Investigation and Analysis of a Hazardous Chemical Accident in the Process Industry: Triggers, Roots, and Lessons Learned


Abstract
:1. Introduction
1.1. Background of the Accident
1.2. Theoretical Basis for Accident Analysis
2. Method
- performing the events segmentation for accidents, especially for those involving domino effects, and identifying the critical events related to the occurrence and development of the accident based on the process or timeline;
- identifying all organizations (e.g., the design institute, the interested parties, the regulators, etc.) related to the accident and finding out the one in which the accident occurred;
- identifying all unsafe acts and unsafe conditions leading to the critical events by consulting related laws or regulations, and classifying them according to the violations, staff, materials, facilities, places, etc.;
- determining the specific flaws in individual safety knowledge, safety awareness, safety habits, psychological status and psychological status according to the unsafe acts or unsafe conditions;
- mining or deducing the deficiencies in the development and implementation of organizational safety management system based on the framework in the OH&S management system.
- mining or deducing the weaknesses in the construction of organizational safety culture carriers (i.e., the medium or tool to display and spread the safety concept) and member understanding for safety culture elements;
- performing the analysis of other causal factors from external organizations according to the above steps;
- achieving the visualization of all causal factors based on the 24Model.
3. Accident Overview
3.1. Substance and Installation
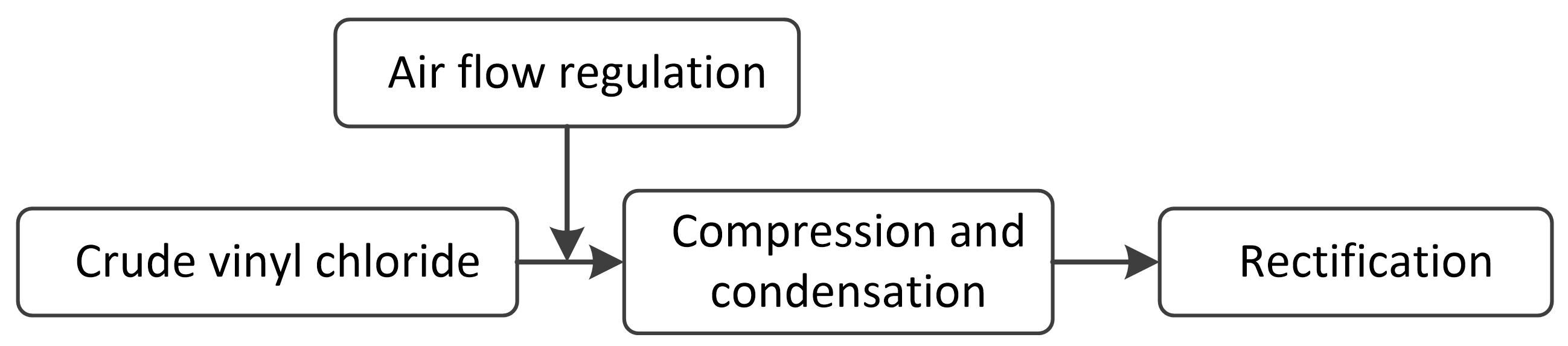
3.2. Process and Consequence
4. Accident Anatomy
4.1. Sequential Events
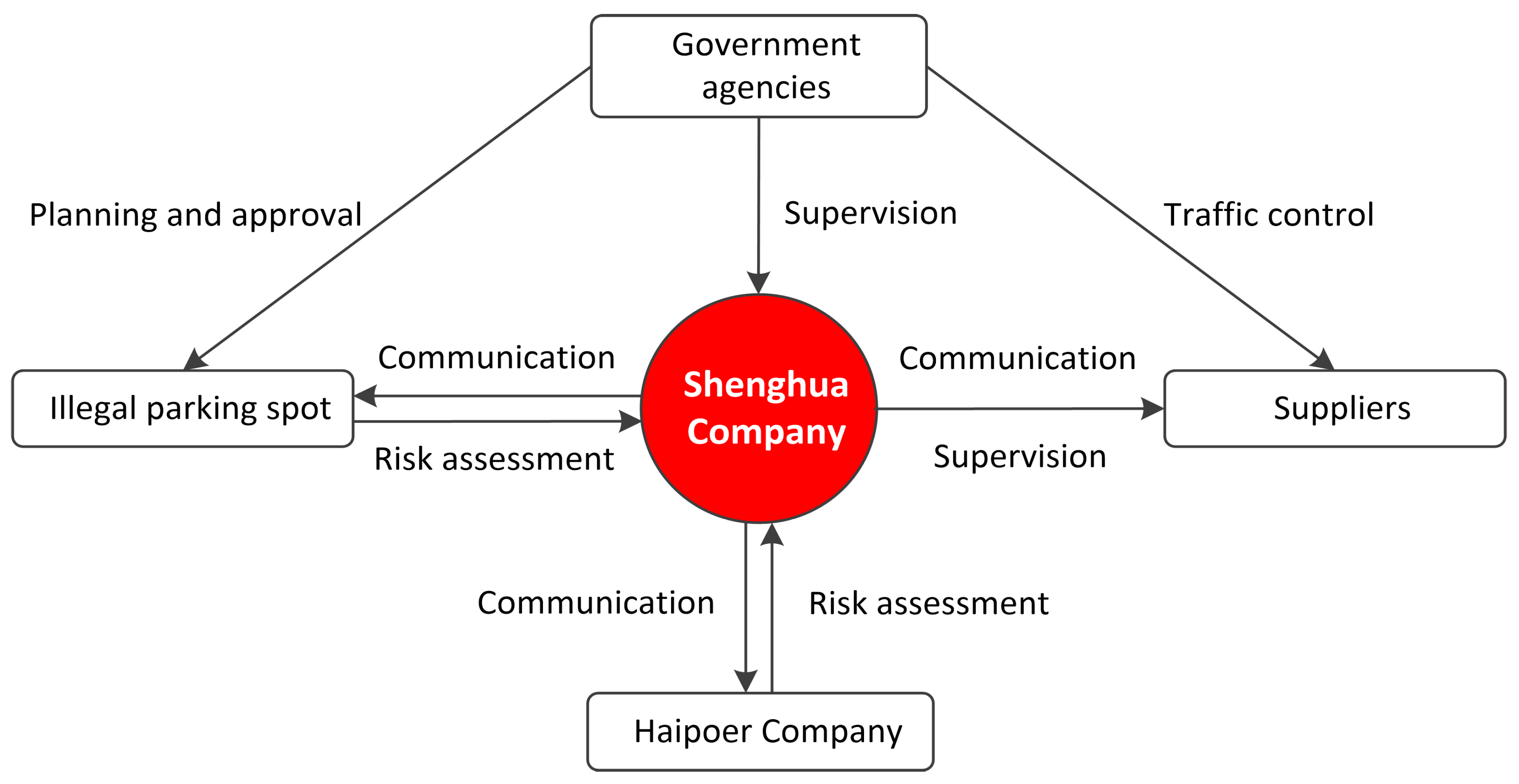
4.2. Involved Organizations
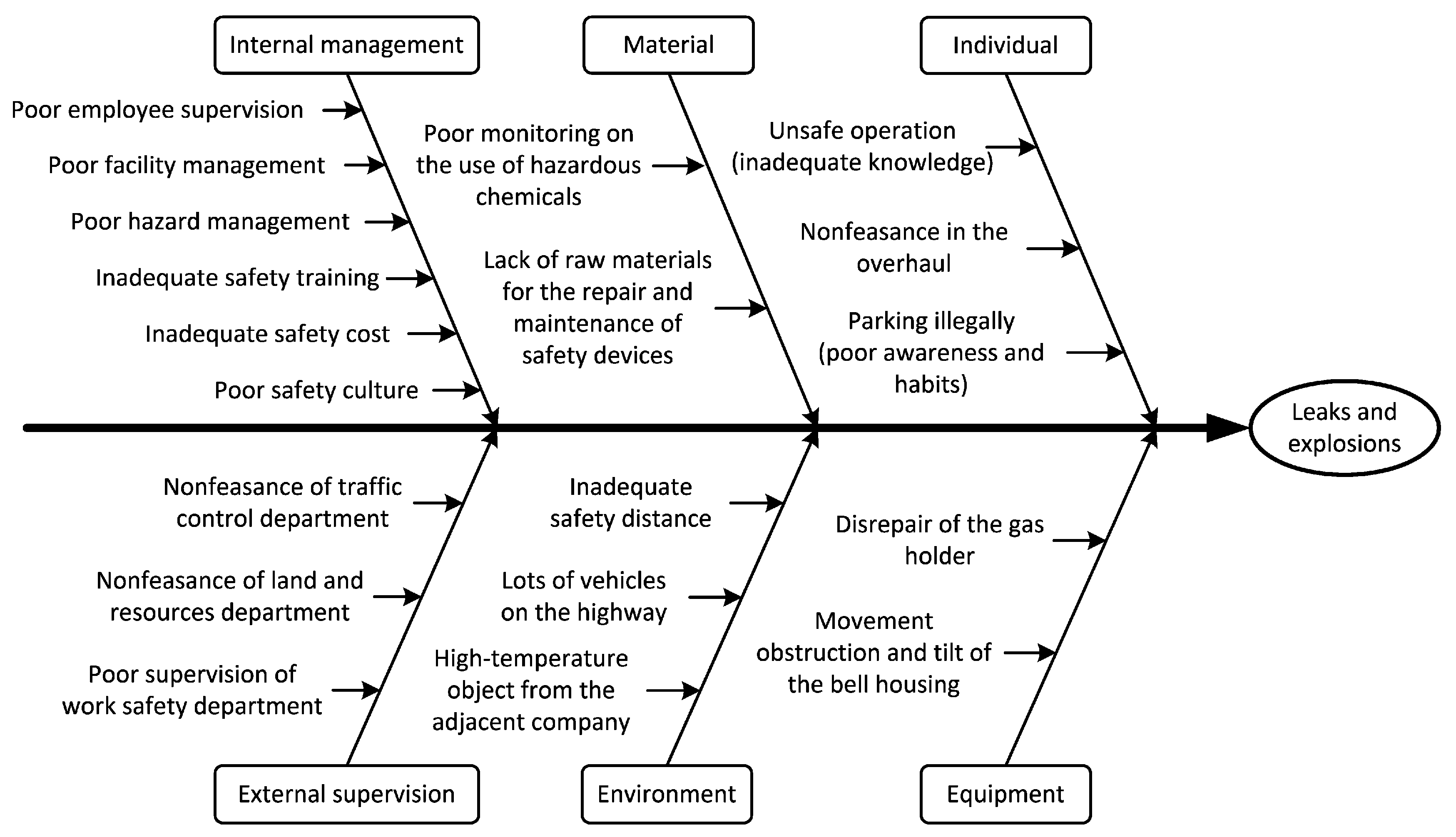
5. Causation Analysis and Discussion
5.1. Unsafe Acts at the Individual Level
5.2. Deficiencies in Organizational Safety Management
5.3. Safety Starts with the Design and Planning Stage
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jiang, J. Safety Technology and Management of Hazardous Chemicals; Chemical Industry Press: Beijing, China, 2015. [Google Scholar]
- Baybutt, P. The treatment of domino effects in process hazard analysis. Process. Saf. Prog. 2014, 34, 220–227. [Google Scholar] [CrossRef]
- Wang, J.; Fu, G.; Yan, M. Comparative analysis of two catastrophic hazardous chemical accidents in China. Process. Saf. Prog. 2020, 39, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.-M.; Chen, G. Modeling and algorithm of domino effect in chemical industrial parks using discrete isolated island method. Saf. Sci. 2011, 49, 463–467. [Google Scholar] [CrossRef]
- Ni, Z.-J.; Wang, Y.; Yin, Z. Relative risk model for assessing domino effect in chemical process industry. Saf. Sci. 2016, 87, 156–166. [Google Scholar] [CrossRef]
- Wang, J.; Yan, M. Application of an Improved Model for Accident Analysis: A Case Study. Int. J. Environ. Res. Public Health 2019, 16, 2756. [Google Scholar] [CrossRef] [Green Version]
- Tencent News. 1653 Accidents and 500 Deaths: An Inventory of the Top 10 Hazardous Chemical Accidents in China in 2019. Available online: https://new.qq.com/rain/a/20191228A075C200 (accessed on 3 February 2019).
- Zhu, Y.; Qian, X.; Liu, Z.; Huang, P.; Yuan, M. Analysis and assessment of the Qingdao crude oil vapor explosion accident: Lessons learnt. J. Loss Prev. Process. Ind. 2015, 33, 289–303. [Google Scholar] [CrossRef]
- Fu, G.; Chen, P.; Zhao, Z.; Li, R. Safety is about doing the right thing. Process. Saf. Prog. 2019, 38, 1–4. [Google Scholar] [CrossRef]
- Broadribb, M.P. What have we really learned? Twenty five years after Piper Alpha. Process. Saf. Prog. 2014, 34, 16–23. [Google Scholar] [CrossRef]
- Accident Investigation Report of Hebei Shenghua Company ’’11•28’’ Vinyl Chloride Leaks and Explosions. Available online: http://yjgl.hebei.gov.cn/portal/index/getPortalNewsDetails?id=7bde0d83-7ff3-4108-9d92-385083c97da8&categoryid=3a9d0375-6937-4730-bf52-febb997d8b48 (accessed on 3 February 2019).
- Fu, G.; Wang, J.; Yan, M. Anatomy of Tianjin Port fire and explosion: Process and causes. Process. Saf. Prog. 2016, 35, 216–220. [Google Scholar] [CrossRef]
- Benner, L. Accident investigation data: Users’ unrecognized challenges. Saf. Sci. 2019, 118, 309–315. [Google Scholar] [CrossRef]
- Greenwood, M.; Woods, H.M. The Incidence of Industrial Accidents upon Individuals with Specific Reference to Multiple Accidents; Report No. 4; Industrial Fatigue Research Board: London, UK, 1919. [Google Scholar]
- Heinrich, H.W.; Petersen, D.; Roos, N.R. Industrial Accident Prevention: A Safety Management Approach, 5th ed.; McGraw-Hill Companies: New York, NY, USA, 1980. [Google Scholar]
- Bird, F.E.J.; Germain, G.L.; Clark, D.M. Practical Loss Control Leadership; Det Norske Veritas; Inc.: Duluth, GA, USA, 2003. [Google Scholar]
- Rasmussen, J. Risk management in a dynamic society: A modelling problem. Saf. Sci. 1997, 27, 183–213. [Google Scholar] [CrossRef]
- Reason, J. Human Error; Cambridge University Press: New York, NY, USA, 1990. [Google Scholar]
- Wiegmann, D.A.; Shappell, S.A. A Human Error Approach to Aviation Accident Analysis–The Human Factors Analysis and Classification System; Ashgate Publishing Ltd.: Burlington, UK, 2003. [Google Scholar]
- Patterson, J.M.; Shappell, S.A. Operator error and system deficiencies: Analysis of 508 mining incidents and accidents from Queensland, Australia using HFACS. Accid. Anal. Prev. 2010, 42, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Leveson, N. A new accident model for engineering safer systems. Saf. Sci. 2004, 42, 237–270. [Google Scholar] [CrossRef] [Green Version]
- Leveson, N.G. Applying systems thinking to analyze and learn from events. Saf. Sci. 2011, 49, 55–64. [Google Scholar] [CrossRef]
- Lenné, M.G.; Salmon, P.M.; Liu, C.C.; Trotter, M. A systems approach to accident causation in mining: An application of the HFACS method. Accid. Anal. Prev. 2012, 48, 111–117. [Google Scholar] [CrossRef]
- Chauvin, C.; Lardjane, S.; Mörel, G.; Clostermann, J.-P.; Langard, B. Human and organisational factors in maritime accidents: Analysis of collisions at sea using the HFACS. Accid. Anal. Prev. 2013, 59, 26–37. [Google Scholar] [CrossRef]
- Fu, G.; Yin, W.; Dong, J.; Di, F. Behavior-based accident causation: The 24Model and its safety implication in coal mines. J. China Coal Soc. 2013, 38, 1123–1129. [Google Scholar]
- Fu, G.; Zhao, Z.; Hao, C.; Wu, Q. The Accident Path of Coal Mine Gas Explosion Based on 24Model: A Case Study of the Ruizhiyuan Gas Explosion Accident. Processes 2019, 7, 73. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Gong, Y.; Fu, G. Causes classification and statistical analysis on falling accidents on construction sites based on “2-4” model. J. Saf. Sci. Technol. 2017, 13, 169–174. [Google Scholar]
- Xue, Y.; Fu, G. A modified accident analysis and investigation model for the general aviation industry: Emphasizing on human and organizational factors. J. Saf. Res. 2018, 67, 1–15. [Google Scholar] [CrossRef]
- Suo, X.; Fu, G.; Wang, C.; Jia, Q. An Application of 24Model to Analyse Capsizing of the Eastern Star Ferry. Pol. Marit. Res. 2017, 24, 116–122. [Google Scholar] [CrossRef] [Green Version]
- Fu, G. Safety Management—A Behavior-Based Approach to Accident Prevention; Science Press: Beijing, China, 2013. [Google Scholar]
- Fu, G.; Fan, Y.; Tong, R.; Gong, Y. A Universal Methodology for the Causation Analysis of Accidents. J. Accid. Prev. 2016, 2, 7–12. [Google Scholar]
- Fu, G.; Lu, B.; Chen, X. Behavior Based Model for Organizational Safety Management. China Saf. Sci. J. 2005, 15, 21–27. [Google Scholar]
- Fu, G.; Zhou, L.; Wang, J.; Shi, M. Analysis of an explosion accident at Dangyang Power Plant in Hubei, China: Causes and lessons learned. Saf. Sci. 2018, 102, 134–143. [Google Scholar] [CrossRef]
- Hale, A.R. Culture’s confusions. Saf. Sci. 2000, 34, 1–14. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). Occupational Health and Safety Management Systems—Requirements with Guidance for Use; ISO Press: Geneva, Switzerland, 2018. [Google Scholar]
- Mearns, K.; Kirwan, B.; Reader, T.W.; Jackson, J.; Kennedy, R.; Gordon, R. Development of a methodology for understanding and enhancing safety culture in Air Traffic Management. Saf. Sci. 2013, 53, 123–133. [Google Scholar] [CrossRef]
- Silla, I.; Navajas, J.; Koves, G.K. Organizational culture and a safety-conscious work environment: The mediating role of employee communication satisfaction. J. Saf. Res. 2017, 61, 121–127. [Google Scholar] [CrossRef]
- Sun, W.; Guo, X.; Li, Y. Safety Technology for Hazardous Chemicals—General Volume, 3rd ed.; Chemical Industry Press: Beijing, China, 2017. [Google Scholar]
- Li, G.; Yang, H.-X.; Yuan, C.-M.; Eckhoff, R. A catastrophic aluminium-alloy dust explosion in China. J. Loss Prev. Process. Ind. 2016, 39, 121–130. [Google Scholar] [CrossRef]
- Abdolhamidzadeh, B.; Hassan, C.R.C.; Hamid, M.D.; FarrokhMehr, S.; Badri, N.; Rashtchian, D. Anatomy of a domino accident: Roots, triggers and lessons learnt. Process. Saf. Environ. Prot. 2012, 90, 424–429. [Google Scholar] [CrossRef]
- Ogle, R.; Ramirez, J.C.; Hetrick, T.M. Domino effect in a catastrophic solid oxidizer fire. Process. Saf. Prog. 2014, 34, 167–171. [Google Scholar] [CrossRef]
- Ishikawa, K.; Lu, D.J. What Is Total Quality Control? Prentice-Hall Inc.: Englewood Cliffs, NJ, USA, 1985. [Google Scholar]
- Luo, T.; Wu, C.; Duan, L. Fishbone diagram and risk matrix analysis method and its application in safety assessment of natural gas spherical tank. J. Clean. Prod. 2018, 174, 296–304. [Google Scholar] [CrossRef]
- Liaw, H.-J. Lessons in process safety management learned from a pesticide plant explosion in Taiwan. Process. Saf. Prog. 2017, 37, 104–109. [Google Scholar] [CrossRef]
- Murphy, J.F. Emergency Management: It Starts with a Question in the Design Stages “What Can Go Wrong?”. Process Saf. Prog. 2017, 36, 325. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | City Where Accidents Occurred | Accident Classification | Process | Deaths | Injuries |
|---|---|---|---|---|---|
| 2013 | Qingdao, Shandong | Leak and explosion of the crude oil | Transport | 62 | 136 |
| 2014 | Suzhou, Jiangsu | Explosion of aluminum-alloy dust | Production | 97 | 163 |
| 2015 | Tianjin Port | Spontaneous combustion of nitrocellulose and explosion of ammonium nitrate | Storage | 173 | 798 |
| 2015 | Dongying, Shandong | Explosion of mixed dinitrobenzene process unit | Production | 13 | 25 |
| 2017 | Lianyungang, Jiangsu | Leak and explosion of M-dichlorobenzene process unit | Production | 10 | 1 |
| 2017 | Linyi, Shandong | Leak and explosion of the liquefied petroleum gas tanker | Loading and unloading | 10 | 9 |
| 2018 | Yibin, Hubei | Explosion of butylamide, sodium chlorate, methylbenzene, etc. | Production | 19 | 12 |
| 2018 | Zhangjiakou, Hebei | Leak and explosion of chloroethylene | Production | 24 | 21 |
| 2019 | Sanmenxia, Henan | Leak of liquid oxygen and explosion of combustible materials | Production | 15 | 16 |
| 2019 | Yancheng, Jiangsu | Spontaneous combustion and explosion of nitrification wastes | Storage | 78 | 716 |
| No. | Unsafe Acts | Consequences | Violations of Relevant Laws and Regulations |
|---|---|---|---|
| 1 | Not having the gas holder overhauled within 6 years. | The bell housing was in a tilted and stagnated state, which was considered a crucial factor causing the leak of vinyl chloride. | In violation of the Regulations for Maintenance and Overhaul of Gas Holders: the period of maintenance and overhaul of gas holders is generally 2–5 years; In violation of the Regulations for Maintenance and Overhaul of Low Pressure Wet-type Gas Holders in Shenghua Company: the medium maintenance period of gas holders is 1–2 years, and the overhaul period is 5–6 years. |
| 2 | Adjusting the return valve of the compressor sharply. | The vinyl chloride broke through the annular water seal and leaked in large quantities. | It was a high-risk act that violated the organizational standard operating procedure that stipulates the matters needing attention in the operation of various equipment. |
| 3 | Improper use and management of gas detection device (e.g., operating roughly, turning off alarm devices frequently). | The gas detection device malfunctioned and did not alert the operator when vinyl chloride leaked. | In violation of the Interim Regulations on the Supervision of Major Hazard Installations for Dangerous Chemicals: major hazard installations should be equipped with reliable monitoring and alarm devices for the leak of combustible and toxic gases, and those devices should have the functions of information transmission, continuous records, accident alerts, as well as information storage. |
| 4 | Parking illegally. | The vehicles were ignited one after another, which expanded the casualties and property losses. | In violation of the safety signs set by the government traffic control department: ten no-parking signs were dispersedly set on Provincial Highway 310 close to the side of Shenghua Company to warn drivers. |
| No. | Safety Management System Elements | Specific Deficiencies | Stipulations in Relevant Laws and Regulations |
|---|---|---|---|
| 1 | Organizational structure and staff allocation |
| Article 21 in the Production Safety Law of the People’s Republic of China: the business entity that produces, manages, and stores hazardous substances shall set up a specialized safety management organization or have sufficient full-time safety management personnel. |
| 2 | Safety responsibility |
| Article 22 in the Production Safety Law of the PRC: both the safety management organization and the safety management personnel of the business entities shall perform their respective accountabilities (total 7 articles). |
| 3 | Safety investment |
| Article 20 in the Production Safety Law of the PRC: business entities shall create a special account for safety costs, and invest sufficient capitals for the safe production every year; meanwhile, the management shall extract the funds strictly in accordance with the provisions, and cannot use them for other purposes. |
| 4 | Facilities management |
| Regulations for the Maintenance and Overhaul of Low Pressure Wet-type Gas Holders in Shenghua Company: the medium maintenance period of gas holders is 1–2 years, and the overhaul period is 5–6 years. Article 13 in the Interim Provisions on the Supervision of Major Hazard Installations for Dangerous Chemicals: major hazard installations shall be equipped with an uninterrupted collection and monitoring system for the temperature, pressure, liquid level, flow and composition, as well as a gas leak detection and alarm device, with functions of information transmission, continuous record, accidents alert, as well as information storage. |
| 5 | Hazard identification |
| Article 38 in the Production Safety Law of the PRC: business entities shall establish a perfect hazards identification and elimination system, and take technological and management measures to discover and eliminate the potential hazards that may cause an accident in a timely manner; meanwhile, the detailed information about the hazards should be accurately recorded and promptly informed to the employees. |
| 6 | Training and education |
| Article 25 in the Production Safety Law of the PRC: business entities shall provide adequate safety education and training programs to employees to ensure that they master necessary safety theory knowledge and safety operation skills, and are familiar with relevant safety regulations, operating procedures and emergency measures. |
| 7 | Emergency disposal |
| Article 12 in the Measures for the Administration of Emergency Plans for Production Safety Accidents: business entities shall, in accordance with the relevant laws, regulations, and standards, as well as in combination with their own safety management system, production scale, and the characteristics of possible accidents, establish a feasible emergency response plan. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Fu, G.; Yan, M. Investigation and Analysis of a Hazardous Chemical Accident in the Process Industry: Triggers, Roots, and Lessons Learned. Processes 2020, 8, 477. https://doi.org/10.3390/pr8040477
Wang J, Fu G, Yan M. Investigation and Analysis of a Hazardous Chemical Accident in the Process Industry: Triggers, Roots, and Lessons Learned. Processes. 2020; 8(4):477. https://doi.org/10.3390/pr8040477
Chicago/Turabian StyleWang, Jianhao, Gui Fu, and Mingwei Yan. 2020. "Investigation and Analysis of a Hazardous Chemical Accident in the Process Industry: Triggers, Roots, and Lessons Learned" Processes 8, no. 4: 477. https://doi.org/10.3390/pr8040477