
Fatigue and Quality of Life in Children with Chronic Kidney Disease
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Instruments
2.4. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harambat, J.; Van Stralen, K.J.; Kim, J.J.; Tizard, E.J. Epidemiology of chronic kidney disease in children. Pediatr. Nephrol. 2012, 27, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Didsbury, M.; van Zwieten, A.; Howell, M.; Kim, S.; Tong, A.; Howard, K.; Nassar, N.; Barton, B.; Lah, S.; et al. Neurocognitive and Educational Outcomes in Children and Adolescents with CKD: A Systematic Review and Meta-Analysis. Clin. J. Am. Soc. Nephrol. 2018, 13, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Gerson, A.C.; Butler, R.; Moxey-Mims, M.; Wentz, A.; Shinnar, S.; Lande, M.B.; Mendley, S.R.; Warady, B.A.; Furth, S.L.; Hooper, S.R. Neurocognitive outcomes in children with chronic kidney disease: Current findings and contemporary endeavors. Ment. Retard. Dev. Disabil. Res. Rev. 2006, 12, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Duquette, P.J.; Hooper, S.R.; Wetherington, C.E.; Icard, P.F.; Gipson, D.S. Brief report: Intellectual and academic functioning in pediatric chronic kidney disease. J. Pediatr. Psychol. 2007, 32, 1011–1017. [Google Scholar] [CrossRef]
- Bakr, A.; Amr, M.; Sarhan, A.; Hammad, A.; Ragab, M.; El-Refaey, A.; El-Mougy, A. Psychiatric disorders in children with chronic renal failure. Pediatr. Nephrol. 2007, 22, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Marciano, R.C.; Soares, C.M.B.; Diniz, J.S.S.; Lima, E.M.; Silva, J.M.P.; Canhestro, M.R.; Gazzinelli, A.; Melo, C.C.D.; Dias, C.S.; Simões e Silva, A.C.; et al. Behavioral disorders and low quality of life in children and adolescents with chronic kidney disease. Pediatr. Nephrol. 2010, 26, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Gerson, A.C.; Wentz, A.; Abraham, A.G.; Mendley, S.R.; Hooper, S.R.; Butler, R.W.; Gipson, D.S.; Lande, M.B.; Shinnar, S.; Moxey-Mims, M.M.; et al. Health-related quality of life of children with mild to moderate chronic kidney disease. Pediatrics 2010, 125, e349–e357. [Google Scholar] [CrossRef]
- Jhamb, M.; Weisbord, S.D.; Steel, J.L.; Unruh, M. Fatigue in patients receiving maintenance dialysis: A review of definitions, measures, and contributing factors. Am. J. Kidney Dis. 2008, 52, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Gregg, L.P.; Bossola, M.; Ostrosky-Frid, M.; Hedayati, S.S. Fatigue in CKD: Epidemiology, Pathophysiology, and Treatment. Clin. J. Am. Soc. Nephrol. 2021, 16, 1445–1455. [Google Scholar] [CrossRef]
- Gollie, J.M.; Patel, S.S.; Harris-Love, M.O.; Cohen, S.D.; Blackman, M.R. Fatigability and the Role of Neuromuscular Impairments in Chronic Kidney Disease. Am. J. Nephrol. 2022, 53, 253–263. [Google Scholar] [CrossRef]
- Bossola, M.; Di Stasio, E.; Antocicco, M.; Panico, L.; Pepe, G.; Tazza, L. Fatigue Is Associated with Increased Risk of Mortality in Patients on Chronic Hemodialysis. Nephron Exp. Nephrol. 2015, 130, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Roumelioti, M.-E.; Wentz, A.; Schneider, M.F.; Gerson, A.C.; Hooper, S.; Benfield, M.; Warady, B.A.; Furth, S.L.; Unruh, M.L. Sleep and fatigue symptoms in children and adolescents with CKD: A cross-sectional analysis from the chronic kidney disease in children (CKiD) study. Am. J. Kidney Dis. 2010, 55, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Burwinkle, T.M.; Szer, I.S. The PedsQL Multidimensional Fatigue Scale in pediatric rheumatology: Reliability and validity. J. Rheumatol. 2004, 31, 2494–2500. [Google Scholar] [PubMed]
- Smout, M.F.; Manzoni, G.M.; Tamini, S.; Marazzi, N.; de Col, A.; Pietrabissa, G.; Castelnuovo, G.; Molinari, E.; Sartorio, A. Pediatric quality of life multidimensional fatigue scale (PedsQL-MFS) detects the effects of a 3-week Inpatient body weight reduction program for children and adolescents with obesity. Health Qual. Life Outcomes 2022, 20, 3. [Google Scholar] [CrossRef]
- Alemdaroglu-Gurbuz, I.; Bulut, N.; Bozgeyik, S.; Ulug, N.; Arslan, S.S.; Yilmaz, O.; Karaduman, A. Reliability and validity of the turkish translation of pedsqlTM multidimensional Fatigue scale in Duchenne Muscular Dystrophy. Neurosciences 2019, 24, 302–310. [Google Scholar] [CrossRef]
- Panepinto, J.A.; Torres, S.; Bendo, C.B.; McCavit, T.L.; Dinu, B.; Sherman-Bien, S.; Bemrich-Stolz, C.; Varni, J.W. PedsQL™ Multidimensional Fatigue Scale in sickle cell disease: Feasibility, reliability, and validity. Pediatr. Blood Cancer 2014, 61, 171–177. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Seid, M.; Skarr, D. The PedsQL 4.0 as a pediatric population health measure: Feasibility, reliability, and validity. Ambul. Pediatr. 2003, 3, 329–341. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL 4.0: Reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Lopes, M.; Ferraro, A.; Koch, V.H. Health-related quality of life of children and adolescents with CKD stages 4–5 and their caregivers. Pediatr. Nephrol. 2014, 29, 1239–1247. [Google Scholar] [CrossRef]
- Neul, S.K.; Minard, C.G.; Currier, H.; Goldstein, S.L. Health-related quality of life functioning over a 2-year period in children with end-stage renal disease. Pediatr. Nephrol. 2013, 28, 285–293. [Google Scholar] [CrossRef]
- Leng, S.; Chen, X.; Mao, G. Frailty syndrome: An overview. Clin. Interv. Aging 2014, 9, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, E.C.; Kennedy, C.C.; Rule, A.D.; LeBrasseur, N.K.; Kirkland, J.L.; Hickson, L.J. Frailty in CKD and Transplantation. Kidney Int. Rep. 2021, 6, 2270–2280. [Google Scholar] [CrossRef] [PubMed]
- Karava, V.; Dotis, J.; Christoforidis, A.; Kondou, A.; Printza, N. Muscle-bone axis in children with chronic kidney disease: Current knowledge and future perspectives. Pediatr. Nephrol. 2021, 36, 3813–3827. [Google Scholar] [CrossRef] [PubMed]
- Karava, V.; Dotis, J.; Christoforidis, A.; Liakopoulos, V.; Kondou, A.; Tsigaras, G.; Tsioni, K.; Kollios, K.; Printza, N. Association between insulin growth factor-1, bone mineral density, and frailty phenotype in children with chronic kidney disease. Pediatr. Nephrol. 2021, 36, 1861–1870. [Google Scholar] [CrossRef] [PubMed]
- Amaral, S.; Sayed, B.A.; Kutner, N.; Patzer, R.E. Preemptive kidney transplantation is associated with survival benefits among pediatric patients with end-stage renal disease. Kidney Int. 2016, 90, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Stabouli, S.; Gidaris, D.; Printza, N.; Dotis, J.; Papadimitriou, E.; Chrysaidou, K.; Papachristou, F.; Zafeiriou, D. Sleep disorders and executive function in children and adolescents with chronic kidney disease. Sleep Med. 2018, 55, 33–39. [Google Scholar] [CrossRef]
- Stabouli, S.; Papadimitriou, E.; Printza, N.; Dotis, J.; Papachristou, F. Sleep disorders in pediatric chronic kidney disease patients. Pediatr. Nephrol. 2015, 31, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.T.; Lin, M.T.; Chen, Y.C.; Lee, C.H.; Hsu, W.C.; Chang, R.E. Prevalence of sleep disorders in children with chronic kidney disease: A meta-analysis. Pediatr. Nephrol. 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Parajuli, S.; Tiwari, R.; Clark, D.F.; Mandelbrot, D.A.; Djamali, A.; Casey, K. Sleep disorders: Serious threats among kidney transplant recipients. Transplant. Rev. 2018, 33, 9–16. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Meyers, K.E.; Dhanantwari, P.; Laney, N.; Frank, R.; Sethna, C.B. Sleep-related breathing disorders and cardiometabolic risk factors in pediatric kidney transplant recipients. Pediatr. Transplant. 2022, 23, e14355. [Google Scholar] [CrossRef]
- Buyan, N.; Türkmen, M.A.; Bilge, I.; Baskin, E.; Haberal, M.; Bilginer, Y.; Mir, S.; Emre, S.; Akman, S.; Ozkaya, O.; et al. Quality of life in children with chronic kidney disease (with child and parent assessments). Pediatr. Nephrol. 2010, 25, 1487–1496. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.L.; Graham, N.; Burwinkle, T.; Warady, B.; Farrah, R.; Varni, J.W. Health-related quality of life in pediatric patients with ESRD. Pediatr. Nephrol. 2006, 21, 846–850. [Google Scholar] [CrossRef] [PubMed]
- McKenna, A.M.; Keating, L.E.; Vigneux, A.; Stevens, S.; Williams, A.; Geary, D.F. Quality of life in children with chronic kidney disease-patient and caregiver assessments. Nephrol. Dial. Transplant. 2006, 21, 1899–1905. [Google Scholar] [CrossRef]
- Dotis, J.; Pavlaki, A.; Printza, N.; Stabouli, S.; Antoniou, S.; Gkogka, C.; Kontodimopoulos, N.; Papachristou, F. Quality of life in children with chronic kidney disease. Pediatr. Nephrol. 2016, 31, 2309–2316. [Google Scholar] [CrossRef]
- Eijsermans, R.M.; Creemers, D.G.; Helders, P.J.; Schröder, C.H. Motor performance, exercise tolerance, and health-related quality of life in children on dialysis. Pediatr. Nephrol. 2004, 19, 1262–1266. [Google Scholar] [CrossRef]
- Chiu, M.C.; Ng, C.F.; Lee, L.P.; Lai, W.M.; Lau, S.C. Automated peritoneal dialysis in children and adolescents--benefits: A survey of patients and parents on health-related quality of life. Perit. Dial. Int. 2007, 27, S138–S142. [Google Scholar] [CrossRef]
- Park, K.-S.; Hwang, Y.J.; Cho, M.H.; Ko, C.W.; Ha, I.S.; Kang, H.G.; Cheong, H.I.; Park, Y.S.; Lee, Y.J.; Lee, J.H.; et al. Quality of life in children with end-stage renal disease based on a PedsQL ESRD module. Pediatr. Nephrol. 2012, 27, 2293–2300. [Google Scholar] [CrossRef]
- Rahman, A.; Hasan, A.U.; Kobori, H. Melatonin in chronic kidney disease: A promising chronotherapy targeting the intrarenal renin-angiotensin system. Hypertens. Res. 2019, 42, 920–923. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| CKD 2–4 10 Patients | CKD 5D 13 Patients | KTx 7 Patients | p | |
|---|---|---|---|---|
| Demographic data | ||||
| Age | 11.5 (7–18) | 13 (7–18) | 14 (8–18) | 0.308 |
| Sex (male) | 6 (60%) | 8 (61.5%) | 5 (71.4%) | 0.877 |
| Inherited kidney disease | 6 (60%) | 11 (84.6%) | 6 (85.7%) | 0.312 |
| Residence place (urban) | 7 (70%) | 6 (46.1%) | 4 (57.1%) | 0.520 |
| Parental education level | 0.212 | |||
| Elementary school | 1 (10%) | 5 (38.4%) | 1 (14.2%) | |
| High school | 3 (30%) | 6 (46.2%) | 3 (42.9%) | |
| University Degree | 6 (60%) | 2 (15.4%) | 3 (42.9%) | |
| Fatigue scores | ||||
| General Fatigue | 89.6 (45.8–100) | 62.5 (45.8–100) | 83.3 (58.3–100) | 0.076 |
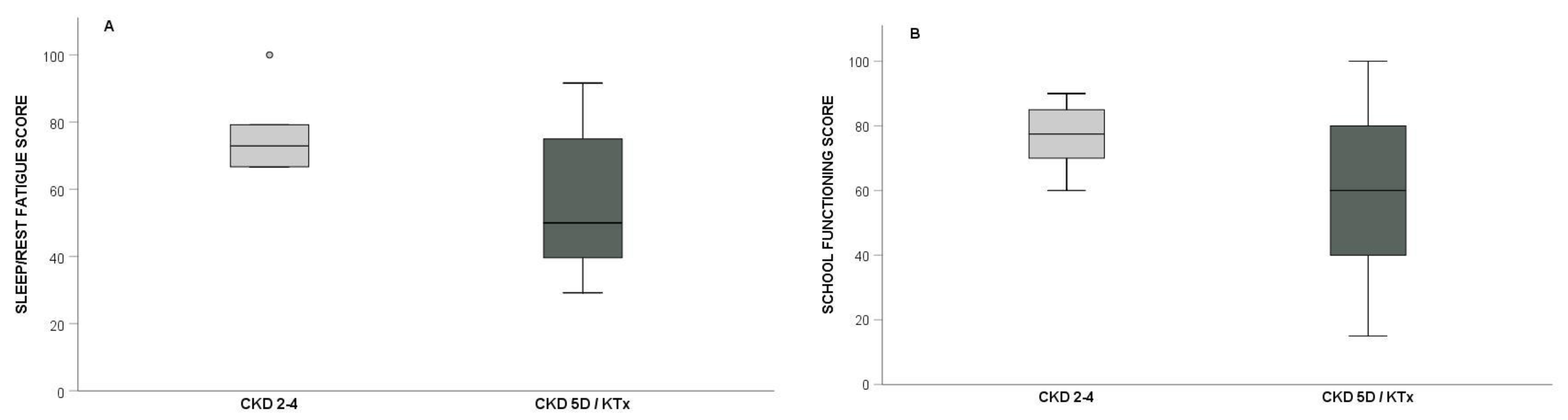
| Sleep/Rest Fatigue | 72.9 (66.6–100) | 50 (29.2–79.2) | 50 (33.3–91.6) | 0.071 |
| Cognitive Fatigue | 83.4 (41.7–100) | 66.7 (25–87.5) | 58.3 (50–100) | 0.215 |
| Total Fatigue | 84.7 (55.5–93.1) | 59.7 (36.1–85.8) | 69.4 (47.2–93) | 0.052 |
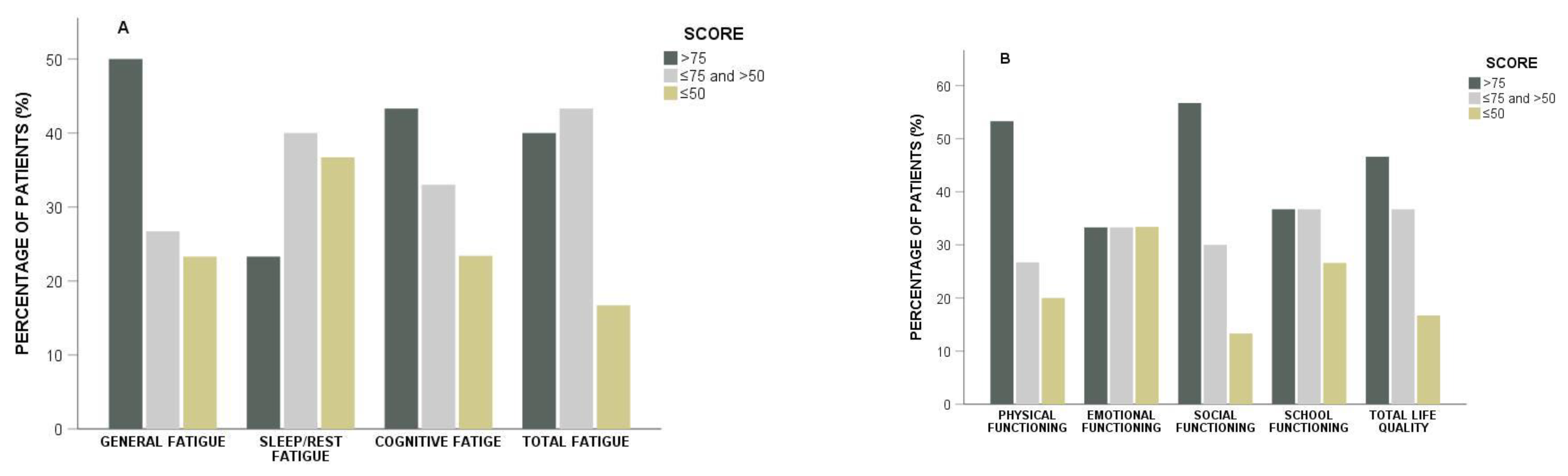
| Low Fatigue scores | ||||
| General Fatigue | 1 (10%) | 6 (46.2%) | 0 (0%) | 0.032 |
| Sleep/Rest Fatigue | 0 (0%) | 7 (53.8%) | 4 (57.1%) | 0.013 |
| Cognitive Fatigue | 1 (10%) | 3 (23.1%) | 3 (42.9%) | 0.289 |
| Total Fatigue | 0 (0%) | 4 (30.8%) | 1 (14.3%) | 0.143 |
| HRQoL scores | ||||
| Physical Functioning | 87.5 (43.75–100) | 75 (28.1–100) | 78.1 (40.6–87.5) | 0.210 |
| Emotional Functioning | 77.5 (30–100) | 55 (20–95) | 65 (25–95) | 0.324 |
| Social Functioning | 82.5 (50–100) | 70 (35–100) | 70 (55–85) | 0.173 |
| School Functioning | 77.5 (60–90) | 60 (17–100) | 60 (15–90) | 0.209 |
| Total HRQoL | 87 (48.9–91.7) | 67.4 (35.9–93.5) | 71.7 (45.7–80.4) | 0.126 |
| Low HRQoL scores | ||||
| Physical Functioning | 1 (10%) | 4 (30.8%) | 1 (14.3%) | 0.425 |
| Emotional Functioning | 2 (20%) | 5 (38.5%) | 3 (42.9%) | 0.538 |
| Social Functioning | 1 (10%) | 3 (23.1%) | 0 (0%) | 0.326 |
| School Functioning | 0 (0%) | 5 (38.5%) | 3 (42.9%) | 0.064 |
| Total HRQoL | 1 (10%) | 3 (23.1%) | 1 (14.3%) | 0.693 |
| Physical Functioning | Emotional Functioning | Social Functioning | School Functioning | Total HRQoL | |
|---|---|---|---|---|---|
| General Fatigue | rs = 0.434, p = 0.017 | rs = 0.409, p = 0.025 | rs = 0.319, p = 0.086 | rs = 0.417, p = 0.019 | rs = 0.504, p = 0.004 |
| Sleep/Rest Fatigue | rs = 0.481, p = 0.007 | rs = 0.302, p = 0.105 | rs = 0.459, p = 0.011 | rs = 0.458, p = 0.011 | rs = 0.503, p = 0.005 |
| Cognitive Fatigue | rs = 0.565, p = 0.001 | rs = 0.455, p = 0.011 | rs = 0.513, p = 0.004 | rs = 0.564, p = 0.001 | rs = 0.654, p < 0.001 |
| Total Fatigue | rs = 0.564, p = 0.001 | rs = 0.414, p = 0.023 | rs = 0.498, p = 0.005 | rs = 0.548, p = 0.002 | rs = 0.625, p < 0.001 |
| Physical Functioning | Emotional Functioning | Social Functioning | School Functioning | Total HRQoL | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| >50 24 pts | ≤50 6 pts | p | >50 20 pts | ≤50 10 pts | p | >50 26 pts | ≤50 4 pts | p | >50 22 pts | ≤50 8 pts | p | >50 25 pts | ≤50 5 pts | p | |
| General Fatigue | 4 (16.7%) | 3 (50%) | 0.120 | 3 (15%) | 4 (40%) | 0.181 | 4 (15.4%) | 3 (75%) | 0.031 | 4 (18.2%) | 3 (37.5%) | 0.345 | 3 (12%) | 4 (80%) | 0.006 |
| Sleep/ Rest Fatigue | 6 (25%) | 5 (83.3%) | 0.016 | 5 (25%) | 6 (60%) | 0.108 | 9 (34.6%) | 2 (50%) | 0.611 | 4 (18.2%) | 7 (87.5%) | 0.001 | 7 (28%) | 4 (80%) | 0.047 |
| Cognitive Fatigue | 4 (16.7%) | 3 (50%) | 0.120 | 3 (15%) | 4 (40%) | 0.181 | 6 (23.1%) | 1 (25%) | 1 | 1 (4.5%) | 6 (75%) | <0.001 | 4 (16%) | 3 (60%) | 0.068 |
| Total Fatigue | 1 (4.2%) | 4 (66.7%) | 0.003 | 1 (5%) | 4 (40%) | 0.031 | 3 (11.5%) | 2 (50%) | 0.119 | 1 (4.5%) | 4 (50%) | 0.011 | 1 (4%) | 4 (80%) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karava, V.; Goutou, S.; Dotis, J.; Kondou, A.; Charela, E.; Dadoudi, O.; Eleftheriadis, T.; Stefanidis, I.; Printza, N. Fatigue and Quality of Life in Children with Chronic Kidney Disease. Children 2022, 9, 1414. https://doi.org/10.3390/children9091414
Karava V, Goutou S, Dotis J, Kondou A, Charela E, Dadoudi O, Eleftheriadis T, Stefanidis I, Printza N. Fatigue and Quality of Life in Children with Chronic Kidney Disease. Children. 2022; 9(9):1414. https://doi.org/10.3390/children9091414
Chicago/Turabian StyleKarava, Vasiliki, Sofia Goutou, John Dotis, Antonia Kondou, Evangelia Charela, Olympia Dadoudi, Theodoros Eleftheriadis, Ioannis Stefanidis, and Nikoleta Printza. 2022. "Fatigue and Quality of Life in Children with Chronic Kidney Disease" Children 9, no. 9: 1414. https://doi.org/10.3390/children9091414