
Interactive Teaching Aid Kit for Cardiopulmonary Resuscitation


Department of Computer Science and Information Engineering, National Quemoy University, Kinmen 89250, Taiwan
Processes 2022, 10(8), 1515; https://doi.org/10.3390/pr10081515
Submission received: 28 June 2022
/
Revised: 28 July 2022
/
Accepted: 29 July 2022
/
Published: 1 August 2022
(This article belongs to the Special Issue Empowering the Smart Consumer Electronics: Opportunities by the Convergence of Sensors, AIoT, Cloud Services, Blockchain, and AR/VR)
Abstract
:Cardiopulmonary resuscitation (CPR) is an emergency procedure performed on a person experiencing cardiac arrest to manually preserve brain function until spontaneous breathing and blood circulation can be restored. If performed timely and properly, it can improve the survival rate of a person experiencing cardiac arrest. The promotion of CPR has always been an important task for countries around the world. Countries around the world often hold relevant study camps and seminars to improve the public’s awareness of CPR. On the basis of this rationale, this paper proposes an interactive teaching aid kit for CPR that uses a CPR manikin and tutoring software to facilitate CPR learning among trainees. The CPR manikin is equipped with sensors that determine whether the CPR steps are performed correctly. Data from the sensors are sent to the tutoring software through wireless transmission. The software provides video demonstrations and textual instructions concerning the standard CPR procedure. In this software, the interactive interface displays real-time information about the trainee’s CPR process, such as information on the CPR step being performed and the number of chest compression and breaths given. Thus, this teaching aid kit allows trainees to learn CPR without an instructor. This system may enable CPR to become a readily learnable skill for the general population.
1. Introduction
Cardiopulmonary resuscitation (CPR) is an emergency procedure performed on a person experiencing cardiac arrest to manually preserve brain function until spontaneous breathing and blood circulation can be restored. CPR is not a single technique; it encompasses a series of assessments and interventions [1]. Cardiopulmonary resuscitation (CPR) has been widely practiced since the clinical utilization of closed chest massage was first reported in 1960 [2]. Patients receiving CPR within 4 min of a cardiac arrest and advanced cardiac life support (ACLS) within 8 min of the life-threatening condition exhibit a survival rate as high as 43% [3]. According to data from the American Heart Association (AHA), more than 135 million deaths due to cardiovascular diseases are registered in the world each year [3]. Therefore, promoting CPR and developing a robust emergency care strategy can reduce mortality rates caused by this condition.
In 2020, the International Consensus on CPR and Emergency Cardiovascular Care Science with Treatment and Recommendations, which is developed by the International Liaison Committee on Resuscitation (ILCOR), published updated recommendations and guidelines for CPR [4]. In the ILCOR resuscitation guidelines, the supports of the important relationship between quality of CPR and resuscitation outcomes have been highlighted [4,5], and two key recommendations are the use of real-time audiovisual feedback as a means to maintain CPR quality and the importance of early initiation of CPR by bystanders [6]. Therefore, in order to raise awareness of the importance of CPR in early childhood education [7], mandatory training of schoolchildren would be an important measure [8,9]. On the other hand, the introduction of CPR training in schools has been also advocated by the World Health Organization [8]. To equip students with the skills and knowledge necessary to prevent deaths from cardiac arrest, the Ministry of Education (MoE) of Taiwan required educational institutions at the secondary level or above to launch CPR training programs for would-be CPR instructors, and that all students should receive a total of 4 h of CPR education in each academic year. This will enable them to learn, apply, and master CPR and thus receive CPR certification. As of now, 85% of students at the secondary level or above should receive CPR education, and that 90% of school nurses and nursing teachers should receive CPR training and repeat it once at least every 2 years.
CPR education can be disseminated through different methods. As early as elementary school, students learn about CPR through videos, and through this teaching method, students gain an adequate understanding of the emergency procedure [6]. To enable the general public to apply CPR in a cardiac emergency, the digital learning methods for CPR are also becoming more and more diverse [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27]. Some of the works are the technological solutions when teaching and practicing CPR technique [10,11,12,13,14,15], and some of the works are the medical applications of virtual reality topic [16,17,18,19,20]. Some studies have proposed approaches that enable students to learn CPR without an instructor, such as the applications of the interactive game, serious game, VR, and AR [10,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31]. As performing CPR requires a focus on precision, it is essential to assess the precision of CPR maneuvers initiated through measurement devices such as a Kinect-based system and Leap Motion [10,25,26,27]. This system uses a camera to determine whether CPR maneuvers are correctly performed; however, it needs to be more interactive. To address this limitation, a Kinect-based system with sensors and augmented reality functionality has been developed [27]; this system reduces the need for the trainee to adopt instinctive learning or to seek instruction from others. Due to the recent COVID-19 pandemic, VR is one of the alternative training options that has gained attention regarding CPR training [28]. Kuyt et al. emphasize the widespread use of VR in medical education and CPR because VR has shown to enhance performance and increase engagement [29]. Jeffers et al. developed and tested an augmented reality head mounted display chest compression (CC) feedback system (AR-CPR) designed to provide real-time CC feedback and guidance [30]. Stumpf et al. aim to develop and validate an application for smartphones which can provide real-time audiovisual and haptic feedback on determinants of CPR quality [31].
Automated real-time feedback devices have been considered a potential tool to improve the quality of CPR. Although many researches have supported the usefulness of such devices during training, do automated real-time feedback devices improve CPR quality [32]? In that paper, the authors aim to assess the effectiveness of artificial real-time feedback devices for improving CPR performance during training, simulation and real-life resuscitation attempts in the adult and pediatric population [30,33,34,35,36,37,38]. In the conclusion of that paper, the use of automated real-time feedback devices enhances skill acquisition and CPR performance during training of healthcare professionals is proposed. Thus, we can know the automated real-time feedback devices could improve CPR quality. Although the cost of the automated real-time feedback device is higher compared with the CPR learning software on the market, such as interactive games, serious games, VR, and AR, the hardware operation can have more practical interactive learning effects. Through the automated real-time feedback device, the user can instantly know whether the operation is correct or not, and then adjust the action of CPR operation. For this reason, everyone can use the automated real-time feedback device learn the CPR operations of self-learning.
On the basis of previous studies, this paper presents an interactive teaching aid kit for CPR that uses a CPR manikin and tutoring software to facilitate CPR learning among trainees. The manikin is equipped with sensors that measure data on CPR maneuvers and sends the measurement data to the tutoring software through wireless transmission. Subsequently, the interactive user interface (UI) of the tutoring software displays real-time information to the trainee about how CPR steps are initiated and whether CPR maneuvers are performed accurately. Such interactive learning reduces the time required to familiarize oneself with the CPR manikin and allows the trainee to self-learn CPR by accessing video demonstrations, textual instructions, and tips through the interactive UI. The software enables not only instruction modes but also Practice and Assessment modes. In the Practice mode, the trainee can practice the CPR steps they are unfamiliar with. In the Assessment mode, the trainee is evaluated according to the criteria developed by Chinese Emergency Medicine Educator Association. Once a CPR test is completed, the test result appears in the numerical format and indicates whether the trainee has passed the test. The trainee can access previous test results to check the score obtained and the number of errors made in each test. These records provide the trainee with an understanding of the CPR steps they must improve on. The trainee can practice these steps in the Practice mode.
2. Framework of the Interactive Teaching Aid Kit for CPR
The proposed interactive CPR teaching aid kit comprises a CPR manikin (consisting of a manikin module, sensor module, and central processing unit (CPU) and interactive CPR tutoring software (composed of a wireless transmission module and interactive UI module). Figure 1 is the framework of the teaching aid kit.
2.1. Teaching Aid Kit for CPR Manikin
The teaching aid kit for CPR manikin is divided into three units, namely the CPR manikin module, the sensor module and the CPU module. The CPR manikin module, which is Resusci Anne, allows to perform CPR steps. The sensor module detects whether CPR steps are accurately performed. The CPU module measurement data received from the sensor module delivers the computation results to the interactive CPR tutoring software through wireless transmission.
In the CPR steps, we use “check, called, CABD”. It is based on the ILCOR resuscitation guidelines in 2020. The steps are as follow: assess the responsiveness of the patient, call for help, and perform the circulation, airway, breathing, and defibrillation (CABD) sequence. Specifically, before starting CPR, check the patient’s responsiveness. If the patient is unresponsive, call for help by dialing 911 immediately to reach a local paramedic unit, and ask anyone nearby to look for an automated external defibrillator (AED). Before an AED is retrieved and an ambulance arrives, perform CPR on the patient in CABD sequence. “C” is for circulation: assess the presence or absence of oxygen circulation; if the patient is not breathing, perform chest compressions on the heart. “A” is for airway: place one hand on the forehead and the other hand under the tip of the chin to tilt the patient’s head backward, thereby opening the airway. With the head in the tilt position, clear any obstructions of the mouth. “B” is for breathing: perform artificial respiration through 30 repeated chest compressions followed by two breaths at a rate of one breath every second. “D” is for defibrillation: once an AED is available on scene, follow the instructions for the AED to restore a normal heart rhythm. Once all cycles are completed, check whether the patient has started to breath or regain consciousness. If the patient has not regained to breath, continue chest compressions until an AED is retrieved. The following is the process description of CPR.
- Check: Assess the patient’s responsiveness;
- Call 911: If unresponsive, call for help;
- Compressions: Give 30 gentle chest compressions at the rate of 100–120/min. Use two or three fingers in the center of the chest just below the nipples. Press down approximately one-third the depth of the chest (about 1 and a half inches);
- Airway: Open the airway using a head tilt lifting of chin. Do not tilt the head too far back;
- Breathing: Rescue breathing starts after the 30 compressions, when the airway is open. Someone doing rescue breathing breathes for the victim by forcing air into the lungs; and
- Defibrillation: When the second rescuer returns, have them follow the AED prompts, apply AED pads and help with CPR.
2.1.1. CPR Manikin Module
The CPR manikin module of Resusci Anne (Figure 2), which was named after a 12-year-old daughter who drowned in a beach and was developed by her father (a physician and toy factory owner) to promote CPR. Resusci Anne has an automatically closing airway, a movable neck, a realistic chest compression feeling, a chest that contracts naturally when artificial respiration is performed, and a body in proportion to the actual human body. Resusci Anne is designed in such manner that enables the trainee to learn how to apply chest compression with proper strength and to acquire crucial CPR skills. The manikin comprises an airway (to oral and nasal passages) and a thoracic cavity. When the trainee tilts the head of the manikin backwards and breathes correctly into its mouth, the air inflates its thoracic cavity. In this way, when the trainee applies chest compressions on the correct position, the air is released from the cavity—an indication of a proper CPR procedure.
2.1.2. Sensor Module
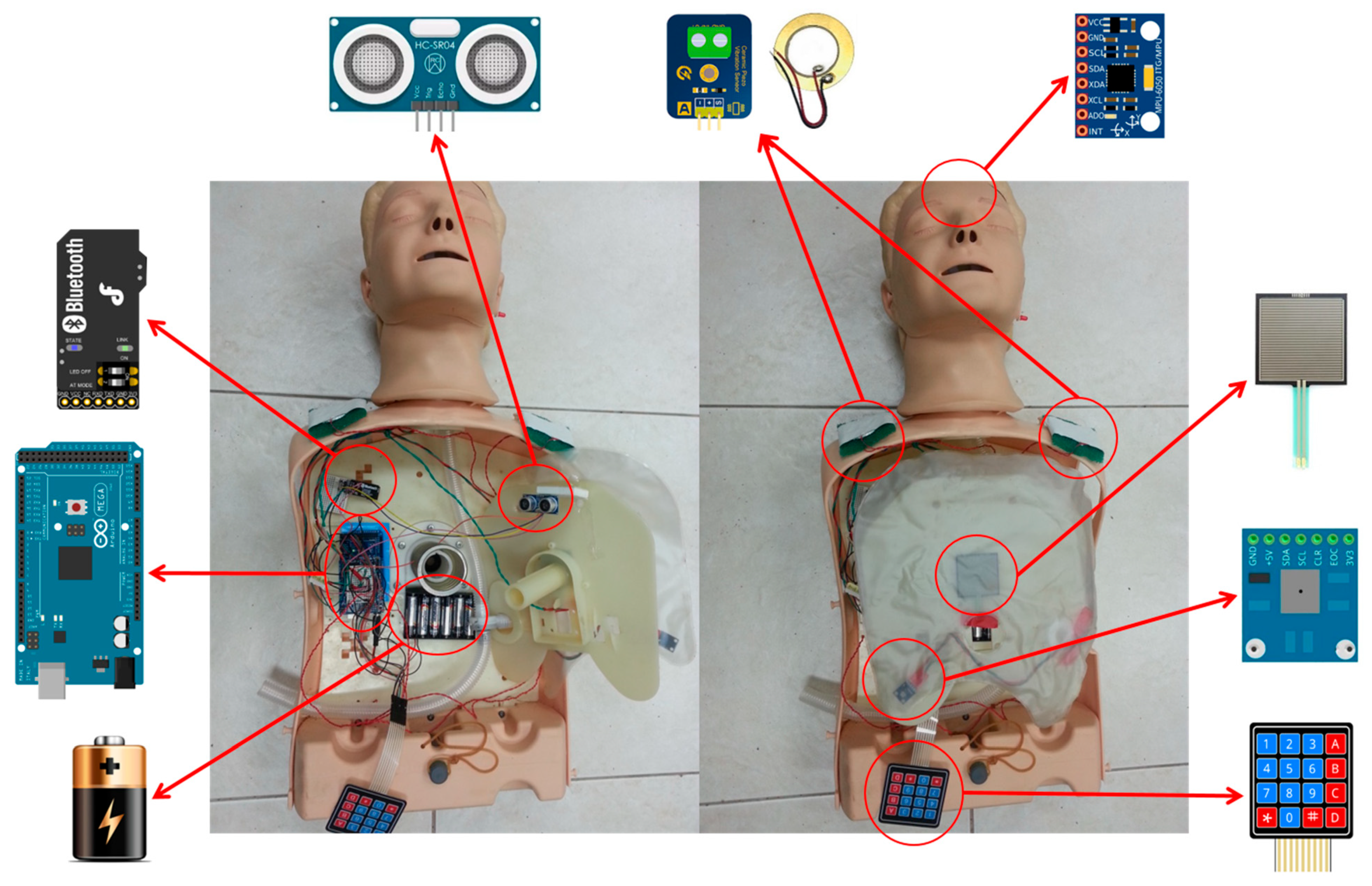
The sensor module consists of an analog piezoelectric ceramic shock sensor, thin-film keyboard, ultrasonic sensor, pressure sensor, gyro sensor, atmosphere sensor, magnetic sensors, and light-emitting-diode (LED) indicator bars. These sensors collect data on the CPR maneuvers performed on the manikin by the trainee. These data are subsequently delivered to the interactive tutoring software and used to determine whether the maneuvers are properly performed.
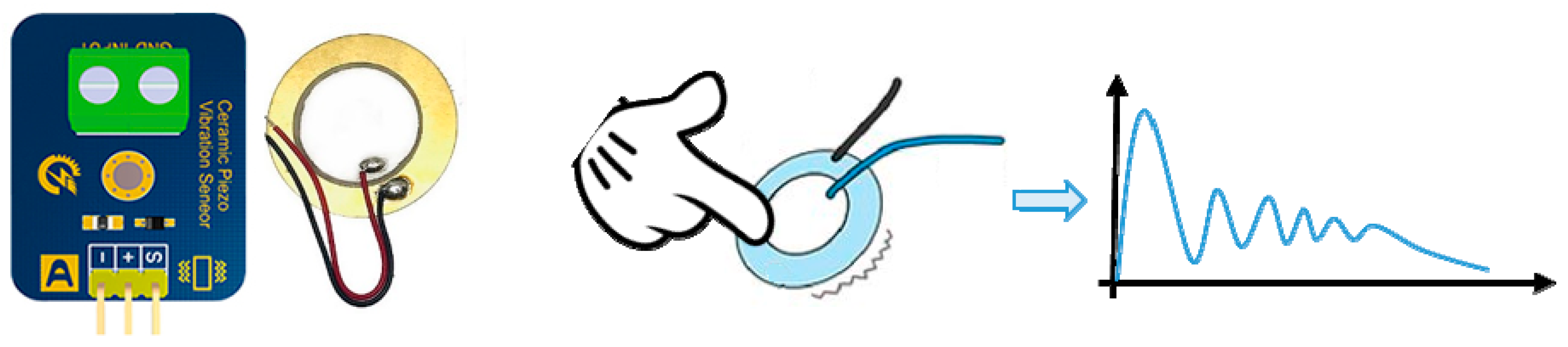
- Analog piezoelectric ceramic shock sensor
The analog piezoelectric ceramic shock sensor (Figure 3) is attached to both shoulders of the manikin module. It detects whether the trainee has patted the shoulders of the manikin to assess the patient’s responsiveness in a simulated cardiac arrest environment. The circuit of the sensor remains open and—when the manikin is patted on the shoulder, with the force of the patting delivered to the center of the sensor—switches to the closed state, sending positive values (or zero values, if otherwise) to the CPU.
- 2.
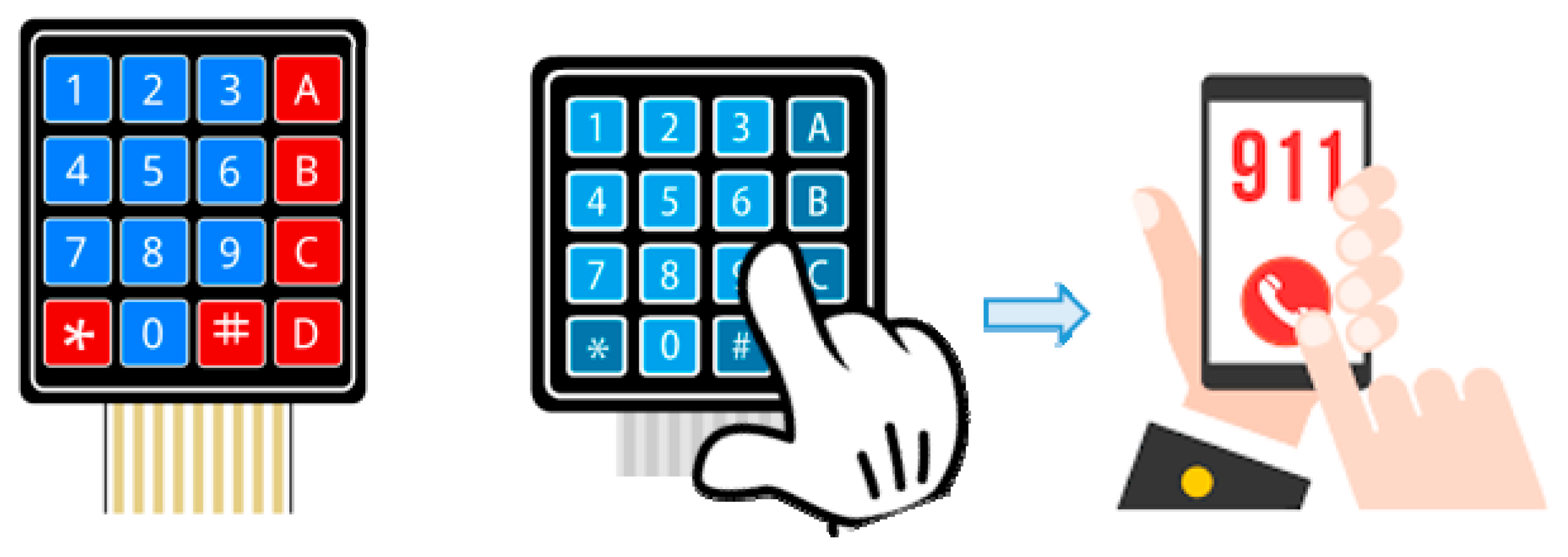
- Thin-film keyboard
Attached to a side of the abdomen of the manikin, where the trainee performs CPR, the thin-film keyboard (Figure 4) allows the trainee to call an ambulance in a cardiac arrest scenario. The trainee needs to press 911 and the pound key (#) on the keyboard to send out a request for immediate medical attention. The keyboard has an 8-PIN connector.
- 3.
- Ultrasonic sensor
Attached in the center of the chest below the nipple line, the ultrasonic sensor (Figure 5) estimates the depth of chest compression and determines whether the trainee performs the compression at a standard depth of up to 5 cm.
- 4.
- Pressure sensor
Attached in the center of the chest above the nipple line the pressure sensor (Figure 6) determines whether the trainee’s hands are placed correctly for CPR.
- 5.
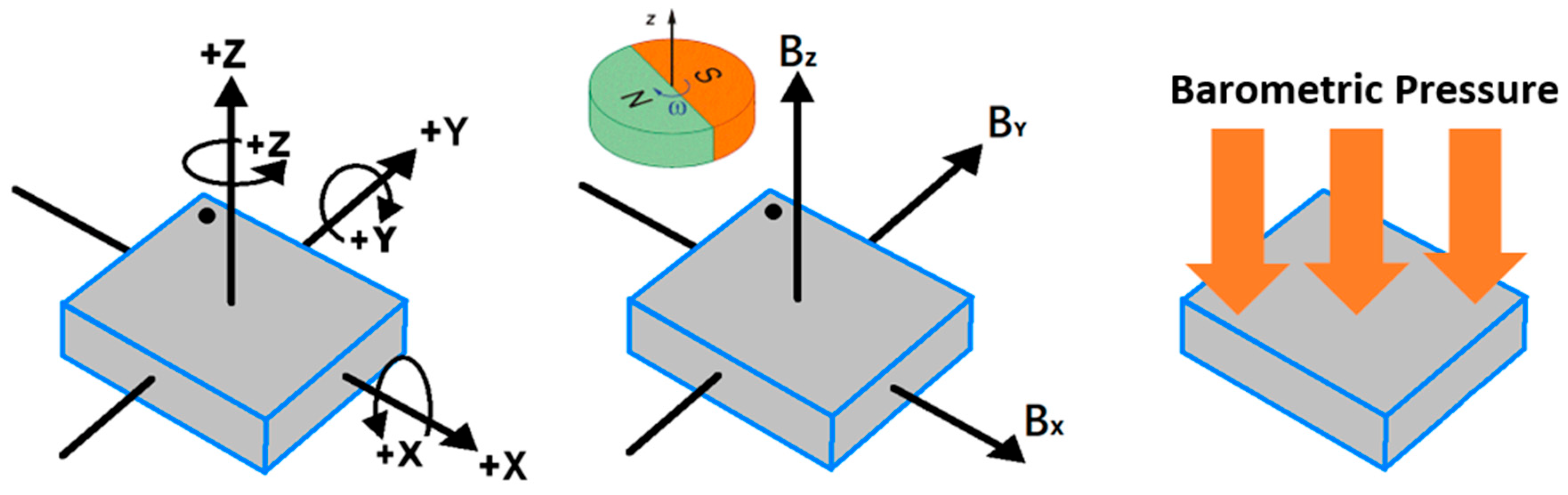
- Gyro sensor
Installed in the head of the manikin, the gyro sensor (Figure 7) determines whether the trainee, while performing the “A” (airway) step in the CABD sequence of CPR, presses the forehead and lifts the chin in a manner that straightens the airway to send air into the lungs.
- 6.
- Hall magnetic sensors
The hall magnetic sensors (Figure 7) are attached to the right side of the chest and the left side of the abdomen, where AED pads are typically placed. The sensors are activated during the “D” (defibrillation) step in the CABD sequence of CPR.
- 7.
- Barometric pressure sensor
Installed in the air bag of the manikin, the barometric pressure sensor (Figure 7) determines whether the breath is successfully provided into the manikin (to expand the thoracic cavity) during the “B” (breathing) step in the CABD sequence of CPR.
- 8.
- LED indicator bars
LED indicator bars are attached below each of the aforementioned sensors. They are activated when a CPR step detected by a given sensor is performed. The bars help to identify the CPR steps being performed and facilitate CPR training.
2.1.3. CPU Module
The Arduino Mega (Figure 8) is used as the CPU to collect measurement data from all sensors, compute the data into useful information, and standardize the information into a series of Bluetooth sequences to ensure that no data packets are lost. The CPU sends the information through Bluetooth to the interactive CPR tutoring software, which subsequently displays real-time feedback information in the form of graphs. These graphs indicate the number of CPR movements repeated by the trainee and whether the trainee’s hand position for CPR is correct.
2.2. Interactive CPR Tutoring Software
The interactive CPR tutoring software is used to present the real-time user operation information and give appropriate teaching and prompting, as shown in Figure 9. The interactive CPR tutoring software comprises the following modules: (1) wireless transmission and (2) interactive interface. The wireless transmission module delivers all CPU-processed data to the interactive interface module. The interactive interface module displays real-time information about the CPR process to the trainee—such as the current CPR steps performed, the number of chest compressions or breaths given, and whether AED pads are placed correctly—as well as provides CPR instructions.
2.2.1. Wireless Transmission Module
The wireless transmission module functions as the interface between the CPR manikin and the interactive CPR tutoring software. It uses a Bluetooth module to send the CPU-processed data to the interactive interface module.
2.2.2. Interactive Interface Module
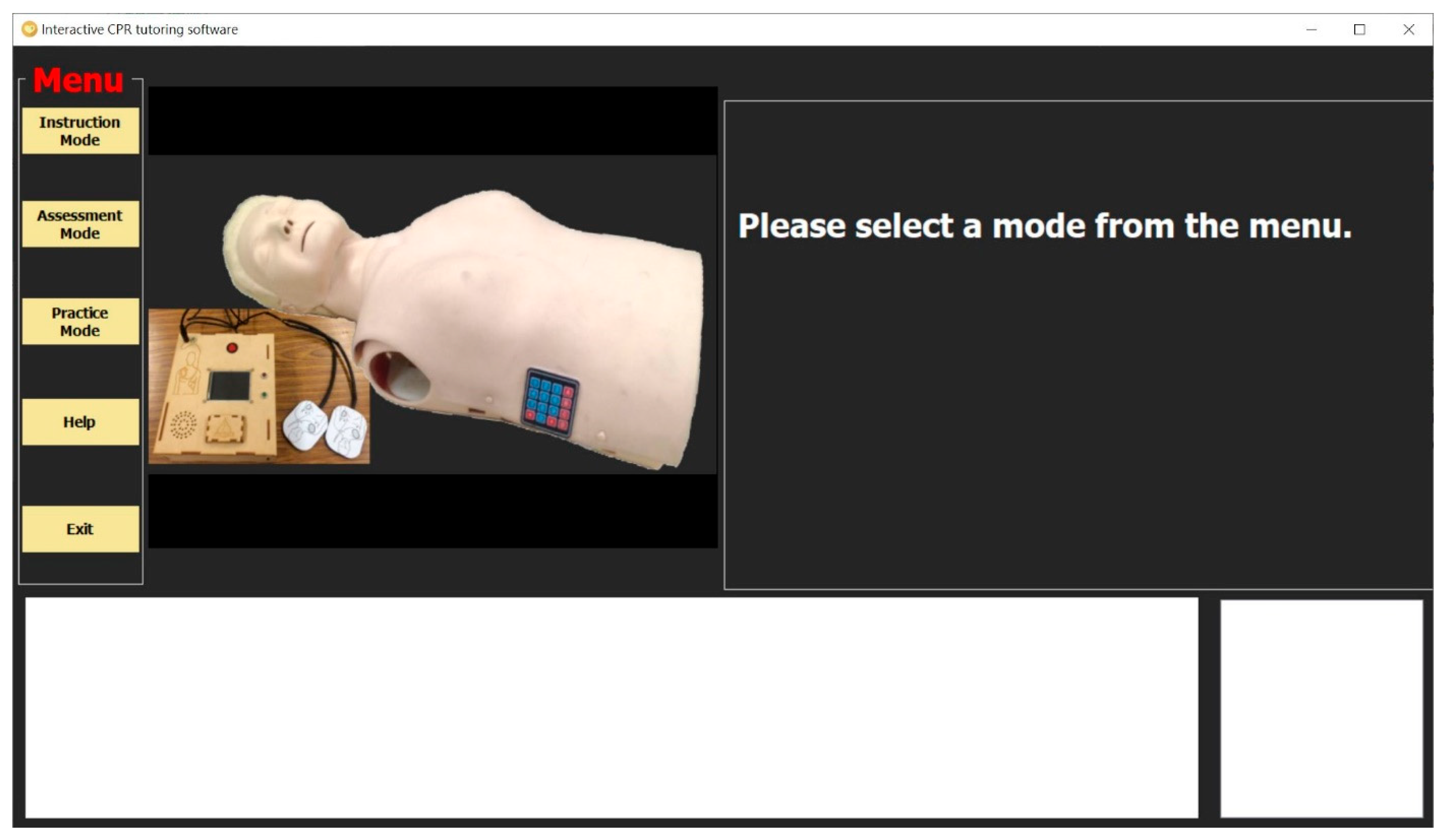
The interactive interface module is the user interface of CPR manikin, and called the interactive CPR tutoring software (Figure 10). This module displays the interactive information with the device on a computer screen. The interface initially shows a home page with the menu on the left-hand side (Figure 11). The menu includes the following items: (1) the modes of “Instruction,” “Assessment,” and “Practice”; (2) “Help” (providing instructions on how to operate the software); and (3) “Exit.” The interface comprises the sections of “Menu,” “Video Instruction,” “Textual Instruction,” “Real-Time Graph,” and “Bluetooth Sequence Display.”
The Menu section is located on the left-hand side of the interface, and the trainee has to select the Instruction, Assessment, or Practice mode. “Start,” “Stop,” and “Exit” functions are built into each mode. The video instruction section is located on the center-left of the interface; it replays a demo clip about the CPR step being performed and hides the clip only in the Assessment mode. The candidate can access the test result by entering his or her name in the Assessment mode. The textual instruction section, which is located on the upper-right of the interface, displays information on the CPR step being performed. The information includes the number of chest compressions and breaths given by the trainee. The Real-Time Graph section is located on the lower center-left of the interface; it receives the CPU-processed data through the Bluetooth module and displays them as the trainee performs CPR on the manikin. The Bluetooth Sequence Display section, located on the right corner of the interface, monitors whether any Bluetooth packets related to the CPR steps are lost. If a Bluetooth packet related to a CPR step is lost, the section ignores the data. Figure 12 presents all CPR steps and their corresponding sensors contained in the proposed interactive teaching aid kit for CPR.
- The instruction mode
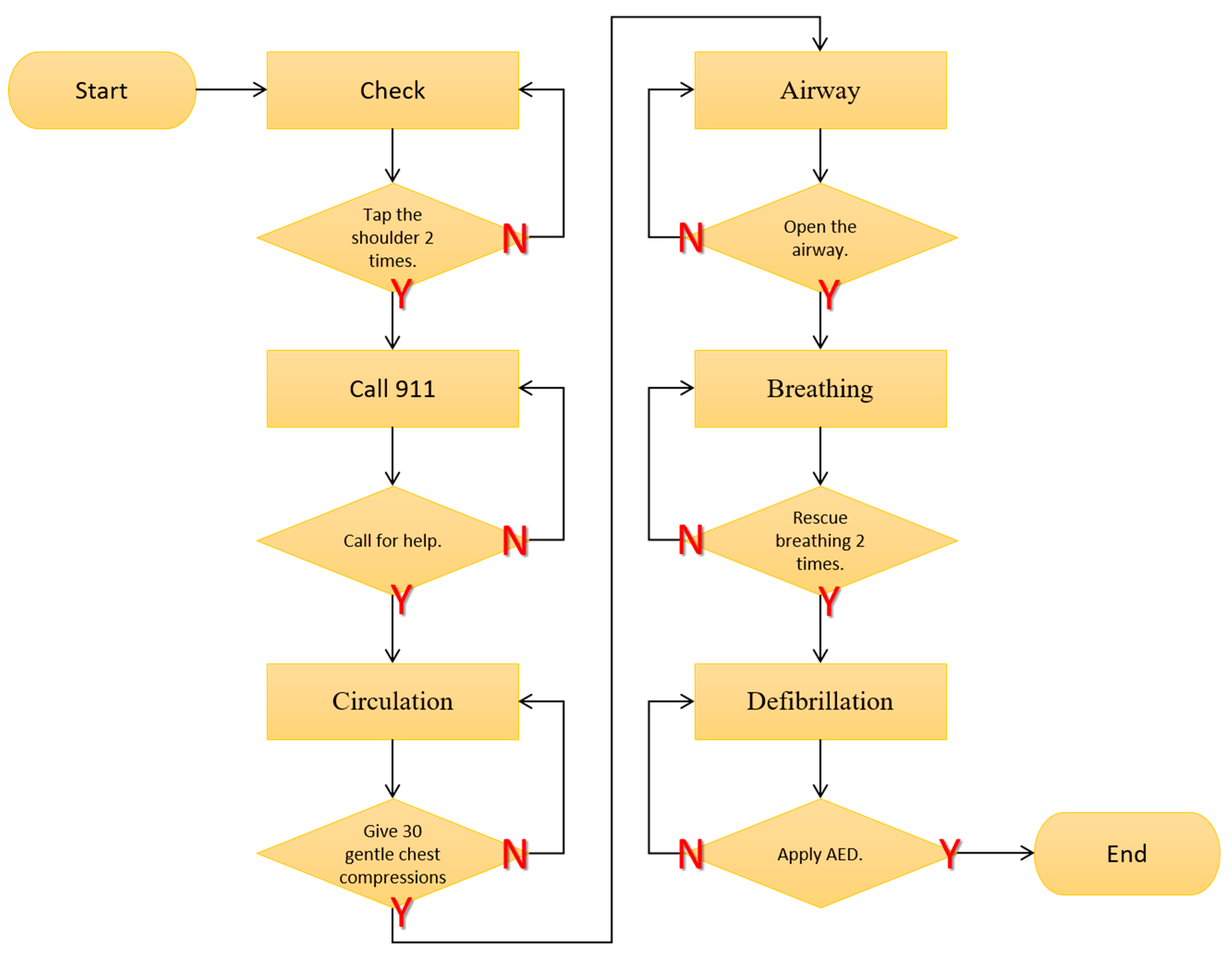
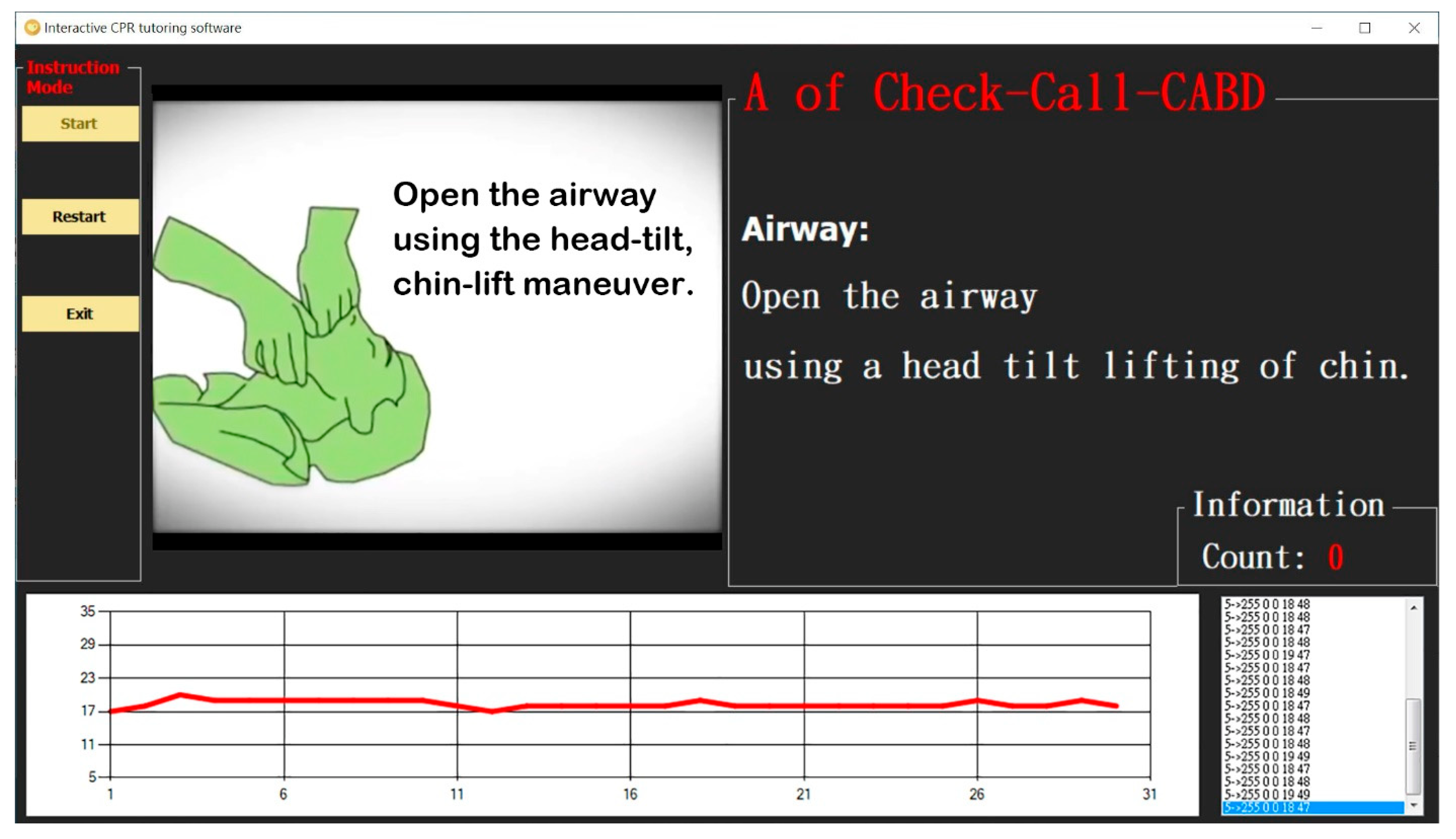
The instruction mode (Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8, Figure 9, Figure 10, Figure 11, Figure 12, Figure 13, Figure 14 and Figure 15) offers a comprehensive course on CPR and introduces all the six steps in the emergency procedure. The steps are: (1) check (assess the patient’s responsiveness), (2) call 911 (call for help), (3) circulation, (4) airway, (5) breathing, and (6) defibrillation (the last four steps are named by the acronym “CABD”). In the first step, the trainee pats the shoulders of the manikin to determine the patient’s responsiveness in a simulated cardiac arrest environment. In the next step, the trainee presses on the pound key of a keyboard to dial 911 to call for an ambulance. Once the second step is performed correctly, the trainee performs 30 compressions—each at a depth of up to 5 cm—on the center of the chest between the nipples. Thereafter, the trainee tilts the head of the manikin backward for 5 s to allow the airway to remain open. The trainee subsequently breathes into the mouth of the manikin, giving two breaths at a time. In this step, the trainee must ensure that the chest inflates noticeably. Finally, the trainee attaches the two magnetic adhesive pads of a self-designed AED each to the right side of the chest and the left side of the abdomen of the manikin. Figure 13 shows the flowchart of the instruction mode. Figure 14 shows the user interface of the instruction mode.
Installed in different positions on the body of the manikin, LED indicator bars are activated when the trainee pats the shoulders to assess responsiveness, applies compression on the center of the chest between the nipples, and attaches the pads of the AED each to the right side of the chest and the left side of the abdomen.
- 2.
- The practice mode
The practice mode allows the trainee to practice any of the six CPR steps until he or she exits the mode or chooses a different step. The user interface of the practice mode difference from the instruction mode is that the upper left menu is changed to the CPR step options. Similar to the instruction mode, LED indicator bars are activated when the trainee pats the shoulders of the manikin, compresses the chest, and attaches AED pads to the right side of its chest and the left side of its abdomen. Figure 15 shows the flowchart of the instruction mode.
- 3.
- The assessment mode
The assessment mode displays the CPR step being initiated and a graph of the real-time results. The user interface of the assessment mode difference from the practice mode is that the video Instruction is turned off. It also presents the number of movements performed for a given CPR step and whether the step is performed correctly or incorrectly. By contrast, the instruction and practice modes only show the number of correctly performed steps. Once a CPR test is completed, the mode generates a score of the test and indicates whether the trainee has passed the test. The user’s score of the test is saved in the database of the software. Previous test scores, coupled with the number of errors made in each CPR step, can be accessed through the interface of the assessment mode. The score sheet of the assessment mode is shown as Table 1. Moreover, the test results can be retrieved for one or multiple test-takers. The results of a given test-taker can be searched by the name alone or by both the name and test date. The results of multiple test-takers can be searched by date or without any particular date, whereby results on all test dates are provided.
2.3. Interactive Teaching Aid Kit for CPR
The interactive teaching aid kit for CPR consists of not only a manikin equipped with a range of sensors but also a thin-film keyboard and a self-designed AED (Figure 16).
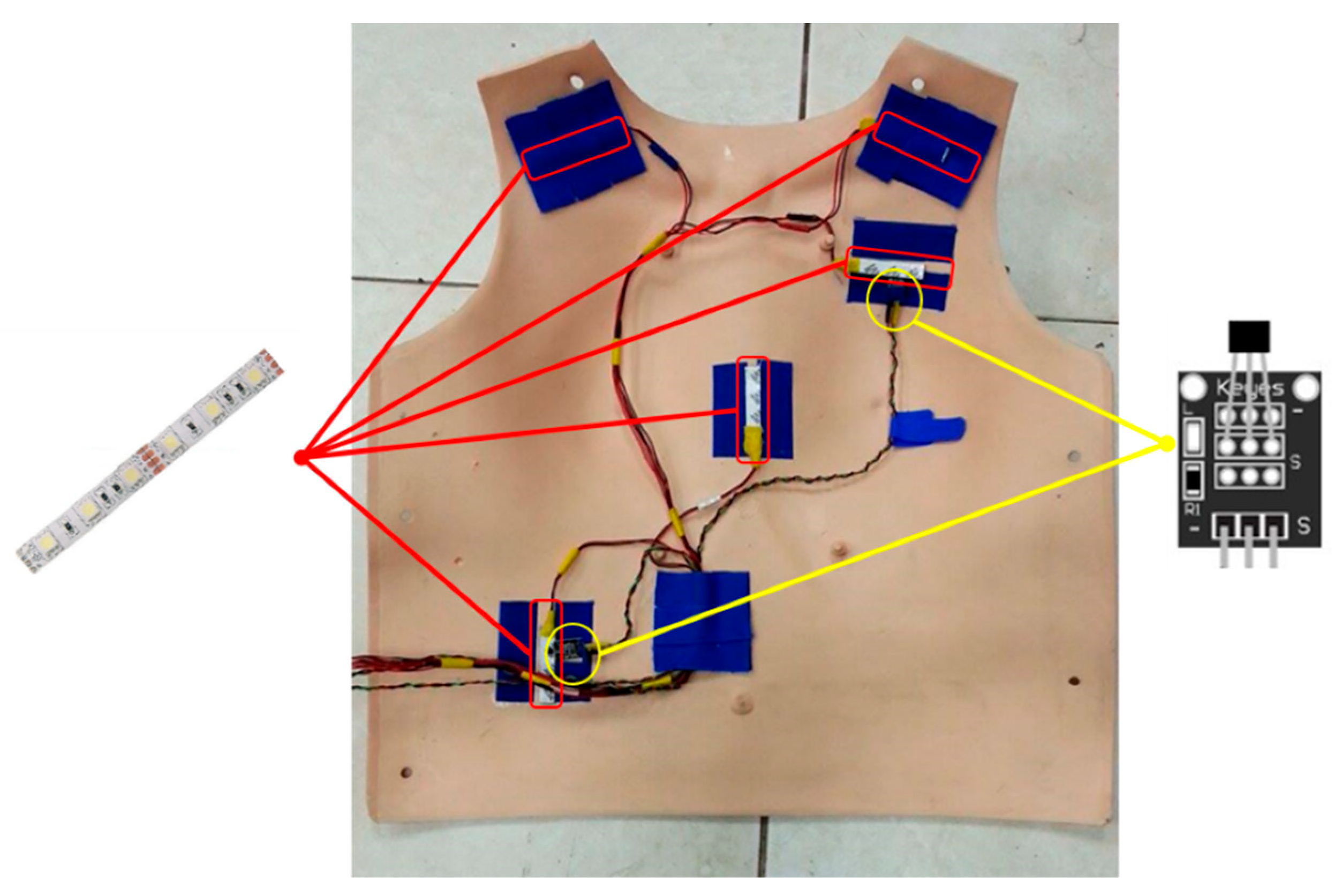
To increase their brightness, all the LED indicator bars are fastened with Velcro to the shoulders (corresponding to the step of assessing responsiveness before the CABD sequence of CPR is initiated), the center of the chest between the nipples (corresponding to the “C” step in the CABD sequence of CPR), and the right side of the chest and the left side of the abdomen (corresponding to the “D” step in the CABD sequence of CPR). The indicator bars for the defibrillation step can be attached using magnetic AED pads to the correct positions on the manikin, because the Real-time Graph section in the interactive tutoring software indicates the positions of the pads. Figure 17 depicts all LED indicator bars in action.
Figure 18 shows the sensors installed inside the CPR manikin. The magnetic sensors and LED indicator bars are attached beneath the skin of the manikin because of the limited detection ranges and LED brightness (Figure 19). A self-designed AED with two magnetic pads (Figure 20) that match the magnetic sensors inside the manikin is also included in the teaching aid kit. Attached with a powerful magnet, the pads can be easily matched to the sensors, which are installed on the standard positions for defibrillation.
3. Experimental Results
3.1. User Testing
The proposed interactive teaching aid kit for CPR allows an individual to learn CPR without an instructor. We invite the visitors to try this system in the public demonstration shown as Figure 21. Visitors who tested the kit completed a questionnaire indicating their satisfaction with the system and their perceived usability of it.
3.2. Questionnaire Design
A questionnaire was designed based on the System Usability Scale [39]. According to the results of the questionnaire (Table 2), participants provided responses that ranged between strongly agreeing and agreeing that the proposed teaching aid kit improves the motivation to learn CPR, and all respondents strongly favor the innovative design of the kit and were highly willing to use it again. The mean score of all responses is 43, as shown in Figure 22.
We assign scores from 1 to 5 between strongly disagree and strongly agree, and calculate the score of the average, standard deviation and standard error of each question, as shown in Table 3. From the average score of each question, it can be seen that the scores of question 4 and question 10 are significantly lower. In question 4, because the survey of the questionnaire is conducted in the public demonstration and most users operate through instructions, it is impossible to clearly answer whether technical assistance is required to use the system. This question is more suitable for answering in an environment that can be operated multiple times. However, we can see that the results of questions 7 and 8 differ from the results of question 4. Most users agree that the system is quick to learn and easy to use. In the question 10, most users think that it is better to have the basic knowledge of CPR before operating the system. Although this system also has a teaching mode, it requires user to have more time to operate to improve this problem.
In the analysis of user groups, since the users age and the users who have learned CPR before are more obvious for the analysis results, we conduct user group analysis and discussion for these two groups, as shown in Table 4 and Table 5. In Table 4, we combine the four ages in the questionnaire into two types, and use the age of college graduation as a distinction to analyze the differences in the satisfaction of young people with the use of the system. We can find that young people have a high degree of Information system acceptance, and they are also quick to learn the operation of equipment and software. In all questions, young people are more satisfied with the system than adults. On the other hand, due to the older age of some users also reflects the unfamiliarity and rejection of the information system, thus lowering the scores of adult groups. In Table 5, we can see that users who have learned CPR before have higher system satisfaction than those who never learned, except for question 1. The result of question 1 shows that the groups who have not learned CPR before think that this system can effectively help them to learn CPR. On the other hand, the results of questions 4, 5, 7, 8, and 9 were significantly different, which highlighted the difference in the system satisfaction of users who have learned CPR or not. It is also because they have learned CPR before, so they can better understand the contribution and substantial assistance of this system to users.
3.3. System Analysis
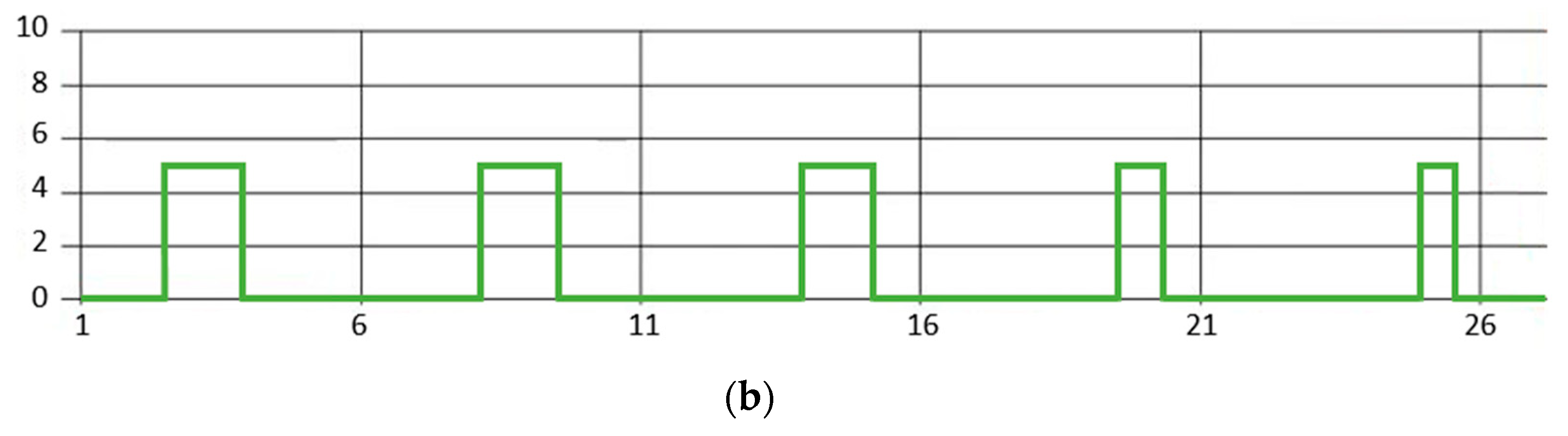
On the problem of CPR step determination, the analysis methods of sensor values are divided into three types, namely threshold trigger method, waveform analysis method, and thin-film keyboard input, as shown in Table 6. The waveform analysis method requires continuous waveform processing. Taking the circulation of the CPR steps as an example, since the data returned by the sensor are real-time continuous data, the data in this CPR step will be a continuous waveform, as shown in Figure 23a. According to the gentle chest compression requirement of the depth of at least 5 cm in this CPR step, we set the threshold to 5 cm and the processed result of the original data as shown in Figure 23b. Then we use the edge trigger method to calculate the number of gentle chest compressions. Through the calculation of the total time, we can get the overall frequency of the gentle chest compression in this CPR step. The frequency is required to be 100 to 120 times per minute shown in Figure 12. In this system, edge triggering can be either positive or negative edge triggering. Because compression and blowing will automatically return to the state, there will be no situation where the state cannot be restored (unless external force is continuously applied). On the other hand, we can also calculate scores for the details of the CPR operation, as shown in Table 1.
In this system, the sensors are independent and only their related sensors are read for each CPR step. Therefore, even if the value of other sensors changes, it will not affect the determination result. Regarding the durability of this system, the sensors used in this system are the generally standard and common sensors in the market, which can withstand a large number of and high-frequency use. Therefore, the durability of the system depends on the hardware and the same as the general CPR model in the market.
4. Conclusions
In this paper, we proposed an interactive teaching aid kit for CPR. This proposed teaching aid kit includes an Arduino as the CPU and many sensors to detect the user actions. The Arduino collects data from all the sensors and sends the data to interactive tutoring software through Bluetooth. The software provides video and textual instructions for beginners to help them comprehend each CPR step. The interactive interface of the software offers a graph that presents real-time data about the CPR step being performed. These feedback data allow the trainee to improve their CPR movements.
The teaching aid kit was exhibited at many fairs and received many considerable suggestions. The system helps improve public awareness of CPR and allows people to repetitively learn to check the responsiveness of a patient in cardiac arrest, call for help, and operate the CABD sequence of CPR. Therefore, users will be able to develop practical knowledge regarding CPR but not merely knowledge limited to textbooks or CPR promotion videos.
Some visitors at the fairs were invited to test the teaching aid kit. They recommended increasing the number of LED indicators and the AED and introducing the system for CPR certification and the evaluation of nurses’ clinical performance. Improvements to this system will be made on the basis of such recommendations to render it more user-friendly and enable the trainee to improve their CPR skills and knowledge. Moreover, the teaching aid kit can be implemented in educational institutions and governmental organizations and can be used to improve the validity and efficiency of CPR certification. In this way, CPR can become a readily learnable skill that people can apply to save a life.
It is not easy to integrate many sensors and develop a complete set of interactive CPR teaching aid kits. In this paper, we propose a low-cost and feasible method to design a product that is not inferior to the expensive CPR equipment on the market. The operation of this system is the same as the normal Resusci Anne, the difference is that this system can send real-time operation information back to the computer. Therefore, the user can instantly know whether the operation is correct or not, and then adjust the action of CPR operation. For this reason, when there is a shortage of professional CPR coaches, we can also use this system to learn CPR operations. One can learn CPR through our proposed interactive CPR tutoring software to achieve the purpose of self-learning CPR. On the other hand, compared with software simulation methods, such as interactive games, serious games, VR, and AR, although the cost of hardware equipment in this system is higher, the hardware operation can have more practical interactive learning effects. In terms of market assessment, as long as there are units with emergency rescue centers, such as schools, government agencies, companies, this system can be built to assist the internal staff of the unit to learn CPR. In terms of future work, this system can be applied to license examinations and ambulance crews training in the future after the system is mature. By assisting the judgment of professional CPR coaches through this system, the needs of more professionals can be saved, so that more people can participate in CPR-related examinations or training. Finally, we hope that through this work, we can effectively achieve the goal of universal popularization of CPR.
Author Contributions
Y.-X.Z.; methodology, Y.-X.Z.; software, Y.-X.Z.; validation, Y.-X.Z.; formal analysis, Y.-X.Z.; investigation, Y.-X.Z.; resources, Y.-X.Z.; data curation, Y.-X.Z.; writing—original draft preparation, Y.-X.Z.; writing—review and editing, Y.-X.Z.; visualization, Y.-X.Z.; supervision, Y.-X.Z.; project administration, Y.-X.Z.; funding acquisition, Y.-X.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Ministry of Science and Technology, Taiwan, under grants MOST 111-2221-E-507-006.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Jones, S.A. ACLS, CPR, and PALS: Clinical Pocket Guide; FA Davis: Philadelphia, PA, USA, 2014. [Google Scholar]
- Kouwenhoven, W.B.; Jude, J.R.; Knickerbocker, G.G. Closed-chest cardiac massage. JAMA 1960, 173, 1064–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aufderheide, T.P.; Kalra, R.; Kosmopoulos, M.; Bartos, J.A.; Yannopoulos, D. Enhancing cardiac arrest survival with extracorporeal cardiopulmonary resuscitation: Insights into the process of death. Ann. N. Y. Acad. Sci. 2022, 1507, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Graesner, J.-T.; Semeraro, F.; Olasveengen, T.; Soar, J.; Lott, C.; Van de Voorde, P.; Madar, J.; Zideman, D.; Mentzelopoulos, S.; et al. European Resuscitation Council Guidelines 2021: Executive summary. Resuscitation 2021, 161, 1–60. [Google Scholar] [CrossRef]
- Morley, P.T.; Atkins, D.L.; Finn, J.C.; Maconochie, I.; Nolan, J.P.; Rabi, Y.; Singletary, E.M.; Wang, T.-L.; Welsford, M.; Olasveengen, T.M.; et al. Evidence Evaluation Process and Management of Potential Conflicts of Interest: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2020, 142 (Suppl. 1), S28–S40. [Google Scholar] [CrossRef] [PubMed]
- Magid, D.J.; Aziz, K.; Cheng, A.; Hazinski, M.F.; Hoover, A.V.; Mahgoub, M.; Panchal, A.R.; Sasson, C.; Topjian, A.A.; Rodriguez, A.J.; et al. Part 2: Evidence Evaluation and Guidelines Development: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142 (Suppl. 2), S358–S365. [Google Scholar] [CrossRef]
- De Buck, E.; Van Remoortel, H.; Dieltjens, T.; Verstraeten, H.; Clarysse, M.; Moens, O.; Vandekerckhove, P. Evidence-based educational pathway for the integration of first aid training in school curricula. Resuscitation 2015, 94, 8–22. [Google Scholar] [CrossRef] [Green Version]
- Böttiger, B.W.; Van Aken, H. Kids save lives: Training school children in cardiopulmonary resuscitation worldwide is now endorsed by the World Health Organization (WHO). Resuscitation 2015, 94, A5–A7. [Google Scholar] [CrossRef]
- Calicchia, S.; Cangiano, G.; Capanna, S.; De Rosa, M.; Papaleo, B. Teaching Life-Saving Manoeuvres in Primary School. BioMed Res. Int. 2016, 2016, 2647235. [Google Scholar] [CrossRef] [Green Version]
- Vaughan, N.; John, N.; Rees, N. CPR Virtual Reality Training Simulator for Schools. In Proceedings of the 2019 International Conference on Cyberworlds (CW), Kyoto, Japan, 2–4 October 2019; pp. 25–28. [Google Scholar]
- Santos, I.; Sa-Couto, C.; Vieira-Marques, P. Gamification in CPR—A Review of Game Dynamics and Mechanics. In Proceedings of the 2019 14th Iberian Conference on Information Systems and Technologies (CISTI), Coimbra, Portugal, 19–22 June 2019; pp. 1–4. [Google Scholar]
- Durai, V.S.I.; Arjunan, R.; Manivannan, M. The Effect of Audio and Visual Modality Based CPR Skill Training with Haptics Feedback in VR. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 910–911. [Google Scholar]
- Habibian, T.; Mehta, A.; Harr, A.; Hernandez, L. Design of a mechanical CPR device: Automated CPR To-Go (ACT). In Proceedings of the 2012 38th Annual Northeast Bioengineering Conference (NEBEC), Philadelphia, PA, USA, 16–18 March 2012; pp. 355–357. [Google Scholar]
- Dumcke, R.; Werger, C.; Bottiger, B.W.; Kucknat, L.; Rahe-Meyer, N. The process of implementing cardiopulmonary resus-citation training in schools: A review of current research. J. Innov. Psychol. Educ. Didact. 2019, 23, 141–166. [Google Scholar]
- Stroop, R.; Kerner, T.; Strickmann, B.; Hensel, M. Mobile phone-based alerting of CPR-trained volunteers simultaneously with the ambulance can reduce the resuscitation-free interval and improve outcome after out-of-hospital cardiac arrest: A German, population-based cohort study. Resuscitation 2020, 147, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Vaughan, N.; John, N.; Rees, N. ParaVR: Paramedic Virtual Reality Training Simulator. In Proceedings of the 2019 International Conference on Cyberworlds (CW), Kyoto, Japan, 2–4 October 2019; pp. 21–24. [Google Scholar]
- Durai, S.I.V.; Arjunan, R.; Manivannan, M. Affordable hi-fidelity VR based CPR simulator with haptics feedback. In Proceedings of the 2017 IEEE International Symposium on Haptic, Audio and Visual Environments and Games (HAVE), Abu Dhabi, United Arab Emirates, 22–23 October 2017; pp. 1–5. [Google Scholar]
- Liyanage, S.U.; Jayaratne, L.; Wickramasinghe, M.; Munasinghe, A. Towards an Affordable Virtual Reality Solution for Car-diopulmonary Resuscitation Training. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 1054–1055. [Google Scholar]
- Everson, T.; Joordens, M.; Forbes, H.; Horan, B. Virtual Reality and Haptic Cardiopulmonary Resuscitation Training Ap-proaches: A Review. IEEE Syst. J. 2021, 16, 1391–1399. [Google Scholar] [CrossRef]
- Semeraro, F.; Ristagno, G.; Giulini, G.; Gnudi, T.; Kayal, J.S.; Monesi, A.; Tucci, R.; Scapigliati, A. Virtual reality cardiopul-monary resuscitation (CPR): Comparison with a standard CPR training mannequin. Resuscitation 2019, 135, 234–235. [Google Scholar] [CrossRef] [Green Version]
- Leary, M.; McGovern, S.K.; Chaudhary, Z.; Patel, J.; Abella, B.S.; Blewer, A.L. Comparing bystander response to a sudden cardiac arrest using a virtual reality CPR training mobile app versus a standard CPR training mobile app. Resuscitation 2019, 139, 167–173. [Google Scholar] [CrossRef]
- Nas, J.; Thannhauser, J.; Vart, P.; Van Geuns, R.-J.; Van Royen, N.; Bonnes, J.L.; Brouwer, M.A. Rationale and design of the Lowlands Saves Lives trial: A randomised trial to compare CPR quality and long-term attitude towards CPR performance between face-to-face and virtual reality training with the Lifesaver VR app. BMJ Open 2019, 9, e033648. [Google Scholar]
- García Fierros, F.J.; Moreno Escobar, J.J.; Sepúlveda Cervantes, G.; Morales Matamoros, O.; Tejeida Padilla, R. Virtual CPR: Virtual Reality Mobile Application for Training in Cardiopulmonary Resuscitation Techniques. Sensors 2021, 21, 2504. [Google Scholar] [CrossRef]
- Boada, I.; Rodriguez-Benitez, A.; Garcia-Gonzalez, J.M.; Olivet, J.; Carreras, V.; Sbert, M. Using a serious game to complement CPR instruction in a nurse faculty. Comput. Methods Programs Biomed. 2015, 122, 282–291. [Google Scholar] [CrossRef]
- Wattanasoontorn, V.; Magdics, M.; Boada, I.; Sbert, M. A Kinect-Based System for Cardiopulmonary Resuscitation Simulation: A Pilot Study. Serious Games Dev. Appl. 2013, 8101, 51–63. [Google Scholar]
- Di Mitri, D.; Schneider, J.; Specht, M.; Drachsler, H. Detecting Mistakes in CPR Training with Multimodal Data and Neural Networks. Sensors 2019, 19, 3099. [Google Scholar] [CrossRef] [Green Version]
- Park, N.; Kwon, Y.; Lee, S.; Woo, W.; Jeong, J. Projected AR-Based Interactive CPR Simulator. In Systems and Applications, Proceedings of the International Conference on Virtual, Augmented and Mixed Reality, Las Vegas, NV, USA, 21–26 July 2013; Springer: Berlin/Heidelberg, Germany, 2013; Volume 8022, pp. 83–89. [Google Scholar]
- Hubail, D.; Mondal, A.; Al Jabir, A.; Patel, B. Comparison of a virtual reality compression-only Cardiopulmonary Resuscitation (CPR) course to the traditional course with content validation of the VR course—A randomized control pilot study. Ann. Med. Surg. 2022, 73, 103241. [Google Scholar] [CrossRef]
- Kuyt, K.; Park, S.-H.; Chang, T.P.; Jung, T.; MacKinnon, R. The use of virtual reality and augmented reality to enhance cardio-pulmonary resuscitation: A scoping review. Adv. Simul. 2021, 6, 11. [Google Scholar] [CrossRef]
- Jeffers, J.M.; Schreurs, B.A.; Dean, J.L.; Scott, B.; Canares, T.; Tackett, S.; Smith, B.; Billings, E.; Billioux, V.; Sampathkumar, H.D.; et al. Paediatric chest compression performance improves via novel augmented-reality cardiopulmonary resuscitation feedback system: A mixed-methods pilot study in a simulation-based setting. Resusc. Plus 2022, 11, 100273. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, E.; Ambati, R.T.; Shekhar, R.; Staffa, S.J.; Zurakowski, D.; Sinha, P. A smartphone application to provide real-time cardiopulmonary resuscitation quality feedback. Am. J. Emerg. Med. 2022, 60, 34–39. [Google Scholar] [CrossRef]
- Gugelmin-Almeida, D.; Tobase, L.; Polastri, T.F.; Peres, H.H.C.; Timerman, S. Do automated real-time feedback devices improve CPR quality? A systematic review of literature. Resusc. Plus 2021, 6, 100108. [Google Scholar] [CrossRef] [PubMed]
- Picard, C.; Drew, R.; Norris, C.M.; O’Dochartaigh, D.; Burnett, C.; Keddie, C.; Douma, M.J. Cardiac Arrest Quality Improvement: A Single-Center Evaluation of Resuscitations Using Defibrillator, Feedback Device, and Survey Data. J. Emerg. Nurs. 2022, 48, 224–232.e8. [Google Scholar] [CrossRef] [PubMed]
- Koyama, Y.; Matsuyama, T.; Kaino, T.; Hoshino, T.; Nakao, J.; Shimojo, N.; Inoue, Y. Adequacy of compression positioning using the feedback device during chest compressions by medical staff in a simulation study. BMC Emerg. Med. 2022, 22, 1–7. [Google Scholar] [CrossRef]
- Lee, S.Y.; Ahn, C. A chest compression feedback device for cardiopulmonary resuscitation in the novel design of a weight-light card holder shape. Resuscitation 2022, 175, 28–29. [Google Scholar] [CrossRef]
- Austin, A.L.; Spalding, C.N.; Landa, K.N.; Myer, B.R.; Cure, D.; Smith, J.E.; Platt, G.; King, H.C. A randomized control trial of cardiopulmonary feedback devices and their impact on infant chest compression quality: A simulation study. Pediatric Emerg. Care 2020, 36, e79–e84. [Google Scholar] [CrossRef]
- Truszewski, Z.; Szarpak, L.; Kurowski, A.; Evrin, T.; Zasko, P.; Bogdanski, L.; Czyzewski, L. Randomized trial of the chest compressions effectiveness comparing 3 feedback CPR devices and standard basic life support by nurses. Am. J. Emerg. Med. 2016, 34, 381–385. [Google Scholar] [CrossRef]
- Vahedian-Azimi, A.; Hajiesmaeili, M.; Amirsavadkouhi, A.; Jamaati, H.; Izadi, M.; Madani, S.J.; Hashemian, S.M.R.; Miller, A.C. Effect of the Cardio First Angel™ device on CPR indices: A randomized controlled clinical trial. Crit. Care 2016, 20, 147. [Google Scholar] [CrossRef] [Green Version]
- Sauro, J. A Practical Guide to the System Usability Scale: Background, Benchmarks & Best Practices; CreateSpace Independent Publishing Platform: Scotts Valley, CA, USA, 2011. [Google Scholar]
Figure 1.
The framework of the teaching aid kit for CPR.

Figure 2.
The manikin module of Resusci Anne.

Figure 3.
The analog piezoelectric ceramic shock sensor.

Figure 4.
The thin-film keyboard.

Figure 5.
The ultrasonic sensor.

Figure 6.
The pressure sensor.

Figure 7.
The gyro sensor, hall magnetic sensor, and barometric pressure sensor.

Figure 8.
The Arduino Mega.

Figure 9.
The interactive CPR tutoring software schematic.

Figure 10.
The interactive CPR tutoring software.

Figure 11.
The user interface of the interactive CPR tutoring software.

Figure 12.
The CPR steps and their corresponding sensors.

Figure 13.
The flowchart of the instruction mode.

Figure 14.
The user interface of the instruction mode.

Figure 15.
The flowchart of the practice mode.

Figure 16.
The interactive teaching aid kit for CPR.

Figure 17.
The LED indicator bars for CPR.

Figure 18.
The sensors installed inside the CPR manikin.

Figure 19.
The magnetic sensors and LED indicator bars installed beneath the skin of the manikin.

Figure 20.
The self-designed AED and the sensor positions of the CPR manikin.

Figure 21.
The example pictures of the public demonstration.


Figure 22.
The analysis results of the questionnaire.

Figure 23.
The waveform analysis of the circulation step: (a) original data; (b) processed data.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The score sheet of the assessment mode.
| Step | Action | Deduct Score |
|---|---|---|
| Check | Operation time exceeds 10 s | 10 |
| Call 911 | Operation time exceeds 10 s | 10 |
| C | Compression depth less than 5 cm | 2 |
| Not reaching the compression at the rate of 100–120/minute | 16 | |
| The chest does not return to its original position | 2 | |
| The interruption time exceeds 10 s | 32 | |
| Incorrect position of the chest compression | 32 | |
| A | Operation time exceeds 15 s | 16 |
| B | Blow time less than 1 s | 8 |
| Blowing too much or too little | 8 | |
| D | Incorrect position of the AED patch | 10 |
Table 2.
The results of the questionnaire.
| System Usability Scale Questionnaire of the Proposed Interactive Teaching Aid Kit for CPR | Strongly Disagree | Disagree | Neutral | Agree | Strongly Agree |
|---|---|---|---|---|---|
| 0 | 2 | 6 | 24 | 11 |
| 0 | 4 | 6 | 17 | 16 |
| 0 | 1 | 8 | 16 | 18 |
| 3 | 5 | 17 | 11 | 7 |
| 0 | 3 | 7 | 22 | 11 |
| 0 | 3 | 7 | 22 | 11 |
| 1 | 0 | 3 | 22 | 17 |
| 0 | 0 | 4 | 20 | 19 |
| 1 | 1 | 5 | 25 | 11 |
| 1 | 5 | 19 | 12 | 6 |
Table 3.
The analysis of the questionnaire.
| System Usability Scale Questionnaire of the Proposed Interactive Teaching Aid Kit for CPR | Average | Standard Deviation | Standard Error |
|---|---|---|---|
| 4.02 | 0.77 | 0.12 |
| 4.05 | 0.95 | 0.14 |
| 4.19 | 0.82 | 0.13 |
| 3.33 | 1.11 | 0.17 |
| 3.95 | 0.84 | 0.13 |
| 3.95 | 0.84 | 0.13 |
| 4.26 | 0.79 | 0.12 |
| 4.35 | 0.65 | 0.10 |
| 4.02 | 0.83 | 0.13 |
| 3.40 | 0.95 | 0.15 |
| Average | 3.95 | 0.86 | 0.13 |
Table 4.
The analysis of the questionnaire in users’ age.
| System Usability Scale Questionnaire of the Proposed Interactive Teaching Aid Kit for CPR | Below 22 Years Old | Above 23 Years Old | Average Deviation |
|---|---|---|---|
| 4.04 | 4.00 | 0.04 |
| 4.17 | 3.89 | 0.27 |
| 4.29 | 4.05 | 0.24 |
| 3.46 | 3.16 | 0.30 |
| 4.04 | 3.84 | 0.20 |
| 4.08 | 3.79 | 0.29 |
| 4.33 | 4.16 | 0.18 |
| 4.50 | 4.16 | 0.34 |
| 4.17 | 3.84 | 0.32 |
| 3.42 | 3.37 | 0.05 |
| Average | 4.05 | 3.83 | 0.22 |
Table 5.
The analysis of the questionnaire in users who have learned CPR before.
| System Usability Scale Questionnaire of the Proposed Interactive Teaching Aid Kit for CPR | Learned CPR Before | Never Learned CPR | Average Deviation |
|---|---|---|---|
| 4.00 | 4.08 | −0.08 |
| 4.13 | 3.83 | 0.30 |
| 4.26 | 4.00 | 0.26 |
| 3.45 | 3.00 | 0.45 |
| 4.10 | 3.58 | 0.51 |
| 4.03 | 3.75 | 0.28 |
| 4.42 | 3.83 | 0.59 |
| 4.48 | 4.00 | 0.48 |
| 4.19 | 3.58 | 0.61 |
| 3.45 | 3.25 | 0.20 |
| Average | 4.05 | 3.69 | 0.36 |
Table 6.
The analysis method of the CPR steps.
| CPR Steps | Related Sensor | Analysis Method |
|---|---|---|
| Check | Analog piezoelectric ceramic shock sensor | Threshold trigger method |
| Call 911 | Thin-film keyboard | Thin-film keyboard input |
| Circulation | Ultrasonic sensor | Waveform analysis method |
| Airway | Gyro sensor | Threshold trigger method |
| Breathing | Barometric pressure sensor | Waveform analysis method |
| Defibrillation | Hall magnetic sensors | Threshold trigger method |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zhao, Y.-X. Interactive Teaching Aid Kit for Cardiopulmonary Resuscitation. Processes 2022, 10, 1515. https://doi.org/10.3390/pr10081515
AMA Style
Zhao Y-X. Interactive Teaching Aid Kit for Cardiopulmonary Resuscitation. Processes. 2022; 10(8):1515. https://doi.org/10.3390/pr10081515
Chicago/Turabian StyleZhao, Yu-Xiang. 2022. "Interactive Teaching Aid Kit for Cardiopulmonary Resuscitation" Processes 10, no. 8: 1515. https://doi.org/10.3390/pr10081515
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.