
Psychophysical and Social Functioning of Patients with Chronic Obstructive Lung Disease and Depression
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.2.1. Pulmonary Obstruction and Dyspnea
2.2.2. Depression
2.2.3. Quality of Life
2.3. Ethics Statements
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Psychophysical and Social Functioning of Subjects in the Study
3.2.1. Quality of Life before and after Medication
3.2.2. Level of Depression and Quality of Life
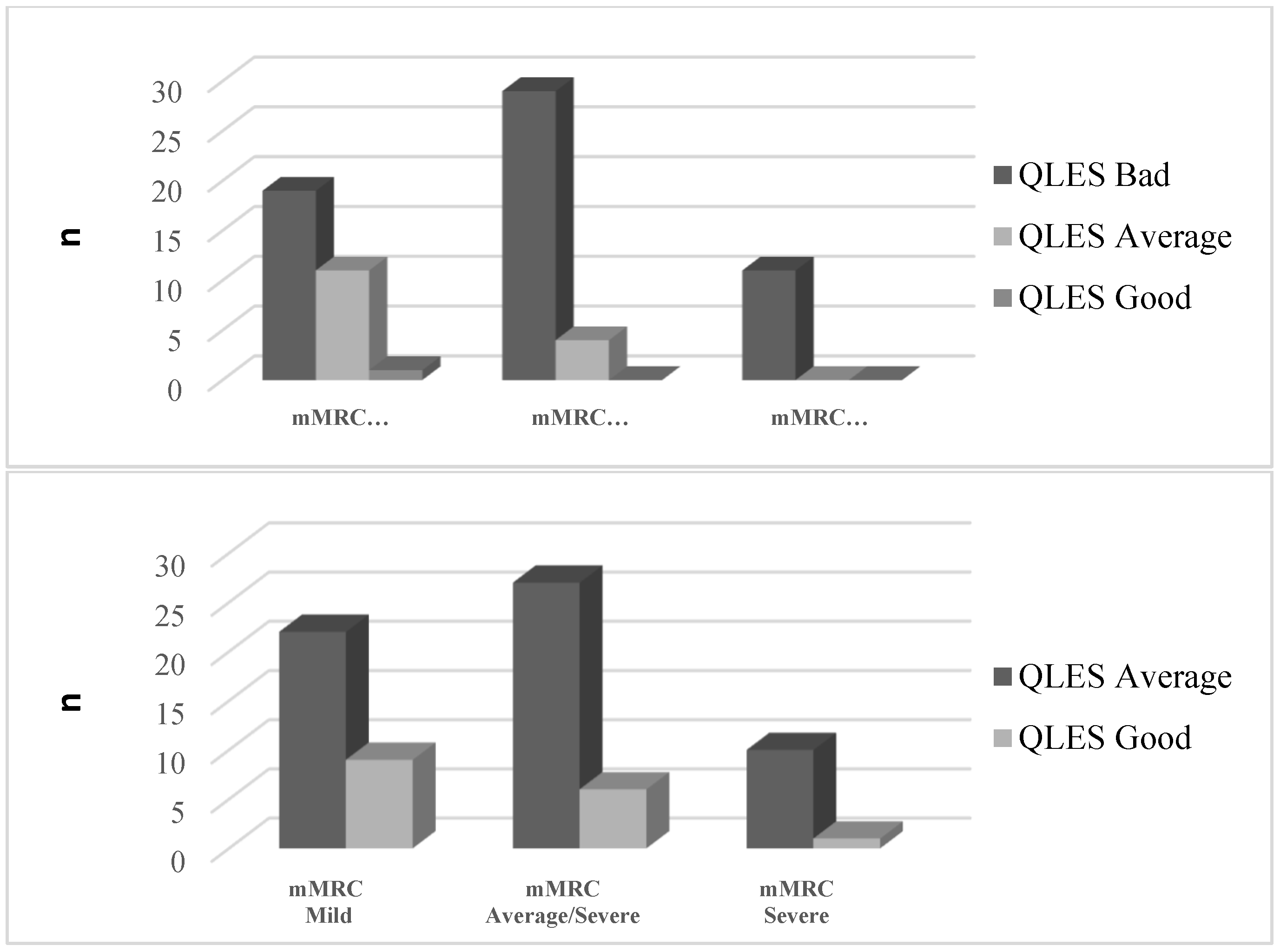
3.2.3. Improvements in Single Domains of Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: 2023 Report; WHO: Geneva, Switzerland, 2023. [Google Scholar]
- World Health Organization. Chronic Obstructive Pulmonary Disease (COPD); WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Zou, J.; Sun, T.; Song, X.; Liu, Y.-M.; Lei, F.; Chen, M.-M.; Chen, Z.; Zhang, P.; Ji, Y.-X.; Zhang, X.-J.; et al. Distributions and trends of the global burden of COPD attributable to risk factors by SDI, age, and sex from 1990 to 2019: A systematic analysis of GBD 2019 data. Respir. Res. 2022, 23, 90. [Google Scholar] [CrossRef]
- Barnes, P.J.; Celli, B.R. Systemic manifestations and comorbidities of COPD. Eur. Respir. J. 2009, 33, 1165–1185. [Google Scholar] [CrossRef]
- Gan, W.Q.; Man, S.F.; Senthilselvan, A.; Sin, D.D. Association between chronic obstructive pulmonary disease and systemic inflammation: A systematic review and a meta-analysis. Thorax 2004, 59, 574–580. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Milne, K.M.; James, M.D.; de Torres, J.P.; Neder, J.A. Dyspnea in COPD: New Mechanistic Insights and Management Implications. Adv. Ther. 2020, 37, 41–60. [Google Scholar] [CrossRef] [PubMed]
- Basara, L.; Jokic Begic, N.; Popovic, S.; Jakopovic, M.; Samardzija, M. Dyspnea from neuropsychiatric perspective: A narrative review. Psychiatr. Danub. 2018, 30, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Currow, D.C.; Chang, S.; Reddel, H.K.; Kochovska, S.; Ferreira, D.; Kinchin, I.; Johnson, M.; Ekström, M. Breathlessness, Anxiety, Depression, and Function–The BAD-F Study: A Cross-Sectional and Population Prevalence Study in Adults. J. Pain Symptom Manag. 2020, 59, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Postolache, P.; Costin, M.; Dumbravă, E.L.; Cojocaru, D.C. Anxiety and depression in patients with chronic obstructive pulmonary disease: An open agenda for research. Rev. Med. Chir. Soc. Med. Nat. Iasi 2014, 118, 39–44. [Google Scholar] [PubMed]
- Di Marco, F.; Verga, M.; Reggente, M.; Casanova, F.M.; Santus, P.; Blasi, F.; Allegra, L.; Centanni, S. Anxiety and depression in COPD patients: The roles of gender and disease severity. Respir. Med. 2006, 100, 1767–1774. [Google Scholar] [CrossRef]
- Van Manen, J.G.; Bindels, P.J.; Dekker, F.W.; IJzermans, C.J.; van der Zee, J.S.; Schadé, E. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Thorax 2020, 57, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef]
- Lacasse, Y.; Rousseau, L.; Maltais, F. Prevalence of depressive symptoms and depression in patients with severe oxygen-dependent chronic obstructive pulmonary disease. J. Cardiopulm. Rehabil. 2001, 21, 80–86. [Google Scholar] [CrossRef]
- Hill, K.; Geist, R.; Goldstein, R.S.; Lacasse, Y. Anxiety and depression in end-stage COPD. Eur. Respir. J. 2008, 31, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Maurer, J.; Rebbapragada, V.; Borson, S.; Goldstein, R.; Kunik, M.E.; Yohannes, A.M.; Hanania, N.A. Anxiety and Depression in COPD. Chest 2008, 134, 43S56S. [Google Scholar] [CrossRef] [PubMed]
- Dalal, A.A.; Shah, M.; Lunacsek, O.; Hanania, N.A. Clinical and Economic Burden of Depression/Anxiety in Chronic Obstructive Pulmonary Disease Patients within a Managed Care Population. COPD J. Chronic Obstr. Pulm. Dis. 2011, 8, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Rahi, M.S.; Thilagar, B.; Balaji, S.; Prabhakaran, S.Y.; Mudgal, M.; Rajoo, S.; Yella, P.R.; Satija, P.; Zagorulko, A.; Gunasekaran, K. The Impact of Anxiety and Depression in Chronic Obstructive Pulmonary Disease. Adv. Respir. Med. 2023, 91, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Jelic, I.; Folic, M.; Mihajlovic, F.; Jankovic, S.; Mihajlovic, G. The Effects of Antidepressant Therapy on Health-Related Quality of Life in Patients with a Chronic Obstructive Pulmonary Disease and Depressive Symptoms. Exp. Appl. Biomed. Res. (EABR) 2022. [Google Scholar] [CrossRef]
- Pollok, J.; van Agteren, J.E.M.; Carson, C.K.V. Pharmacological interventions for the treatment of depression in chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2018, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Kulić, L.; Vujović, M.; Krstović-Spremo, V.; Jovanović, J.; Jovanović, J. Examination of the impact of use of invasive cardiological procedures on quality of life of patients suffering from myocardial infarction. Zdr. Zaštita 2019, 48, 8–14. [Google Scholar] [CrossRef]
- Higginson, I.J.; Carr, A.J. Using quality of life measures in the clinical setting. BMJ 2001, 322, 1297–1300. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2021 Report; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the medical research council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Jelić, I.; Mihajlović, G.; Mihajlović, F.; Minić, N.; Ratinac, M.; Pantović-Stefanović, M. COPD and Depression Analysis In Regard to Obstructive Pulmonary Levels. Healthcare 2023, 11, 1175. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- American Psychological Association. Depression Assessment Instruments; APA: Washington, DC, USA, 2023. [Google Scholar]
- Farag, T.S.; Sobh, E.S.; Elsawy, S.B.; Fahmy, B.M. Evaluation of health-related quality of life in patients with chronic obstructive pulmonary disease. Egypt. J. Bronchol. 2018, 12, 288–294. [Google Scholar] [CrossRef]
- Hobart, M.; Zhang, P.; Weiss, C.; Meehan, S.R.; Eriksson, H. Adjunctive brexpiprazole and functioning in major depressive disorder: A pooled analysis of six randomized studies using the Sheehan Disability Scale. Int. J. Neuropsychopharmacol. 2019, 22, 173–179. [Google Scholar] [CrossRef]
- Morton, E.; Bhat, V.; Giacobbe, P.; Lou, W.; Michalak, E.E.; McInerney, S.; Chakrabarty, T.; Frey, B.N.; Milev, R.V.; Müller, D.J.; et al. Predictors of Quality of Life Improvement with Escitalopram and Adjunctive Aripiprazole in Patients with Major Depres-sive Disorder: A CAN-BIND Study Report. CNS Drugs 2021, 35, 439–450. [Google Scholar] [CrossRef]
- Denton, M.; Walters, V. Gender differences in structural and behavioral determinants of health: An analysis of the social pro-duction of health. Soc. Sci. Med. 1999, 48, 1221–1235. [Google Scholar] [CrossRef]
- Maharaj, S.; Lees, T.; Lal, S. Prevalence and risk factors of depression, anxiety, and stress in a cohort of Australian nurses. Int. J. Environ. Res. Public Health 2019, 16, 61. [Google Scholar] [CrossRef]
- Gupta, S.; Verma, H.V. Mindfulness, mindful consumption, and life satisfaction: An experiment with higher education students. J. Appl. Res. High. Educ. 2020, 12, 456–474. [Google Scholar] [CrossRef]
- Solé, B.; Verdolini, N.; Amoretti, S.; Montejo, L.; Rosa, A.R.; Hogg, B.; Garcia-Rizo, C.; Mezquida, G.; Bernardo, M.; Martinez-Aran, A.; et al. Effects of the COVID-19 pandemic and lockdown in Spain: Comparison between community controls and pa-tients with a psychiatric disorder. Preliminary results from the BRIS-MHC STUDY. J. Affect. Disord. 2021, 281, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.U.; Park, C.K.; Kim, T.H.; Jang, A.S.; Park, Y.B.; Rhee, C.K.; Jung, K.S.; Yoo, K.H.; Lee, W.Y.; Yoon, H.K. The difficulty of improving quality of life in COPD patients with depression and associated factors. Int. J. Chron. Obs. Pulmon. Dis. 2019, 14, 2331–2341. [Google Scholar] [CrossRef] [PubMed]
- Martinez Rivera, C.; Costan Galicia, J.; Alcázar Navarrete, B.; Garcia-Polo, C.; Ruiz Iturriaga, L.A.; Herrejón, A.; Ros Lucas, J.A.; García-Sidro, P.; Tirado-Conde, G.; López-Campos, J.L.; et al. Factors associated with depression in COPD: A multicenter study. Lung 2016, 194, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Fan, V.S.; Ramsey, S.D.; Giardino, N.D.; Make, B.J.; Emery, C.F.; Diaz, P.T.; Benditt, J.O.; Mosenifar, Z.; McKenna, R.; Curtis, J.L.; et al. Sex, depression, and risk of hospitalization and mortality in chronic obstructive pulmonary disease. Arch. Intern. Med. 2007, 167, 2345–2353. [Google Scholar] [CrossRef] [PubMed]
- Cafarella, P.A.; Effing, T.W.; Usmani, Z.A.; Frith, P.A. Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: A literature review. Respirology 2012, 17, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Pekmezovic, T.; Popovic, A.; Kisic Tepavcevic, D.; Gazibara, T.; Paunic, M. Factors associated with health-related quality of life among Belgrade University students. Qual. Life Res. 2011, 20, 391–397. [Google Scholar] [CrossRef]
- LaGrant, B.; Marquis, B.O.; Berg, A.T.; Grinspan, Z.M. Depression and anxiety in children with epilepsy and other chronic health conditions: National estimates of prevalence and risk factors. Epilepsy Behav. 2020, 103, 106828. [Google Scholar] [CrossRef]
- Gray, C.; Ambady, L.; Chao, S.; Smith, W.; Yoon, J. Virtual Management of Chronic Conditions During the COVID-19 Pandemic: Insights From Primary Care Providers and Clinical Pharmacists. Mil. Med. 2022, 188, e2615–e2620. [Google Scholar] [CrossRef]
- Balcells, E.; Gea, J.; Ferrer, J.; Serra, I.; Orozco-Levi, M.; de Batlle, J.; Rodriguez, E.; Benet, M.; Donaire-González, D.; Antó, J.M.; et al. Factors affecting the relationship between psychological status and quality of life in COPD patients. Health Qual. Life Outcomes 2010, 8, 108. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Group | % (N) | Mean | SD | F/Cohen’s d/p * |
|---|---|---|---|---|---|
| Age | Male | 34.84% (30) | 47.614 | 7.311 | 0.115/−0.489/0.033 |
| Female | 65.52% (57) | 51.167 | 7.206 | ||
| Variable | Group | All % (N) | Male % (N) | Female % (N) | χ2/p ** |
| HAM-D1 | 1 | 40.2% (35) | 33.3% (10) | 43.9% (25) | 3.282/0.194 |
| 2 | 48.3% (42) | 46.7% (14) | 49.1% (28) | ||
| 3 | 11.5% (10) | 20.0% (6) | 7.0% (4) | ||
| HAM-D2 | 0 | 37.9% (33) | 30.0% (9) | 42.1% (24) | 4.337/0.261 |
| 1 | 49.4% (43) | 50.0% (15) | 49.1% (28) | ||
| 2 | 12.6% (11) | 20.0% (6) | 8.8% (5) | ||
| mMRC | 1 | 37.9% (33) | 30.0% (9) | 42.1% (34) | 4.672/0.099 |
| 2 | 51.7% (45) | 50.0% (15) | 52.6% (30) | ||
| 3 | 10.5% (9) | 20.0% (6) | 5.3% (3) |
| mMRC | Q-LES-Q-SF after | Male | Female | ||||
|---|---|---|---|---|---|---|---|
| Q-LES-Q-SF Scores before 8 Weeks Therapy | Q-LES-Q-SF Scores before 8 Weeks Therapy | ||||||
| Bad n (%) | Average * n (%) | Good n (%) | Bad n (%) | Average * n (%) | Good n (%) | ||
| 1 | Average * | 5 (35.7) | - | - | 14 (50) | 3 (1) | - |
| Good | - | 3 (64.3) | - | 2 (6.7) | 9 (30) | 1 (3.3) | |
| 2 | Average * | 9 (90) | - | - | 19 (90.2) | - | - |
| Good | - | 2 (10) | - | 1 (2.5) | 4 (7.3) | - | |
| 3 | Average * | 11 (100) | - | - | 4 (100) | - | - |
| Good | - | - | - | - | - | - | |
| Variable | Mean ± SD | Z/η2/p * |
|---|---|---|
| HAM-D1 score before SSRI therapy | 21.79 ± 4.43 | −9.528/1.043/ <0.001 |
| HAM-D2 score after 8 weeks of SSRI therapy | 13.02 ± 3.97 | |
| Q-LES-Q-SF score before AD | 37.30 ± 3.31 | −8.191/0.771/ <0.001 |
| Q-LES-Q-SF score after AD | 45.07 ± 2.47 | |
| Difference in Q-LES-Q-SF score (after-before) | 7.42 ± 1.64 |
| Study Period | Ability to Function in Daily Life Median (IQR) | Physical Health Median (IQR) | Life Satisfaction Median (IQR) | Relationship to Family Median (IQR) |
|---|---|---|---|---|
| Baseline | 2 (0) | 2 (1) | 2 (0) | 3 (0) |
| After 8 weeks | 3 (0) | 3 (1) | 3 (0) | 3 (1) |
| Z/η2/p * | −8.062/0.747/<0.001 | −8.442/0.819/<0.001 | −8.885/0.908/<0.001 | −2.236/0.057/0.060 |
| Q-LES-Q-SF | Females Median (IQR) | Males Median (IQR) | U/η2/p |
|---|---|---|---|
| Q-LES-Q-SF score before AD Q-LES-Q-SF score after AD | 37 (4) | 36 (2) | −2.865/0.675/0.042 |
| 47 (4) | 45 (2) | −2.563/0.674/0.040 | |
| Life satisfaction before AD Life satisfaction after AD | 3 (0) | 2 (0) | −3.225/0.676/0.027 |
| 3 (2) | 2 (1) | −2.963/0.675/0.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jelić, I.; Mihajlović, G.; Ratinac, M.; Mihajlović, K.; Mijailović, S.; Čekerevac, I. Psychophysical and Social Functioning of Patients with Chronic Obstructive Lung Disease and Depression. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2841-2852. https://doi.org/10.3390/ejihpe13120196
Jelić I, Mihajlović G, Ratinac M, Mihajlović K, Mijailović S, Čekerevac I. Psychophysical and Social Functioning of Patients with Chronic Obstructive Lung Disease and Depression. European Journal of Investigation in Health, Psychology and Education. 2023; 13(12):2841-2852. https://doi.org/10.3390/ejihpe13120196
Chicago/Turabian StyleJelić, Ivana, Goran Mihajlović, Miloš Ratinac, Katarina Mihajlović, Sara Mijailović, and Ivan Čekerevac. 2023. "Psychophysical and Social Functioning of Patients with Chronic Obstructive Lung Disease and Depression" European Journal of Investigation in Health, Psychology and Education 13, no. 12: 2841-2852. https://doi.org/10.3390/ejihpe13120196