
Long-Term Observational Outcomes after Total Correction of Congenital Heart Disease in Korean Patients with Down Syndrome: A National Cohort Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Collection
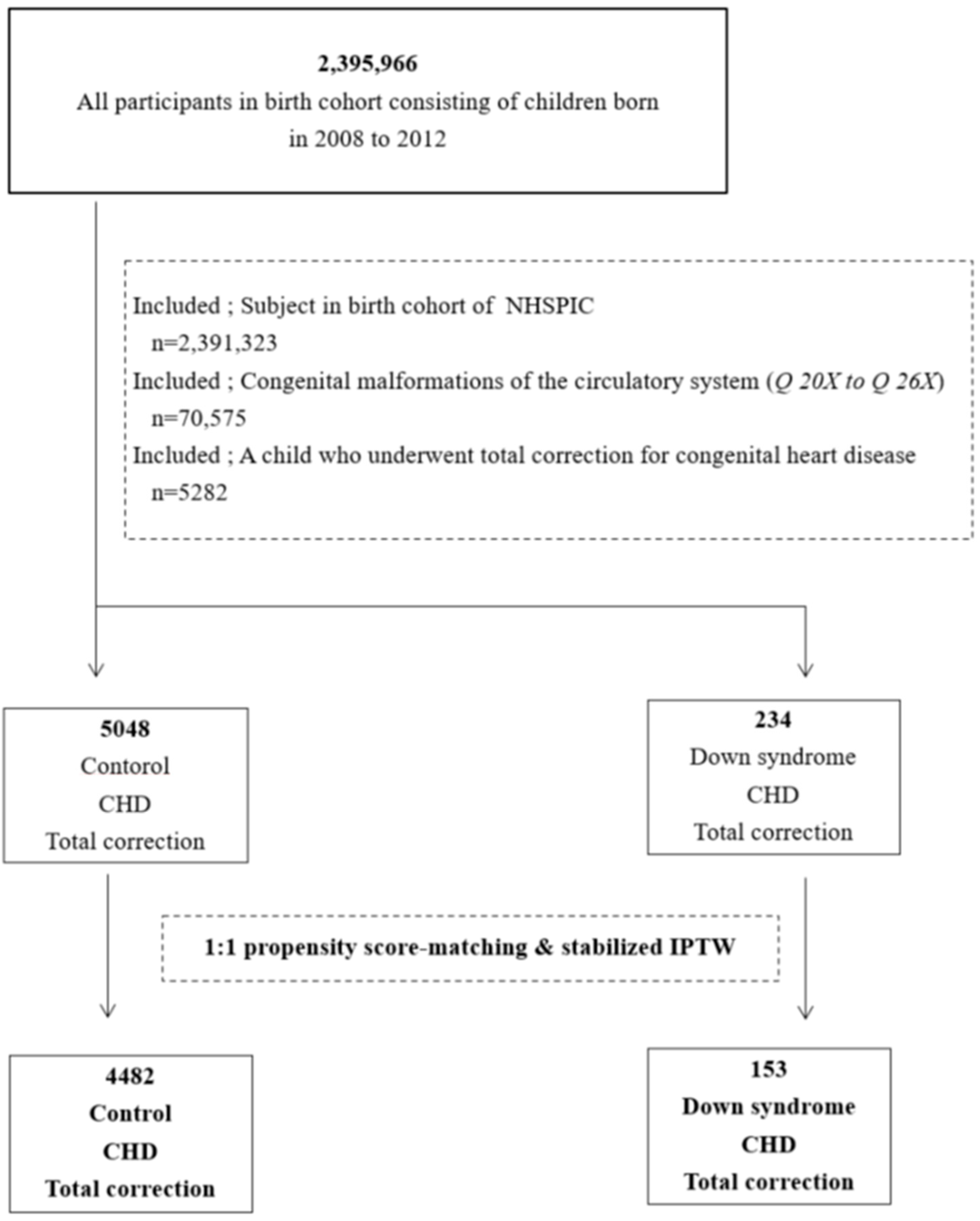
2.2. Study Population
2.3. Definition of Down Syndrome and Congenital Heart Disease
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Participants
3.2. Preoperative Distribution of Congenital Heart Disease
3.3. Type of Cardiac Surgery and Age (Table 3)

{kind=link}
{kind=link}
| Surgery | Controls (N = 5048) | Down Syndrome (N = 234) | p-Value |
|---|---|---|---|
| N Based on Surgery Type, n | |||
| Total correction | 4521 | 217 | 0.118 |
| Total correction after palliation | 527 | 17 | 0.118 |
| Age at Surgery, months(IQR) a | |||
| Total correction | 4 (1–9) | 4 (2–7) | 0.575 |
| Total correction after palliation | 9 (3–26) | 7 (6–12) | 0.458 |
| Palliation | 1 (0–3) | 1 (0–2) | 0.501 |
3.4. Postoperative Mortality and Surgical Outcomes (Table 4)
| Observed Data (N = 5282) | Propensity-Matched Data (N = 4635) | Modified Poisson | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Control | Down Syndrome | p-Value | Control | Down Syndrome | p-Value | Risk Ratio | (95% CI) | p-Value | |
| Mortality | |||||||||
| In-hospital mortality (<30 days after operation) * | 91 (1.8) | 7 (2.9) | 0.18 | 4 (0.0) | 1 (0.6) | 0.454 | 3.1 | (0.1–70.6) | 0.477 |
| Late mortality (≥30 days after operation) * | 184 (3.6) | 19 (8.1) | 0.000 | 40 (0.8) | 6 (3.9) | 0.000 | 4.4 | (1.8–10.3) | 0.000 |
| Cardiac complication | |||||||||
| Heart failure a,* | 901 (17.8) | 48 (20.5) | 0.299 | 795 (17.7) | 30 (19.6) | 0.641 | 1.0 | (0.7–1.5) | 0.672 |
| Pulmonary hypertension b,* | 355 (7.0) | 63 (26.9) | <0.001 | 296 (6.6) | 37 (24.1) | <0.000 | 3.6 | (2.5–5.1) | <0.0001 |
| Arrhythmias c,* | 672 (13.3) | 25 (10.6) | 0.245 | 549 (12.2) | 16 (10.4) | 0.425 | 0.8 | (0.4–1.3) | 0.455 |
| Clinical course | |||||||||
| Length of hospitalization d (at total correction) g | 11 (6–19) | 14 (10–25) | <0.001 | 11 (8–18) | 15 (10–23) | 0.000 | 1.2 | (1.2–1.2) | <0.0001 |
| Number of emergency room visits e,g | 2 (1–4) | 2 (1–4) | 0.875 | 2 (1–5) | 2 (1–4) | 0.072 | 0.8 | (0.7–0.9) | 0.016 |
| Readmission frequency f,g | 5 (4–9) | 5 (3–8) | <0.001 | 6 (4–9) | 5 (3–8) | 0.008 | 1.6 | (1.5–1.7) | <0.0001 |
3.5. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bergström, S.; Carr, H.; Petersson, G.; Stephansson, O.; Bonamy, A.-K.E.; Dahlström, A.; Halvorsen, C.P.; Johansson, S. Trends in Congenital Heart Defects in Infants with Down Syndrome. Pediatrics 2016, 138, e20160123. [Google Scholar] [CrossRef]
- Brodwall, K.; Greve, G.; Leirgul, E.; Klungsøyr, K.; Holmstrøm, H.; Vollset, S.E.; Øyen, N. The five-year survival of children with Down syndrome in Norway 1994–2009 differed by associated congenital heart defects and extracardiac malformations. Acta Paediatr. 2018, 107, 845–853. [Google Scholar] [CrossRef]
- Morales-Demori, R. Congenital heart disease and cardiac procedural outcomes in patients with trisomy 21 and Turner syndrome. Congenit. Heart Dis. 2017, 12, 820–827. [Google Scholar] [CrossRef]
- Lal, P.S.; Chavan, B.; Devendran, V.R.; Varghese, R.; Murmu, U.C.; Kumar, R.S. Surgical outcome of congenital heart disease in Down’s syndrome. Asian Cardiovasc. Thorac. Ann. 2013, 21, 166–169. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, J.E.; Shim, S.M.; Ha, E.K.; Yon, D.K.; Kim, O.H.; Baek, J.H.; Koh, H.Y.; Chae, K.Y.; Lee, S.W.; et al. Cohort profile: National Investigation of Birth Cohort in Korea study 2008 (NICKs-2008). Clin. Exp. Pediatr. 2021, 64, 480–488. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.-Y.; Khang, Y.-H.; Heon Park, J.; Kang, H.-J.; Lee, H.; Do, C.-H.; Song, J.-S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef]
- Vozoris, N.T.; Pequeno, P.; Li, P.; Austin, P.C.; Stephenson, A.L.; O’Donnell, D.E.; Gill, S.S.; Gershon, A.S.; Rochon, P.A. Morbidity and mortality associated with prescription cannabinoid drug use in COPD. Thorax 2021, 76, 29–36. [Google Scholar] [CrossRef]
- Brookhart, M.A.; Wyss, R.; Layton, J.B.; Stürmer, T. Propensity Score Methods for Confounding Control in Nonexperimental Research. Circ. Cardiovasc. Qual. Outcomes 2013, 6, 604–611. [Google Scholar] [CrossRef]
- Sato, T.; Matsuyama, Y. Marginal Structural Models as a Tool for Standardization. Epidemiology 2003, 14, 680–686. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [Green Version]
- Zou, G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Kwon, J.Y.; Park, I.Y.; Park, Y.G.; Lee, Y.; Lee, G.; Shin, J.C. Korean-Specific Parameter Models for Calculating the Risk of Down Syndrome in the Second Trimester of Pregnancy. J. Korean Med. Sci. 2011, 26, 1619–1624. [Google Scholar] [CrossRef]
- Vis, J.C.; Duffels, M.G.J.; Winter, M.M.; Weijerman, M.E.; Cobben, J.M.; Huisman, S.A.; Mulder, B.J.M. Down syndrome: A cardiovascular perspective. J. Intellect. Disabil. Res. 2009, 53, 419–425. [Google Scholar] [CrossRef]
- Freeman, S.B.; Taft, L.F.; Dooley, K.J.; Allran, K.; Sherman, S.L.; Hassold, T.J.; Khoury, M.J.; Saker, D.M. Population-based study of congenital heart defects in Down syndrome. Am. J. Med. Genet. 1998, 80, 213–217. [Google Scholar] [CrossRef]
- Marino, B. Congenital heart disease in patients with Down’s syndrome: Anatomic and genetic aspects. Biomed. Pharmacother. 1993, 47, 197–200. [Google Scholar] [CrossRef]
- Fudge, J.C., Jr.; Li, S.; Jaggers, J.; O’Brien, S.M.; Peterson, E.D.; Jacobs, J.P.; Welke, K.F.; Jacobs, M.L.; Li, J.S.; Pasquali, S.K. Congenital Heart Surgery Outcomes in Down Syndrome: Analysis of a National Clinical Database. Pediatrics 2010, 126, 315–322. [Google Scholar] [CrossRef]
- Martínez-Quintana, E.; Rodríguez-González, F.; Medina-Gil, J.M.; Agredo-Muñoz, J.; Nieto-Lago, V. Clinical outcome in Down syndrome patients with congenital heart disease. Cir. Cir. 2010, 78, 245–250. [Google Scholar]
- Cullen, S.M.; Cronk, C.E.; Pueschel, S.M.; Schnell, R.R.; Reed, R.B. Social development and feeding milestones of young Down syndrome children. Am. J. Ment. Defic. 1981, 85, 410–415. [Google Scholar]
- Malec, E.; Mroczek, T.; Pajak, J.; Januszewska, K.; Zdebska, E. Results of surgical treatment of congenital heart defects in children with Down’s syndrome. Pediatr. Cardiol. 1999, 20, 351–354. [Google Scholar] [CrossRef]
- Reller, M.D.; Morris, C.D. Is Down syndrome a risk factor for poor outcome after repair of congenital heart defects? J. Pediatr. 1998, 132, 738–741. [Google Scholar] [CrossRef]
- Boneva, R.S.; Botto, L.D.; Moore, C.A.; Yang, Q.; Correa, A.; Erickson, J.D. Mortality associated with congenital heart defects in the United States: Trends and racial disparities, 1979–1997. Circulation 2001, 103, 2376–2381. [Google Scholar] [CrossRef]
- Bertapelli, F.; Martin, J.E.S.-S.; Gonçalves, E.M.; de Oliveira Barbeta, V.J.; Guerra-Júnior, G. Growth curves in Down syndrome: Implications for clinical practice. Am. J. Med Genet. Part A 2014, 164, 844–847. [Google Scholar] [CrossRef]
- Santos, F.C.G.B.; Croti, U.A.; De Marchi, C.H.; Murakami, A.N.; Brachine, J.D.P.; Borim, B.C.; Finoti, R.G.; De Godoy, M.F. Surgical Treatment for Congenital Heart Defects in Down Syndrome Patients. Braz. J. Cardiovasc. Surg. 2019, 34, 1–7. [Google Scholar] [CrossRef]


| Demographic Characteristics | Observed Data (N = 5282) | Propensity-Matched Data (N = 4635) | ||||
|---|---|---|---|---|---|---|
| Total Correction for CHD, N (%) a | Total Correction for CHD, N (%) a | |||||
| Control | Down | SMD b | Control | Down | SMD b | |
| Total, n | 5048 | 234 | 4482 | 153 | ||
| Male | 2641 (52.3) | 126 (53.8) | −0.02 | 2343 (52.3) | 74 (48.4) | 0.07 |
| Female | 2407 (47.7) | 108 (46.2) | 2139 (47.7) | 79 (51.6) | ||
| Prematurity, n c | 433 (8.5) | 24 (10.30) | 0.10 | 437 (9.8) | 22 (14.4) | 0.14 |
| Birth weight d, kg (IQR) e | 3.1 (2.7–3.4) | 2.9 (2.5–3.2) | −0.29 | 3.0 (2.7–3.4) | 2.9 (2.6–3.2) | −0.17 |
| Birthplace, n f | ||||||
| Seoul | 1059 (21.0) | 50 (21.4) | 0.03 | 926 (20.7) | 30 (19.6) | −0.02 |
| Metropolitan area | 1178 (23.3) | 54 (23.1) | −0.04 | 1049 (23.4) | 34 (22.2) | −0.02 |
| Urban area | 2338 (46.3) | 104 (44.4) | −0.04 | 2084 (46.5) | 76 (49.7) | 0.06 |
| Rural | 421 (8.3) | 25 (10.7) | 0.10 | 377 (8.4) | 11 (7.2) | −0.02 |
| Economic status, n g | ||||||
| 1st (low) | 419 (8.3) | 22 (9.4) | 0.07 | 364 (8.1) | 10 (6.5) | −0.06 |
| 2nd | 722 (14.3) | 33 (14.1) | 0.02 | 632 (14.1) | 21 (13.7) | −0.01 |
| 3rd | 1301 (25.8) | 63 (26.9) | 0.02 | 1182 (26.4) | 45 (29.4) | 0.07 |
| 4th | 1524 (30.2) | 54 (23.1) | −0.16 | 1363 (30.4) | 45 (29.4) | −0.02 |
| 5th | 873 (17.3) | 50 (21.4) | 0.04 | 757 (16.9) | 26 (17.0) | 0.01 |
| Year of birth | ||||||
| 2008 | 925 (18.3) | 44 (18.8) | −0.00 | 763 (17.0) | 23 (15.0) | −0.05 |
| 2009 | 917 (18.2) | 46 (19.7) | −0.01 | 808 (18.0) | 29 (19.0) | 0.02 |
| 2010 | 1006 (19.9) | 40 (17.1) | −0.04 | 900 (20.1) | 33 (21.6) | 0.04 |
| 2011 | 1070 (21.2) | 53 (22.6) | 0.03 | 984 (22.0) | 33 (21.6) | 0.00 |
| 2012 | 1130 (22.4) | 51 (21.8) | 0.03 | 1027 (22.9) | 34 (22.2) | −0.01 |
| Surgery | ||||||
| Total correction, n | 4521 (88.9) | 217 (92.7) | 0.14 | 4042 (90.2) | 141 (92.2) | 0.06 |
| Palliation and total correction, n | 527 (10.4) | 17 (7.3) | −0.14 | 440 (9.8) | 12 (7.8) | −0.06 |
| Age at total correction, months (IQR) e | 4 (1–11) | 4 (2–7) | −0.24 | 4 (1–11) | 5 (2–8) | −0.18 |
| CHD | Priority | Total (N = 5282) | Control (N = 5048) | Down Syndrome (N = 234) | |||
|---|---|---|---|---|---|---|---|
| n | n | % | n | % | p-Value | ||
| AVSD * | 1 | 674 | 585 | 11.5 | 89 | 38.0 | <0.0001 |
| TOF | 2 | 863 | 844 | 16.7 | 19 | 8.1 | 0.000 |
| TGA | 3 | 398 | 396 | 7.8 | 2 | 0.8 | <0.0001 |
| SV | 4 | 170 | 170 | 3.3 | 0 | 0.0 | 0.004 |
| CoA | 5 | 353 | 346 | 6.8 | 7 | 2.9 | 0.020 |
| DORV | 6 | 119 | 113 | 2.2 | 6 | 2.5 | 0.742 |
| VSD | 7 | 1731 | 1640 | 32.4 | 91 | 38.8 | 0.041 |
| PA | 8 | 44 | 43 | 0.8 | 1 | 0.4 | 0.484 |
| AS | 9 | 27 | 27 | 0.5 | 0 | 0.0 | 0.262 |
| PS | 10 | 113 | 112 | 2.2 | 1 | 0.4 | 0.064 |
| PDA | 11 | 142 | 137 | 2.7 | 5 | 2.1 | 0.593 |
| ASD | 12 | 581 | 568 | 11.2 | 13 | 5.5 | 0.006 |
| TAPVR and PAPVR | 13 | 46 | 46 | 0.9 | 0 | 0.0 | 0.142 |
| OTHERS | 14 | 21 | 21 | 0.4 | 0 | 0.0 | 0.322 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwak, J.H.; Lee, S.W.; Cha, H.R.; Huh, J.; Kang, I.-S.; Jun, T.-G.; Yang, J.-H.; Han, M.Y.; Song, J. Long-Term Observational Outcomes after Total Correction of Congenital Heart Disease in Korean Patients with Down Syndrome: A National Cohort Study. Children 2022, 9, 1329. https://doi.org/10.3390/children9091329
Kwak JH, Lee SW, Cha HR, Huh J, Kang I-S, Jun T-G, Yang J-H, Han MY, Song J. Long-Term Observational Outcomes after Total Correction of Congenital Heart Disease in Korean Patients with Down Syndrome: A National Cohort Study. Children. 2022; 9(9):1329. https://doi.org/10.3390/children9091329
Chicago/Turabian StyleKwak, Ji Hee, Seung Won Lee, Hye Ryeong Cha, June Huh, I-Seok Kang, Tae-Gook Jun, Ji-Hyuk Yang, Man Yong Han, and Jinyoung Song. 2022. "Long-Term Observational Outcomes after Total Correction of Congenital Heart Disease in Korean Patients with Down Syndrome: A National Cohort Study" Children 9, no. 9: 1329. https://doi.org/10.3390/children9091329