
Postoperative Alanine Aminotransferase Levels Are Associated with Outcomes in Pediatric Patients Undergoing Total Cavopulmonary Connection
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Subjects Stratified by Maximal ALT Value within 48 h Post-TCPC
3.2. Univariate and Multivariate Logistic Analyses of Risk Factors Associated with High ALT Following TCPC Operation
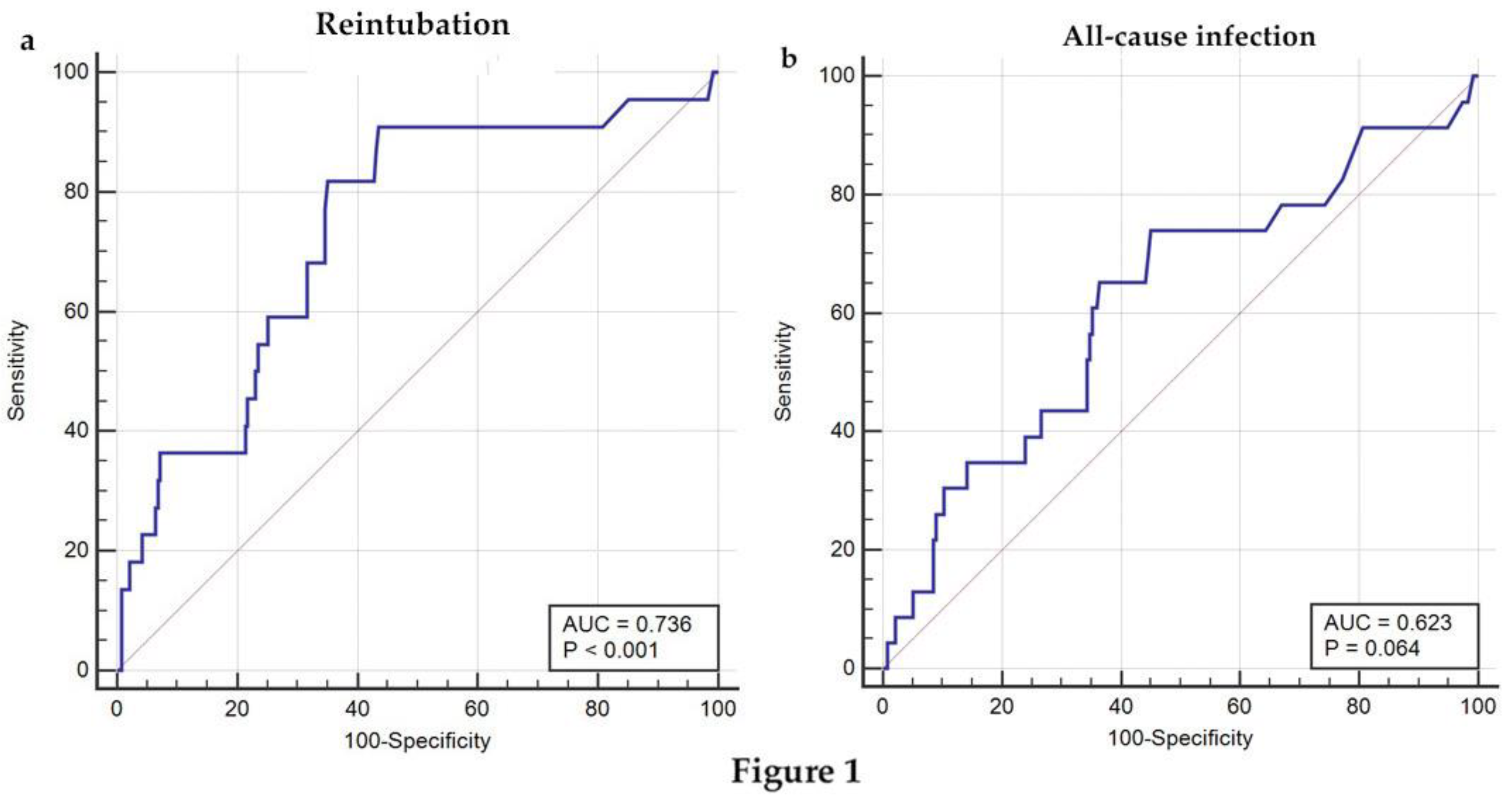
3.3. ROC Analysis of Postoperative ALT in Predicting Reintubation or All-Cause Infection for Pediatric Patients Undergoing TCPC Operation
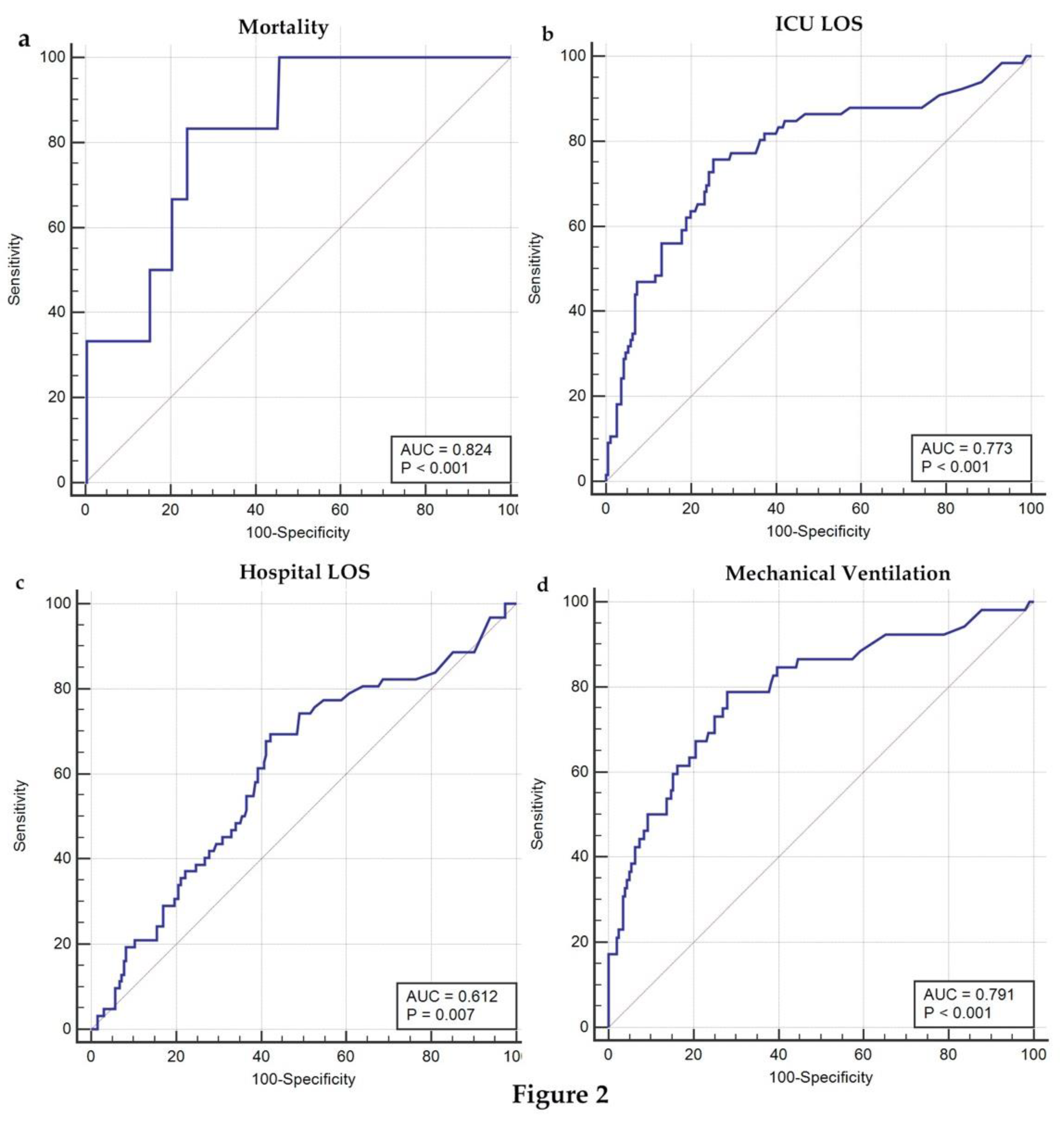
3.4. ROC Analysis of Postoperative ALT in Predicting Clinical Outcomes for Pediatric Patients Undergoing TCPC Operation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoashi, T.; Shimada, M.; Imai, K.; Komori, M.; Kurosaki, K.; Ohuchi, H.; Ichikawa, H. Long-term therapeutic effect of Fontan conversion with an extracardiac conduit. Eur. J. Cardiothorac. Surg. 2020, 57, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Robbers-Visser, D.; Miedema, M.; Nijveld, A.; Boersma, E.; Bogers, A.J.; Haas, F.; Helbing, W.A.; Kapusta, L. Results of staged total cavopulmonary connection for functionally univentricular hearts; comparison of intra-atrial lateral tunnel and extracardiac conduit. Eur. J. Cardiothorac. Surg. 2010, 37, 934–941. [Google Scholar] [CrossRef] [PubMed]
- Ono, M.; Georgiev, S.; Burri, M.; Mayr, B.; Cleuziou, J.; Strbad, M.; Balling, G.; Hager, A.; Horer, J.; Lange, R. Early extubation improves outcome following extracardiac total cavopulmonary connection. Interact. Cardiovasc. Thorac. Surg. 2019, 29, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Hoashi, T.; Shimada, M.; Komori, M.; Nakata, T.; Kurosaki, K.; Ichikawa, H. Long-term Outcomes of Extracardiac Total Cavopulmonary Connection for Apicocaval Juxtaposition. Ann. Thorac. Surg. 2021, 112, 1326–1333. [Google Scholar] [CrossRef]
- Radman, M.; Keller, R.L.; Oishi, P.; Datar, S.A.; Wellnitz, K.; Azakie, A.; Hanley, F.; Char, D.; Hsu, J.H.; Amrinovin, R.; et al. Preoperative B-type natriuretic peptide levels are associated with outcome after total cavopulmonary connection (Fontan). J. Thorac. Cardiovasc. Surg. 2014, 148, 212–219. [Google Scholar] [CrossRef]
- Ono, M.; Kasnar-Samprec, J.; Hager, A.; Cleuziou, J.; Burri, M.; Langenbach, C.; Callegari, A.; Strbad, M.; Vogt, M.; Horer, J.; et al. Clinical outcome following total cavopulmonary connection: A 20-year single-centre experience. Eur. J. Cardiothorac. Surg. 2016, 50, 632–641. [Google Scholar] [CrossRef]
- Senior, J.R. Alanine aminotransferase: A clinical and regulatory tool for detecting liver injury-past, present, and future. Clin. Pharmacol. Ther. 2012, 92, 332–339. [Google Scholar] [CrossRef]
- Deorsola, L.; Aidala, E.; Cascarano, M.T.; Valori, A.; Agnoletti, G.; Pace Napoleone, C. Liver stiffness modifications shortly after total cavopulmonary connection. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 513–518. [Google Scholar] [CrossRef]
- Luo, Q.; Jia, Y.; Su, Z.; Wang, H.; Li, Y.; Wu, X.; Liu, Q.; Liu, X.; Yuan, S.; Yan, F. Persistent Liver Dysfunction in Pediatric Patients After Total Cavopulmonary Connection Surgery. Front. Cardiovasc. Med. 2022, 9, 820791. [Google Scholar] [CrossRef]
- Ono, M.; Beran, E.; Burri, M.; Cleuziou, J.; Pabst von Ohain, J.; Strbad, M.; Rohlig, C.; Hager, A.; Horer, J.; Schreiber, C.; et al. Long-term outcome of preadolescents, adolescents, and adult patients undergoing total cavopulmonary connection. J. Thorac. Cardiovasc. Surg. 2018, 156, 1166–1176.e1164. [Google Scholar] [CrossRef] [Green Version]
- Bekkelund, S.I. Serum alanine aminotransferase activity and risk factors for cardiovascular disease in a Caucasian population: The Tromso study. BMC Cardiovasc. Disord. 2021, 21, 29. [Google Scholar] [CrossRef] [PubMed]
- Maeda, D.; Sakane, K.; Kanzaki, Y.; Okuno, T.; Nomura, H.; Hourai, R.; Akamatsu, K.; Tsuda, K.; Ito, T.; Sohmiya, K.; et al. Relation of Aspartate Aminotransferase to Alanine Aminotransferase Ratio to Nutritional Status and Prognosis in Patients with Acute Heart Failure. Am. J. Cardiol. 2021, 139, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Schmiegelow, M.D.; Idorn, L.; Gislason, G.; Hlatky, M.; Kober, L.; Torp-Pedersen, C.; Sondergaard, L. Cardiovascular complications in patients with total cavopulmonary connection: A nationwide cohort study. Int. J. Cardiol. 2020, 305, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Anigwe, C.; Yogeswaran, V.; Moon-Grady, A.; McAllister, S.; Aggarwal, A.; Blissett, S.; Harris, I.S.; Kouretas, P.C.; Mahadevan, V.S.; Sabanayagam, A.; et al. Outcomes among adult survivors of total cavopulmonary Fontan palliation for single ventricle. Heart 2021, 108, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Ono, M.; Burri, M.; Cleuziou, J.; Pabst von Ohain, J.; Beran, E.; Strbad, M.; Hager, A.; Horer, J.; Schreiber, C.; Lange, R. Impact of early Fontan completion on postoperative outcomes in patients with a functional single ventricle. Eur. J. Cardiothorac. Surg. 2017, 51, 995–1002. [Google Scholar] [CrossRef]
- Ono, M.; Burri, M.; Mayr, B.; Anderl, L.; Cleuziou, J.; Strbad, M.; Hager, A.; Horer, J.; Lange, R. Flow Dynamics of Bilateral Superior Cavopulomonary Shunts Influence Outcomes After Fontan Completion. Pediatr. Cardiol. 2020, 41, 816–826. [Google Scholar] [CrossRef]
- Vitanova, K.; Shiraishi, S.; Mayr, B.; Beran, E.; Cleuziou, J.; Strbad, M.; Rohlig, C.; Hager, A.; Horer, J.; Lange, R.; et al. Impact of Characteristics at Stage-2-Palliation on Outcome Following Fontan Completion. Pediatr. Cardiol. 2019, 40, 1476–1487. [Google Scholar] [CrossRef]
- Odenwald, T.; Quail, M.A.; Giardini, A.; Khambadkone, S.; Hughes, M.; Tann, O.; Hsia, T.Y.; Muthurangu, V.; Taylor, A.M. Systemic to pulmonary collateral blood flow influences early outcomes following the total cavopulmonary connection. Heart 2012, 98, 934–940. [Google Scholar] [CrossRef]
- Liu, Z.; Que, S.; Xu, J.; Peng, T. Alanine aminotransferase-old biomarker and new concept: A review. Int. J. Med. Sci. 2014, 11, 925–935. [Google Scholar] [CrossRef]
- Varma, A.; Trudeau, S.; Zhou, Y.; Jafri, S.M.; Krajenta, R.; Lamerato, L.; Brown, K.; Luzzi, V.; Lu, M.; Gordon, S.C. African Americans Demonstrate Significantly Lower Serum Alanine Aminotransferase Compared to Non-African Americans. J. Racial. Ethn. Health Disparities 2021, 8, 1533–1538. [Google Scholar] [CrossRef]
- Chung, S.M.; Moon, J.S.; Yoon, J.S.; Won, K.C.; Lee, H.W. Low alanine aminotransferase levels predict low muscle strength in older patients with diabetes: A nationwide cross-sectional study in Korea. Geriatr. Gerontol. Int. 2020, 20, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zeng, Q.; Xue, N.; Wu, M.; Liang, Y.; Xu, Q.; Feng, L.; Xing, S.; Chen, S. A Nomogram Based on Aspartate Aminotransferase/Alanine Aminotransferase (AST/ALT) Ratio to Predict Prognosis After Surgery in Gastric Cancer Patients. Cancer Control 2020, 27, 1073274820954458. [Google Scholar] [CrossRef] [PubMed]
- Gultekin, Y.; Bolat, A.; Hatice, K.; Tekeli Kunt, A. Does Aspartate Aminotransferase to Alanine Aminotransferase Ratio Predict Acute Kidney Injury After Cardiac Surgery? Heart Surg. Forum. 2021, 24, E506–E511. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Normal-ALT Group (n = 134) | High-ALT Group (n = 122) | p-Value |
|---|---|---|---|
| Male (%) | 88 (65.7%) | 87 (71.3%) | 0.404 |
| Female (%) | 46 (34.3%) | 35 (28.7%) | 0.404 |
| Age (years) | 4.7 [3.7; 7.7] | 6.3 [3.9; 11.8] | 0.019 * |
| Height (cm) | 105.0 [97.0; 122.0] | 109.5 [97.0; 143.0] | 0.179 |
| Weight (kg) | 16.0 [14.0; 20.0] | 17.0 [14.0; 32.0] | 0.085 |
| Preoperative WBC (10⁹/L) | 7.9 [6.6; 9.3] | 7.9 [6.4; 10.0] | 0.809 |
| Preoperative hemoglobin (g/L) | 165.0 [154.0; 180.0] | 167.0 [154.0; 183.0] | 0.497 |
| Preoperative platelet (10⁹/L) | 253.0 [208.0; 316.0] | 233.0 [189.0; 301.0] | 0.067 |
| Preoperative creatinine (μmol/L) | 33.0 [26.9; 44.0] | 37.0 [30.0; 50.0] | 0.018 * |
| Preoperative ALT (U/L) | 15.0 [12.0; 19.0] | 15.5 [13.0; 19.0] | 0.536 |
| Preoperative total bilirubin (μmol/L) | 13.0 [9.2; 16.9] | 12.8 [10.3; 17.8] | 0.528 |
| Preoperative direct bilirubin (μmol/L) | 3.7 [2.7; 4.8] | 4.3 [3.0; 5.8] | 0.035 * |
| Preoperative fibrinogen (mg/dL) | 2.6 [2.3; 3.2] | 2.7 [2.4; 3.3] | 0.059 |
| Cardiopulmonary bypass time (h) | 118.5 [88.0; 142.0] | 123.5 [91.0; 163.0] | 0.099 |
| Aortic cross clamp time (h) | 47.0 [0.0; 67.0] | 48.5 [0.0; 84.0] | 0.516 |
| Transfusion of RBC (U) | 2.0 [1.0; 3.0] | 3.0 [2.0; 6.0] | <0.001 ** |
| eTCPC (%) | 49 (36.6%) | 47 (38.5%) | 0.846 |
| TCPC fenestration (%) | 17 (12.7%) | 21 (17.2%) | 0.4 |
| Maximal ALT within 48 h post-TCPC (U/L) | 20.0 [16.0; 25.0] | 379.0 [125.0; 1749.0] | <0.001 ** |
| Circulatory fluid load 24 h post-TCPC (mL) | 104.8 [–91.0; 397.3] | 495.5 [20.0; 1170.0] | <0.001 ** |
| Vasoactive inotropic score 24 h post-TCPC | 5.0 [4.0; 8.0] | 8.0 [5.0;15.0] | <0.001 ** |
| Postoperative diastolic arterial pressure within 1 h post-TCPC (mmHg) | 58.0 [50.0; 65.0] | 55.5 [49.0; 62.0] | 0.251 |
| Postoperative ICVP 1 h post-TCPC (mmHg) | 16.0 [13.0; 18.5] | 17.0 [15.0; 20.0] | 0.005 ** |
| Postoperative Hospital LOS (d) | 14.0 [11.0; 22.0] | 22.0 [16.0; 35.0] | <0.001 ** |
| Postoperative mechanical ventilation (h) | 5.0 [4.0; 8.0] | 16.0 [6.0; 80.0] | <0.001 ** |
| Postoperative ICU LOS (d) | 44.0 [24.0; 86.0] | 109.0 [46.0; 165.0] | <0.001 ** |
| Postoperative mortality (%) | 0 (0.0%) | 6 (4.9%) | 0.029 * |
| Postoperative all-cause infection (%) | 6 (4.5%) | 17 (13.9%) | 0.015 * |
| Postoperative reintubation (%) | 2 (1.5%) | 20 (16.4%) | <0.001 ** |
| Variables | Univariate Analyses | Multivariate Analyses | ||||
|---|---|---|---|---|---|---|
| Crude OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value | |
| Hospital LOS | 2.992 | 1.635–5.477 | <0.001 ** | 3.235 | 1.606–6.516 | 0.001 ** |
| Mechanical ventilation | 7.56 | 3.494–16.355 | <0.001 ** | 2.879 | 1.143–7.253 | 0.025 * |
| ICU LOS | 7.149 | 3.641–14.039 | <0.001 ** | 4.911 | 2.223–10.849 | <0.001 ** |
| Reintubation | 12.941 | 2.957–56.642 | 0.001 ** | 11.317 | 2.339–54.758 | 0.003 ** |
| All-cause infection | 3.454 | 1.315–9.078 | 0.012 * | 2.393 | 0.789–7.255 | 0.123 |
| AUC | Cutoff Point | Sensitivity | Specificity | 95% CI | Z Statistic | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Mechanical ventilation | 0.791 | 76 | 78.85 | 72.06 | 0.736–0.839 | 7.667 | <0.0001 | 1.606–6.516 |
| ICU LOS | 0.773 | 76 | 75.76 | 74.74 | 0.717–0.823 | 7.476 | <0.0001 | 1.143–7.253 |
| Hospital LOS | 0.612 | 37 | 69.35 | 57.73 | 0.550–0.672 | 2.702 | 0.0069 | 2.223–10.849 |
| Reintubation | 0.623 | 40 | 73.91 | 54.94 | 0.560–0.682 | 1.852 | 0.0641 | 2.339–54.758 |
| All-cause infection | 0.736 | 40 | 90.91 | 56.41 | 0.678–0.789 | 4.174 | <0.0001 | 0.789–7.255 |
| Mortality | 0.824 | 305 | 83.33 | 76 | 0.771–0.868 | 4.588 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Wang, H.; Luo, D.; Zhang, C. Postoperative Alanine Aminotransferase Levels Are Associated with Outcomes in Pediatric Patients Undergoing Total Cavopulmonary Connection. Children 2022, 9, 1410. https://doi.org/10.3390/children9091410
Chen S, Wang H, Luo D, Zhang C. Postoperative Alanine Aminotransferase Levels Are Associated with Outcomes in Pediatric Patients Undergoing Total Cavopulmonary Connection. Children. 2022; 9(9):1410. https://doi.org/10.3390/children9091410
Chicago/Turabian StyleChen, Siyao, Han Wang, Dandong Luo, and Chongjian Zhang. 2022. "Postoperative Alanine Aminotransferase Levels Are Associated with Outcomes in Pediatric Patients Undergoing Total Cavopulmonary Connection" Children 9, no. 9: 1410. https://doi.org/10.3390/children9091410