
Changing Epidemiology of Acute Viral Respiratory Infections in Hospitalized Children: The Post-Lockdown Effect

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
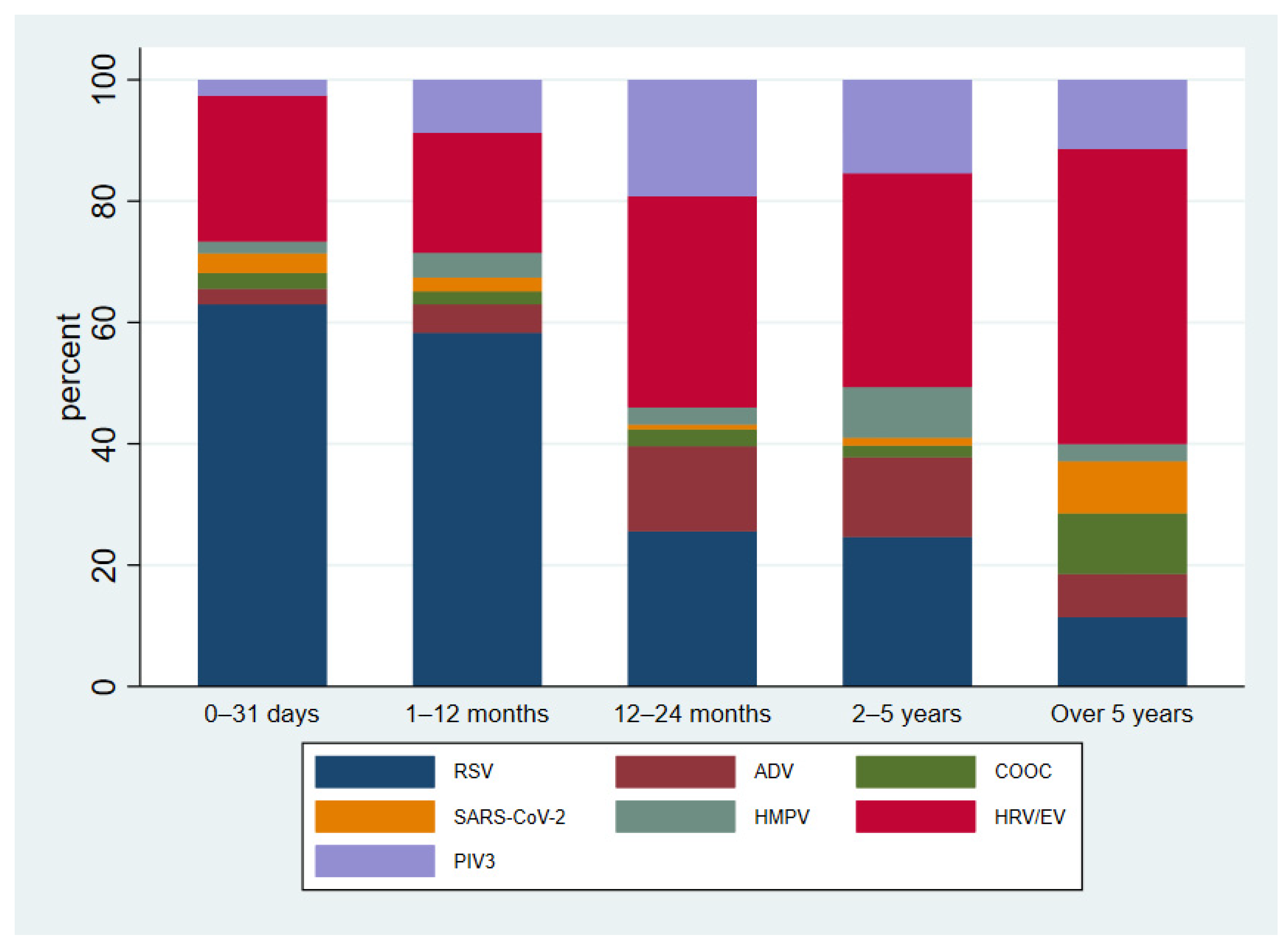
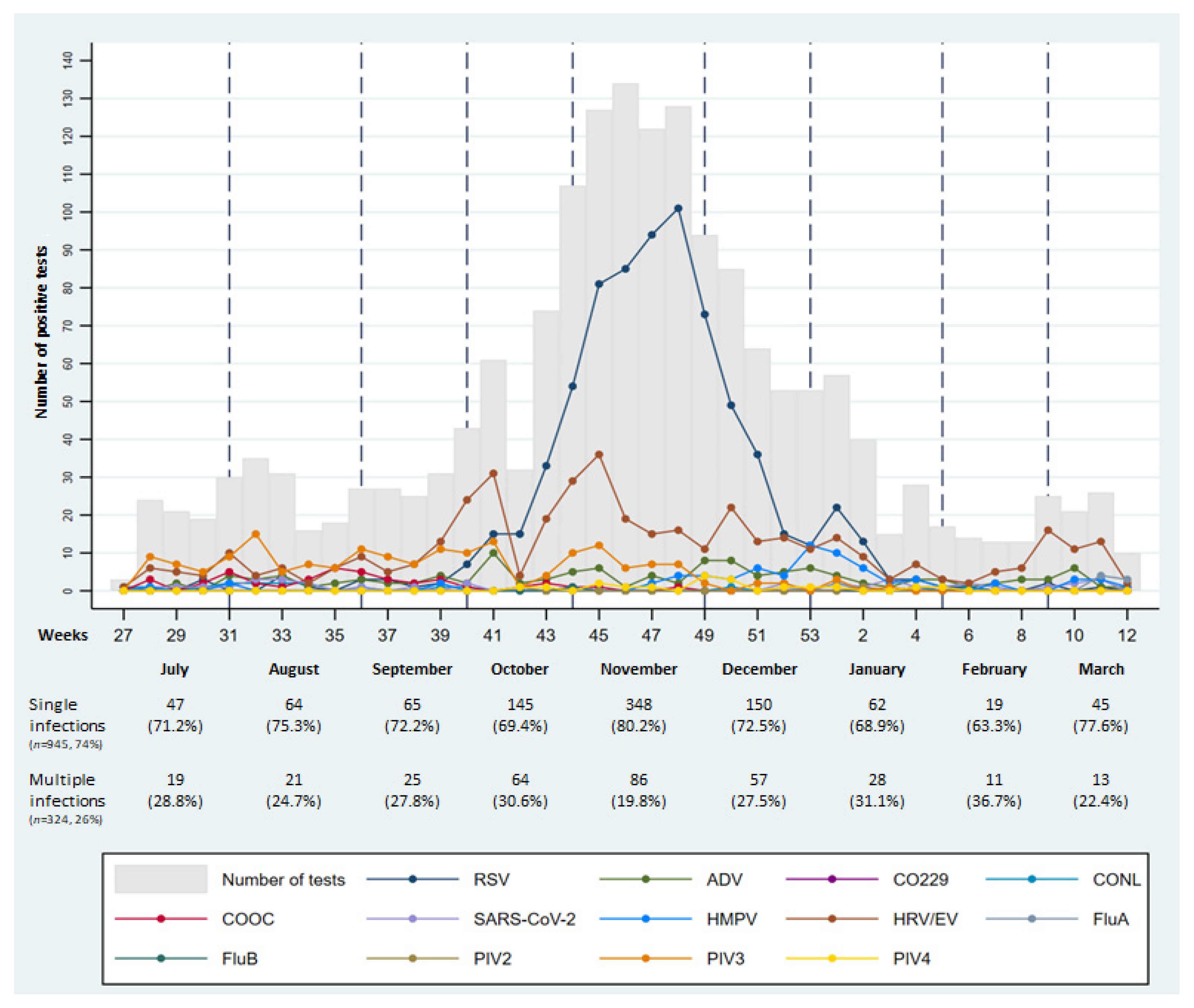
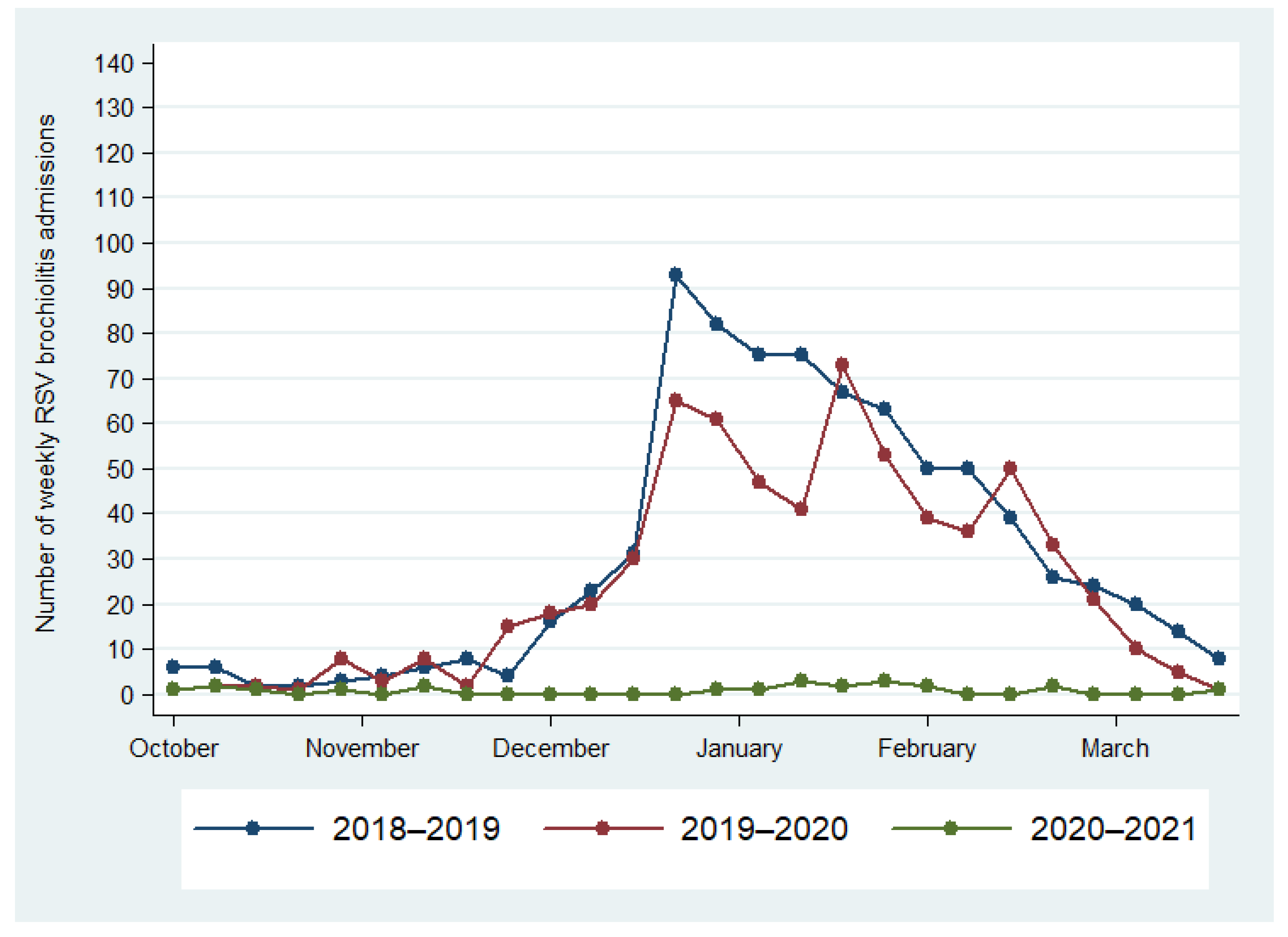
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uitti, J.M.; Tähtinen, P.A.; Laine, M.K.; Huovinen, P.; Ruuskanen, O.; Ruohola, A. Role of Nasopharyngeal Bacteria and Respiratory Viruses in Acute Symptoms of Young Children. Pediatr. Infect. Dis. J. 2015, 34, 1056–1062. [Google Scholar] [CrossRef]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef]
- Jefferson, T.; Del Mar, C.B.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; Bawazeer, G.A.; Driel, M.L.; Jones, M.A.; Thorning, S.; Beller, E.M.; et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst. Rev. 2020, 11, CD006207. [Google Scholar] [PubMed]
- Amaddeo, A.; Cason, C.; Cozzi, G.; Ronfani, L.; Comar, M. Social distancing measures for COVID-19 are changing winter season. Arch. Dis. Child. 2021, 106, e47. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, H.; Song, K.H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of Public Health Interventions on Seasonal Influenza Activity during the COVID-19 Outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef] [PubMed]
- Agha, R.; Avner, J.R. Delayed Seasonal RSV Surge Observed during the COVID-19 Pandemic. Pediatrics 2021, 148, e2021052089. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, D.K.; Foley, D.A.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Blyth, C.C.; Moore, H.C. The impact of COVID-19 public health measures on detections of influenza and respiratory syncytial virus in children during the 2020 Australian winter. Clin. Infect. Dis. 2020, 72, 2199–2202. [Google Scholar] [CrossRef] [PubMed]
- Fitzner, J.; Qasmieh, S.; Mounts, A.W.; Alexander, B.; Besselaar, T.; Briand, S.; Brown, C.; Clark, S.; Dueger, E.; Gross, D.; et al. Revision of clinical case definitions: Influenza-like illness and severe acute respiratory infection. Bull. World Health Organ. 2018, 96, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Florin, T.A.; Plint, A.C.; Zorc, J.J. Viral bronchiolitis. Lancet 2017, 389, 211–224. [Google Scholar] [CrossRef]
- Camporesi, A.; Morello, R.; Ferro, V.; Pierantoni, L.; Rocca, A.; Lanari, M.; Trobia, G.L.; Sciacca, T.; Bellinvia, A.G.; De Ferrari, A.; et al. Epidemiology, Microbiology and Severity of Bronchiolitis in the First Post-Lockdown Cold Season in Three Different Geographical Areas in Italy: A Prospective, Observational Study. Children 2022, 9, 491. [Google Scholar] [CrossRef] [PubMed]
- Van Summeren, J.; Meijer, A.; Aspelund, G.; Casalegno, J.S.; Erna, G.; Hoang, U.; Lina, B.; VRS Study Group in Lyon; de Lusignan, S.; Teirlinck, A.C.; et al. Low levels of respiratory syncytial virus activity in Europe during the 2020/21 season: What can we expect in the coming summer and autumn/winter? EuroSurveillance 2021, 26, 2100639. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.A.; Yeoh, D.K.; Minney-Smith, C.A.; Martin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Moore, H.C.; Blyth, C.C. The Interseasonal Resurgence of Respiratory Syncytial Virus in Australian Children Following the Reduction of Coronavirus Disease 2019-Related Public Health Measures. Clin. Infect. Dis. 2021, 73, e2829–e2830. [Google Scholar] [CrossRef] [PubMed]
- Weinberger Opek, M.; Yeshayahu, Y.; Glatman-Freedman, A.; Kaufman, Z.; Sorek, N.; Brosh-Nissimov, T. Delayed respiratory syncytial virus epidemic in children after relaxation of COVID-19 physical distancing measures, Ashdod, Israel, 2021. EuroSurveillance 2021, 26, 2100706. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N. Resurgence of Respiratory Syncytial Virus Infections during COVID-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef] [PubMed]
- Horemheb-Rubio, G.; Eggeling, R.; Schmeiβer, N.; Pfeifer, N.; Lengauer, T.; Gärtner, B.C.; Prifert, C.; Kochanek, M.; Scheid, C.; Adams, O.; et al. Respiratory viruses dynamics and interactions: Ten years of surveillance in central Europe. BMC Public Health 2022, 22, 1167. [Google Scholar] [CrossRef] [PubMed]
- Achten, N.B.; Wu, P.; Bont, L.; Blanken, M.O.; Gebretsadik, T.; Chappell, J.D.; Wang, L.; Yu, C.; Larkin, E.K.; Carroll, K.N.; et al. Interference between Respiratory Syncytial Virus and Human Rhinovirus Infection in Infancy. J. Infect. Dis. 2017, 215, 1102–1106. [Google Scholar] [CrossRef] [PubMed]
- Britton, P.N.; Hu, N.; Saravanos, G.; Shrapnel, J.; Davis, J.; Snelling, T.; Dalby-Payne, J.; Kesson, A.M.; Wood, N.; Macartney, K.; et al. COVID-19 public health measures and respiratory syncytial virus. Lancet Child Adolesc. Health 2020, 4, e42–e43. [Google Scholar] [CrossRef]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Giannattasio, A.; Maglione, M.; D’Anna, C.; Muzzica, S.; Angrisani, F.; Acierno, S.; Perrella, A.; Tipo, V. Silent RSV in infants with SARS-CoV-2 infection: A case series. Pediatr. Pulmonol. 2021, 56, 3044–3046. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Lisi, G.C.; et al. Epidemiology and prevention of respiratory syncytial virus infections in children in Italy. Ital. J. Pediatr. 2021, 47, 198. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Infections * (n = 1674) | Multiple Infections (n = 324) | |||
|---|---|---|---|---|
| n | % | n | % | |
| RSV | 733 | 43.8 | 171 | 52.8 |
| ADV | 124 | 7.4 | 98 | 30.2 |
| CO229E | 4 | 0.2 | 2 | 0.6 |
| CONL | 17 | 1.0 | 10 | 3.1 |
| COOC | 42 | 2.5 | 22 | 6.8 |
| SARS-CoV-2 | 36 | 2.2 | 15 | 4.6 |
| HMPV | 72 | 4.3 | 42 | 13 |
| HRV/EV | 433 | 25.9 | 246 | 75.9 |
| FluA | 11 | 0.7 | 5 | 1.5 |
| FluB | 1 | 0.1 | 1 | 0.3 |
| PIV2 | 2 | 0.1 | 2 | 0.6 |
| PIV3 | 181 | 10.8 | 100 | 30.9 |
| PIV4 | 18 | 1.1 | 15 | 4.6 |
| Multiple Infections | Univariate Analysis | Multivariate Analysis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes (n = 324, 26%) | No (n = 945, 74%) | |||||||||||
| n | % | n | % | OR | 95% CI | p | OR | 95% CI | p | |||
| Gender | 0.89 | 0.69 | 1.14 | 0.36 | 0.81 | 0.63 | 1.06 | 0.12 | ||||
| Male | 181 | 26.6 | 500 | 73.4 | ||||||||
| Female | 143 | 24.3 | 445 | 75.7 | ||||||||
| Age group | ||||||||||||
| 0–31 days | 24 | 18.3 | 107 | 81.7 | ||||||||
| 1–12 months | 138 | 20.2 | 545 | 79.8 | 1.13 | 0.70 | 1.83 | 0.62 | 1.11 | 0.69 | 1.80 | 0.67 |
| 12–24 months | 65 | 36.7 | 112 | 63.3 | 2.59 | 1.51 | 4.43 | <0.001 | 2.61 | 1.51 | 4.49 | <0.001 |
| 2–5 years | 82 | 37.4 | 137 | 62.6 | 2.67 | 1.59 | 4.49 | <0.001 | 2.72 | 1.61 | 4.59 | <0.001 |
| Over 5 years | 15 | 25.4 | 44 | 74.6 | 1.52 | 0.73 | 3.17 | 0.26 | 1.43 | 0.68 | 3.02 | 0.34 |
| Season | ||||||||||||
| Summer | 60 | 27.5 | 158 | 72.5 | ||||||||
| Autumn | 204 | 24.2 | 638 | 75.7 | 0.84 | 0.60 | 1.18 | 0.32 | 1.05 | 0.74 | 1.49 | 0.79 |
| Winter | 60 | 28.7 | 149 | 71.3 | 1.06 | 0.70 | 1.62 | 0.79 | 1.21 | 0.79 | 1.87 | 0.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maglione, M.; Pascarella, A.; Botti, C.; Ricci, G.; Morelli, F.; Camelia, F.; Micillo, A.; Calì, C.; Savoia, F.; Tipo, V.; et al. Changing Epidemiology of Acute Viral Respiratory Infections in Hospitalized Children: The Post-Lockdown Effect. Children 2022, 9, 1242. https://doi.org/10.3390/children9081242
Maglione M, Pascarella A, Botti C, Ricci G, Morelli F, Camelia F, Micillo A, Calì C, Savoia F, Tipo V, et al. Changing Epidemiology of Acute Viral Respiratory Infections in Hospitalized Children: The Post-Lockdown Effect. Children. 2022; 9(8):1242. https://doi.org/10.3390/children9081242
Chicago/Turabian StyleMaglione, Marco, Antonia Pascarella, Chiara Botti, Giuseppe Ricci, Fiorella Morelli, Fabiana Camelia, Alberto Micillo, Camilla Calì, Fabio Savoia, Vincenzo Tipo, and et al. 2022. "Changing Epidemiology of Acute Viral Respiratory Infections in Hospitalized Children: The Post-Lockdown Effect" Children 9, no. 8: 1242. https://doi.org/10.3390/children9081242