with allopurinol: A case report with review of literature. Dermatol. Sin. 2019, 37, 162. [Google Scholar]
- Lavery, M.J.; Winters, S.; Lorenzelli, D.; Low, S.E.; Sharma, N.; Ngan, K. Acquired reactive perforating collagenosis in association with pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 253, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Grube, V.L.; Safeer, L.Z.; Hafeez, F. Acquired Reactive Perforating Collagenosis Occurring in Association With Nonred Ink Tattoo. Am. J. Dermatopathol. 2022, 44, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Ren, W.; Wang, M.; Li, X.; Pan, M. Acquired reactive perforating collagenosis combined with MRSA: A case report. Med. Int. 2023, 3, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.A.; Quan, V.L.; Colavincenzo, M.L.; Zheng, L. Acquired perforating dermatosis in patients with copper deficiency. JAAD Case Rep. 2021, 15, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Rajan, A.; Pai, V.V.; Shukla, P. Perforating folliculitis in Down’s syndrome—A rare case report. Egypt. J. Dermatol. Venerol. 2022, 42, 73. [Google Scholar] [CrossRef]
- Wang, F.Y.; Ng, C.Y.; Wu, J.; Kuo, K.L.; Chang, Y.Y.; Kuo, T.T. Acquired perforating calcific collagenosis in a drug addict with rhabdomyolysis and transient hypercalcemia. J. Cutan. Pathol. 2019, 46, 84–87. [Google Scholar] [CrossRef] [Green Version]
- Dheeraj, D.S.; Devi, B.G.; Gopal, K.V.T.; RAO, T.N. Reactive Perforating Collagenosis in Two Siblings—A Rare Case Presentation. IOSR J. Dent. Med. Sci. 2020, 19, 47–50. [Google Scholar]
- McMichael, J.; Stoff, B.K. Treatment of a perforating dermatosis with apremilast. JAAD Case Rep. 2021, 16, 155–157. [Google Scholar] [CrossRef]
- Kharghoria, G.; Grover, C. Treatment of acquired perforating dermatosis with colchicine. Indian Dermatol. Online J. 2022, 13, 131–132. [Google Scholar]
- Mattos, A.B.N.D.; Brummer, C.F.; Funchal, G.D.G.; Nunes, D.H. Perforating necrobiosis lipoidica: Good response to adalimumab. An. Bras. Dermatol. 2020, 94, 769–771. [Google Scholar] [CrossRef]
- Gao, L.; Gu, L.; Chen, Z.; Cao, S. Doxycycline combined with NB-UVB phototherapy for acquired reactive perforating collagenosis. Ther. Clin. Risk Manag. 2020, 16, 917–921. [Google Scholar] [CrossRef]
- Guo, L.; Zeng, Y.P.; Jin, H.Z. Reactive perforating collagenosis treated with dupilumab: A case report and literature review. Dermatol. Ther. 2022, 35, e15916. [Google Scholar] [CrossRef] [PubMed]
- Alsebayel, M.M.; Alzaid, T.; Alobaida, S.A. Dupilumab in acquired perforating dermatosis: A potential new treatment. JAAD Case Rep. 2022, 28, 34–36. [Google Scholar] [CrossRef]
- Izzat, M.B.; Kahila, A.; Izzat, A.W.; Zamlout, A.; Alashi, S. Uncharted surgical therapy for acquired perforating dermatoses. Asian Cardiovasc. Thorac. Ann. 2023, 31, 148–150. [Google Scholar] [CrossRef]
- Ye, B.; Cao, Y.; Liu, Y. Successful treatment of acquired reactive perforating collagenosis with itraconazole. Eur. J. Med. Res. 2021, 26, 74. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.F.; Mei, X.L.; Wang, L.; Li, L.F. Clinical characteristics and prognosis of acquired perforating dermatosis: A case report. Exp. Ther. Med. 2020, 19, 3634–3640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil, F.; Cardoso, J.C.; Gil, J. Successful treatment of acquired perforating dermatosis with colchicine. Indian Dermatol. Online J. 2021, 12, 355. [Google Scholar] [CrossRef]
- Eljazouly, M.; Alj, M.; Chahboun, F.; Chahdi, H.; Chiheb, S.; Chahdi Sr, H. Acquired reactive perforating collagenosis: A case report. Cureus 2021, 13, e13583. [Google Scholar] [CrossRef]
- Gil-Lianes, J.; Riquelme-Mc Loughlin, C.; Mascaró, J.M., Jr. Reactive perforating collagenosis successfully treated with dupilumab. Australas. J. Dermatol. 2022, 63, 398. [Google Scholar] [CrossRef]
- Kawakami, T.; Akiyama, M.; Ishida-Yamamoto, A.; Nakano, H.; Mitoma, C.; Yoneda, K.; Suga, Y. Clinical practice guide for the treatment of perforating dermatosis. J. Dermatol. 2020, 47, 1374–1382. [Google Scholar] [CrossRef]
- Pap, N.; Bradamante, M.; Ljubojević-Hadžavdić, S. Localized perforating granuloma annulare. Acta Dermatovenerol. Croat. 2019, 27, 33. [Google Scholar]
- Deza, G.; Vidal, A.; Gallardo, F.; Iranzo, P.; de la Iglesia, L.C.; Pujol, R.M. Generalized Necrobiotic Palisading Granulomatous Follicular Eruption: A Peculiar Pustular Variant of Perforating Granuloma Annulare or an Individualized Disease? Am. J. Dermatopathol. 2020, 42, e22–e25. [Google Scholar] [CrossRef]
- Karadag, A.S.; Uzuncakmak, T.K.; Zemheri, E.I.; Arikan, E.E.; Ozkanli, S.; Akdeniz, N. Perforating Granuloma Annulare: A Case Report/Perforan Granuloma Annulare: Olgu Sunumu. Dermatoz 2020, 11, 21–24. [Google Scholar] [CrossRef]
- Maghfour, S.; El Abed, Y.H.; Gammoudi, R.; Boussofara, L.; Aouinallah, A.; Mokni, S.; Ghariani, N.; Belajouza, C.; Denguezli, M. Perforating necrobiosis lipoidica: A new case report. Endocr. Abstr. Biosci. 2019, 63, 886. [Google Scholar] [CrossRef]
- Gori, N.; Di Stefani, A.; De Luca, E.V.; Peris, K. A case of disseminated perforating necrobiosis lipoidica. Clin. Case Rep. 2020, 8, 808–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Chen, K.R. Perforating plaque-type pretibial sarcoidosis with granulomatous phlebitis. Am. J. Dermatopathol. 2020, 42, 225–226. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, H.T.; Chaturvedi, C.; Thammaiah, S.; Patel, V. Transepidermal elimination of suture material in lip biopsy specimen. J. Oral Maxillofac. Pathol. JOMFP 2022, 26, 392. [Google Scholar] [CrossRef]
- Bathina, M.; Hegde, S.P.; Shanavaz, A.A.; Saldanha, P.P. Pruritic periumbilical plaque as a presentation of a rare perforating dermatosis. Indian Dermatol. Online J. 2020, 11, 68. [Google Scholar] [PubMed]
- Mehta, P.; Rana, A. Periumbilical Perforating Pseudoxanthoma Elasticum/PPPXE—A Rare Case Report. J. Med. Sci. Clin. Res. 2021, 9. [Google Scholar] [CrossRef]
- Zhang, Y.; Feng, L.; Wang, M.; Wang, L. Perforating pseudoxanthoma elasticum of the arms: A rare case report. Eur. J. Dermatol. 2020, 30, 731–732. [Google Scholar]
- Watabe, D.; Mori, S.; Akasaka, T.; Motegi, S.I.; Ishikawa, O.; Amano, H. Six cases of perforating pilomatricoma: Anetodermic changes with expression of matrix metalloproteinases. J. Dermatol. 2020, 47, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Iinuma, S.; Takahashi, C.; Hayashi, K.; Ishida-Yamamoto, A. Perforating pilomatricoma presenting as a cutaneous horn in a patient with myotonic dystrophy. Eur. J. Dermatol. 2022, 32, 284–285. [Google Scholar] [PubMed]
- Endo, M.; Yamamoto, T. A case of multiple perforating pilomatricomas. An. Bras. Dermatol. 2022, 97, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Erdoğan, O. Sialolithiasis perforating the floor of mouth: A case report. Mucosa 2022, 5, 59–62. [Google Scholar] [CrossRef]
- Sikkerimath, S.; Anshu, A.; Jose, A. Perforating Sialolith: A Case Report. Asian J. Dent. Sci. 2020, 3, 12–15. [Google Scholar]
- LeWitt, T.; Quan, V.L.; Yazdan, P.; Zhou, X.A. Perforating lichen nitidus. JAAD Case Rep. 2021, 8, 4–8. [Google Scholar] [CrossRef]
- Li, X.Q.; Chen, X.; Li, B.; Du, J.; Hong, Y.S.; Zhang, J.Z.; Zhou, C. Dermoscopy of perforating lichen nitidus: A case report. Chin. Med. J. 2020, 133, 2135–2136. [Google Scholar] [CrossRef]
- Zipperer, K.; Munoz, A.; Kelly, E.; Goodwin, B. Acquired Perforating Osteoma Cutis: A Rare Histopathological Diagnosis. Am. J. Dermatopathol. 2022, 10, 1097. [Google Scholar] [CrossRef]
- Wee, C.L.P.; Lim, J.H.L.; Lee, J.S.S. Cryocrystalglobulinemia—An Uncommon Cutaneous Presentation of Multiple Myeloma and Novel Finding of Transepidermal Elimination of Crystals. Am. J. Dermatopathol. 2021, 43, e241–e244. [Google Scholar] [CrossRef]
- Jordaan, H.F. Transepidermal elimination in exogenous ochronosis: A report of two cases. Am. J. Dermatopathol. 1991, 13, 418–424. [Google Scholar] [CrossRef]
- Ziani, J.; Baybay, H.; Bennani, M.; Douhi, Z.; Elloudi, S.; Mernissi, F.Z. Perforating Granuloma Annulare in Children: A Case Report. Available online: https://www.oatext.com/perforating-granuloma-annulare-in-children-a-case-report.php#Article (accessed on 24 May 2023).
- Smith, C.; Hamilton, D.; Waterston, S. Rare case of multiple and perforating pilomatrixomas in a young girl with lymphovascular malformation reveals a potential new disease association. BMJ Case Rep. CP 2022, 15, e248076. [Google Scholar] [CrossRef] [PubMed]
- Aizman, L.; Gelman, A.; Marathe, K. A case of verrucous perforating collagenoma in a toddler. Pediatr. Dermatol. 2019, 36, 739–740. [Google Scholar] [CrossRef] [PubMed]
- Witkoff, B.M.; Ivanov, N.N.; Trotter, S.C. Perforating granuloma annulare appearing as a psoriasiform lesion. Case Rep. Dermatol. 2019, 11, 233. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.S.; Krenek, G.; Tschen, J. Perforating granuloma annulare mimicking psoriasis. Cureus 2020, 12, e9983. [Google Scholar] [CrossRef]
- Seo, B.H.; Kim, J.H.; Oh, Y.W.; Kim, D.H.; Suh, H.S.; Choi, Y.S. P338: A case of perforating pilomatricoma mimicking intradermal nevus on the scalp. 프로그램북 (구 초록집) 2019, 71, 485–486. [Google Scholar]
- De Silva, L.; Lokuhetty, M.S. Giant variant of acquired perforating dermatosis, clinically masquerading as a sarcoma: A report of a rare case. Indian J. Pathol. Microbiol. 2020, 63, 128. [Google Scholar] [CrossRef]
- Ornetti, P.; Guillier, D.; Jeudy, G. Perforating Rheumatoid Nodule Mimicking Malignant Soft-tissue Mass of the Forearm. J. Rheumatol. 2021, 48, 1103. [Google Scholar] [CrossRef]
- Kossard, S. Eruptive necrotizing infundibular crystalline folliculitis: An expression of an abortive sebaceous follicular repair pathway linked to committed infundibular stem cells? Am. J. Dermatopathol. 2021, 43, 867. [Google Scholar] [CrossRef]
- Wiedemeyer, K.; Brenn, T.; Naert, K. Necrotizing Infundibular Crystalline Folliculitis—A Case Report of a Rare Entity and Review of the Literature. Am. J. Dermatopathol. 2022, 10, 1097. [Google Scholar] [CrossRef]
- Fischer, A.S.; Pei, S.; Shields, B.E.; Rosenbach, M.; Rubin, A.I. Dermatomal necrotizing infundibular crystalline folliculitis following herpes zoster in a patient on PD-1 inhibitor therapy. J. Cutan. Pathol. 2020, 47, 501–505. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Primary | ||
|---|---|---|
| Source | Disease | TE Material |
| Endogenous material | Elastosis perforans serpiginosa | Elastin |
| Reactive perforating collagenosis | Collagen | |
| Kyrle’s disease | Keratin and other material | |
| Perforating folliculitis | Elastin and/or Collagen | |
| Acquired perforating dermatosis | Umbrella term for the entities listed above | |
| Secondary | ||
| Source | Disease | TE Material |
| Abnormal endogenous material | Chondrodermatitis nodularis helicis | Degraded cartilage |
| Perforating pseudoxanthoma elasticum | Abnormal elastin | |
| Perforating osteoma cutis | Ectopic bone | |
| Perforating calcinosis cutis | Ectopic calcium | |
| Perforating calcific collagenosis | Calcified collagen | |
| Perforating calcific elastosis | Calcified elastin | |
| Deposits | Perforating mucinosis | Mucin |
| Perforating amyloidosis | Amyloid | |
| Perforating cryocrystalglobulinemia | Cryocrystalglobulins | |
| Infection with deposits | Botryomycosis | Extra-bacterial granule |
| Granulomas | Perforating granuloma annulare | Necrobiotic granulomas with mucin |
| Perforating necrobiosis lipoidica | necrobiotic granulomas | |
| Perforating sarcoidosis | Sarcoidal granulomas | |
| Perforating rheumatoid nodule | Granuloma, fibrinoid | |
| Perforating foreign body | Foreign body granulomas and foreign material | |
| Perforating tattoo reaction | Granulomatous inflammation with tattoo pigment | |
| Perforating ochronosis | Granulomatous inflammation with homogentisic acid | |
| Perforating gout | Granulomatous inflammation with monosodium urate | |
| Granulomatous Infections | Schistosomiasis | Granulomatous inflammation |
| Chromomycosis | Granulomatous inflammation | |
| Tuberculosis | Granulomas | |
| Leprosy | Granulomas | |
| Leishmaniasis | Granulomatous inflammation | |
| Histoplasmosis | Granulomatous inflammation | |
| Other | Lichen nitidus | Inflammatory cells |
| Melanoma | Melanocytes | |
| Nevus | Melanocytes | |
| Pilomatricoma | abnormal immature keratinocytes | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bohdanowicz, M.; Bradshaw, S.H. Perforating Gout: Expanding the Differential for Transepidermal Elimination. Dermatopathology 2023, 10, 207-218. https://doi.org/10.3390/dermatopathology10030029
Bohdanowicz M, Bradshaw SH. Perforating Gout: Expanding the Differential for Transepidermal Elimination. Dermatopathology. 2023; 10(3):207-218. https://doi.org/10.3390/dermatopathology10030029
Chicago/Turabian StyleBohdanowicz, Michal, and Scott H. Bradshaw. 2023. "Perforating Gout: Expanding the Differential for Transepidermal Elimination" Dermatopathology 10, no. 3: 207-218. https://doi.org/10.3390/dermatopathology10030029