
The CSHQ-DE Questionnaire Uncovers Relevant Sleep Disorders in Children and Adolescents with Long COVID

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort Composition
2.2. CSHQ-DE
2.3. Further Investigations
2.4. Statistical Analysis
3. Results
4. Discussion
Treatment Recommendations
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Howard-Jones, A.R.; Burgner, D.P.; Crawford, N.W.; Goeman, E.; Gray, P.E.; Hsu, P.; Kuek, S.; McMullan, B.J.; Tosif, S.; Wurzel, D.; et al. COVID-19 in children. II: Pathogenesis, disease spectrum and management. J. Paediatr. Child Health 2021, 58, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, P.; Pittet, L.F.; Curtis, N. The Challenge of Studying Long COVID: An Updated Review. Pediatric Infect. Dis. J. 2022, 41, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Kikkenborg Berg, S.; Dam Nielsen, S.; Nygaard, U.; Bundgaard, H.; Palm, P.; Rotvig, C.; Vinggaard Christensen, A. Long COVID symptoms in SARS-CoV-2-positive adolescents and matched controls (Long COVIDKidsDK): A national, cross-sectional study. Lancet Child Adolesc. Health 2022, 6, 240–248. [Google Scholar] [CrossRef]
- COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/ng188/resources/COVID19-rapid-guideline-managing-the-longterm-effects-of-COVID19-pdf-51035515742 (accessed on 22 July 2022).
- Coronavirus Disease (COVID-19): Post COVID-19 Condition. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(COVID-19)-post-COVID-19-condition (accessed on 8 July 2022).
- Koczulla, A.R.; Ankermann, T.; Behrends, U.; Berlit, P.; Böing, S.; Brinkmann, F.; Franke, C.; Glöckl, R.; Gogoll, C.; Hummel, T.; et al. S1 Guideline Post-COVID/Long-COVID. Available online: https://www.awmf.org/uploads/tx_szleitlinien/020-027l_S1_Post_COVID_Long_COVID_2022-08.pdf (accessed on 8 July 2022).
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long COVID-mechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef]
- Garg, M.; Maralakunte, M.; Garg, S.; Dhooria, S.; Sehgal, I.; Seith Bhalla, A.; Vijayvergiya, R.; Grover, S.; Bhatia, V.; Jagia, P.; et al. The Conundrum of ‘Long-COVID-19’: A Narrative Review. Int. J. Gen. Med. 2021, 14, 2491–2506. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Nguyen, N.N.; Hoang, V.T.; Dao, T.L.; Dudouet, P.; Eldin, C.; Gautret, P. Clinical patterns of somatic symptoms in patients suffering from post-acute long COVID: A systematic review. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 515–545. [Google Scholar] [CrossRef]
- Borch, L.; Holm, M.; Knudsen, M.; Ellermann-Eriksen, S.; Hagstroem, S. Long COVID symptoms and duration in SARS-CoV-2 positive children—A nationwide cohort study. Eur. J. Pediatrics 2022, 181, 1597–1607. [Google Scholar] [CrossRef]
- Töpfner, N.; Deutsche Gesellschaft für Pädiatrische Infektiologie e. V. (DGPI); Alberer, M.; Gesellschaft für Pädiatrische Pneumologie e. V. (GPP); Bender, S.; Deutsche Gesellschaft für Kinder- und Jugendpsychiatrie, Psychosomatik und Psychotherapie e. V. (DGKJP); Berner, R.; de Laffolie, J.; Gesellschaft für Pädiatrische Gastroenterologie und Ernährung e. V. (GPGE); Dingemann, J.; et al. Recommendation for standardized medical care for children and adolescents with long COVID. Montasschrift Kinderheilkd. 2022, 170, 539–547. [Google Scholar] [CrossRef]
- shkenazi-Hoffnung, L.; Shmueli, E.; Ehrlich, S.; Ziv, A.; Bar-On, O.; Birk, E.; Lowenthal, A.; Paris, D. Long COVID in Children: Observations From a Designated Pediatric Clinic. Pediatric Infect. Dis. J. 2021, 40, e509–e511. [Google Scholar] [CrossRef]
- Lewandowski, A.S.; Ward, T.M.; Palermo, T.M. Sleep problems in children and adolescents with common medical conditions. Pediatr. Clin. North Am. 2011, 58, 699–713. [Google Scholar] [PubMed]
- Schlarb, A.A.; Schwerdtle, B.; Hautzinger, M. Validation and psychometric properties of the German version of the Children’s Sleep Habits Questionnaire (CSHQ-DE). Somnologie 2010, 14, 260–266. [Google Scholar] [CrossRef]
- Schwerdtle, B.; Kanis, J.; Kahl, L.; Kübler, A.; Schlarb, A. A new diagnostic tool for children with sleep disorders. Somnologie 2013, 17, 199–204. [Google Scholar] [CrossRef]
- Owens, J.A.; Spirito, A.; McGuinn, M. The Children’s Sleep Habits Questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep 2000, 23, 1–9. [Google Scholar] [CrossRef]
- van Kessel, S.A.M.; Olde Hartmann, T.C.; Lucassen, P.L.B.J.; van Jaarsveld, C.H.M. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2022, 39, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Nemati, H.; Shahisavandi, M.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; et al. Long COVID in children and adolescents. World J. Pediatrics 2021, 17, 495–499. [Google Scholar] [CrossRef]
- Stephenson, T.; Allin, B.; Nugawela, M.D.; Rojas, N.; Dalrymple, E.; Pinto Pereira, S.; Soni, M.; Knight, M.; Cheung, E.Y.; Heyman, I. Long COVID (post-COVID-19 condition) in children: A modified Delphi process. Arch. Dis. Child. 2022, 107, 674–680. [Google Scholar] [CrossRef]
- Bhat, S.; Chokroverty, S. Sleep disorders and COVID-19. Sleep Med. 2022, 91, 253–261. [Google Scholar] [CrossRef]
- Semyachkina-Glushkovskaya, O.; Mamedova, A.; Vinnik, V.; Klimova, M.; Saranceva, E.; Ageev, V.; Tingting, Y.; Zhu, D.; Penzel, T.; Kurths, J. Brain Mechanisms of COVID-19-Sleep Disorders. Int. J. Mol. Sci. 2021, 22, 6917. [Google Scholar] [CrossRef]
- Yong, S.J. Persistent Brainstem Dysfunction in Long-COVID: A Hypothesis. ACS Chem. Neurosci. 2021, 12, 573–580. [Google Scholar] [CrossRef]
- Krueger, J.M.; Majde, J.A.; Rector, D.M. Cytokines in immune function and sleep regulation. Handb. Clin. Neurol. 2011, l98, 229–240. [Google Scholar]
- Marshall, L.; Born, J. Brain-immune interactions in sleep. Int. Rev. Neurobiol. 2002, 52, 93–131. [Google Scholar] [PubMed]
- Mardani, M. Post COVID syndrome. Arch. Clin. Infect Dis. 2020, 15, e108819. [Google Scholar] [CrossRef]
- Kappelmann, N.; Dantzer, R.; Khandaker, G.M. Interleukin-6 as potential mediator of long-term neuropsychiatric symptoms of COVID-19. Psychoneuroendocrinology 2021, 131, 105295. [Google Scholar] [CrossRef]
- Novelli, L.; Motta, F.; De Santis, M.; Ansari, A.A.; Gershwin, M.E.; Selmi, C. The JANUS of chronic inflammatory and autoimmune diseases onset during COVID-19—A systematic review of the literature. J. Autoimmun. 2021, 117, 102592. [Google Scholar] [CrossRef] [PubMed]
- Seeßle, J.; Waterboer, T.; Hippchen, T.; Simon, J.; Kirchner, M.; Lim, A.; Müller, B.; Merle, U. Persistent symptoms in adult patients one year after COVID-19: A prospective cohort study. Clin. Infect Dis. 2021, 74, 1191–1198. [Google Scholar] [CrossRef]
- Wallukat, G.; Hohberger, B.; Wenzel, K.; Fürst, J.; Schulze-Rothe, S.; Wallukat, A.; Hönicke, A.-S.; Müller, J. Functional autoantibodies against G-protein coupled receptors in patients with persistent Long-COVID-19 symptoms. J. Transl. Autoimmun. 2021, 4, 100100. [Google Scholar] [CrossRef]
- Quintero, O.L.; Amador-Patarroya, M.J.; Montoya-Ortiz, G.; Rojas-Villarraga, A.; Anaya, J.-M. Autoimmune disease and gender: Plausible mechanisms for the female predominance of autoimmunity. J. Autoimmun. 2012, 38, J109–J119. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of Antibody Immunity to SARS-CoV-2. bioRxiv 2020. [Google Scholar] [CrossRef]
- Rudroff, T.; Fietsam, A.C.; Deters, J.R.; Bryant, A.D.; Kamholz, J. Post-COVID-19 Fatigue: Potential Contributing Factors. Brain Sci. 2020, 10, 1012. [Google Scholar] [CrossRef]
- Schilling, C.; Meyer-Lindenberg, A.; Schweiger, J.I. Kognitive Störungen und Schlafstörungen bei Long-COVID. Der Nervenarzt 2022, 93, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Vitti-Ruela, B.V.; Dokkedal-Silva, V.; Rosa, D.S.; Tufik, S.; Levy Andersen, M. Possible sequelae in post-SARS-CoV-2 patients: Effects on sleep and general health condition. Sleep Breath 2020, 25, 963–964. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xu, D.; Xie, B.; Zhang, Y.; Huang, H.; Liu, H.; Chen, H.; Sun, Y.; Shang, Y.; Hashimoto, K.; et al. Poor-sleep is associated with slow recovery from lymphopenia and an increased need for ICU care in hospitalized patients with COVID-19: A retrospective cohort study. Brain Behav. Immun. 2020, 88, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, C.A.; Rizvydeen, M.; Conroy, D.A.; O’Brien, L.M.; Gupta, G.; Somers, E.C.; Sharma, P.; Golob, J.L.; Troost, J.P.; Burgess, H.J. The prevalence and impact of pre-existing sleep disorder diagnoses and objective sleep parameters in patients hospitalized for COVID-19. J. Clin. Sleep Med. 2021, 17, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Niu, Y.; Zhao, W.; Bao, P.; Li, D. Reduced sleep in the week prior to diagnosis of COVID-19 is associated with the severity of COVID-19. Nat. Sci. Sleep 2020, 12, 999–1007. [Google Scholar] [CrossRef]
- Coulson, R.L.; Morrain, P.; Wang, G.X. Sleep deficiency as a driver of cellular stress and damage in neurological disorders. Sleep Med. Rev. 2022, 63, 101616. [Google Scholar] [CrossRef]
- Neuhauser, H.; Poethko-Müller, C. Chronische Erkrankungen und impfpräventable Infektionserkrankungen bei Kindern und Jugendlichen in Deutschland. In Robert Koch-Institut, Epidemiologie und Gesundheitsberichterstattung; Springer: Berlin/Heidelberg, Germany, 2014; Volume 57. [Google Scholar]
- Rao, S.; Lee, G.M.; Razzaghi, H.; Lorman, V.; Mejias, A.; Pajor, N.M.; Thacker, D.; Webb, R.; Dickinson, K.; Bailey, L.C.; et al. Clinical Features and Burden of Postacute Sequelae of SARS-CoV-2 Infection in Children and Adolescents. JAMA Pediatr. 2022. published online Aug 22, 2022 (preprint). [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Kinder- und Jugendpsychiatrie, Psychosomatik und Psychotherapie e.V. (DGKJP). S1-Leitlinie: Nichtorganische Schlafstörungen (F51). Available online: https://www.awmf.org/uploads/tx_szleitlinien/028-012l_S1_Nicht-organische-Schlafstoerungen_2022-01.pdf (accessed on 22 July 2022).
- Jarrott, B.; Head, R.; Pringle, K.G.; Lumbers, E.R.; Martin, J.H. “LONG COVID”—A hypothesis for understanding the biological basis and pharmacological treatment strategy. Pharm. Res. Perspect 2022, 10, e00911. [Google Scholar] [CrossRef]
- Anderson, G.; Reiter, R.J. Melatonin: Roles in Influenza, COVID-19, and Other Viral Infections. Rev. Med. Virol. 2020, 30, e2109. [Google Scholar] [CrossRef]
- Lowes, D.A.; Webster, N.R.; Murphy, M.P.; Galley, H.F. Antioxidants that protect mitochondria reduce interleukin-6 and oxidative stress, improve mitochondrial function, and reduce biochemical markers of organ dysfunction in a rat model of acute sepsis. Br. J. Anaesth. 2013, 110, 472–539. [Google Scholar] [CrossRef]
- Vilser, D. Long COVID/Post-COVID-19-Syndrom bei Kindern und Jugendlichen. Pädiatrie 2022, 34, 20–25. [Google Scholar] [CrossRef]
- Galley, H.F.; Lowes, D.A.; Allen, L.; Cameron, G.; Aucott, L.S.; Webster, N.R. Melatonin as a potential therapy for sepsis: A phase I dose escalation study and an ex vivo whole blood model under conditions of sepsis. J. Pineal Res. 2014, 56, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Evans, P.C.; Rainger, G.E.; Mason, J.C.; Guzik, T.J.; Osto, E.; Stamataki, Z.; Neil, D.; Hoefer, I.E.; Fragiadaki, M.; Waltenberger, J.; et al. Endothelial dysfunction in COVID-19: A position paper of the ESC Working Group for Atherosclerosis and Vascular Biology, and the ESC Council of Basic Cardiovascular Science. Cardiovasc. Res. 2020, 116, 2177–2184. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Mejia-Renteria, H.; Travieso, A.; Sagir, A.; Martinez-Gómez, E.; Carrascosa-Granada, A.; Toya, T.; Nunez-Gil, I.; Estrada, V.; Lerman, A.; Escaned, J. In-vivo evidence of systemic endothelial vascular dysfunction in COVID-19. Int. J. Cardiol. 2021, 354, 153–155. [Google Scholar] [CrossRef]
- Rovas, A.; Osiaevi, I.; Buscher, K.; Sackarnd, J.; Tepasse, P.-R.; Fobker, M.; Kühn, J.; Braune, S.; Göbel, U.; Thölking, G.; et al. Microvascular dysfunction in COVID-19: The MYSTIC study. Angiogenesis 2021, 24, 145–157. [Google Scholar] [CrossRef]
- Wang, X.; Kant Sahu, K.; Cerny, J. Coagulopathy, endothelial dysfunction, thrombotic microangiopathy and complement activation: Potential role of complement system inhibition in COVID-19. J Thromb Thrombolysis 2021, 51, 657–662. [Google Scholar] [CrossRef]
- Otifi, H.M.; Adiga, B.K. Endothelial Dysfunction in COVID-19 Infection. Am. J. Med. Sci. 2022, 363, 281–287. [Google Scholar] [CrossRef]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef]
- Sashindranath, M.; Nandurkar, H.H. Endothelial Dysfunction in the Brain: Setting the Stage for Stroke and Other Cerebrovascular Complications of COVID-19. Stroke 2021, 52, 1895–1904. [Google Scholar] [CrossRef]
- Ergul, E.; Yilmaz, A.S.; Ögütveren, M.M.; Emlek, N.; Kostakoglu, U.; Cetin, M. COVID 19 disease independently predicted endothelial dysfunction measured by flow-mediated dilatation. Int. J. Cardiovasc. Imaging 2022, 38, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.; Souvaliotis, N.; Lampsas, S.; Siasos, G.; Poulakou, G.; Theofilis, P.; Papaioannou, T.G.; Haidich, A.-B.; Tsaousi, G.; Papaioannou, T.G.; et al. Endothelial dysfunction in acute and long standing COVID−19: A prospective cohort study. Vasc. Pharmacol. 2022, 144, 106975. [Google Scholar]
- Seitz, A.; Ong, P. Endothelial dysfunction in COVID-19: A potential predictor of long-COVID? Int. J. Cardiol. 2022, 349, 155–156. [Google Scholar] [CrossRef]
- Gupte, A.A.; Lyon, C.J.; Hsueh, W.A. Nuclear factor (erythroid-derived 2)-like-2 factor (Nrf2), a key regulator of the antioxidant response to protect against atherosclerosis and nonalcoholic steatohepatitis. Curr. Diab Rep. 2013, 13, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.; Maes, M.; Markus, R.P.; Rodrigues, M. Ebola virus: Melatonin as a readily available treatment option. J. Med. Virol. 2015, 87, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Paemanee, A.; Hitakarun, A.; Roytrakul, S.; Smith, D.R. Screening of melatonin, α-tocopherol, folic acid, acetyl-L-carnitine and resveratrol for anti-dengue 2 virus activity. BMC Res Notes 2018, 11, 307. [Google Scholar] [CrossRef] [PubMed]
- Kotb Elmahallawy, E.; Ortega Luque, J.; Saleh Aloweidi, A.; Gutierrez-Fernandez, J.; Sampedro-Martinez, A.; Rodriguez-Granger, J.; Kaki, A.; Agil, A. Potential relevance of melatonin against some infectious agents: A review and assessment of recent research. Curr. Med. Chem. 2015, 22, 3848–3861. [Google Scholar] [CrossRef]
- Cross, K.M.; Landis, D.M.; Sehgal, L.; Payne, J.D. Melatonin for the early treatment of COVID-19: A narrative review of current evidence and possible efficacy. Endocr Prac. 2021, 27, 850–855. [Google Scholar] [CrossRef]
- International Clinical Trials Registry Platform (ICTRP)—Important Information about the COVID-19 Outbreak. Available online: https://www.who.int/clinical-trials-registry-platform (accessed on 22 July 2022).
- Al-Ameri, L.T.; Hameed, E.K.; Maroof, B.S. Sleep quality in COVID-19 recovered patients. Sleep Sci. 2022, 15, 168–171. [Google Scholar] [CrossRef]
- Camacho-Montano, L.R.; Iranzo, A.; Martinez-Piédrola, R.; Camacho-Montano, L.; Huertas-Hoyas, E.; Serrada-Tejeda, S.; Garcia-Bravo, C.; de Heredia-Torres, M. Effects of COVID-19 home confinement on sleep in children: A systematic review. Sleep Med. Rev. 2022, 62, 101596. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n | Distribution |
|---|---|---|
| n | 45 | |
| Age, mean in years | 45 | 10.0 (IQR 8.0, 14.0) |
| Female gender | 45 | 29 (64%) |
| BMI percentile, mean (based on CDC) | 45 | 74.0 (IQR 39.0, 89.0) |
| COVID-19 Course | 45 | |
| -Asymptomatic | 5 (11%) | |
| -Mild | 35 (78%) | |
| -Moderate | 5 (11%) | |
| Medical History | ||
Pulmonary/allergic diseases
| 10 (22%) −2 −3 −3 −1 −1 | |
Neurological diseases
| 5 (11%) −2 −1 −1 −1 | |
| von Willebrand disease (type 1) | 1 | |
| Right-sided aortic arch * Autoimmune hepatitis or primary sclerosing cholangitis Constipation | 1 1 1 | |
| Obesity Metabolic syndrome | 2 1 | |
| Psychogenic gait disorder or somatization disorder | 1 | |
| Williamsbeuren Syndrome | 1 | |
| Prematurity (32 and 34 weeks gestation) | 2 |
| Symptoms | In Total (%) |
|---|---|
| Fatigue/stress intolerance | 30/45 (62%) |
| Concentration/learning difficulties | 20/45 (44%) |
| Sleep disorders | 19/45 (42%) |
| Pulmonary symptoms | 17/45 (38%) |
| Headache | 16/45 (36%) |
| Gastrointestinal symptoms | 14/45 (31%) |
| Cardiac symptoms | 10/45 (22%) |
| Dizziness | 10/45 (22%) |
| Muscle and joint symptoms | 9/45 (20%) |
| Neurological symptoms | 9/45 (20%) |
| Smell and taste disorders | 9/45 (20%) |
| Hair loss | 6/45 (13%) |
| Skin changes | 4/45 (9%) |
| Symptoms | In Total (%) |
|---|---|
| Fatigue/stress intolerance | 30/45 (62%) |
| 0–5 years | 5/9 (56%) |
| 6–11 years | 11/18 (61%) |
| 12–18 years | 12/18 (67%) |
| Concentration/learning difficulties | 20/45 (44%) |
| 0–5 years | 1/9 (11%) |
| 6–11 years | 10/18 (56%) |
| 12–18 years | 9/18 (50%) |
| Sleep disorders (reported in the medical history) | 19/45 (42%) |
| 0–5 years | 3/9 (33%) |
| 6–11 years | 7/18 (39%) |
| 12–18 years | 9/18 (50%) |
| Pulmonary symptoms | 17/45 (38%) |
| 0–5 years | 5/9 (55.6%) |
| 6–11 years | 5/18 (28%) |
| 12–18 years | 7/18 (39%) |
| Headache | 16/45 (36%) |
| 0–5 years | 0/9 (0%) |
| 6–11 years | 8/18 (44%) |
| 12–18 years | 8/18 (44%) |
| Gastrointestinal symptoms | 14/45 (31%) |
| 0–5 years | 4/9 (44%) |
| 6–11 years | 3/18 (17%) |
| 12–18 years | 7/18 (39%) |
| Cardiac symptoms | 10/45 (22%) |
| 0–5 years | 0/9 (0%) |
| 6–11 years | 4/18 (22%) |
| 12–18 years | 6/18 (33%) |
| Dizziness | 10/45 (22%) |
| 0–5 years | 2/9 (22%) |
| 6–11 years | 2/18 (11%) |
| 12–18 years | 6/18 (33%) |
| Muscle and joint symptoms | 9/45 (20%) |
| 0–5 years | 2/9 (22%) |
| 6–11 years | 3/18 (17%) |
| 12–18 years | 4/18 (22%) |
| Neurological symptoms | 9/45 (20%) |
| 0–5 years | 2/9 (22%) |
| 6–11 years | 4/18 (22%) |
| 12–18 years | 3/18 (17%) |
| Smell and taste disorders | 9/45 (20%) |
| 0–5 years | 0/9 (0%) |
| 6–11 years | 2/18 (11%) |
| 12–18 years | 7/18 (39%) |
| Hair loss | 6/45 (13%) |
| 0–5 years | 1/9 (11%) |
| 6–11 years | 1/18 (6%) |
| 12–18 years | 4/18 (22%) |
| Skin changes | 4/45 (9%) |
| 0–5 years | 1/9 (11%) |
| 6–11 years | 3/18 (17%) |
| 12–18 years | 0/18 (0%) |
| Age Group | Total CSHQ-DE | p-Value | ||
|---|---|---|---|---|
| Pre-COVID | Post-COVID 1st Assessment | Post-COVID 2nd Assessment | ||
| 0–5 years | 49.0 (IQR 46.0, 61.0) | 55.0 (IQR 53.0, 58.0) | 48.0 (IQR 45.0, 53.0) | 0.131 |
| 6–11 years | 46.5 (IQR 40.0, 52.25) | 54.0 (IQR 45.0, 56.0) | 47.0 (IQR 44.0, 55.75) | 0.035 |
| 12–18 years | 43.0 (IQR 38.25, 44.0) | 45.0 (IQR 41.0, 46.75) | 43.5(IQR 40.25, 46.75) | 0.007 |
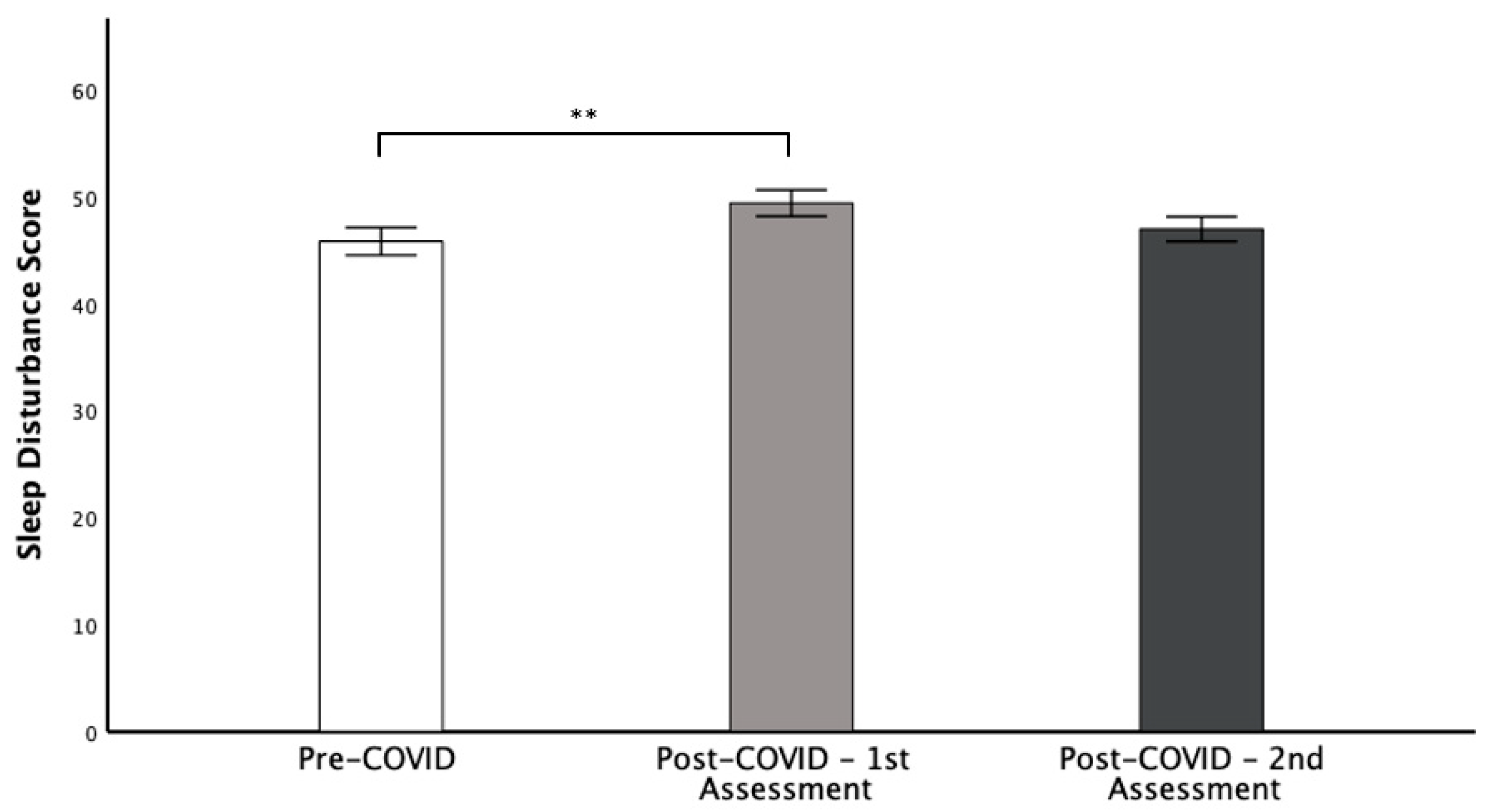
| CSHQ-DE Subscales | Pre-COVID-19 | Post-COVID-19 Initial Presentation | Post-COVID-19 Re-Presentation | p-Value |
|---|---|---|---|---|
| Bedtime resistance | 8.2 (± 2.7) | 8.4 (± 2.4) | 8.0 (± 2.7) | 0.495 |
| Sleep onset delay | 1.8 (± 0.9) | 2.0 (± 0.8) | 2.0 (± 0.9) | 0.239 |
| Sleep duration | 4.1 (± 1.3) | 4.6 (± 1.4) | 4.5 (± 1.6) | 0.150 |
| Sleep anxiety | 5.4 (± 2.1) | 5.5 (± 1.9) | 5.3 (± 2.2) | 0.665 |
| Night waking | 4.0 (± 1.6) | 4.5 (± 1.6) | 4.2 (± 1.5) | 0.130 |
| Parasomnia | 9.0 (± 2.6) | 9.3 (± 2.4) | 9.1 (± 2.4) | 0.645 |
| Sleep-disordered breathing | 3.5 (± 1.1) | 3.5 (± 1.0) | 3.6 (± 1.3) | 0.543 |
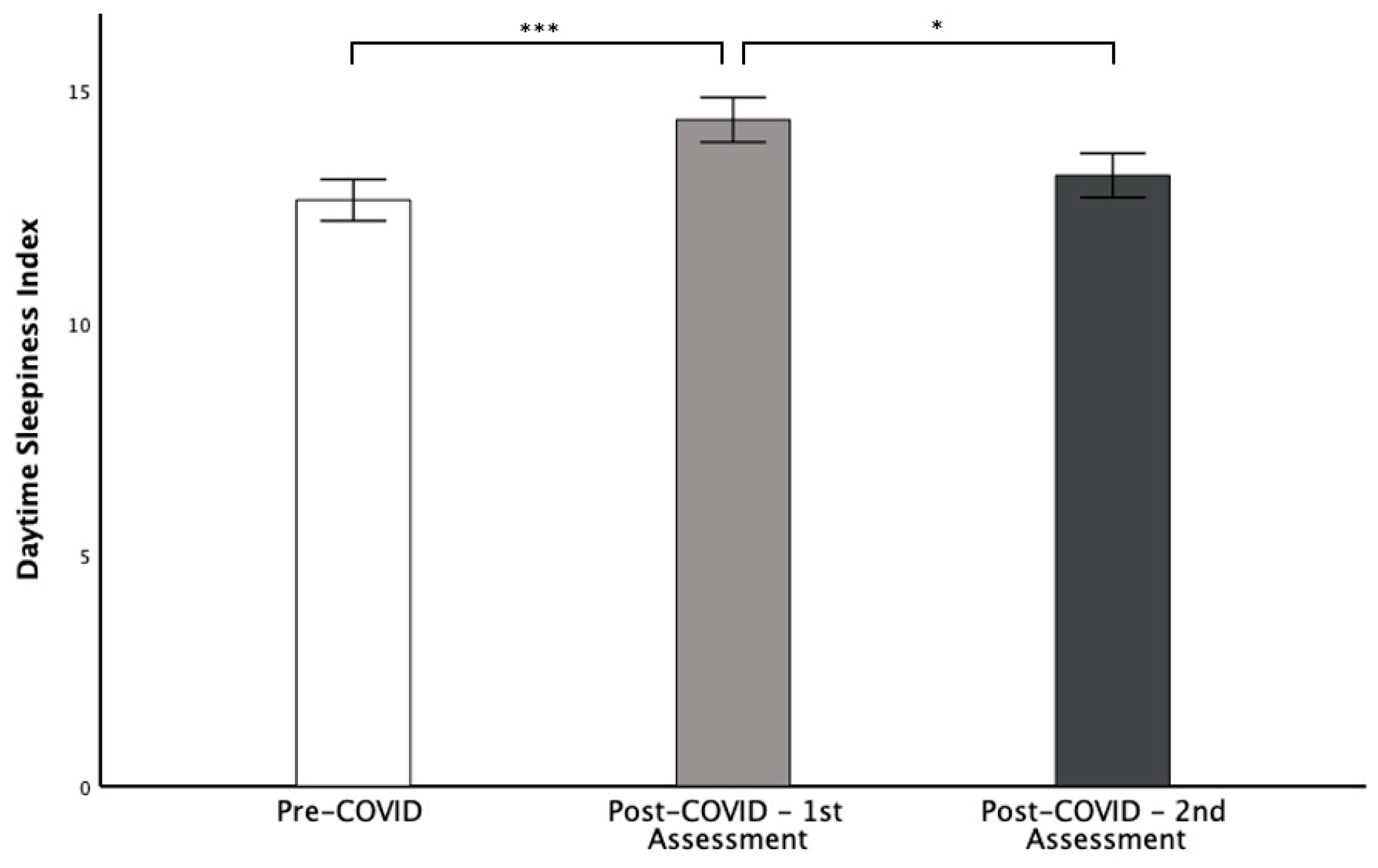
| Daytime sleepiness | 12.6 (± 3.0) | 14.4 (± 3.2) | 13.2 (± 3.2) | < 0.001 |
|
|
|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Werner, S.; Doerfel, C.; Biedermann, R.; Lorenz, M.; Rasche, M.; Proquitté, H.; Newman, L.; Vilser, D. The CSHQ-DE Questionnaire Uncovers Relevant Sleep Disorders in Children and Adolescents with Long COVID. Children 2022, 9, 1419. https://doi.org/10.3390/children9091419
Werner S, Doerfel C, Biedermann R, Lorenz M, Rasche M, Proquitté H, Newman L, Vilser D. The CSHQ-DE Questionnaire Uncovers Relevant Sleep Disorders in Children and Adolescents with Long COVID. Children. 2022; 9(9):1419. https://doi.org/10.3390/children9091419
Chicago/Turabian StyleWerner, Sarah, Claus Doerfel, Richard Biedermann, Michael Lorenz, Marius Rasche, Hans Proquitté, Lars Newman, and Daniel Vilser. 2022. "The CSHQ-DE Questionnaire Uncovers Relevant Sleep Disorders in Children and Adolescents with Long COVID" Children 9, no. 9: 1419. https://doi.org/10.3390/children9091419