
Self-Perceived Physical Level and Fitness Performance in Children and Adolescents with Inflammatory Bowel Disease
 , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Methods
2.2.1. Anthropometric Features
2.2.2. Inflammatory Bowel Disease Definition and Disease Activity Scores
Disease Definition
Disease Activity Scores
2.2.3. The Physical Activity Questionnaire for Older Children (PAQ-C)
2.2.4. The International Fitness Enjoyment Scale (IFIS)
3. Statistical Analysis
4. Results
4.1. IBD Patients and Controls
4.2. Group of IBD and Severity Disease
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Däbritz, J.; Gerner, P.; Enninger, A.; Claßen, M.; Radke, M. Inflammatory Bowel Disease in Childhood and Adolescence. Dtsch. Arztebl. Int. 2017, 114, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Rosen, M.J.; Dhawan, A.; Saeed, S.A. Inflammatory Bowel Disease in Children and Adolescents. JAMA Pediatrics 2015, 169, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Yorulmaz, E.; Adali, G.; Yorulmaz, H.; Ulasoglu, C.; Tasan, G.; Tuncer, I. Metabolic syndrome frequency in inflammatory bowel diseases. Saudi J. Gastroenterol. 2011, 17, 376–382. [Google Scholar] [CrossRef]
- Hyun, C.K. Molecular and Pathophysiological Links between Metabolic Disorders and Inflammatory Bowel Diseases. Int. J. Mol. Sci. 2021, 22, 9139. [Google Scholar] [CrossRef]
- Lechuga, S.; Ivanov, A.I. Disruption of the epithelial barrier during intestinal inflammation: Quest for new molecules and mechanisms. Biochim. Biophys. Acta. Mol. Cell Res. 2017, 1864, 1183–1194. [Google Scholar] [CrossRef]
- Vancamelbeke, M.; Vermeire, S. The intestinal barrier: A fundamental role in health and disease. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 821–834. [Google Scholar] [CrossRef]
- Singer, K.; Lumeng, C.N. The initiation of metabolic inflammation in childhood obesity. J. Clin. Investig. 2017, 127, 65–73. [Google Scholar] [CrossRef]
- Calcaterra, V.; Regalbuto, C.; Porri, D.; Pelizzo, G.; Mazzon, E.; Vinci, F.; Zuccotti, G.; Fabiano, V.; Cena, H. Inflammation in Obesity-Related Complications in Children: The Protective Effect of Diet and Its Potential Role as a Therapeutic Agent. Biomolecules 2020, 10, 1324. [Google Scholar] [CrossRef]
- Calcaterra, V.; Vandoni, M.; Rossi, V.; Berardo, C.; Grazi, R.; Cordaro, E.; Tranfaglia, V.; Carnevale Pellino, V.; Cereda, C.; Zuccotti, G. Use of Physical Activity and Exercise to Reduce Inflammation in Children and Adolescents with Obesity. Int. J. Environ. Res. Public Health 2022, 19, 6908. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour for Children and Adolescents, Adults and Older Adults. Available online: https://www.who.int/docs/default-source/physical-activity/call-for-consultation/draft-guideline-on-physical-activity-and-sedentray-behaviour.pdf?sfvrsn=ddf523d5_4 (accessed on 8 July 2022).
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A Developmental Perspective on the Role of Motor Skill Competence in Physical Activity: An Emergent Relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Mählmann, L.; Gerber, M.; Furlano, R.I.; Legeret, C.; Kalak, N.; Holsboer-Trachsler, E.; Brand, S. Psychological wellbeing and physical activity in children and adolescents with inflammatory bowel disease compared to healthy controls. BMC Gastroenterol. 2017, 17, 160. [Google Scholar] [CrossRef] [PubMed]
- Bourdier, P.; Saidi, O.; Rochette, E.; Ratel, S.; Merlin, E.; Pereira, B.; Duché, P. Physical activity and sedentary levels in children with juvenile idiopathic arthritis and inflammatory bowel disease. A systematic review and meta-analysis. Pediatric Res. 2019, 86, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Ploeger, H.E.; Takken, T.; Wilk, B.; Issenman, R.M.; Sears, R.; Suri, S.; Timmons, B.W. Exercise capacity in pediatric patients with inflammatory bowel disease. J. Pediatrics 2011, 158, 814–819. [Google Scholar] [CrossRef] [PubMed]
- Werkstetter, K.J.; Ullrich, J.; Schatz, S.B.; Prell, C.; Koletzko, B.; Koletzko, S. Lean body mass, physical activity and quality of life in paediatric patients with inflammatory bowel disease and in healthy controls. J. Crohn’s Colitis 2012, 6, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Gatti, A.; Pugliese, L.; Carnevale Pellino, V.; Del Bianco, M.; Vandoni, M.; Lovecchio, N. Self-Declared Physical Activity Levels and Self-Reported Physical Fitness in a Sample of Italian Adolescents during the COVID-19 Pandemic. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 655–665. [Google Scholar] [CrossRef]
- Calcaterra, V.; Winickoff, J.P.; Klersy, C.; Schiano, L.M.; Bazzano, R.; Montalbano, C.; Musella, V.; Regalbuto, C.; Larizza, D.; Cena, H. Smoke exposure and cardio-metabolic profile in youth with type 1 diabetes. Diabetol. Metab. Syndr. 2018, 10, 53. [Google Scholar] [CrossRef]
- Calcaterra, V.; De Giuseppe, R.; Biino, G.; Mantelli, M.; Marchini, S.; Bendotti, G.; Madè, A.; Avanzini, M.A.; Montalbano, C.; Cossellu, G.; et al. Relation between circulating oxidized-LDL and metabolic syndrome in children with obesity: The role of hypertriglyceridemic waist phenotype. J. Pediatric Endocrinol. Metab. JPEM 2017, 30, 1257–1263. [Google Scholar] [CrossRef]
- WHO. Child Growth Standards. World Health Organization. Available online: https://www.who.int/tools/child-growth-standards (accessed on 20 July 2022).
- Hyams, J.S.; Ferry, G.D.; Mandel, F.S.; Gryboski, J.D.; Kibort, P.M.; Kirschner, B.S.; Griffiths, A.M.; Katz, A.J.; Grand, R.J.; Boyle, J.T. Development and validation of a pediatric Crohn’s disease activity index. J. Pediatric Gastroenterol. Nutr. 1991, 12, 439–447. [Google Scholar] [CrossRef]
- Loonen, H.J.; Griffiths, A.M.; Merkus, M.P.; Derkx, H.H. A critical assessment of items on the Pediatric Crohn’s Disease Activity Index. J. Pediatric Gastroenterol. Nutr. 2003, 36, 90–95. [Google Scholar] [CrossRef]
- Hyams, J.; Markowitz, J.; Otley, A.; Rosh, J.; Mack, D.; Bousvaros, A.; Kugathasan, S.; Pfefferkorn, M.; Tolia, V.; Evans, J.; et al. Evaluation of the pediatric crohn disease activity index: A prospective multicenter experience. J. Pediatric Gastroenterol. Nutr. 2005, 41, 416–421. [Google Scholar] [CrossRef]
- Turner, D.; Otley, A.R.; Mack, D.; Hyams, J.; de Bruijne, J.; Uusoue, K.; Walters, T.D.; Zachos, M.; Mamula, P.; Beaton, D.E.; et al. Development, validation, and evaluation of a pediatric ulcerative colitis activity index: A prospective multicenter study. Gastroenterology 2007, 133, 423–432. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Hyams, J.; Markowitz, J.; Lerer, T.; Mack, D.R.; Evans, J.; Pfefferkorn, M.; Rosh, J.; Kay, M.; Crandall, W.; et al. Appraisal of the pediatric ulcerative colitis activity index (PUCAI). Inflamm. Bowel Dis. 2009, 15, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Physician Global Assessment: ImproveCareNow. Available online: https://d3n8a8pro7vhmx.cloudfront.net/improvecarenow/pages/283/attachments/original/1456525231/PGA_Clinical_Guidelines.pdf?1456525231 (accessed on 20 July 2022).
- Benítez-Porres, J.; López-Fernández, I.; Raya, J.F.; Álvarez Carnero, S.; Alvero-Cruz, J.R.; Álvarez Carnero, E. Reliability and Validity of the PAQ-C Questionnaire to Assess Physical Activity in Children. J. Sch. Health 2016, 86, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Sánchez-López, M.; Solera-Martínez, M.; Fernández-Sánchez, A.; Sjöström, M.; Martínez-Vizcaino, V. Self-reported and measured cardiorespiratory fitness similarly predict cardiovascular disease risk in young adults. Scand. J. Med. Sci. Sports 2013, 23, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Tomporowski, P.D.; Lambourne, K.; Okumura, M.S. Physical activity interventions and children’s mental function: An introduction and overview. Prev. Med. 2011, 52 (Suppl. S1), S3–S9. [Google Scholar] [CrossRef]
- Fanjiang, G.; Kleinman, R.E. Nutrition and performance in children. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 342–347. [Google Scholar] [CrossRef]
- Marchioni Beery, R.M.; Li, E.; Fishman, L.N. Impact of pediatric inflammatory bowel disease diagnosis on exercise and sports participation: Patient and parent perspectives. World J. Gastroenterol. 2019, 25, 4493–4501. [Google Scholar] [CrossRef]
- Godin, J.P.; Martin, F.P.; Breton, I.; Schoepfer, A.; Nydegger, A. Total and activity-induced energy expenditure measured during a year in children with inflammatory bowel disease in clinical remission remain lower than in healthy controls. Clin. Nutr. (Edinb. Scotl.) 2020, 39, 3147–3152. [Google Scholar] [CrossRef]
- Greenley, R.N.; Naftaly, J.P.; Walker, R.J.; Kappelman, M.D.; Martin, C.F.; Schneider, K.L. Sports Participation in Youth with Inflammatory Bowel Diseases: The Role of Disease Activity and Subjective Physical Health Symptoms. Inflamm. Bowel Dis. 2018, 24, 247–253. [Google Scholar] [CrossRef]
- Legeret, C.; Mählmann, L.; Gerber, M.; Kalak, N.; Köhler, H.; Holsboer-Trachsler, E.; Brand, S.; Furlano, R. Favorable impact of long-term exercise on disease symptoms in pediatric patients with inflammatory bowel disease. BMC Pediatrics 2019, 19, 297. [Google Scholar] [CrossRef] [Green Version]
- Kuloglu, Z.; Çetin, F.; Urgancı, N.; Önal, Z.; Sarı, S.; Yüksekkaya, H.; Çaltepe, G.; Kutluk, G.; Dumlupinar, E. Turkish Inflammatory Bowel Disease Study Group. Nutritional characteristic of children with inflammatory bowel disease in the nationwide inflammatory bowel disease registry from the Mediterranean region. Eur. J. Clin. Nutr. 2022, 76, 1289–1296. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Escher, J.; Hébuterne, X.; Kłęk, S.; Krznaric, Z.; Schneider, S.; Shamir, R.; Stardelova, K.; Wierdsma, N.; Wiskin, A.E.; et al. Guía ESPEN: Nutrición clínica en la enfermedad inflamatoria intestinal [ESPEN guideline: Clinical nutrition in inflammatory bowel disease]. Nutr. Hosp. 2022, 39, 678–703. [Google Scholar] [PubMed]
- Lamers, C.R.; de Roos, N.M.; Heerink, H.H.; van de Worp-Kalter, L.A.; Witteman, B. Lower Impact of Disease on Daily Life and Less Fatigue in Patients With Inflammatory Bowel Disease Following a Lifestyle Intervention. Inflamm. Bowel Dis. 2022. advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Nhantumbo, L.; Ribeiro Maia, J.A.; dos Santos, F.K.; Jani, I.V.; Gudo, E.S.; Katzmarzyk, P.T.; Prista, A. Nutritional status and its association with physical fitness, physical activity and parasitological indicators in youths from rural Mozambique. Am. J. Hum. Biol. 2013, 25, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Ruiz, M.E.; Peredo-Escárcega, A.E.; Cano-Martínez, A.; Guarner-Lans, V. An Evolutionary Perspective of Nutrition and Inflammation as Mechanisms of Cardiovascular Disease. Int. J. Evol. Biol. 2015, 2015, 179791. [Google Scholar] [CrossRef]
- Babaei, P.; Hoseini, R. Exercise training modulates adipokine dysregulations in metabolic syndrome. Sports Med. Health Sci. 2022, 4, 18–28. [Google Scholar] [CrossRef]
- Yu, S.; Sun, Y.; Shao, X.; Zhou, Y.; Yu, Y.; Kuai, X.; Zhou, C. Leaky Gut in IBD: Intestinal Barrier-Gut Microbiota Interaction. J. Microbiol. Biotechnol. 2022, 32, 825–834. [Google Scholar] [CrossRef]
- Li, Q.; Zhou, S.; Wang, Y.; Cong, J. Changes of intestinal microbiota and microbiota-based treatments in IBD. Arch. Microbiol. 2022, 204, 442. [Google Scholar] [CrossRef]
- Pu, D.; Zhang, Z.; Feng, B. Alterations and Potential Applications of Gut Microbiota in Biological Therapy for Inflammatory Bowel Diseases. Front. Pharmacol. 2022, 13, 906419. [Google Scholar] [CrossRef]
- Clauss, M.; Gérard, P.; Mosca, A.; Leclerc, M. Interplay Between Exercise and Gut Microbiome in the Context of Human Health and Performance. Front. Nutr. 2021, 8, 637010. [Google Scholar] [CrossRef]
- Sigurdsson, G.V.; Schmidt, S.; Mellström, D.; Ohlsson, C.; Karlsson, M.; Lorentzon, M.; Saalman, R. Physical exercise is associated with beneficial bone mineral density and body composition in young adults with childhood-onset inflammatory bowel disease. Scand. J. Gastroenterol. 2021, 56, 699–707. [Google Scholar] [CrossRef]
- Vandoni, M.; Carnevale Pellino, V.; Gatti, A.; Lucini, D.; Mannarino, S.; Larizza, C.; Rossi, V.; Tranfaglia, V.; Pirazzi, A.; Biino, V.; et al. Effects of an Online Supervised Exercise Training in Children with Obesity during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 9421. [Google Scholar] [CrossRef] [PubMed]
- Vandoni, M.; Codella, R.; Pippi, R.; Carnevale Pellino, V.; Lovecchio, N.; Marin, L.; Silvestri, D.; Gatti, A.; Magenes, V.C.; Regalbuto, C.; et al. Combatting Sedentary Behaviors by Delivering Remote Physical Exercise in Children and Adolescents with Obesity in the COVID-19 Era: A Narrative Review. Nutrients 2021, 13, 4459. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Verduci, E.; Vandoni, M.; Rossi, V.; Di Profio, E.; Carnevale Pellino, V.; Tranfaglia, V.; Pascuzzi, M.C.; Borsani, B.; Bosetti, A.; et al. Telehealth: A Useful Tool for the Management of Nutrition and Exercise Programs in Pediatric Obesity in the COVID-19 Era. Nutrients 2021, 13, 3689. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| IBD Patientsn = 54 | Controlsn = 70 | p | Adjusted p* | |
|---|---|---|---|---|
| Age (years) mean (sd) | 14.6 ± 2.2 | 13.5 ± 2.2 | 0.68 | |
| Sex (M) N(%) | 22 (40.7) | 22 (32.3) | 0.34 | |
| Weight (kg) mean (sd) | 55.9 (15.4) | 45.9 (10.1) | <0.001 | na |
| Height (cm) mean (sd) | 150 (13) | 156 (11) | 0.12 | na |
| BMI (kg/m2) mean (sd) | 21.6 (4.3) | 18.7 (3.4) | <0.001 | na |
| BMI z-score median (IQR) | 0.29 (−0.91–1.04) | −0.75 (−1.3–0.06) | 0.002 | na |
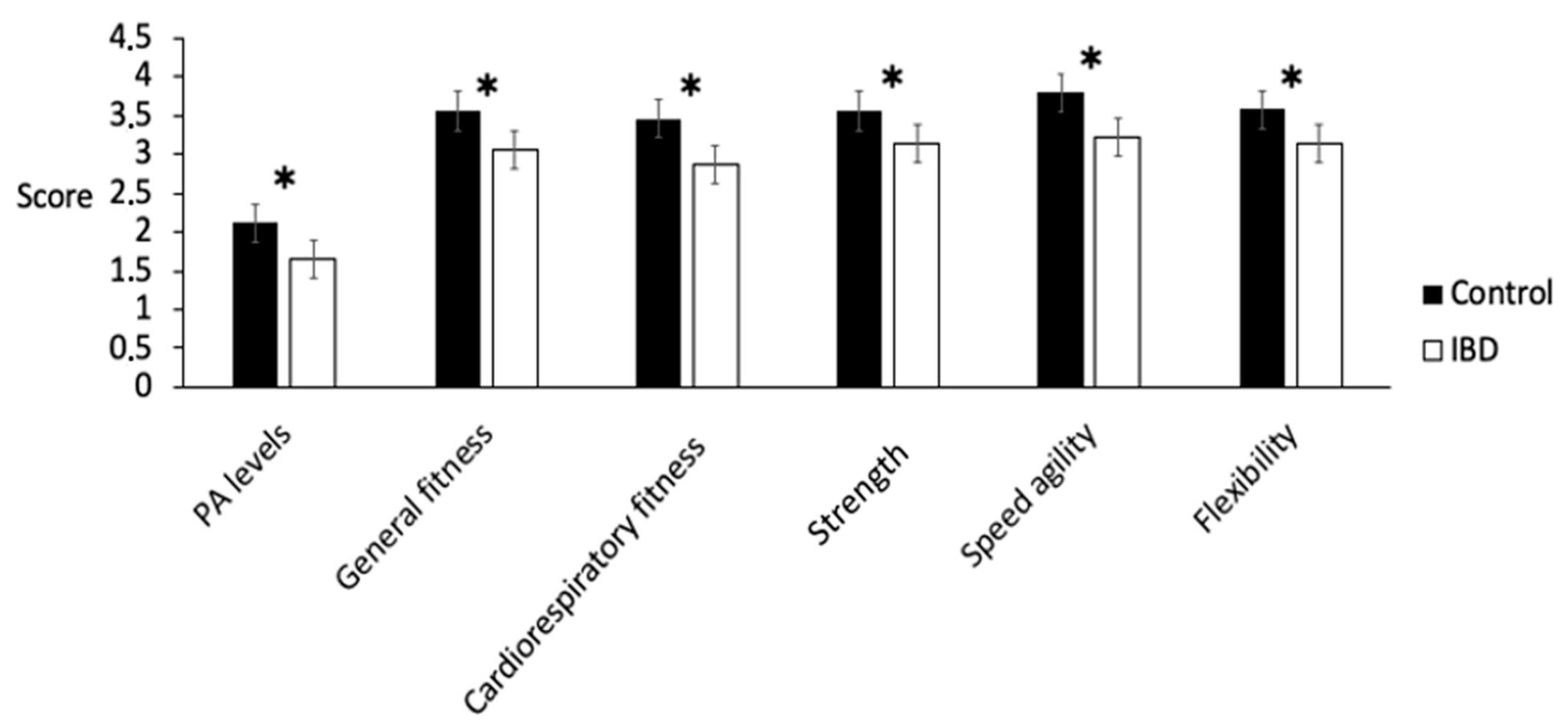
| Physical activity level mean (sd) | 1.50 (0.34) | 2.06 (0.42) | <0.001 | <0.001 |
| General fitness mean (sd) | 3.05 (1.00) | 3.55 (0.88) | 0.003 | 0.13 |
| Cardiorespiratory fitness mean (sd) | 2.87 (1.10) | 3.46 (1.00) | 0.002 | 0.026 |
| Strength mean (sd) | 3.14 (1.05) | 3.55 (0.85) | 0.01 | 0.043 |
| Speed agility mean (sd) | 3.20 (1.20) | 3.78 (0.99) | 0.003 | 0.31 |
| Flexibility mean (sd) | 3.12 (1.01) | 3.57 (1.03) | 0.01 | 0.26 |
| PA Levels | General Fitness | Cardiorespiratory Fitness | Strength | Speed Agility | Flexibility | |
|---|---|---|---|---|---|---|
| PGA | ||||||
| 1 | 1.57 (0.35) | 2.96 (0.95) | 3.0 (1.06) | 3.15 (1.12) | 3.24 (1.14) | 3.12(0.89) |
| 2 | 1.45 (0.30) | 3.53 (1.05) | 2.84 (1.21) | 3.15 (1.14) | 3.30 (1.49) | 3 (1.29) |
| 3 | 1.33 (0.24) | 2.62 (0.91) | 2.37 (1.06) | 3.12 (0.64) | 2.87 (0.99) | 3.37 (1.06) |
| Total | 1.50 (0.33) | 3.05 (0.99) | 2.87 (01.09) | 3.14 (1.05) | 3.20 (1.20) | 3.12(1.01) |
| PUCAI/PCDAI | ||||||
| inactive disease/remission | 1.54 (0.33) | 3.0 (0.98) | 2.90 (1.16) | 3.14 (1.13) | 3.23 (1.20) | 3.07 (0.99) |
| mild/moderate | 1.37 (0.32) | 3.25 (1.05) | 2.75 (0.86) | 3.16 (0.71) | 3.08 (1.24) | 3.33 (1.07) |
| Total | 1.50 (0.33) | 3.05 (0.99) | 2.87 (1.09) | 3.14 (1.05) | 3.20 (1.20) | 3.12 (1.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penagini, F.; Calcaterra, V.; Dilillo, D.; Vandoni, M.; Gianolio, L.; Gatti, A.; Rendo, G.; Giuriato, M.; Cococcioni, L.; De Silvestri, A.; et al. Self-Perceived Physical Level and Fitness Performance in Children and Adolescents with Inflammatory Bowel Disease. Children 2022, 9, 1399. https://doi.org/10.3390/children9091399
Penagini F, Calcaterra V, Dilillo D, Vandoni M, Gianolio L, Gatti A, Rendo G, Giuriato M, Cococcioni L, De Silvestri A, et al. Self-Perceived Physical Level and Fitness Performance in Children and Adolescents with Inflammatory Bowel Disease. Children. 2022; 9(9):1399. https://doi.org/10.3390/children9091399
Chicago/Turabian StylePenagini, Francesca, Valeria Calcaterra, Dario Dilillo, Matteo Vandoni, Laura Gianolio, Alessandro Gatti, Giulia Rendo, Matteo Giuriato, Lucia Cococcioni, Annalisa De Silvestri, and et al. 2022. "Self-Perceived Physical Level and Fitness Performance in Children and Adolescents with Inflammatory Bowel Disease" Children 9, no. 9: 1399. https://doi.org/10.3390/children9091399