


Challenges of Pharyngeal Cancer Screening in Lower-Income Countries during Economic and Social Transitions: A Population-Based Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethical Considerations and Approval
3. Results
3.1. Clinical Presentation
3.2. Histopathological Results
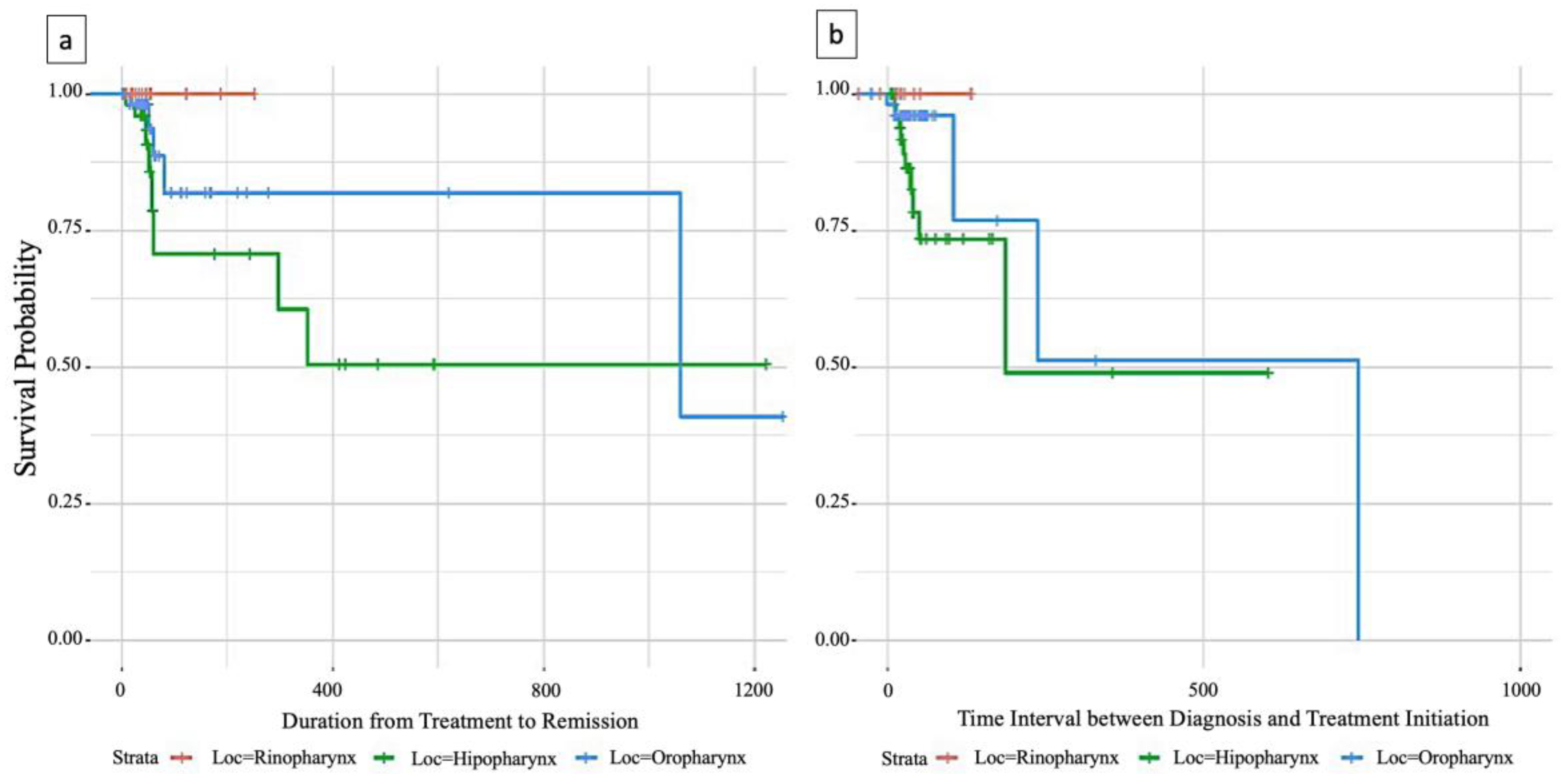
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef]
- Guha, N.; Boffetta, P.; Wünsch Filho, V.; Eluf Neto, J.; Shangina, O.; Zaridze, D.; Curado, M.P.; Koifman, S.; Matos, E.; Menezes, A.; et al. Oral health and risk of squamous cell carcinoma of the head and neck and esophagus: Results of two multicentric case-control studies. Am. J. Epidemiol. 2007, 166, 1159–1173. [Google Scholar] [CrossRef]
- Tsang, C.M.; Lui, V.W.Y.; Bruce, J.P.; Pugh, T.J.; Lo, K.W. Translational genomics of nasopharyngeal cancer. Semin. Cancer Biol. 2020, 61, 84–100. [Google Scholar] [CrossRef]
- Hashim, D.; Genden, E.; Posner, M.; Hashibe, M.; Boffetta, P. Head and neck cancer prevention: From primary prevention to impact of clinicians on reducing burden. Ann. Oncol. 2019, 30, 744–756. [Google Scholar] [CrossRef]
- Tuyns, A.J.; Estève, J.; Raymond, L.; Berrino, F.; Benhamou, E.; Blanchet, F.; Boffetta, P.; Crosignani, P.; del Moral, A.; Lehmann, W.; et al. Cancer of the larynx/hypopharynx, tobacco and alcohol: IARC international case-control study in Turin and Varese (Italy), Zaragoza and Navarra (Spain), Geneva (Switzerland) and Calvados (France). Int. J. Cancer 1988, 41, 483–491. [Google Scholar] [CrossRef]
- Freedman, N.D.; Park, Y.; Subar, A.F.; Hollenbeck, A.R.; Leitzmann, M.F.; Schatzkin, A.; Abnet, C.C. Fruit and vegetable intake and head and neck cancer risk in a large United States prospective cohort study. Int. J. Cancer 2008, 122, 2330–2336. [Google Scholar] [CrossRef]
- Pulte, D.; Brenner, H. Changes in survival in head and neck cancers in the late 20th and early 21st century: A period analysis. Oncologist 2010, 15, 994–1001. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Anderson, W.F.; Lortet-Tieulent, J.; Curado, M.P.; Ferlay, J.; Franceschi, S.; Rosenberg, P.S.; Bray, F.; Gillison, M.L. Worldwide trends in incidence rates for oral cavity and oropharyngeal cancers. J. Clin. Oncol. 2013, 31, 4550–4559. [Google Scholar] [CrossRef]
- Enache, S.G. The Economic and Social Situation in Romania. Available online: https://www.eesc.europa.eu/sites/default/files/resources/docs/qe-01-15-435-en-n.pdf (accessed on 7 August 2023).
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef]
- Evers, C.; Ostheimer, C.; Sieker, F.; Vordermark, D.; Medenwald, D. Benefit from surgery with additional radiotherapy in N1 head and neck cancer at the time of IMRT: A population-based study on recent developments. PLoS ONE 2020, 15, e0229266. [Google Scholar] [CrossRef]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef]
- Kis, A.M.; Macasoi, I.; Paul, C.; Radulescu, M.; Buzatu, R.; Watz, C.G.; Cheveresan, A.; Berceanu, D.; Pinzaru, I.; Dinu, S.; et al. Methotrexate and Cetuximab—Biological Impact on Non-Tumorigenic Models: In Vitro and In Ovo Assessments. Medicina 2022, 58, 167. [Google Scholar] [CrossRef]
- Marzouki, H.; Addas, M.A.; Nujoom, M.; Zawawi, F.; Almarzouki, H.Z.; Merdad, M. Hypopharyngeal Reconstruction: Possibilities, Outcomes, and Updates for Improving the Human Health for Quality of Life. Comput. Intell. Neurosci. 2022, 2022, 6132481. [Google Scholar] [CrossRef]
- State of Health in the EU: Country Health Profiles. Romania: Country Health Profile 2019. Available online: https://read.oecd-ilibrary.org/social-issues-migration-health/romania-country-health-profile-2019_f345b1db-en#page3 (accessed on 7 August 2023).
- Chevalier, C.; Bertaut, A.; Quivrin, M.; Vulquin, N.; Desandes, C.; Folia, M.; Duvillard, C.; Truc, G.; Crehange, G.; Maingon, P. Impact of waiting time on nodal staging in head and neck squamous-cell carcinoma treated with radical intensity modulated radiotherapy. Clin. Transl. Radiat. Oncol. 2016, 1, 27–32. [Google Scholar] [CrossRef]
- Huang, S.H.; Xu, W.; Waldron, J.; Siu, L.; Shen, X.; Tong, L.; Ringash, J.; Bayley, A.; Kim, J.; Hope, A.; et al. Refining American Joint Committee on Cancer/Union for International Cancer Control TNM stage and prognostic groups for human papillomavirus-related oropharyngeal carcinomas. J. Clin. Oncol. 2015, 33, 836–845. [Google Scholar] [CrossRef]
- Pynnonen, M.A.; Gillespie, M.B.; Roman, B.; Rosenfeld, R.M.; Tunkel, D.E.; Bontempo, L.; Brook, I.; Chick, D.A.; Colandrea, M.; Finestone, S.A.; et al. Clinical practice guideline: Evaluation of the neck mass in adults. Otolaryngol. Head Neck Surg. 2017, 157, S1–S30. [Google Scholar] [CrossRef]
- Cheol Park, G.; Roh, J.L.; Cho, K.J.; Seung Kim, J.; Hyeon Jin, M.; Choi, S.H.; Yuhl Nam, S.; Yoon Kim, S. 18F-FDG PET/CT vs. human papillomavirus, p16 and Epstein-Barr virus detection in cervical metastatic lymph nodes for identifying primary tumors. Int. J. Cancer 2017, 140, 1405–1412. [Google Scholar] [CrossRef]
- Lee, N.C.J.; Kelly, J.R.; Park, H.S.; An, Y.; Judson, B.L.; Burtness, B.A.; Husain, Z.A. Patterns of failure in high-metastatic node number human papillomavirus-positive oropharyngeal carcinoma. Oral Oncol. 2018, 85, 35–39. [Google Scholar] [CrossRef]
- Stack, B.C., Jr.; Duan, F.; Subramaniam, R.M.; Romanoff, J.; Sicks, J.D.; Bartel, T.; Chen, C.; Lowe, V.J. FDG-PET/CTand Pathology in Newly Diagnosed Head and Neck Cancer: ACRIN 6685 Trial, FDG-PET/CT cN0. Otolaryngol. Head Neck Surg. 2021, 164, 1230–1239. [Google Scholar] [CrossRef]
- Xing, Y.; Zhang, J.; Lin, H.; Gold, K.A.; Sturgis, E.M.; Garden, A.S.; Lee, J.J.; William, W.N., Jr. Relation between the level of lymph node metastasis and survival in locally advanced head and neck squamous cell carcinoma. Cancer 2016, 122, 534–545. [Google Scholar] [CrossRef] [PubMed]
- Jäckel, M.C.; Ambrosch, P.; Christiansen, H.; Martin, A.; Steiner, W. Value of postoperative radiotherapy in patients with pathologic N1 neck disease. Head Neck 2008, 30, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Hanai, N.; Asakage, T.; Kiyota, N.; Homma, A.; Hayashi, R. Controversies in relation to neck management in N0 early oral tongue cancer. Jpn. J. Clin. Oncol. 2019, 49, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Prodea, M.; Boia, E.R.; Ceausu, R.A.; Librimir, C.; Iovanescu, G.; Mederle, O.A. Lung Delayed Hypersensitivity. A case with particular features. Rev. Chim. 2018, 69, 2071–2073. [Google Scholar] [CrossRef]
- Cerezo, L.; Millan, I.; Torre, A.; Aragon, G.; Otero, J. Prognostic factors for survival and tumor control in cervical lymph node metastases from head and neck cancer: A multivariate study of 492 cases. Cancer 1992, 69, 1224–1234. [Google Scholar] [CrossRef]
- Ho, A.S.; Kim, S.; Tighiouart, M.; Gudino, C.; Mita, A.; Scher, K.S.; Laury, A.; Prasad, R.; Shiao, S.L.; Van Eyk, J.E.; et al. Metastatic Lymph Node Burden and Survival in Oral Cavity Cancer. J. Clin. Oncol. 2017, 35, 3601–3609. [Google Scholar] [CrossRef]
- Divi, V.; Harris, J.; Harari, P.M.; Cooper, J.S.; McHugh, J.; Bell, D.; Sturgis, E.M.; Cmelak, A.J.; Suntharalingam, M.; Raben, D.; et al. Establishing quality indicators for neck dissection: Correlating the number of lymph nodes with oncologic outcomes (NRG Oncology RTOG 9501 and RTOG 0234). Cancer 2016, 122, 3464–3471. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Dong, Z.; Vodopyanov, D.; Imai, A.; Helman, J.I.; Prince, M.E.; Wicha, M.S.; Nör, J.E. Endothelial cell-initiated signaling promotes the survival and self-renewal of cancer stem cells. Cancer Res. 2010, 70, 9969–9978. [Google Scholar] [CrossRef]
- Hammerlid, E.; Silander, E.; Hornestam, L.; Sullivan, M. Health-related quality of life three years after diagnosis of head and neck cancer—A longitudinal study. Head Neck 2001, 23, 113–125. [Google Scholar] [CrossRef]
- Mehanna, H.M.; Morton, R.P. Deterioration in quality-of-life of late (10-year) survivors of head and neck cancer. Clin. Otolaryngol. 2006, 31, 204–211. [Google Scholar] [CrossRef]
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Type of Cancer | Romania | Worldwide Annual Number of New Cancer Cases (%) | |||
|---|---|---|---|---|---|
| New Cases (No) | Rank by Incidence Worldwide | Percentage of Death (%) | 5-Year Survival Prevalence/100,000 | ||
| Nasopharynx | 403 | 27th | 0.34 | 6.66 | 0.5 |
| Hypopharynx | 634 | 24th | 0.22 | 5.76 | 0.4 |
| Oropharynx | 1351 | 21st | 1.4 | 19.12 | 0.7 |
| Benign (n = 165) | Malign (n = 350) | Total (n = 513) | p-Value | |
|---|---|---|---|---|
| Age | <0.001 1 | |||
| Mean (SD) | 47.3 (15.6) | 59.7 (9.8) | 55.7 (13.3) | |
| Range | 17.0–83.0 | 21.0–86.0 | 17.0–86.0 | |
| Site | <0.001 2 | |||
| Hypopharynx | 7.0 (4.2%) | 150.0 (42.9%) | 157.0 (30.5%) | |
| Oropharynx | 55.0 (33.3%) | 144.0 (41.1%) | 199.0 (38.6%) | |
| Rhino pharynx | 103.0 (62.4%) | 56.0 (16.0%) | 159.0 (30.9%) | |
| Sex | <0.001 2 | |||
| M | 88.0 (53.3%) | 302.0 (86.3%) | 390.0 (75.7%) | |
| F | 77.0 (46.7%) | 48.0 (13.7%) | 125.0 (24.3%) | |
| Year | 0.739 2 | |||
| 2014 | 22.0 (13.3%) | 57.0 (16.3%) | 79.0 (15.3%) | |
| 2015 | 29.0 (17.6%) | 61.0 (17.4%) | 90.0 (17.5%) | |
| 2016 | 41.0 (24.8%) | 83.0 (23.7%) | 124.0 (24.1%) | |
| 2017 | 33.0 (20.0%) | 79.0 (22.6%) | 112.0 (21.7%) | |
| 2018 | 40.0 (24.2%) | 70.0 (20.0%) | 110.0 (21.4%) | |
| Area | 0.466 2 | |||
| Urban area | 91.0 (55.2%) | 181.0 (51.7%) | 272.0 (52.8%) | |
| Rural area | 74.0 (44.8%) | 169.0 (48.3%) | 243.0 (47.2%) | |
| Nodal staging | <0.001 2 | |||
| N0 | 146.0 (88.5%) | 199.0 (56.9%) | 345.0 (67.0%) | |
| N1 | 10.0 (6.1%) | 54.0 (15.4%) | 64.0 (12.4%) | |
| N2 | 4.0 (2.4%) | 36.0 (10.3%) | 40.0 (7.8%) | |
| N3 | 5.0 (3.0%) | 61.0 (17.4%) | 66.0 (12.8%) | |
| Days of admission | <0.001 1 | |||
| Mean (SD) | 3.7 (2.7) | 5.4 (4.7) | 4.9 (4.2) | |
| Range | 1.0–23.0 | 1.0–37.0 | 1.0–37.0 | |
| Deceased | 1.0 (0.6%) | 33.0 (9.4%) | 34.0 (6.6%) | <0.001 2 |
| Acute respiratory failure | 0.0 (0.0%) | 34.0 (9.7%) | 34.0 (6.6%) | <0.001 2 |
| Histopathological Diagnosis | (n = 515) |
|---|---|
| Benign | n = 165 |
| Inflammatory polyp | 3.0 (1.8%) |
| Adenoid vegetations | 2.0 (1.2%) |
| Chronic hypertrophic adenoiditis | 5.0 (3.0%) |
| Chronic hypertrophic tonsillitis | 15.0 (9.1%) |
| Chronic granulomatous inflammation | 6.0 (3.6%) |
| Reactive hyperplasia of lymphoid follicles | 76.0 (46.1%) |
| Squamous papilloma | 11.0 (6.7%) |
| Chronic inflammatory process | 21.0 (12.7%) |
| Malign | n = 350 |
| Squamous cell carcinoma | 200.0 (57.1%) |
| Keratinizing squamous cell carcinoma | 68.0 (19.4%) |
| In situ squamous cell carcinoma | 7.0 (2.0%) |
| UCNT | 24.0 (6.9%) |
| NHL | 24.0 (6.9%) |
| Other cancers | 27.0 (7.7%) |
| Dependent: Deceased | No | Yes | OR (Univariable) | OR (Multivariable) | |
|---|---|---|---|---|---|
| N staging | N0 | 327 (94.8) | 18 (5.2) | - | - |
| N1 | 61 (95.3) | 3 (4.7) | 0.89 (0.20–2.74, p = 0.860) | 0.41 (0.06–1.62, p = 0.266) | |
| N2 | 36 (90.0) | 4 (10.0) | 2.02 (0.56–5.77, p = 0.226) | 1.43 (0.34–4.86, p = 0.592) | |
| N3 | 57 (86.4) | 9 (13.6) | 2.87 (1.18–6.56, p = 0.015) | 1.56 (0.55–4.16, p = 0.389) | |
| Grading | No | 31 (91.2) | 3 (8.8) | - | - |
| G1 | 6 (85.7) | 1 (14.3) | 1.72 (0.08–16.37, p = 0.661) | 0.51 (0.02–7.31, p = 0.641) | |
| G2 | 206 (91.2) | 20 (8.8) | 1.00 (0.32–4.43, p = 0.996) | 0.17 (0.03–1.11, p = 0.051) | |
| G3 | 35 (92.1) | 3 (7.9) | 0.89 (0.15–5.09, p = 0.887) | 0.12 (0.01–0.95, p = 0.044) | |
| In situ | 5 (62.5) | 3 (37.5) | 6.20 (0.93–43.32, p = 0.049) | 1.13 (0.11–11.70, p = 0.916) | |
| Subsite | Hypopharynx | 142 (90.4) | 15 (9.6) | - | - |
| Oropharynx | 181 (91.0) | 18 (9.0) | 0.94 (0.46–1.96, p = 0.869) | 1.23 (0.52–2.95, p = 0.631) | |
| Rhino pharynx | 158 (99.4) | 1 (0.6) | 0.06 (0.00–0.30, p = 0.007) | 0.14 (0.01–1.27, p = 0.129) | |
| Acute respiratory failure | No | 452 (94.0) | 29 (6.0) | - | - |
| Yes | 29 (85.3) | 5 (14.7) | 2.69 (0.87–6.95, p = 0.048) | 1.90 (0.55–5.69, p = 0.271) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kis, A.M.; Watz, C.G.; Motofelea, A.C.; Chiriac, S.; Poenaru, M.; Dehelean, C.A.; Borza, C.; Ionita, I. Challenges of Pharyngeal Cancer Screening in Lower-Income Countries during Economic and Social Transitions: A Population-Based Analysis. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2226-2237. https://doi.org/10.3390/ejihpe13100157
Kis AM, Watz CG, Motofelea AC, Chiriac S, Poenaru M, Dehelean CA, Borza C, Ionita I. Challenges of Pharyngeal Cancer Screening in Lower-Income Countries during Economic and Social Transitions: A Population-Based Analysis. European Journal of Investigation in Health, Psychology and Education. 2023; 13(10):2226-2237. https://doi.org/10.3390/ejihpe13100157
Chicago/Turabian StyleKis, Andreea M., Claudia G. Watz, Alexandru C. Motofelea, Sorin Chiriac, Marioara Poenaru, Cristina A. Dehelean, Claudia Borza, and Ioana Ionita. 2023. "Challenges of Pharyngeal Cancer Screening in Lower-Income Countries during Economic and Social Transitions: A Population-Based Analysis" European Journal of Investigation in Health, Psychology and Education 13, no. 10: 2226-2237. https://doi.org/10.3390/ejihpe13100157