
The Effect of Mineralized Plasmatic Matrix and Chitosan on the Healing of Critical-Sized Mandibular Bone Defects in a Rabbit Model


 , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Animals
2.3. Animal Grouping
- (a)
- Control group (C): the defect was filled with sterile saline solution (Otsuka, Japan).
- (b)
- Chitosan group (Ch): the defect was filled by chitosan.
- (c)
- MPM group: defect was filled by MPM.
2.4. Surgical Procedures
2.5. Clinical Evaluation
2.5.1. Radiography and Radiographic Scoring
2.5.2. Histopathology
2.5.3. Immunohistochemical Procedures
2.6. Statistical Analysis
3. Results
3.1. Clinical Findings
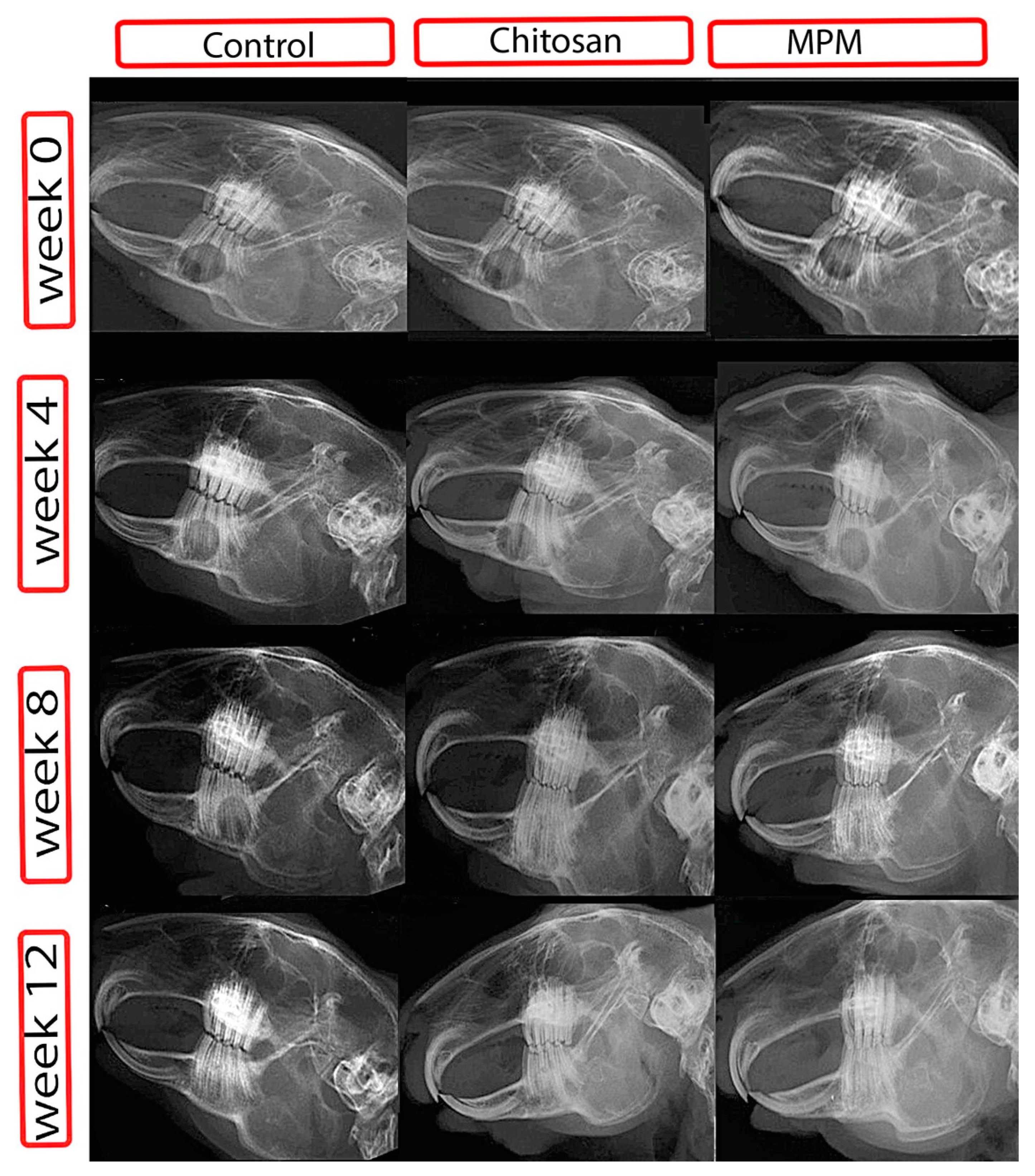
3.2. Radiographic Findings
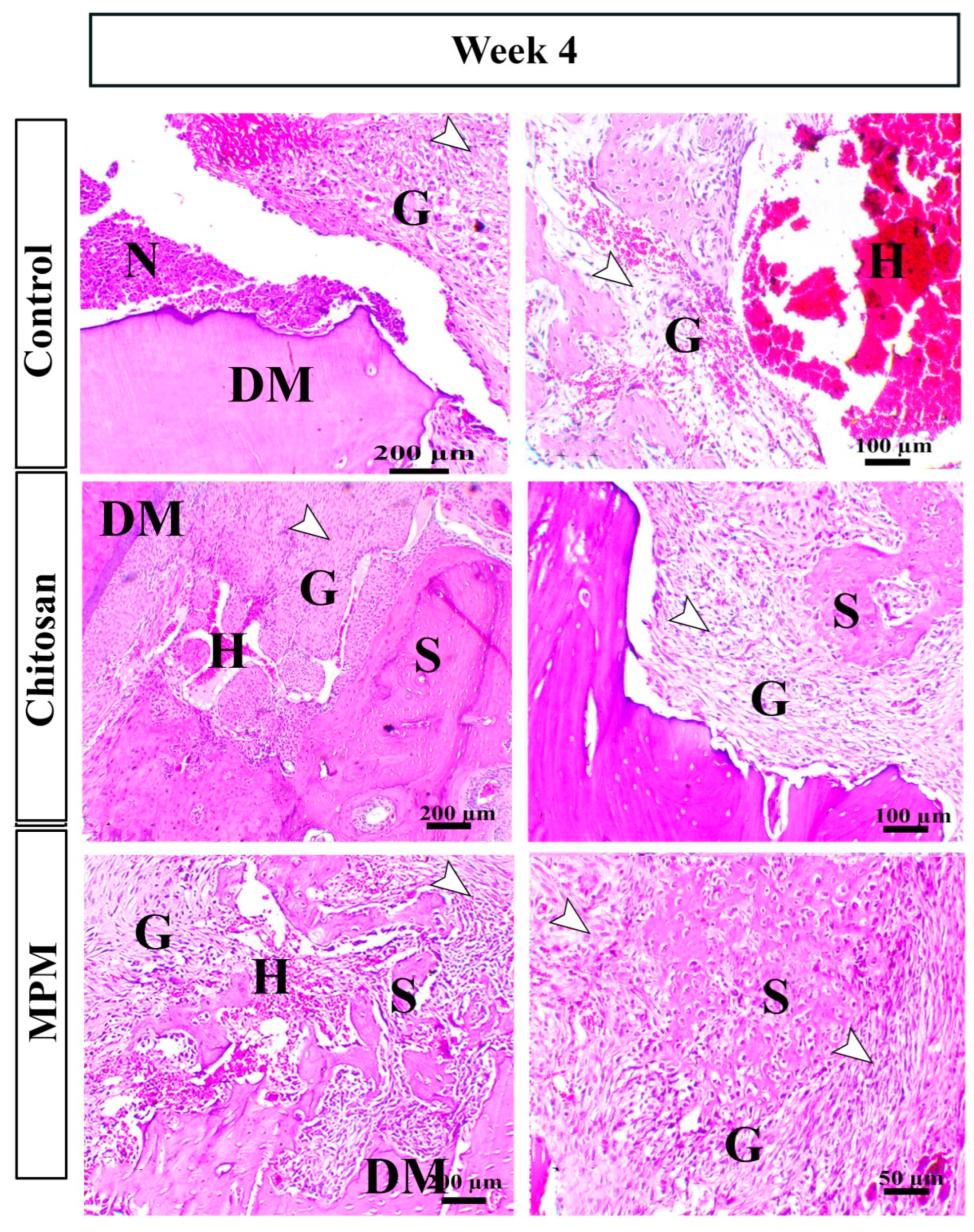
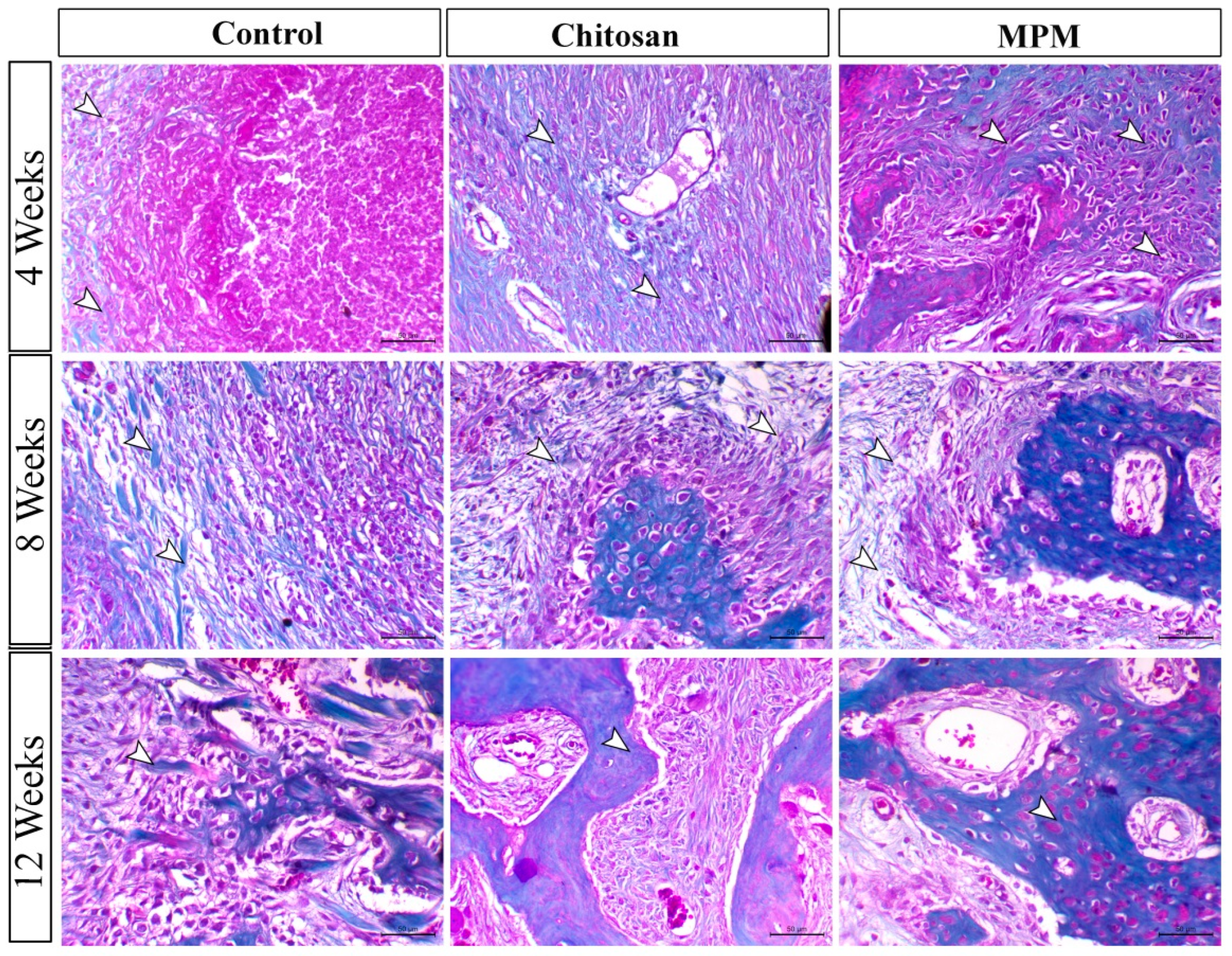
3.3. Histological Findings
3.3.1. H&E-Staining
3.3.2. Masson’s Trichrome Staining
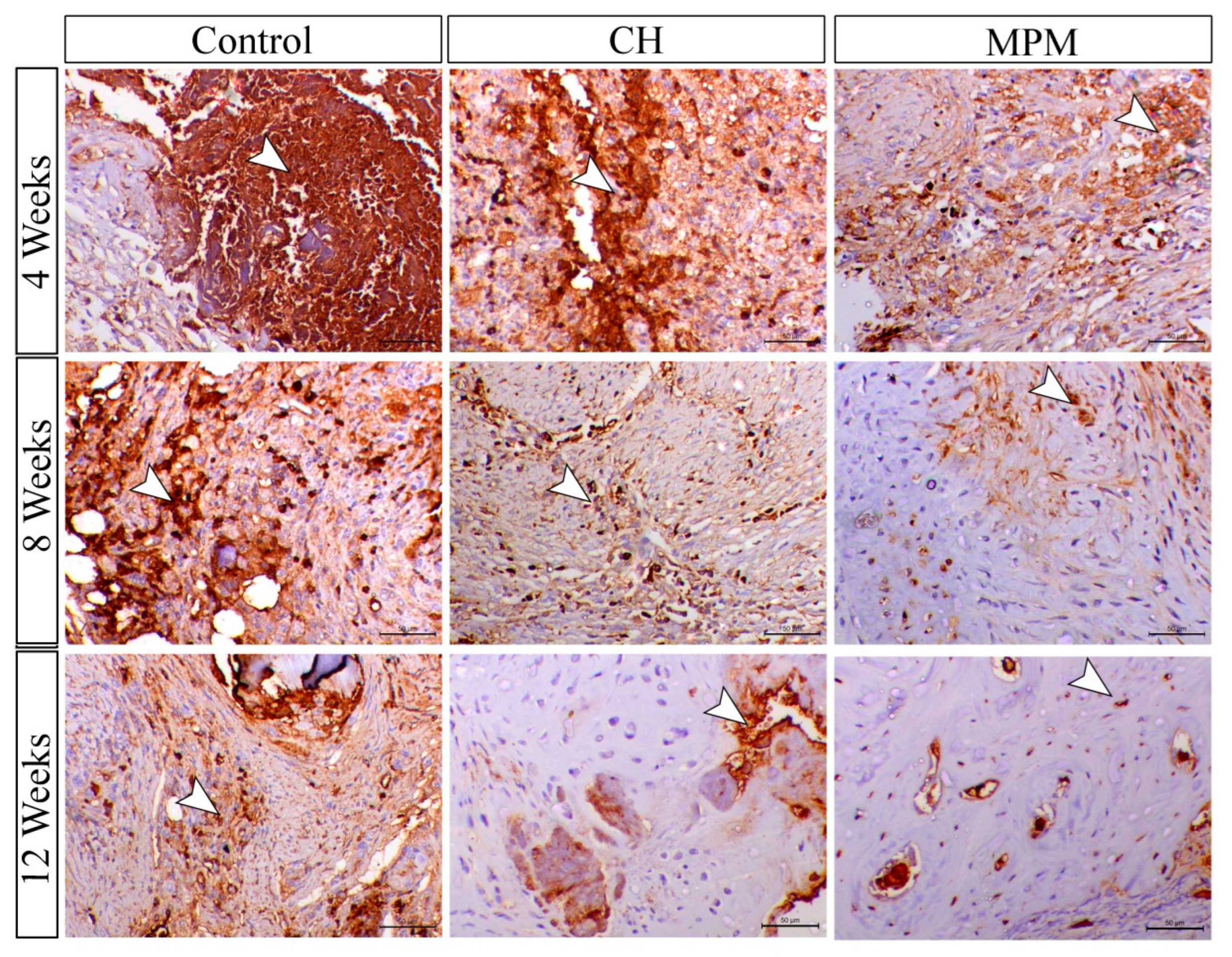
3.4. Immunohistochemical Findings
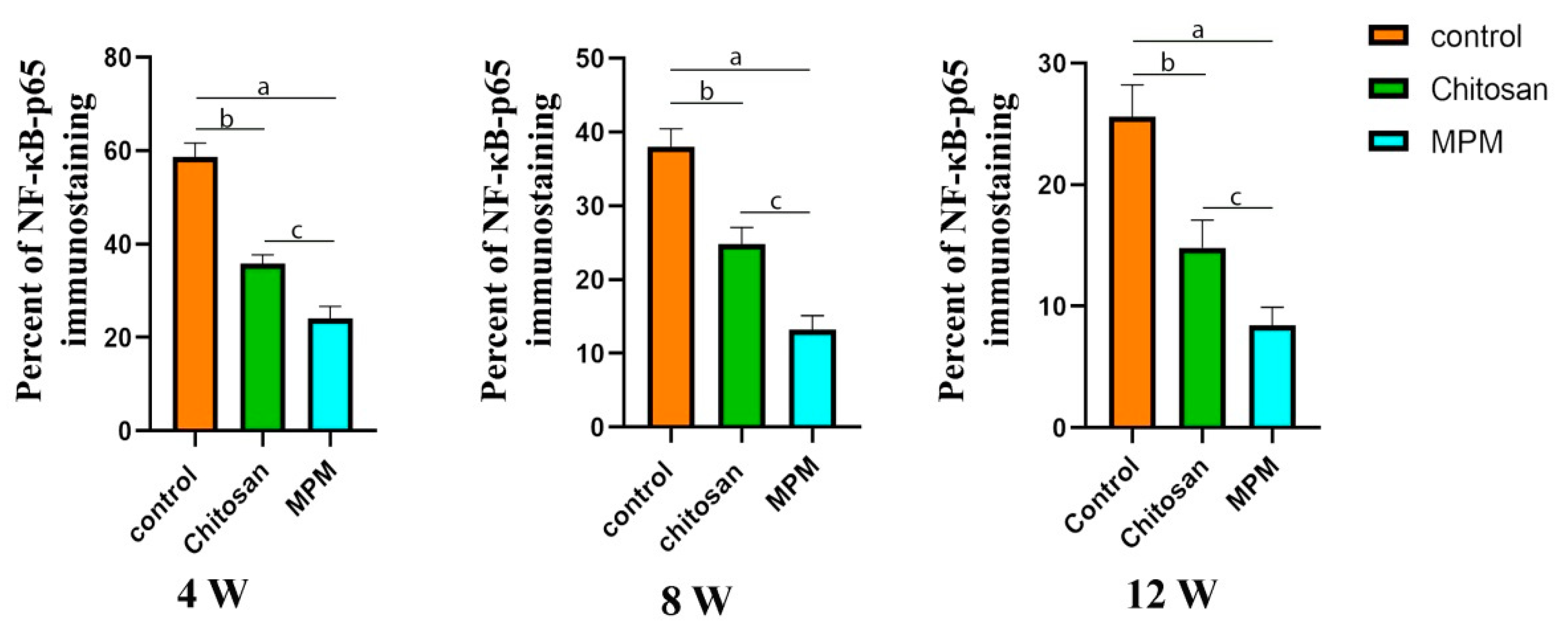
3.4.1. Nuclear Factor Immune Staining (NF-κB (P65))
3.4.2. Matrix Metalloproteinase-9 Immune Staining
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dimitriou, R.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Bone regeneration: Current concepts and future directions. BMC Med. 2011, 9, 66. [Google Scholar] [CrossRef] [PubMed]
- Holban, A.M.; Grumezescu, A. Materials for Biomedical Engineering: Hydrogels and Polymer-Based Scaffolds; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Oryan, A.; Alidadi, S.; Moshiri, A.; Maffulli, N. Bone regenerative medicine: Classic options, novel strategies, and future directions. J. Orthop. Surg. Res. 2014, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liu, J.; Wang, L.; Xie, A.; Liu, D. Bone histomorphometry detection of autologous bone powder graft repair of partial mandibular defects in rabbits. Genet. Mol. Res. 2015, 14, 13812–13822. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.P.; Venkatesh, V.; Kumar, K.; Yadav, B.Y.; Mohan, S.R. Mandibular reconstruction: Overview. J. Maxillofac. Oral Surg. 2016, 15, 425–441. [Google Scholar] [CrossRef]
- Zhang, Q.; Wu, W.; Qian, C.; Xiao, W.; Zhu, H.; Guo, J.; Meng, Z.; Zhu, J.; Ge, Z.; Cui, W. Advanced biomaterials for repairing and reconstruction of mandibular defects. Mater. Sci. Eng. C 2019, 103, 109858. [Google Scholar] [CrossRef]
- Saikia, K.; Bhattacharya, T.; Bhuyan, S.; Talukdar, D.; Saikia, S.; Jitesh, P. Calcium phosphate ceramics as bone graft substitutes in filling bone tumor defects. Indian J. Orthop. 2008, 42, 169. [Google Scholar] [CrossRef]
- Bauer, T.W.; Muschler, G.F. Bone graft materials: An overview of the basic science. Clin. Orthop. Relat. Res. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Denny, H.; Butterworth, S. A Guide to Canine and Feline Orthopaedic Surgery; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Campana, V.; Milano, G.; Pagano, E.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J. Mater. Sci. Mater. Med. 2014, 25, 2445–2461. [Google Scholar] [CrossRef]
- Zamiri, B.; Shahidi, S.; Eslaminejad, M.B.; Khoshzaban, A.; Gholami, M.; Bahramnejad, E.; Moghadasali, R.; Mardpour, S.; Aghdami, N. Reconstruction of human mandibular continuity defects with allogenic scaffold and autologous marrow mesenchymal stem cells. J. Craniofacial Surg. 2013, 24, 1292–1297. [Google Scholar] [CrossRef]
- Moshiri, A.; Shahrezaee, M.; Shekarchi, B.; Oryan, A.; Azma, K. Three-dimensional porous gelapin–simvastatin scaffolds promoted bone defect healing in rabbits. Calcif. Tissue Int. 2015, 96, 552–564. [Google Scholar] [CrossRef]
- Saravanan, S.; Leena, R.; Selvamurugan, N. Chitosan based biocomposite scaffolds for bone tissue engineering. Int. J. Biol. Macromol. 2016, 93, 1354–1365. [Google Scholar] [CrossRef] [PubMed]
- Soares, M.Q.S.; Van Dessel, J.; Jacobs, R.; Yaedú, R.Y.F.; Sant’Ana, E.; da Silva Corrêa, D.; Madeira, M.F.C.; Duarte, M.A.H.; Rubira-Bullen, I.R.F. Morphometric evaluation of bone regeneration in segmental mandibular bone defects filled with bovine bone xenografts in a split-mouth rabbit model. Int. J. Implant Dent. 2019, 5, 32. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, E.M. The use of growth factors fibrin network to enhance architecture, mechanical and biological aspect of the graft particles. Int. J. Prev. Clin. Dent. Res. 2014, 1, 41–44. [Google Scholar]
- Mudalal, M.; Zhou, Y. Biological additives and platelet concentrates for tissue engineering on regenerative dentistry basic Science and concise review. Asian J. Pharm. 2017, 11, 255–263. [Google Scholar]
- Weibrich, G.; Kleis, W.K.; Hafner, G. Growth factor levels in the platelet-rich plasma produced by 2 different methods: Curasan-type PRP kit versus PCCS PRP system. Int. J. Oral Maxillofac. Implant. 2002, 17, 184–190. [Google Scholar]
- Mehrabani, D.; Khodakaram-Tafti, A.; Shaterzadeh-Yazdi, H.; Zamiri, B.; Omidi, M. Comparison of the regenerative effect of adipose-derived stem cells, fibrin glue scaffold, and autologous bone graft in experimental mandibular defect in rabbit. Dent. Traumatol. 2018, 34, 413–420. [Google Scholar] [CrossRef]
- Amirthalingam, S.; Rajendran, A.K.; Mani, P.; Rangasamy, J. Perspectives and Challenges of Using Chitosan in Various Biological Applications. Chitosan Biomater. III 2021, 287, 1–22. [Google Scholar]
- Keating, J.F.; Simpson, A.; Robinson, C. The management of fractures with bone loss. J. Bone Jt. Surg. Br. Vol. 2005, 87, 142–150. [Google Scholar] [CrossRef]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Elgendy, M.; Elsayad, G.; Seleim, M.; Abdo, W.; Baty, R.S.; Elmahallawy, E.K.; Atiba, A. Flunixin Meglumine Enhanced Bone Fracture Healing in Rabbits Associated with Activation of Early Collagen Deposition and Enhancement of Vascular Endothelial Growth Factor Expression. Animals 2021, 11, 2834. [Google Scholar] [CrossRef]
- Alidadi, S.; Oryan, A.; Bigham-Sadegh, A.; Moshiri, A. Comparative study on the healing potential of chitosan, polymethylmethacrylate, and demineralized bone matrix in radial bone defects of rat. Carbohydr. Polym. 2017, 166, 236–248. [Google Scholar] [CrossRef] [PubMed]
- Ghanem, M.A.; Sharara, A.A.; Sweedan, A.O.; Khalil, N.M. Evaluation of using mineralized plasmatic matrix in osseous regeneration (experimental and histomorphometric study on rabbits). Alex. Dent. J. 2018, 43, 53–59. [Google Scholar] [CrossRef]
- Monir, A.; Mukaibo, T.; El-Aal, A.; Nodai, T.; Munemasa, T.; Kondo, Y.; Masaki, C.; El-Shair, M.A.; Matsuo, K.; Hosokawa, R. Local administration of HMGB-1 promotes bone regeneration on the critical-sized mandibular defects in rabbits. Sci. Rep. 2021, 11, 8950. [Google Scholar] [CrossRef] [PubMed]
- Segundo, F.A.d.S.; Costa, E.I.d.S.; Azevedo, A.S.d.; Araújo, A.L.d.; Silva, A.C.d.F.; de Lima, G.G.; de Sá, M.J.C. Platelet-rich plasma, hydroxyapatite, and chitosan in the bone and cartilaginous regeneration of femoral trochlea in rabbits: Clinical, radiographic, and histomorphometric evaluations. J. Healthc. Eng. 2018, 2018, 6917958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.R.; Young, S.; Goldman, J.L.; Jansen, J.A.; Wong, M.E.; Mikos, A.G. A composite critical-size rabbit mandibular defect for evaluation of craniofacial tissue regeneration. Nat. Protoc. 2016, 11, 1989–2009. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, A.; Zein, N.; Harmouch, E.; Hafdi, B.; Bornert, F.; Offner, D.; Clauss, F.; Fioretti, F.; Huck, O.; Benkirane-Jessel, N. Application of chitosan in bone and dental engineering. Molecules 2019, 24, 3009. [Google Scholar] [CrossRef] [PubMed]
- Al-Fotawei, R.; Ayoub, A.F.; Heath, N.; Naudi, K.B.; Tanner, K.E.; Dalby, M.J.; McMahon, J. Radiological assessment of bioengineered bone in a muscle flap for the reconstruction of critical-size mandibular defect. PLoS ONE 2014, 9, e107403. [Google Scholar] [CrossRef] [PubMed]
- Suvarna, K.S.; Layton, C.; Bancroft, J.D. Bancroft’s Theory and Practice of Histological Techniques E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Gholipour, H.; Meimandi-Parizi, A.; Oryan, A.; Bigham Sadegh, A. The effects of gelatin, fibrin-platelet glue and their combination on healing of the experimental critical bone defect in a rat model: Radiological, histological, scanning ultrastructural and biomechanical evaluation. Cell Tissue Bank. 2018, 19, 341–356. [Google Scholar] [CrossRef]
- Abdo, W.; Ghattas, S.; Sakai, H.; Hirata, A.; Yanai, T. Assessment of proliferative activity by proliferative cell nuclear antigen (PCNA) and anti-bromodeoxyuridine (BrdU) immunolabeling in the tissues of japanese eels (Anguilla japonica). Turk. J. Fish. Aquat. Sci. 2014, 14, 413–419. [Google Scholar] [CrossRef]
- Chang, S.-H.; Hsu, Y.-M.; Wang, Y.J.; Tsao, Y.-P.; Tung, K.-Y.; Wang, T.-Y. Fabrication of pre-determined shape of bone segment with collagen-hydroxyapatite scaffold and autogenous platelet-rich plasma. J. Mater. Sci. Mater. Med. 2009, 20, 23–31. [Google Scholar] [CrossRef]
- Lim, J.; Donahue, H.J. Biomaterial characteristics important to skeletal tissue engineering. J. Musculoskelet. Neuronal Interact. 2004, 4, 396. [Google Scholar] [PubMed]
- Thomaidis, V.; Kazakos, K.; Lyras, D.N.; Dimitrakopoulos, I.; Lazaridis, N.; Karakasis, D.; Botaitis, S.; Agrogiannis, G. Comparative study of 5 different membranes for guided bone regeneration of rabbit mandibular defects beyond critical size. Med. Sci. Monit. 2008, 14, BR67–BR73. [Google Scholar] [PubMed]
- Schmitz, J.P.; Hollinger, J.O. The critical size defect as an experimental model for craniomandibulofacial nonunions. Clin. Orthop. Relat. Res. 1986, 205, 299–308. [Google Scholar] [CrossRef]
- Oryan, A.; Sahvieh, S. Effectiveness of chitosan scaffold in skin, bone and cartilage healing. Int. J. Biol. Macromol. 2017, 104, 1003–1011. [Google Scholar] [CrossRef]
- Cheng, G.; Li, Z.; Wan, Q.; Lv, K.; Li, D.; Xing, X.; Li, Z. A novel animal model treated with tooth extraction to repair the full-thickness defects in the mandible of rabbits. J. Surg. Res. 2015, 194, 706–716. [Google Scholar] [CrossRef]
- Sivashankari, P.; Prabaharan, M. Prospects of chitosan-based scaffolds for growth factor release in tissue engineering. Int. J. Biol. Macromol. 2016, 93, 1382–1389. [Google Scholar] [CrossRef]
- Nair, P.N.R. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef]
- Amine, K.; Gharibi, A.; Hsaine, A.; Kissa, J. Effect of bone regeneration with mineralized plasmatic matrix for implant placement in aesthetic zone. Case Rep. Dent. 2017, 2017, 2639564. [Google Scholar] [CrossRef]
- Moheb, M.E.; Al-Zarea, B.; Sghaireen, M.G.; Toriya, J.; Mizohata, A.; Patil, S.; Siada, A.; Brad, B.; Kochaji, N.; Alam, M.K. Mineralized plasmatic matrix to enhance the bone grafting technique. J. Hard Tissue Biol. 2017, 26, 289–292. [Google Scholar] [CrossRef]
- Lawrence, T. The nuclear factor NF-κB pathway in inflammation. Cold Spring Harb. Perspect. Biol. 2009, 1, a001651. [Google Scholar] [CrossRef]
- Wang, Y.; Ni, H.; Li, H.; Deng, H.; Xu, L.S.; Xu, S.; Zhen, Y.; Shen, H.; Pan, H.; Yao, M. Nuclear factor kappa B regulated monocyte chemoattractant protein-1/chemokine CC motif receptor-2 expressing in spinal cord contributes to the maintenance of cancer-induced bone pain in rats. Mol. Pain 2018, 14, 1744806918788681. [Google Scholar] [CrossRef] [PubMed]
- Takayanagi, H. Inflammatory bone destruction and osteoimmunology. J. Periodontal Res. 2005, 40, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Elsharkawy, A.M.; Mann, D.A. Nuclear factor-κB and the hepatic inflammation-fibrosis-cancer axis. Hepatology 2007, 46, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-K.; Lorenzo, J. Cytokines regulating osteoclast formation and function. Curr. Opin. Rheumatol. 2006, 18, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Khosla, S. Minireview: The opg/rankl/rank system. Endocrinology 2001, 142, 5050–5055. [Google Scholar] [CrossRef]
- Hong, S.; Hsu, H.-J.; Kaunas, R.; Kameoka, J. Collagen microsphere production on a chip. Lab Chip 2012, 12, 3277–3280. [Google Scholar] [CrossRef]
- Arai, Y.; Choi, B.; Kim, B.J.; Park, S.; Park, H.; Moon, J.J.; Lee, S.-H. Cryptic ligand on collagen matrix unveiled by MMP13 accelerates bone tissue regeneration via MMP13/Integrin α3/RUNX2 feedback loop. Acta Biomater. 2021, 125, 219–230. [Google Scholar] [CrossRef]
- Intini, G. The use of platelet-rich plasma in bone reconstruction therapy. Biomaterials 2009, 30, 4956–4966. [Google Scholar] [CrossRef]
- Rahman, S.; Sutedja, E.; Ayu, O.; Amirsyah, M. The Effect of Platelet-Rich Plasma on Type I Collagen Production, VEGF Expression, and Neovascularization after Femoral Bone Implants: A Study on Rat Models. Orthop. Res. Rev. 2022, 14, 207. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Kim, S.-G.; Oh, J.-S.; Jin, S.-C.; Son, J.-S.; Kim, S.-Y.; Lim, S.-Y. Analysis of the inorganic component of autogenous tooth bone graft material. J. Nanosci. Nanotechnol. 2011, 11, 7442–7445. [Google Scholar] [CrossRef]
- Gomes, M.F.; Da Silva Dos Anjos, M.J.; de Oliveira Nogueira, T.; Guimarães, S.A.C. Histologic evaluation of the osteoinductive property of autogenous demineralized dentin matrix on surgical bone defects in rabbit skulls using human amniotic membrane for guided bone regeneration. Int. J. Oral Maxillofac. Implant. 2001, 16, 563–571. [Google Scholar]
- Rocha, C.A.; Cestari, T.M.; Vidotti, H.A.; de Assis, G.F.; Garlet, G.P.; Taga, R. Sintered anorganic bone graft increases autocrine expression of VEGF, MMP-2 and MMP-9 during repair of critical-size bone defects. J. Mol. Histol. 2014, 45, 447–461. [Google Scholar] [CrossRef] [PubMed]
- Schipani, E.; Maes, C.; Carmeliet, G.; Semenza, G.L. Regulation of osteogenesis-angiogenesis coupling by HIFs and VEGF. J. Bone Miner. Res. 2009, 24, 1347–1353. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.T. Interdependent roles for hypoxia inducible factor and nuclear factor-κB in hypoxic inflammation. J. Physiol. 2008, 586, 4055–4059. [Google Scholar] [CrossRef]
- Page-McCaw, A.; Ewald, A.J.; Werb, Z. Matrix metalloproteinases and the regulation of tissue remodelling. Nat. Rev. Mol. Cell Biol. 2007, 8, 221–233. [Google Scholar] [CrossRef] [PubMed]
- Ortega, N.; Behonick, D.; Stickens, D.; Werb, Z. How proteases regulate bone morphogenesis. Ann. N. Y. Acad. Sci. 2003, 995, 109–116. [Google Scholar] [CrossRef]
- Davis, G.E.; Senger, D.R. Endothelial extracellular matrix: Biosynthesis, remodeling, and functions during vascular morphogenesis and neovessel stabilization. Circ. Res. 2005, 97, 1093–1107. [Google Scholar] [CrossRef]
- Ortega, N.; Behonick, D.J.; Werb, Z. Matrix remodeling during endochondral ossification. Trends Cell Biol. 2004, 14, 86–93. [Google Scholar] [CrossRef]
- Karsdal, M.A.; Larsen, L.; Engsig, M.T.; Lou, H.; Ferreras, M.; Lochter, A.; Delaissé, J.-M.; Foged, N.T. Matrix metalloproteinase-dependent activation of latent transforming growth factor-β controls the conversion of osteoblasts into osteocytes by blocking osteoblast apoptosis. J. Biol. Chem. 2002, 277, 44061–44067. [Google Scholar] [CrossRef]
- Zwingenberger, B.; Vater, C.; Bell, R.L.; Bolte, J.; Mehnert, E.; Brünler, R.; Aibibu, D.; Zwingenberger, S. Treatment of Critical-Size Femoral Bone Defects with Chitosan Scaffolds Produced by a Novel Process from Textile Engineering. Biomedicines 2021, 9, 1015. [Google Scholar] [CrossRef]
- Rodríguez-Merchán, E.C. Bone healing materials in the treatment of recalcitrant nonunions and bone defects. Int. J. Mol. Sci. 2022, 23, 3352. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Usas, A.; Olshanski, A.; Ho, A.M.; Gearhart, B.; Cooper, G.M.; Huard, J. VEGF improves, whereas sFlt1 inhibits, BMP2-induced bone formation and bone healing through modulation of angiogenesis. J. Bone Miner. Res. 2005, 20, 2017–2027. [Google Scholar] [CrossRef] [PubMed]
- Wernike, E.; Montjovent, M.-O.; Liu, Y.; Wismeijer, D.; Hunziker, E.B.; Siebenrock, K.-A.; Hofstetter, W.; Klenke, F.M. VEGF incorporated into calcium phosphate ceramics promotes vascularisation and bone formation in vivo. Eur. Cell Mater. 2010, 19, 30–40. [Google Scholar] [PubMed]













Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendawy, A.; Atiba, A.; Abdo, W.; Osman, A.; Sadakah, A.; Abou ElReash, A.; Elsayad, G.; Xie, X. The Effect of Mineralized Plasmatic Matrix and Chitosan on the Healing of Critical-Sized Mandibular Bone Defects in a Rabbit Model. Processes 2022, 10, 1890. https://doi.org/10.3390/pr10091890
Hendawy A, Atiba A, Abdo W, Osman A, Sadakah A, Abou ElReash A, Elsayad G, Xie X. The Effect of Mineralized Plasmatic Matrix and Chitosan on the Healing of Critical-Sized Mandibular Bone Defects in a Rabbit Model. Processes. 2022; 10(9):1890. https://doi.org/10.3390/pr10091890
Chicago/Turabian StyleHendawy, Ahmed, Ayman Atiba, Walied Abdo, Amira Osman, Abdelfattah Sadakah, Ashraf Abou ElReash, Gamal Elsayad, and Xiaoli Xie. 2022. "The Effect of Mineralized Plasmatic Matrix and Chitosan on the Healing of Critical-Sized Mandibular Bone Defects in a Rabbit Model" Processes 10, no. 9: 1890. https://doi.org/10.3390/pr10091890