
Diagnostic Tools in the Detection of Physical Child Abuse: A Systematic Review
 , , , ,
, , , ,
Abstract
:1. Introduction
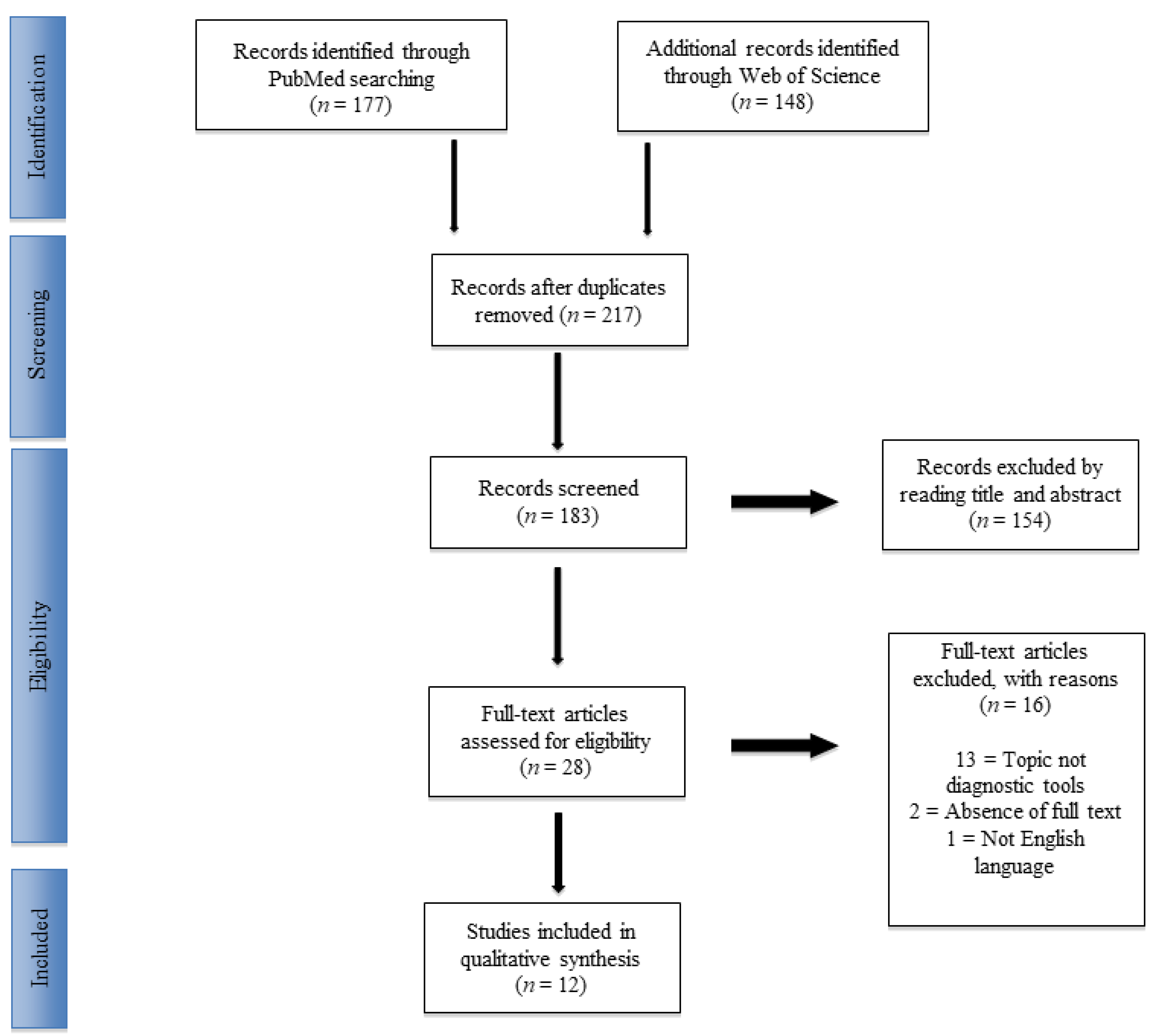
2. Materials and Methods
2.1. Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Risk of Bias Assessment
3. Results
3.1. Escape
3.2. ISPCAN Child Abuse Screening Tools Retrospective Version (ICAST-R)
3.3. Child Trauma Questionnaire (CTQ-SF)
3.4. Burn Screening
3.5. Predicting Abusive Head Trauma (PredAHT) Tool
3.6. SPUTOVAMO-R
3.7. Screening Index for Physical Child Abuse (SIPCA)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marine, M.B.; Forbes-Amrhein, M.M. Fractures of Child Abuse. Pediatr. Radiol. 2021, 51, 1003–1013. [Google Scholar] [CrossRef] [PubMed]
- Sethi, D.; Yon, Y.; Parekh, N.; Anderson, T.; Huber, J.; Rakovac, I.; Meinck, F. European Status Report on Preventing Child Maltreatment; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Butchart, A.; Mikton, C.; Dahlberg, L.L.; Krug, E.G. Global Status Report on Violence Prevention 2014. Inj Prev. 2015, 21, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayakumar, P.; Barry, M.; Ramachandran, M. Orthopaedic Aspects of Paediatric Non-Accidental Injury. J. Bone Jt. Surg. 2010, 92, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, D.; Bethencourt Mirabal, A.; McCall, J.D. Child Abuse and Neglect. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hung, K.-L. Pediatric Abusive Head Trauma. Biomed. J. 2020, 43, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Offiah, A.; van Rijn, R.R.; Perez-Rossello, J.M.; Kleinman, P.K. Skeletal Imaging of Child Abuse (Non-Accidental Injury). Pediatr. Radiol. 2009, 39, 461–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodner, C.; Wetherton, A. Diagnosis and Management of Physical Abuse in Children. Am. Fam. Physician 2013, 88, 669–675. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louwers, E.C.F.M.; Korfage, I.J.; Affourtit, M.J.; Ruige, M.; van den Elzen, A.P.M.; de Koning, H.J.; Moll, H.A. Accuracy of a Screening Instrument to Identify Potential Child Abuse in Emergency Departments. Child Abus. Negl. 2014, 38, 1275–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunne, M.P.; Zolotor, A.J.; Runyan, D.K.; Andreva-Miller, I.; Choo, W.Y.; Dunne, S.K.; Gerbaka, B.; Isaeva, O.; Jain, D.; Kasim, M.S.; et al. ISPCAN Child Abuse Screening Tools Retrospective Version (ICAST-R): Delphi Study and Field Testing in Seven Countries. Child Abus. Negl. 2009, 33, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.; Gallardo-Pujol, D.; Pereda, N.; Arntz, A.; Bernstein, D.P.; Gaviria, A.M.; Labad, A.; Valero, J.; Gutiérrez-Zotes, J.A. Initial Validation of the Spanish Childhood Trauma Questionnaire-Short Form: Factor Structure, Reliability and Association With Parenting. J. Interpers Violence 2013, 28, 1498–1518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karos, K.; Niederstrasser, N.; Abidi, L.; Bernstein, D.P.; Bader, K. Factor Structure, Reliability, and Known Groups Validity of the German Version of the Childhood Trauma Questionnaire (Short-Form) in Swiss Patients and Nonpatients. J. Child Sex. Abus. 2014, 23, 418–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinhoven, P.; Penninx, B.W.; Hickendorff, M.; van Hemert, A.M.; Bernstein, D.P.; Elzinga, B.M. Childhood Trauma Questionnaire: Factor Structure, Measurement Invariance, and Validity across Emotional Disorders. Psychol. Assess. 2014, 26, 717–729. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhong, X.; Gao, Y.; Xiong, G.; Yao, S. Psychometric Properties of the Chinese Version of the Childhood Trauma Questionnaire-Short Form (CTQ-SF) among Undergraduates and Depressive Patients. Child Abus. Negl. 2019, 91, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Kongerslev, M.T.; Bach, B.; Rossi, G.; Trauelsen, A.M.; Ladegaard, N.; Løkkegaard, S.S.; Bo, S. Psychometric Validation of the Childhood Trauma Questionnaire-Short Form (CTQ-SF) in a Danish Clinical Sample. Child Abus. Negl. 2019, 94, 104026. [Google Scholar] [CrossRef] [PubMed]
- Spies, G.; Kidd, M.; Seedat, S. A Factor Analytic Study of the Childhood Trauma Questionnaire-Short Form in an All-Female South African Sample with and without HIV Infection. Child Abus. Negl. 2019, 92, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.D.; Tepper, D.; Jenny, C. Effect of a Screening Profile on the Diagnosis of Nonaccidental Burns in Children. Pediatr. Emerg. Care 1997, 13, 259–261. [Google Scholar] [CrossRef]
- Cowley, L.E.; Farewell, D.M.; Kemp, A.M. Potential Impact of the Validated Predicting Abusive Head Trauma (PredAHT) Clinical Prediction Tool: A Clinical Vignette Study. Child Abus. Negl. 2018, 86, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Sittig, J.S.; Uiterwaal, C.S.P.M.; Moons, K.G.M.; Russel, I.M.B.; Nievelstein, R.A.J.; Nieuwenhuis, E.E.S.; van de Putte, E.M. Value of Systematic Detection of Physical Child Abuse at Emergency Rooms: A Cross-Sectional Diagnostic Accuracy Study. BMJ Open 2016, 6, e010788. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.C.; Knight, V.M.; Ziegfeld, S.; Haider, A.; Paidas, C. The Multi-Institutional Validation of the New Screening Index for Physical Child Abuse. J. Pediatr. Surg. 2005, 40, 114–119. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Samples | Intervention | Outcome Measures | Results | Limits of the Study |
|---|---|---|---|---|---|
| Louwers et al., 2014 | 89 children (55 were potential abuse cases, 44 were really positive) Average age was 5.5, 57% were male, 44 were positive | They prospectively examined children for child abuse with ESCAPE questionnaire | Sensitivity, specificity, +LR, −LR | The sensitivity was 0.80, the specificity was 0.98, +LR was 40, −LR was 0.20 Therefore, the escape instrument is useful for identifying children who are at high risk of abuse | The real rate of child abuse is not available because potential abuse could distort the end result |
| Dunne et al., 2009 | 842 children (18–26 years) | Delphy group developed and validated a questionnaire for child abuse in 7 countries, ICAST-R | Cronbach’s alpha | Cronbach’s alpha was moderate, 0.610, for physical abuse | The sample was small, Gender differenceswere missing, The validity and reliability have not been verified |
| Hernandez et al., 2013 | 185 women abused (18–65 years) | They validated the Spanish version of CTQ-SF questionnaire, retrospectively, for child abuse | Cronbach’s alpha S-B χ2, p, S-B χ2/df, CFI, RMS | S-B χ2 (265) = 380.51, p < 0.001,…; S-B χ2/df = 1.43 CFI = 0.94, RMS = 0.04, Cronbach’s alpha was 0.88 Cronbach’s α coefficients obtained were really satisfactory | The results obtained cannot be extended to the non-clinical or male population, and the data could be distorted |
| Bernesteid et al., 2014 | 661 individuals divided into 3 different clinical populations | They validated the German version of CTQ-SF questionnaire for child abuse | Cronbach’s alpha | Cronbach’s alpha was 0.82 for physical abuse and 0.53 for physical neglect This study shows a good validity of the German model with the exception of the physical neglect scale | There are no means to verify the answers. The use of a mainly clinical sample is another limitation of the present study. Finally, it would have been useful to check whether the results could be generalized to non-Swiss German-speaking people |
| Spinhoven et al., 2014 | 2308 patients (18–65 years) | They verified the validity of CTQ-SF and its association with the CTI | Cronbach’s alpha | Cronbach’s alpha was good for physical abuse (0.88) and moderate for the physical neglect scale (0.60) The results on validity and reliability available make the CTQ-SF a valid tool for the screening of various forms of abuse | In this study there may have been flawed memories in the reconstruction of the abuse by the patient |
| He et al., 2019 | 3431 (1943 men; 1488 women) | They examined the psychometric properties of the 28-item CTQ-SF in a Chinese population | Cronbach’s alpha | CTQ-SF total was 0.79; emotional neglect 0.76; physical neglect 0.52; Emotional abuse 0.68; Physical abuse 0.72; Sexual abuse 0.77 | Lack of diversity in the selection of subjects. Horizontal study. |
| Kongerslev et al., 2019 | 142; 68% women; | They evaluated the psychometric properties of the Danish CTQ-SF in a clinical sample. | Comparative fit index | CTQ-SF total was 0.878; emotional neglect 0.62; physical neglect 0.48; emotional abuse 0.62; physical abuse 0.37; sexual abuse 0.93 | A small subsample of adult outpatients diagnosed with personality disorders. Horizontal study. |
| Spies et al., 2019 | 314 women (170 HIV uninfected; 144 HIV infected) | They evaluated the psychometric properties of the South Africa CTQ-SF in a clinical sample. | Comparative fit index; goodness of fit index | Comparative fit index 0.94; goodness of fit index 0.85 | Lack of diversity in the selection of subjects. Horizontal study. |
| Clark et al., 1997 | 215 patients | They prospectively validated the effectiveness of a new list with 13 factors associated with abusive burns | Number of new diagnoses of child abuse to ED | Reports rose to 12.1% | A limitation of this study is the few cases used |
| Sittig et al., 2016 | 4290 children (0–7 years) | They investigated a new questionnaire, SPUTOVAMO-R, for child abuse | Prevalence, positive PV, false-positive rate, false-negative rate | The physical abuse’s prevalence was 0.07% (95% CI 0.01 to 0.2). For every 100 cases of suspected child abuse, only 3 were really abused (positive PV of 0.03); however, 97 were not really abused (false-positive rate of 0.97 (95% CI from 0.915 to 0.904), and 0 were lost to follow-up (false-negative rate of 0.0, 95% CI 0.0 to 0.006(8). This study shows that this questionnaire gives a high rate of false positives, 97%, which could lead to unnecessary treatment | A certain level of implicit bias cannot be excluded |
| Chang et al., 2005 | 58,558 children In 17 cities | They examined the effectiveness of the SIPCA questionnaire for child abuse | Sensitivity, specificity | A SIPCA score of 3 had a sensitivity of 86.6% and a specificity of 80.5%, a SPICA score of 4 had a specificity of 93.1%, but had a lower sensitivity of 71.8. The study shows a high rate of sensitivity and specificity for a SPICA score of 3 and a higher sensitivity and a lower specificity for a SPICA score of 4. Therefore, a score of 3 on SIPCA represents a good compromise | The truthfulness of the data in hospital records |
| Cowley et al., 2018 | Children under 3 years age | A clinical vignette study analyzing the Predicting Abusive Head Trauma (PredAHT) tool to estimate the likelihood of abusive head injury (AHT) | Sensitivity, specificity | The sensitivity of PredAHT was 72.3% and the specificity was 85.7%.PredAHT significantly influenced clinicians’ probability estimates (p < 0.001) | Since vignettes differ from real situations, studies on vignettes are often criticized because of the potential limits of external validity and their propensity for evaluation error by the clinicians, who are also influenced by distractors |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavone, V.; Vescio, A.; Lucenti, L.; Amico, M.; Caldaci, A.; Pappalardo, X.G.; Parano, E.; Testa, G. Diagnostic Tools in the Detection of Physical Child Abuse: A Systematic Review. Children 2022, 9, 1257. https://doi.org/10.3390/children9081257
Pavone V, Vescio A, Lucenti L, Amico M, Caldaci A, Pappalardo XG, Parano E, Testa G. Diagnostic Tools in the Detection of Physical Child Abuse: A Systematic Review. Children. 2022; 9(8):1257. https://doi.org/10.3390/children9081257
Chicago/Turabian StylePavone, Vito, Andrea Vescio, Ludovico Lucenti, Mirko Amico, Alessia Caldaci, Xena Giada Pappalardo, Enrico Parano, and Gianluca Testa. 2022. "Diagnostic Tools in the Detection of Physical Child Abuse: A Systematic Review" Children 9, no. 8: 1257. https://doi.org/10.3390/children9081257