Non-Antagonistic Contradictoriness of the Progress of Advanced Digitized Production with SARS-CoV-2 Virus Transmission in the Area of Dental Engineering

 , , ,
, , ,
Abstract
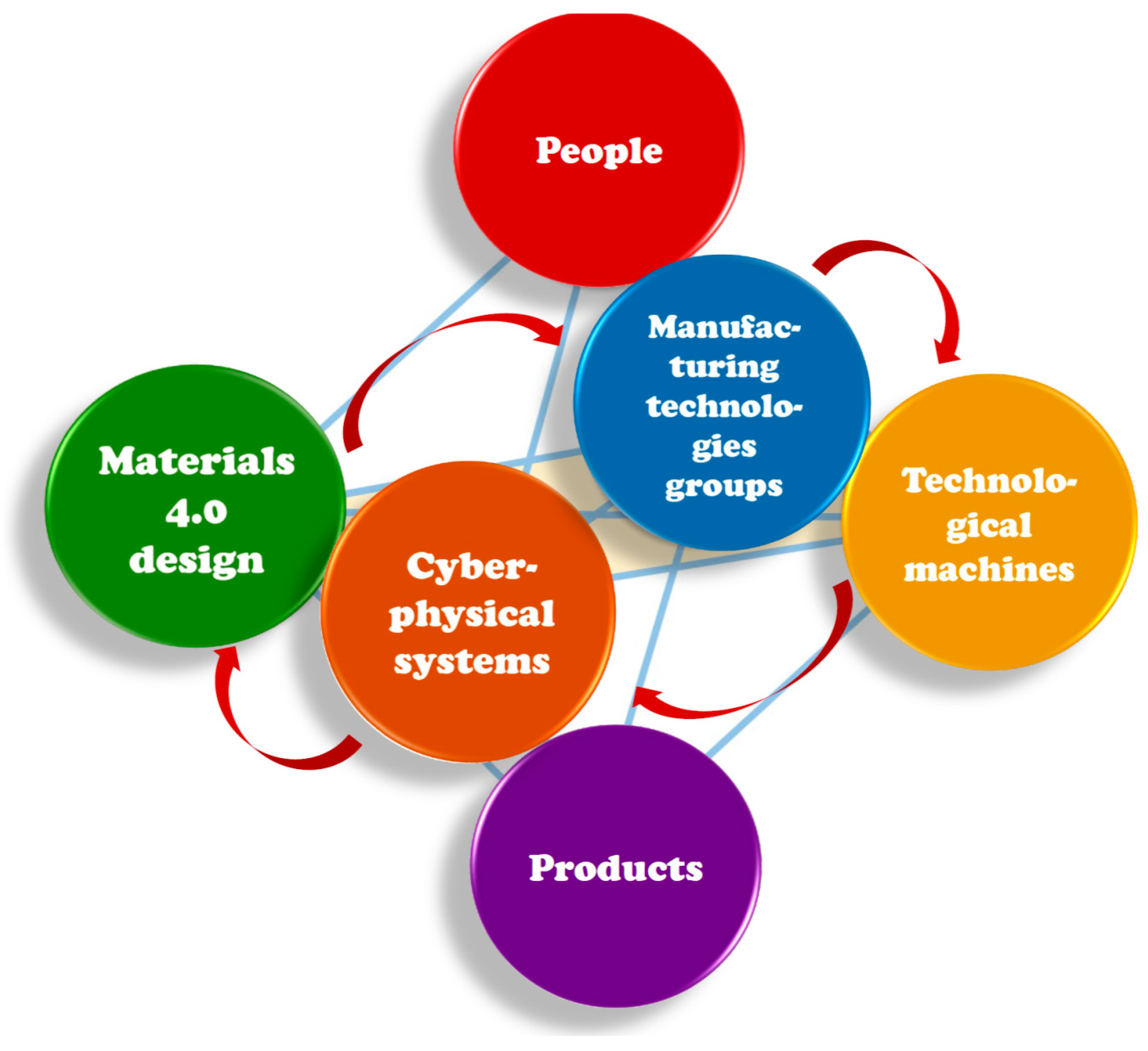
:1. General Goals of Advanced Digitized Production in the Industry 4.0 Stage of the Industrial Revolution
2. Multifaceted Implications of the COVID-19 Disease Pandemic Caused by SARS-CoV-2 Virus Transmission
3. The Concept of Elimination of the Mixture of Bioaerosol with Pathogenic Microorganisms and Clinical Aerosol in the Conditions of Performing Dental Procedures
4. Comparative Assessment of the Authors Solution against the Available Methods of Protection against the Effects of the SARS-CoV-2 Coronavirus
5. Engineering Aspects of Digitized Design and Manufacturing of an Authors Device for Dental Purposes that Protect the Doctor and Medical Staff against the SARS-CoV-2 Coronavirus
6. Recapitulation
- I.
- In the case that is dear to the authors, i.e., dentistry and dental engineering, the principle of “stay at home” quickly turned into another “do nothing”, because contacting the patient you can contract a deadly disease [24,25,26,27,28]. The Hippocratic Oath and ethics ...? [29]. We quickly developed the authors’ SPEC strategy, which involves activity, not passive waiting, and hitting the heart of the problem to remove the cause that makes our life difficult. Of course, we know that the solution at the root of this problem is to invent the right vaccine. On 14 August 2020, the European Union concluded an agreement with AstraZeneca, cooperating with the University of Oxford, to purchase 300 million doses of the vaccine. The AstraZeneca vaccine is already in Phase II/III of large-scale clinical trials. Talks are also being held with other vaccine manufacturers, i.e., Sanofi-GSK, Johnson & Johnson, CureVac, and Moderna [30]. U.S. government placed a similar agreement with Pfizer and Biontech and on 22 July 2020, and submitted an initial order of 100 million doses and can acquire up to 500 million additional doses [31]. But we still do not know when these vaccines will actually be delivered to recipients. We have to wait until this process ends positively.
- II.
- We want to help people by treating their sick teeth and removing the effects of these diseases, which can have a very complex impact on the health of many people. There is a high risk of complications, not only local but also systemic, resulting from pulp diseases [32]. Bacterial endocarditis, coronary artery disease, cerebral abscess, stroke, rheumatoid arthritis, osteoporosis, nephritis, pneumonia, and even preterm labor can be caused by an oral disease primary lesion [33,34,35,36,37,38,39]. In a favorable situation, caries and periodontal diseases may directly contribute to the patient’s death.
- III.
- It is obvious that the lack of teeth causes serious diseases [40,41,42,43,44,45,46,47,48,49,50]. It is possible to include chronic inflammatory changes gastric mucosa, upper gastrointestinal and pancreatic cancer, and an increased incidence of duodenal ulcers apart from aesthetic considerations. Tooth loss causes malocclusion, which affects the metabolism of the cerebrospinal fluid that nourishes the brain. The consequence may be headaches, migraines, pains in the cervical spine, and mood disorders, and also obstructive sleep apnea and neurocognitive dysfunction. Completely edentulous patients are more prone to electrocardiographic abnormalities, hypertension, heart failure, ischemic heart disease, stroke, aortic sclerosis, and coronary plaque formation. Toothlessness is a predictor of cardiovascular mortality. It may also cause rheumatoid arthritis, chronic kidney disease, non-insulin-dependent diabetes mellitus, and some cancers. A higher number of illnesses comorbid on the toothlessness are existing.
- IV.
- The consequence of caries and periodontal diseases is the necessity to insert implants and prosthetic restorations, including bridges and crowns. It allows us to alleviate the effects of these diseases, and even effectively eliminate some of them. Improving the bite may have a positive effect on reducing the symptoms of multiple sclerosis. The restoring the dentition in the elderly has a positive effect on the hippocampus in the temporal lobe of the cerebral forebrain, responsible, among others, for spatial memory and for creating and recreating episodic memories. The systemic effect of masticatory disorder is an epidemiological risk factor for dementia. Toothlessness is often the direct cause of shortening human life. Chewing dysfunction causes morphological and functional changes in the hippocampus while chewing helps to maintain the proper functions of the hippocampus [51,52,53,54,55,56,57].
- V.
- The coming of the SARS-CoV-2 virus blocked almost all dental treatment activities. Most dental procedures in almost the entire world have been abandoned for many months [18,19,20,21,22], although starting from June/July 2020 adequately, the initial restrictions have been slightly relaxed in various countries, but not entirely waived. The result is an obvious deterioration in dental welfare and an exacerbation of the negative effects of all untreated oral diseases and the systemic comorbidities and diseases that are caused thereby, as described above. This is the conflict that is signaled in the title of this paper. On the other hand, it was its occurrence that forced the authors to be active in this area. Most likely, had it not been for this, they would never have addressed the matter. That is why it was decided that, despite the fact that this conflict arose, it is non-antagonistic because it mobilized the authors to act positively. The sooner the reasons underlying the decision to treat only emergency cases in dentistry are resolved, the sooner proper dental care will be provided again. The authors are deeply convinced that the solution proposed in this paper serves this matter well.
- VI.
- This paper presents a breakthrough authors solution, implemented by the active SPEC strategy, and aims to eliminate clinical aerosol at the source by negative pressure aspirating bioaerosol at the patient’s mouth line. The comparative benchmarking analysis and its results show that only the proprietary solution with a set of devices eliminates the threat at the source, while the remaining known methods do not meet the expectations in this aspect. It was only possible to solve this problem thanks to progress in advanced digitized production. Please note that the essence of the problem concerns the correct selection of materials to be used in the manufacture of this device and materials processing technologies with the use of additive technologies and surface engineering.
- VII.
- So the question arises whether, when this virus disappears and its pandemic will finally end, will our solution still be needed. That’s it. This pandemic has taught the people something, Nature has let the people know about its enormous power and helplessness of people, although they consider themselves the masters of the situation on Earth. As we can see, it is not so. Viruses live with us and next to us. Every now and then, some epidemic breaks out, i.e., Spanish flu, avian flu, swine flu, cholera, Ebola, SARS 1 and 2, and flu every year [58,59]. They are diseases that take thousands of lives. Each disease transmitted by airborne droplets requires protection, e.g., the way is presented in this paper. This has to be done routinely because we never know who is infected.
- VIII.
- Despite the tragic events that inspired this action, the general conclusion is optimistic. The authors have found a solution to the problem that seriously threatens us.
Author Contributions
Funding
Conflicts of Interest
Intention
References
- Kagermann, H.; Wahlster, W.; Helbig, J. Recommendations for Implementing the Strategic Initiative INDUSTRIE 4.0: Final Report of the Industrie 4.0 Working Group; Federal Ministry of Education and Research: Bonn, Germany, 2013.
- Rüßmann, M.; Lorenz, M.; Gerbert, P.; Waldner, M.; Justus, J.; Engel, P.; Harnisch, M. Industry 4.0: The Future of Productivity and Growth in Manufacturing Industries; Boston Consulting Group: Boston, MA, USA, 2015. [Google Scholar]
- European Commision. Commission Sets out Path to Digitise European Industry; European Commission: Brussels, Belgium, 2016; Available online: http://web.archive.org/web/20200403145542/https://ec.europa.eu/commission/presscorner/detail/en/IP_16_1407 (accessed on 17 August 2020).
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Why Are Carbon-Based Materials Important in Civilization Progress and Especially in the Industry 4.0 Stage of the Industrial Revolution. Mater. Perform. Charact. 2019, 8, 337–370. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Applications of Laser Processing of Materials in Surface Engineering in the Industry 4.0 Stage of the Industrial Revolution. Mater. Perform. Charact. 2019, 8, 1091–1129. [Google Scholar] [CrossRef]
- Dobrzański, L.A. Effect of Heat and Surface Treatment on the Structure and Properties of the Mg-Al-Zn-Mn Casting Alloys. In Magnesium and Its Alloys; CRC Press: Boca Raton, FL, USA, 2019; pp. 91–202. [Google Scholar]
- Dobrzański, L.A.; Dobrzański, L.B. Approach to the Design and Manufacturing of Prosthetic Dental Restorations According to the Rules of Industry 4.0. Mater. Perform. Charact. 2020, 9, 394–476. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B. Dentistry 4.0 Concept in the Design and Manufacturing of Prosthetic Dental Restorations. Processes 2020, 8, 525. [Google Scholar] [CrossRef]
- United Nations Industrial Development Organization. Industrial Development Report 2020. Industrializing in the Digital Age. 2019. Available online: https://www.unido.org/sites/default/files/files/2019-11/UNIDO_IDR2020-MainReport_overview.pdf (accessed on 17 August 2020).
- CDC; Eckert, A.; Higgins, D. Available online: https://phil.cdc.gov/Details.aspx?pid=23312 (accessed on 17 August 2020).
- WHO. Coronavirus Disease (COVID-19) Dashboard Data. Available online: https://covid19.who.int/ (accessed on 17 August 2020).
- May, B. Research Briefing/Global Coronavirus Watch: Cautious pessimism warranted (Oxford Economic, 20 July 2020). Available online: http://blog.oxfordeconomics.com/coronavirus/cautious-pessimism-warranted (accessed on 17 August 2020).
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Raport Amnesty International MJM, Pracownicy Medyczni na Całym Świecie są Uciszani, Narażani i Atakowani. Available online: https://amnesty.org.pl/pracownicy-medyczni-na-calym-swiecie-sa-uciszani-narazani-i-atakowani/ (accessed on 17 August 2020).
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382. [Google Scholar] [CrossRef] [PubMed]
- Fallahi, H.R.; Keyhan, S.O.; Zandian, D.; Kim, S.-G.; Cheshmi, B. Being a front-line dentist during the Covid-19 pandemic: a literature review. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yonis, O.B.; Alyahya, M.; Khader, Y.S.; Al Nsour, M.; Al-Batayneh, O.B.; Saadeh, R.; Bashier, H.; Alfaqih, M.; Al-Azzam, S.; Alshurman, B.A. Dentists’ Awareness, Perception, and Attitude Regarding COVID-19 and Infection Control: Cross-Sectional Study Among Jordanian Dentists. JMIR Public Health Surveill. 2020, 6, e18798. [Google Scholar] [CrossRef]
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Akcesorium do ochrony osobistej personelu dentystycznego przed koronawirusem SARS-CoV-2 i innymi drobnoustrojami chorobotwórczymi. Zgłoszenie patentowe P.434391, Poland, data zgłoszenia: 19.06.2020 r.
- Dobrzański, L.B.; Dobrzański, L.A.; Dobrzańska, J. CleanDENTworkspace—A medical aerosol absorption system generated during medical procedures in the patient’s mouth during dental, ENT and general medical procedures in order to effectively protect personnel and patients against viruses (including SARS-cov-2) and other microorganisms (wniosek o dofinansowanie Projektu nr: POIR.01.01.01-00-0637/20, 04.06.2020 złożony do NCBiR, Warsaw, Poland).
- Dobrzańska-Danikiewicz, A.D. Księga Technologii Krytycznych Kształtowania Struktury i Własności Powierzchni Materiałów Inżynierskich; International OCSCO World Press: Gliwice, Poland, 2013; pp. 1–823. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Inżynieria Powierzchni Materiałów: Kompendium Wiedzy i Podręcznik Akademicki; International OCSCO World Press: Gliwice, Poland, 2018; pp. 1–1138. [Google Scholar]
- Dobrzański, L.A.; Dobrzański, L.B. Innovative Dental and Maxillo-Facial Implant-Scaffold Manufactured Using the Innovative Technology and Additive Computer-Aided Materials Design. Medical and Dental Engineering Centre for Research; Design, and Production: Gliwice, Poland, 2017–2021. [Google Scholar]
- Available online: https://www.worldometers.info/watch/world-population/ (accessed on 5 August 2020).
- Guidance for Dental Settings, Interim Infection Prevention and Control Guidance for Dental Settings during the Coronavirus Disease 2019 (COVID-19) Pandemic. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html (accessed on 28 August 2020).
- Management of Acute Dental Problems during COVID-19 Pandemic. Available online: https://www.sdcep.org.uk/published-guidance/acute-dental-problems-covid-19/ (accessed on 28 August 2020).
- Dental Care and Coronavirus (COVID-19). Available online: https://www.dentalhealth.org/Pages/FAQs/Category/coronavirus (accessed on 28 August 2020).
- Guidance on COVID-19, Guidance on Managing Infection Related Risks in Dental Services. Available online: https://www.fdiworlddental.org/sites/default/files/media/documents/guidance_on_managing_infection_related_risks_in_dental_services_0.pdf (accessed on 28 August 2020).
- COVID-19 and Dental Practice; What Has Been Done in China? Available online: https://www.fdiworlddental.org/sites/default/files/media/documents/covid-19_and_dental_practice_what_has_been_done_in_china.pdf (accessed on 28 August 2020).
- WMA Declaration of Geneva (adopted by the 2nd General Assembly of the World Medical Association, Geneva, Switzerland, September 1948 and amended by the 22nd World Medical Assembly, Sydney, Australia, August 1968 and the 35th World Medical Assembly, Venice, Italy, October 1983 and the 46th WMA General Assembly, Stockholm, Sweden, September 1994 and editorially revised by the 170th WMA Council Session, Divonne-les-Bains, France, May 2005 and the 173rd WMA Council Session, Divonne-les-Bains, France, May 2006 and amended by the 68th WMA General Assembly, Chicago, United States, October 2017). Available online: https://www.wma.net/policies-post/wma-declaration-of-geneva/ (accessed on 28 August 2020).
- Convention for the Protection of Human Rights and Fundamental Freedoms, Rome. Refug. Surv. Q. 2005, 24, 147–148. [CrossRef]
- Coronavirus: Commission Reaches First Agreement on a Potential Vaccine. Available online: https://ec.europa.eu/commission/presscorner/detail/en/ip_20_1438 (accessed on 28 August 2020).
- Pfizer and Biontech Announce an Agreement with U.S. Government for up to 600 Million Doses of Mrna-Based Vaccine Candidate against sars-cov-2. Available online: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-agreement-us-government-600 (accessed on 28 August 2020).
- Al-Nawas, B.; Maeurer, M. Severe versus Local Odontogenic Bacterial Infections: Comparison of Microbial Isolates. Eur. Surg. Res. 2007, 40, 220–224. [Google Scholar] [CrossRef]
- Mueller, A.; Saldamli, B.; Stübinger, S.; Walter, C.; Flückiger, U.; Merlo, A.; Schwenzer-Zimmerer, K.; Zeilhofer, H.-F.; Zimmerer, S. Oral bacterial cultures in nontraumatic brain abscesses: Results of a first-line study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Tronstad, L.; Olsen, I. Brain abscesses caused by oral infection. Dent. Traumatol. 1999, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Scannapieco, F.A. Role of Oral Bacteria in Respiratory Infection. J. Periodontol. 1999, 70, 793–802. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Bush, R.B.; Paju, S. Associations between Periodontal Disease and Risk for Nosocomial Bacterial Pneumonia and Chronic Obstructive Pulmonary Disease. A Systematic Review. Ann. Periodontol. 2003, 8, 54–69. [Google Scholar] [CrossRef] [Green Version]
- Alexander, M.; Krishnan, B.; Shenoy, N. Diabetes mellitus and odontogenic infections—an exaggerated risk? Oral Maxillofac. Surg. 2008, 12, 129–130. [Google Scholar] [CrossRef] [PubMed]
- López, N.J.; Smith, P.C.; Gutiérrez, J. Periodontal Therapy May Reduce the Risk of Preterm Low Birth Weight in Women with Peridotal Disease: A randomized Controlled Trial. J. Periodontol. 2002, 73, 911–924. [Google Scholar] [CrossRef] [PubMed]
- Pallasch, T.J.; Wahl, M.J. Focal infection: New age or ancient history? Endod. Top. 2003, 4, 32–45. [Google Scholar] [CrossRef] [Green Version]
- Burzyńska, B.; Mierzwińska-Nastalska, E. Rehabilitacja protetyczna pacjentów bezzębnych. Nowa Stomatol. 2011, 4, 167–169. [Google Scholar]
- Felton, D.A. Edentulism and Comorbid Factors. J. Prosthodont. 2009, 18, 88–96. [Google Scholar] [CrossRef]
- Felton, D.A. Complete Edentulism and Comorbid Diseases: An Update. J. Prosthodont. 2015, 25, 5–20. [Google Scholar] [CrossRef]
- Abnet, C.C.; Qiao, Y.-L.; Dawsey, S.M.; Dong, Z.-W.; Taylor, P.R.; Mark, S.D. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int. J. Epidemiol. 2005, 34, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Sierpinska, T.; Golebiewska, M.; Dlugosz, J.; Kemona, A.; Laszewicz, W. Connection between masticatory efficiency and pathomorphologic changes in gastric mucosa. Quintessence Int. 2007, 38, 31–37. [Google Scholar] [PubMed]
- Bagchi, S.; Tripathi, A.; Tripathi, S.; Kar, S.; Tiwari, S.C.; Singh, J. Obstructive Sleep Apnea and Neurocognitive Dysfunction in Edentulous Patients. J. Prosthodont. 2018, 28, e837–e842. [Google Scholar] [CrossRef] [PubMed]
- Völzke, H.; Schwahn, C.; Hummel, A.; Wolff, B.; Kleine, V.; Robinson, D.M.; Dahm, J.B.; Felix, S.B.; John, U.; Kocher, T. Tooth loss is independently associated with the risk of acquired aortic valve sclerosis. Am. Hear. J. 2005, 150, 1198–1203. [Google Scholar] [CrossRef]
- Takata, Y.; Ansai, T.; Matsumura, K.; Awano, S.; Hamasaki, T.; Sonoki, K.; Kusaba, A.; Akifusa, S.; Takehara, T. Relationship between tooth loss and electrocardiographic abnormalities in octogenarians. J. Dent. Res. 2001, 80, 1648–1652. [Google Scholar] [CrossRef]
- Holmlund, A.; Holm, G.; Lind, L. Number of Teeth as a Predictor of Cardiovascular Mortality in a Cohort of 7674 Subjects Followed for 12 Years. J. Periodontol. 2010, 81, 870–876. [Google Scholar] [CrossRef]
- De Pablo, P.; Dietrich, T.; McAlindon, T.E. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J. Rheumatol. 2007, 35, 70–76. [Google Scholar]
- Chen, H.; Iinuma, M.; Onozuka, M.; Kubo, K.-Y. Chewing Maintains Hippocampus-Dependent Cognitive Function. Int. J. Med Sci. 2015, 12, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Lexomboon, D.; Trulsson, M.; Wårdh, I.; Parker, M.G. Chewing Ability and Tooth Loss: Association with Cognitive Impairment in an Elderly Population Study. J. Am. Geriatr. Soc. 2012, 60, 1951–1956. [Google Scholar] [CrossRef]
- Stein, P.S.; Desrosiers, M.; Donegan, S.J.; Yepes, J.F.; Kryscio, R.J. Tooth loss, dementia and neuropathology in the Nun Study. J. Am. Dent. Assoc. 2007, 138, 1314–1322. [Google Scholar] [CrossRef]
- Henke, K. A model for memory systems based on processing modes rather than consciousness. Nat. Rev. Neurosci. 2010, 11, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Kawahata, M.; Ono, Y.; Ohno, A.; Kawamoto, S.; Kimoto, K.; Onozuka, M. Loss of molars early in life develops behavioral lateralization and impairs hippocampus-dependent recognition memory. BMC Neurosci. 2014, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onishi, M.; Iinuma, M.; Tamura, Y.; Kubo, K.-Y. Learning deficits and suppression of the cell proliferation in the hippocampal dentate gyrus of offspring are attenuated by maternal chewing during prenatal stress. Neurosci. Lett. 2014, 560, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Obata, T.; Takahashi, H.; Tachibana, A.; Kuroiwa, D.; Takahahi, T.; Ikehira, H.; Onozuka, M. Effects of chewing on cognitive processing speed. Brain Cogn. 2013, 81, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Procyk-Lewandowska, I. Historia Pandemii na Świecie—Koronawirus SARS-CoV-2 na tle Innych Pandemii. Available online: https://www.medicover.pl/o-zdrowiu/historia-pandemii-na-swiecie-koronawirus-sars-cov-2-na-tle-innych-pandemii,6788,n,168 (accessed on 28 August 2020).
- Hays, J.N. Epidemics and Pandemics: Their Impacts on Human History; ABC-CLIO: Santa Barbara, CA, USA; Denver, CO, USA; London, UK, 2005. [Google Scholar]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Criterion | Weight | No | Criterion | Weight |
|---|---|---|---|---|---|
| Potential | Atttractiveness | ||||
| P1 | Effectiveness of eliminating the risk of coronavirus | 0.50 | A1 | The sense of security of medical personnel | 0.50 |
| P2 | Ergonomic factor and 4-hand work | 0.25 | A2 | Patients’ sense of safety | 0.20 |
| P3 | Comprehensive approach | 0.10 | A3 | Difficulties in applying the method | 0.20 |
| P4 | Safety of cleaning elements | 0.10 | A4 | Importance for the profitability of the practice | 0.05 |
| P5 | Installation cost | 0.05 | A5 | Impact on the clinics’ development prospects | 0.05 |
| No | Type of Method Known in the Literature, State-Of-The-Art Including Own Solution | Potential | Attracti Veness |
|---|---|---|---|
| 1 | Installation of air filtering devices in the treatment room | 6.7 | 4.0 |
| 2 | Equipment operating with HEPA or carbon filters or with UV radiation | 5.95 | 4.0 |
| 3 | Dental saliva extractor attachments | 3.3 | 5.8 |
| 4 | “Extract from the treatment area” devices | 3.7 | 6.6 |
| 5 | Patient enclosures in the form of glass or PMMA boxes | 1.45 | 3.9 |
| 6 | Original solution eliminating the threat at the source with the set of devices for virus elimination | 9.0 | 8.5 |
| Version | Model Volume [cm3] | SLA Approximate Material Loss (Supports) [cm3] | Number of Discs Used for Details Manufacturing | Volume of the Working Space of the Disc [cm3] | Total Volume of Disks [cm3] | CNC Approximate Material Loss [cm3] |
|---|---|---|---|---|---|---|
| basic | 72.15 | 1.97 | 9 | 177.12 | 1594.04 | 1521.89 |
| expanded | 150.35 | 48.4 | 19 | 3365.2 | 3214.84 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Non-Antagonistic Contradictoriness of the Progress of Advanced Digitized Production with SARS-CoV-2 Virus Transmission in the Area of Dental Engineering. Processes 2020, 8, 1097. https://doi.org/10.3390/pr8091097
Dobrzański LA, Dobrzański LB, Dobrzańska-Danikiewicz AD, Dobrzańska J, Rudziarczyk K, Achtelik-Franczak A. Non-Antagonistic Contradictoriness of the Progress of Advanced Digitized Production with SARS-CoV-2 Virus Transmission in the Area of Dental Engineering. Processes. 2020; 8(9):1097. https://doi.org/10.3390/pr8091097
Chicago/Turabian StyleDobrzański, Leszek A., Lech B. Dobrzański, Anna D. Dobrzańska-Danikiewicz, Joanna Dobrzańska, Karolina Rudziarczyk, and Anna Achtelik-Franczak. 2020. "Non-Antagonistic Contradictoriness of the Progress of Advanced Digitized Production with SARS-CoV-2 Virus Transmission in the Area of Dental Engineering" Processes 8, no. 9: 1097. https://doi.org/10.3390/pr8091097