
Customized Cost-Effective Cranioplasty for Large Asymmetrical Defects
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
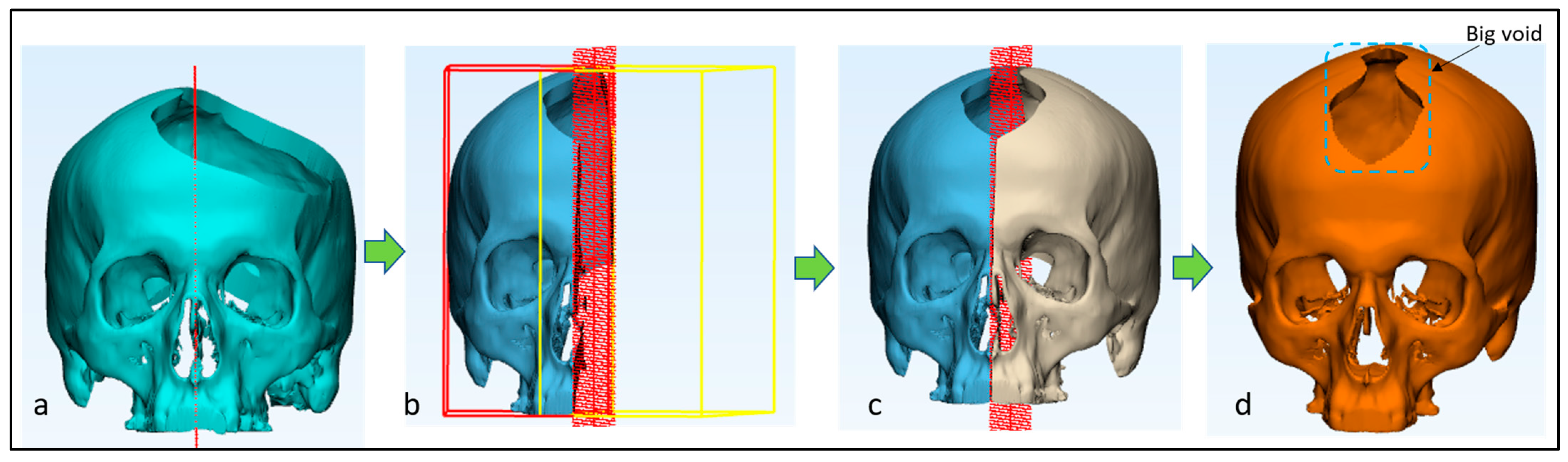
2.1. Image Processing and Creation of Artificial Defect
2.2. Skull and Implant Design
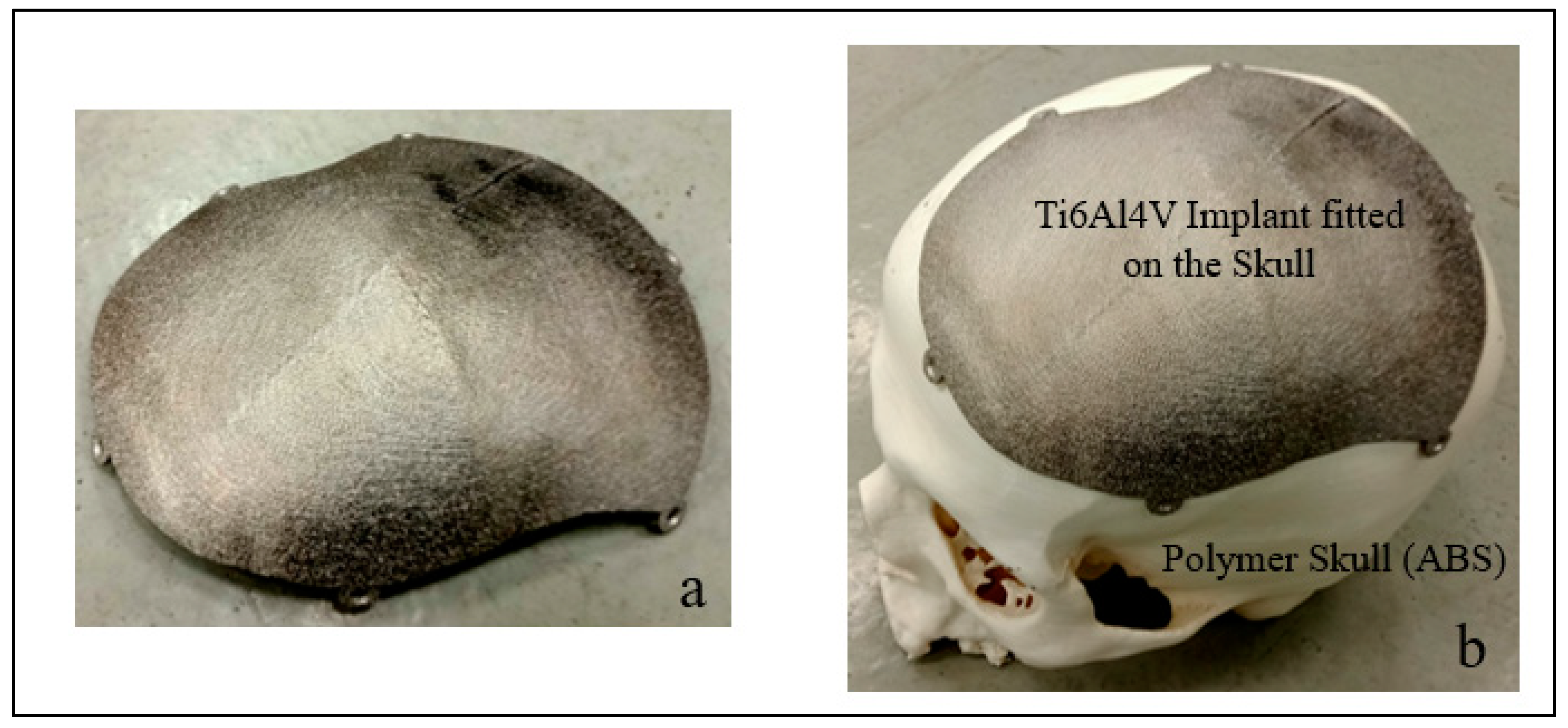
2.3. Fabrication
- Preheating/sintering the powder;
- Melting with focused electron beam;
- Lowering the build platform;
- Raking the powder.
2.4. EBM-Built Cranial Implant Cost and Time Analysis
2.5. Implant Accuracy Evaluation
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jeyaraj, P. Split Calvarial Grafting for Closure of Large Cranial Defects: The Ideal Option? J. Maxillofac. Oral Surg. 2019, 18, 518–530. [Google Scholar] [CrossRef]
- Iaccarino, C.; Kolias, A.G.; Roumy, L.-G.; Fountas, K.; Adeleye, A.O. Cranioplasty Following Decompressive Craniectomy. Front. Neurol. 2020, 10, 1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, S.; Kuether, J.; Fong, A.; Reid, R. Cranioplasty for Large-Sized Calvarial Defects in the Pediatric Population: A Review. Craniomaxillofac. Trauma Reconstr. 2015, 8, 159–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thimukonda Jegadeesan, J.; Baldia, M.; Basu, B. Next-Generation Personalized Cranioplasty Treatment. Acta Biomater. 2022, 154, 63–82. [Google Scholar] [CrossRef] [PubMed]
- Parthasarathy, J. 3D Modeling, Custom Implants and Its Future Perspectives in Craniofacial Surgery. Ann. Maxillofac. Surg. 2014, 4, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandolini, M.; Caragiuli, M.; Brunzini, A.; Mazzoli, A.; Pagnoni, M. A Procedure for Designing Custom-Made Implants for Forehead Augmentation in People Suffering from Apert Syndrome. J. Med. Syst. 2020, 44, 146. [Google Scholar] [CrossRef]
- Zuo, W.; Yu, L.; Lin, J.; Yang, Y.; Fei, Q. Properties Improvement of Titanium Alloys Scaffolds in Bone Tissue Engineering: A Literature Review. Ann. Transl. Med. 2021, 9, 1259. [Google Scholar] [CrossRef]
- Sarraf, M.; Rezvani Ghomi, E.; Alipour, S.; Ramakrishna, S.; Liana Sukiman, N. A State-of-the-Art Review of the Fabrication and Characteristics of Titanium and Its Alloys for Biomedical Applications. Bio-Des. Manuf. 2022, 5, 371–395. [Google Scholar] [CrossRef]
- do Nascimento, J.P.L.; Ferreira, M.O.A.; Gelamo, R.V.; Scarmínio, J.; Steffen, T.T.; da Silva, B.P.; Aoki, I.V.; dos Santos Jr, A.G.; de Castro, V.V.; de Fraga Malfatti, C.; et al. Enhancing the Corrosion Protection of Ti-6Al-4V Alloy through Reactive Sputtering Niobium Oxide Thin Films. Surf. Coat. Technol. 2021, 428, 127854. [Google Scholar] [CrossRef]
- Ni, J.; Ling, H.; Zhang, S.; Wang, Z.; Peng, Z.; Benyshek, C.; Zan, R.; Miri, A.K.; Li, Z.; Zhang, X.; et al. Three-Dimensional Printing of Metals for Biomedical Applications. Mater. Today Bio. 2019, 3, 100024. [Google Scholar] [CrossRef]
- Bozkurt, Y.; Karayel, E. 3D Printing Technology; Methods, Biomedical Applications, Future Opportunities and Trends. J. Mater. Res. Technol. 2021, 14, 1430–1450. [Google Scholar] [CrossRef]
- Chunhua, S.; Guangqing, S. Application and Development of 3D Printing in Medical Field. Mod. Mech. Eng. 2020, 10, 25–33. [Google Scholar] [CrossRef]
- Egger, J.; Gall, M.; Tax, A.; Üçal, M.; Zefferer, U.; Li, X.; von Campe, G.; Schäfer, U.; Schmalstieg, D.; Chen, X. Interactive Reconstructions of Cranial 3D Implants under MeVisLab as an Alternative to Commercial Planning Software. PLoS ONE 2017, 12, 20. [Google Scholar] [CrossRef] [PubMed]
- Dreizin, D.; Nam, A.J.; Hirsch, J.; Bernstein, M.P. New and Emerging Patient-Centered CT Imaging and Image-Guided Treatment Paradigms for Maxillofacial Trauma. Emerg. Radiol. 2018, 25, 533–545. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-T.; Yang, Y.-H.; Chang, Y.-Z. Three-Dimensional Deep Learning to Automatically Generate Cranial Implant Geometry. Sci. Rep. 2022, 12, 2683. [Google Scholar] [CrossRef]
- Johnston, D.T.; Lohmeier, S.J.; Langdell, H.C.; Pyfer, B.J.; Komisarow, J.; Powers, D.B.; Erdmann, D. Current Concepts in Cranial Reconstruction: Review of Alloplastic Materials. Plast. Reconstr. Surg.–Glob. Open 2022, 10, e4466. [Google Scholar] [CrossRef]
- Murr, L.E.; Gaytan, S.M.; Martinez, E.; Medina, F.; Wicker, R.B. Next Generation Orthopaedic Implants by Additive Manufacturing Using Electron Beam Melting. Available online: https://www.hindawi.com/journals/ijbm/2012/245727/ (accessed on 3 February 2021).
- Ti6Al4V ELI Titanium Alloy-Arcam-PDF Catalogs|Technical Documentation|Brochure. Available online: https://pdf.directindustry.com/pdf/arcam/ti6al4v-eli-titanium-alloy/19734-503505-_2.html (accessed on 20 February 2023).
- Arthur, N.K.K.; Pityana, S. Microstructure and Material Properties of LENS Fabricated Ti-6Al-4V Components. RD J. 2018, 34, 33–36. [Google Scholar]
- Kadir, A.Z.A.; Yusof, Y.; Wahab, M.S. Additive Manufacturing Cost Estimation Models—A Classification Review. Int. J. Adv. Manuf. Technol. 2020, 107, 4033–4053. [Google Scholar] [CrossRef]
- Mahadik, A.; Masel, D. Implementation of Additive Manufacturing Cost Estimation Tool (AMCET) Using Break-down Approach. Procedia Manuf. 2018, 17, 70–77. [Google Scholar] [CrossRef]
- Syam, W.; Al-Ahmari, A.; Mannan, M.; Al-Shehri, H.; Al-Wazzan, K. Metallurgical, Accuracy and Cost Analysis of Ti6Al4V Dental Coping Fabricated by Electron Beam Melting Process. In Proceedings of the 5th International Conference on Advanced Research in Virtual and Rapid Prototyping, Leiria, Portugal, 28 September–1 October 2011; ISBN 978-0-415-68418-7. [Google Scholar]
- Pushparaj, R.M.; Aravind Raj, S.; Jayakrishna, K.; Vezhavendhan, R. Analyzing the Cost Drivers and Process Optimization in Additive Manufacturing. IOP Conf. Ser. Mater. Sci. Eng. 2019, 561, 012062. [Google Scholar] [CrossRef]
- Priarone, P.C.; Robiglio, M.; Ingarao, G.; Settineri, L. Assessment of Cost and Energy Requirements of Electron Beam Melting (EBM) and Machining Processes. In Sustainable Design and Manufacturing 2017; Campana, G., Howlett, R.J., Setchi, R., Cimatti, B., Eds.; Smart Innovation, Systems and Technologies; Springer International Publishing: Cham, Switzerland, 2017; Volume 68, pp. 723–735. ISBN 978-3-319-57077-8. [Google Scholar]
- Thomas, D. Costs, Benefits, and Adoption of Additive Manufacturing: A Supply Chain Perspective. Int. J. Adv. Manuf. Technol. 2016, 85, 1857–1876. [Google Scholar] [CrossRef] [Green Version]
- Arcam A2 Setting the Standard for Additive Manufacturing. Available online: http://www.arcam.com/wp-content/uploads/Arcam-A2.pdf (accessed on 12 July 2019).
- Wycisk, E.; Munsch, M.; Schmidt-Lehr, M. Ampower Insights: Additive Manufacturing-Make or Buy; Ampower Insights: Hamburg, Germany, 2017. [Google Scholar]
- Binhammer, A.; Jakubowski, J.; Antonyshyn, O.; Binhammer, P. Comparative Cost-Effectiveness of Cranioplasty Implants. Plast. Surg. 2020, 28, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Azad, T.D.; Veeravagu, A.; Bhatti, I.; Long, C.; Ratliff, J.K.; Li, G. Cranioplasty Complications and Costs: A National Population-Level Analysis Using the MarketScan Longitudinal Database. World Neurosurg. 2017, 102, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Kinsman, M.; Aljuboori, Z.; Ball, T.; Nauta, H.; Boakye, M. Rapid High-Fidelity Contour Shaping of Titanium Mesh Implants for Cranioplasty Defects Using Patient-Specific Molds Created with Low-Cost 3D Printing: A Case Series. Surg. Neurol. Int. 2020, 11, 288. [Google Scholar] [CrossRef] [PubMed]
- De La Peña, A.; De La Peña-Brambila, J.; Pérez-De La Torre, J.; Ochoa, M.; Gallardo, G.J. Low-Cost Customized Cranioplasty Using a 3D Digital Printing Model: A Case Report. 3D Print. Med. 2018, 4, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manrique, O.J.; Lalezarzadeh, F.; Dayan, E.; Shin, J.; Buchbinder, D.; Smith, M. Craniofacial Reconstruction Using Patient-Specific Implants Polyether Ether Ketone with Computer-Assisted Planning. J. Craniofac. Surg. 2015, 26, 663. [Google Scholar] [CrossRef]
- Mian, S.H.; Moiduddin, K.; Abdo, B.M.A.; Sayeed, A.; Alkhalefah, H. Modelling and Evaluation of Meshed Implant for Cranial Reconstruction. Int. J. Adv. Manuf. Technol. 2022, 118, 1967–1985. [Google Scholar] [CrossRef]
- Ferrari, R.; Figueira, W.F.; Pratchett, M.S.; Boube, T.; Adam, A.; Kobelkowsky-Vidrio, T.; Doo, S.S.; Atwood, T.B.; Byrne, M. 3D Photogrammetry Quantifies Growth and External Erosion of Individual Coral Colonies and Skeletons. Sci. Rep. 2017, 7, 16737. [Google Scholar] [CrossRef] [Green Version]
- Hammad Mian, S.; Abdul Mannan, M.; Al-Ahmari, A.M. The Influence of Surface Topology on the Quality of the Point Cloud Data Acquired with Laser Line Scanning Probe. Sens. Rev. 2014, 34, 255–265. [Google Scholar] [CrossRef]
- Hill, S.; Franco-Sepulveda, E.; Komeili, A.; Trovato, A.; Parent, E.; Hill, D.; Lou, E.; Adeeb, S. Assessing Asymmetry Using Reflection and Rotoinversion in Biomedical Engineering Applications. Proc. Inst. Mech. Eng. 2014, 228, 523–529. [Google Scholar] [CrossRef]
- Patete, P.; Eder, M.; Raith, S.; Volf, A.; Kovacs, L.; Baroni, G. Comparative Assessment of 3D Surface Scanning Systems in Breast Plastic and Reconstructive Surgery. Surg. Innov. 2013, 20, 509–515. [Google Scholar] [CrossRef]
- Herford, A.S.; Miller, M.; Lauritano, F.; Cervino, G.; Signorino, F.; Maiorana, C. The Use of Virtual Surgical Planning and Navigation in the Treatment of Orbital Trauma. Chin. J. Traumatol. Zhonghua Chuang Shang Za Zhi 2017, 20, 9–13. [Google Scholar] [CrossRef]
- Lor, L.S.; Massary, D.A.; Chung, S.A.; Brown, P.J.; Runyan, C.M. Cost Analysis for In-House versus Industry-Printed Skull Models for Acute Midfacial Fractures. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2831. [Google Scholar] [CrossRef] [PubMed]
- Moiduddin, K.; Mian, S.H.; Umer, U.; Alkhalefah, H. Fabrication and Analysis of a Ti6Al4V Implant for Cranial Restoration. Appl. Sci. 2019, 9, 2513. [Google Scholar] [CrossRef] [Green Version]
- Fuessinger, M.A.; Schwarz, S.; Cornelius, C.-P.; Metzger, M.C.; Ellis, E.; Probst, F.; Semper-Hogg, W.; Gass, M.; Schlager, S. Planning of Skull Reconstruction Based on a Statistical Shape Model Combined with Geometric Morphometrics. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 519–529. [Google Scholar] [CrossRef]
- Wittner, C.; Borowski, M.; Pirl, L.; Kastner, J.; Schrempf, A.; Schäfer, U.; Trieb, K.; Senck, S. Thickness Accuracy of Virtually Designed Patient-specific Implants for Large Neurocranial Defects. J. Anat. 2021, 239, 755–770. [Google Scholar] [CrossRef] [PubMed]
- Rana, M.; Moellmann, H.L.; Schorn, L.; Lommen, J.; Rana, M.; Wilkat, M.; Hufendiek, K. Primary Orbital Reconstruction with Selective Laser Melting (SLM) of Patient-Specific Implants (PSIs): An Overview of 96 Surgically Treated Patients. J. Clin. Med. 2022, 11, 3361. [Google Scholar] [CrossRef]
- Fuessinger, M.A.; Metzger, M.C.; Rothweiler, R.; Brandenburg, L.S.; Schlager, S. Cranial Reconstruction Evaluation-Comparison of European Statistical Shape Model Performance on Chinese Dataset. Bone Rep. 2022, 17, 101611. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Aluminum (Al) % | Vanadium (V) % | Titanium (Ti) % |
|---|---|---|---|
| Feed stock Powder [18] | 6.04 | 4.05 | 89.76 |
| ASTM F136 [19] | 5.5–6.5 | 3.5–4.5 | 88.48 |
| Titanium Implant | 6.24 | 3.89 | 89.87 |
| Cost Distribution Factors | |||
|---|---|---|---|
| Raw material cost | |||
| Material consumption (Grams) MConsumption | Weight of implant with supports | 81.46 g | |
| Mconsumption (Material consumed for cranial implant with supports) | 81.46 g | ||
| Raw material cost (Per gram) | RM cost (Ti6Al4V ELI cost price) | USD 0.24/gram | USD 240/kg |
| (MConsumption × RWCost) | Implant cost | USD 19.55 | (81.46 g × USD 0.24/g) |
| Energy consumption cost | |||
| Fabrication Time (Hours) FTime (Fabrication of cranial implant) | Time to obtain a desired vacuum level | 0:40 hh:mm | |
| Time to heat start plate | 0.50 hh:mm | ||
| EBM cool-down time | 4–6 hh:mm | Avg 5 h | |
| Build time for cranial implant | 4:50 hh:mm | ||
| FTime Time for completion of cranial implant | 11.33 h | Time for desired vacuum level + heating start plate + EBM cool down time + part build time (0:40 + 0:50 + 5:00 + 4:50) =11:20 hh:mm = 11.33 h | |
| EBM energy consumption (KW) for Implant fabrication EBuild | EBM Power supply | 7 KW [26] | |
| EBM Electricity cost (Per hour) ECost | ECost (Energy consumption cost for EBM) | USD 0.085/KWh | Electricity tariff = Sar 0.32/KWh “https://www.se.com.sa/en-us/customers/Pages/TariffRates.aspx (accessed on 24 December 2022)” Conversion of Sar to USD = USD 0.085/KWh |
| EBuild × FTime × ECost | Cranial implant with support | USD 6.74 | =(EBM power consumption × EBM built time for cranial implant with supports × EBM energy consumption cost) =7 KW × 11.33 h × USD 0.085/KWh |
| Machine running cost | |||
| Mcost (Machine running cost/h) | EBM machine running cost is EUR 32/h [27] | USD 33.78/h | |
| FTime (EBM running time) | EBM running time, which includes heating (0.50) and melting cycle (4.50) | 5.40 hh:mm | 5.66 h (5.40 hh:mm) |
| Mcost × FTime | EBM running cost for cranial implant | USD 191.19 | USD 33.78 × 5.66 |
| Total Cost for fabricating cranial implant | Cranial Implant cost | USD 217.50 | (Material cost + Energy consumption cost + EBM running cost) = USD19.55 + USD 6.74 + USD 191.19 |
| Implant Replicas | 1 | 2 | 3 | Mean (mm) |
|---|---|---|---|---|
| Modeling error d0 | 0.0718 | 0.0613 | 0.0866 | 0.0732 |
| Fabrication error d1 | ||||
| 1 | 0.5429 | 0.5590 | 0.5708 | |
| 2 | 0.5268 | 0.5652 | 0.6064 | |
| 3 | 0.5534 | 0.5743 | 0.5935 | |
| Mean | 0.5038 | 0.5588 | 0.5808 | 0.5613 |
| Overall customized implant accuracy | 0.6345 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moiduddin, K.; Mian, S.H.; Alkhalefah, H.; Ramalingam, S.; Sayeed, A. Customized Cost-Effective Cranioplasty for Large Asymmetrical Defects. Processes 2023, 11, 1760. https://doi.org/10.3390/pr11061760
Moiduddin K, Mian SH, Alkhalefah H, Ramalingam S, Sayeed A. Customized Cost-Effective Cranioplasty for Large Asymmetrical Defects. Processes. 2023; 11(6):1760. https://doi.org/10.3390/pr11061760
Chicago/Turabian StyleMoiduddin, Khaja, Syed Hammad Mian, Hisham Alkhalefah, Sundar Ramalingam, and Abdul Sayeed. 2023. "Customized Cost-Effective Cranioplasty for Large Asymmetrical Defects" Processes 11, no. 6: 1760. https://doi.org/10.3390/pr11061760