
Review of a 25-Year Experience in the Management of Ovarian Masses in Neonates, Children and Adolescents: From Laparoscopy to Robotics and Indocyanine Green Fluorescence Technology

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
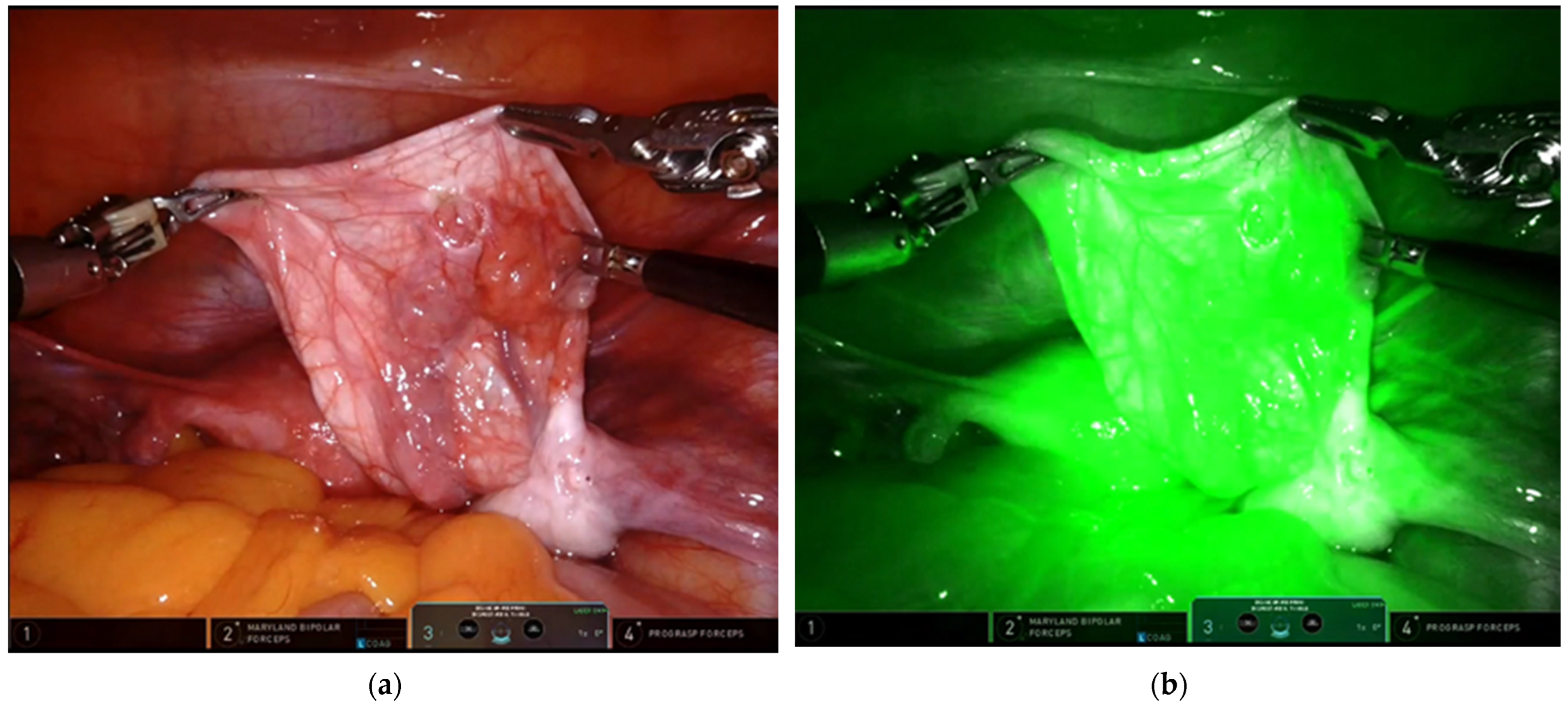
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Heling, K.-S.; Chaoui, R.; Kirchmair, F.; Stadie, S.; Bollmann, R. Fetal ovarian cysts: Prenatal diagnosis, management and postnatal outcome. Ultrasound Obstet. Gynecol. 2002, 20, 47–50. [Google Scholar] [CrossRef]
- Ahmed, S. Neonatal and childhood ovarian cysts. J. Pediatr. Surg. 1971, 6, 702–708. [Google Scholar] [CrossRef]
- Ein, S.H.; Darte, J.M.M.; Stephens, C.A. Cystic and solid ovarian tumors in children: A 44-year review. J. Pediatr. Surg. 1970, 5, 148–156. [Google Scholar] [CrossRef]
- Groeber, W.R. Ovarian tumors during infancy and childhood. Am. J. Obstet. Gynecol. 1963, 86, 1027–1035. [Google Scholar] [CrossRef]
- Henes, M.; Engler, T.; Taran, F.; Brucker, S.; Rall, K.; Janz, B.; Lawrenz, B. Ovarian cyst removal influences ovarian reserve dependent on histology, size and type of operation. Women’s Health 2018, 14, 1745506518778992. [Google Scholar] [CrossRef] [PubMed]
- Anthony, E.Y.; Caserta, M.P.; Singh, J.; Chen, M.Y.M. Adnexal Masses in Female Pediatric Patients. Am. J. Roentgenol. 2012, 198, W426–W431. [Google Scholar] [CrossRef] [PubMed]
- Bagolan, P.; Riovosecchi, M.; Giorlandino, C.; Bilancioni, E.; Nahom, A.; Zaccara, A.; Trucchi, A.; Ferro, F. Prenatal diagnosis and clinicaloutcome of ovariancysts. J. Pediatr. Surg. 1992, 27, 879–881. [Google Scholar] [CrossRef]
- Brandt, M.L.; Luks, F.I.; Filiatrault, D.; Garel, L.; Desjardins, J.G.; Youssef, S. Surgical indications in antenatally diagnosed ovarian cysts. J. Pediatr. Surg. 1991, 26, 276–282. [Google Scholar] [CrossRef]
- Sakala, E.P.; Leon, Z.A.; Rouse, G.A. Management of antenatally diagnosed fetal ovarian cysts. Obstet. Gynecol. Surv. 1991, 46, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, A.E.; Minneci, P.C.; Deans, K.J. Ovary-sparing surgery for benign pediatric ovarian masses. Curr. Opin. Pediatr. 2019, 31, 386–390. [Google Scholar] [CrossRef]
- Brandt, M.L.; Helmrath, M.A. Ovarian cysts in infants and children. Semin. Pediatr. Surg. 2005, 14, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Esposito, C.; Garipoli, V.; Di Matteo, G.; De Pasquale, M. Laparoscopic management of ovarian cysts in newborns. Surg. Endosc. 1998, 12, 1152–1154. [Google Scholar] [CrossRef] [PubMed]
- Takayasu, H.; Masumoto, K.; Tanaka, N.; Aiyoshi, T.; Sasaki, T.; Ono, K.; Chiba, F.; Urita, Y.; Shinkai, T. A clinical review of ovarian tumors in children and adolescents. Pediatr. Surg. Int. 2020, 36, 701–709. [Google Scholar] [CrossRef]
- Zhang, W.; Lei, P.; Dong, X.; Men, X. Advances in tumor markers of ovarian cancer for early diagnosis. Indian J. Cancer 2014, 51 (Suppl. S3), 72–76. [Google Scholar] [CrossRef]
- Cronen, P.W.; Nagaraj, H.S. Ovarian tumors in children. South. Med. J. 1988, 81, 464–468. [Google Scholar] [CrossRef]
- Oue, T.; Uehara, S.; Sasaki, T.; Nose, S.; Saka, R.; Yamanaka, H.; Ueno, T.; Tazuke, Y.; Okuyama, H. Treatment and ovarian preservation in children with ovarian tumors. J. Pediatr. Surg. 2015, 50, 2116–2118. [Google Scholar] [CrossRef]
- Hermans, A.J.; Kluivers, K.B.; Wijnen, M.H.; Bulten, J.; Massuger, L.F.; Coppus, S. Diagnosis and Treatment of Adnexal Masses in Children and Adolescents. Obstet. Gynecol. 2015, 125, 611–615. [Google Scholar] [CrossRef]
- Heo, S.H.; Kim, J.W.; Shin, S.S.; Jeong, S.I.; Lim, H.S.; Choi, Y.D.; Lee, K.H.; Kang, W.D.; Jeong, Y.Y.; Kang, H.K. Review of ovarian tumors in children and adolescents: Radiologic-pathologic correlation. Radiographics 2014, 34, 2039–2055. [Google Scholar] [CrossRef]
- Banlı-Cesur, I.; Tanrıdan-Okcu, N.; Özçelik, Z. Ovarian masses in children and adolescents: Analysis on 146 patients. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101901. [Google Scholar] [CrossRef]
- Dasgupta, R.; Renaud, E.; Goldin, A.; Baird, R.; Cameron, D.B.; Arnold, M.A.; Karen, A.; Diefenbach, K.A.; Gosain, A.; Grabowski, J.; et al. Ovarian torsion in pediatric and adolescent patients: A systematic review. J. Pediatr. Surg. 2018, 53, 1387–1391. [Google Scholar] [CrossRef]
- Esposito, C.; Coppola, V.; Del Conte, F.; Cerulo, M.; Esposito, G.; Farina, A.; Crocetto, F.; Castagnetti, M.; Settimi, A.; Escolino, M. Near-Infraredfluorescenceimagingusingindocyanine green (ICG): Emergingapplications in pediatricurology. J. Pediatr. Urol. 2020, 16, 700–707. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Right Side | Laparoscopic | Robotic | ICG- Technology | Benign Lesion | Malignant Lesions | |
|---|---|---|---|---|---|---|---|
| Neonates (G1) | 111 | 73 | 111 | 0 | 6 | 111 | 0 |
| Adolescents (G2) | 36 | 18 | 28 | 8 | 14 | 30 | 6 |
| Newborns | Teenagers | |
|---|---|---|
| Conversion to open surgery * | 0 | 0 |
| Mass excision | 80 | 30 |
| Positive tumor makers | - | 6 |
| - Benign Lesions | 3 (10%) | |
| - Malignant Lesions | 4 (66%) | |
| Complications after surgery | 0 | 0 |
| Needs of re-interventions | 0 | 0 |
| Mean operative time before ICG system | 51.4 min | 53.2 min |
| Mean operative time after ICG system | 47.2 min | 37.2 min |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciro, E.; Vincenzo, C.; Mariapina, C.; Fulvia, D.C.; Vincenzo, B.; Giorgia, E.; Roberto, C.; Lepore, B.; Castagnetti, M.; Califano, G.; et al. Review of a 25-Year Experience in the Management of Ovarian Masses in Neonates, Children and Adolescents: From Laparoscopy to Robotics and Indocyanine Green Fluorescence Technology. Children 2022, 9, 1219. https://doi.org/10.3390/children9081219
Ciro E, Vincenzo C, Mariapina C, Fulvia DC, Vincenzo B, Giorgia E, Roberto C, Lepore B, Castagnetti M, Califano G, et al. Review of a 25-Year Experience in the Management of Ovarian Masses in Neonates, Children and Adolescents: From Laparoscopy to Robotics and Indocyanine Green Fluorescence Technology. Children. 2022; 9(8):1219. https://doi.org/10.3390/children9081219
Chicago/Turabian StyleCiro, Esposito, Coppola Vincenzo, Cerulo Mariapina, Del Conte Fulvia, Bagnara Vincenzo, Esposito Giorgia, Carulli Roberto, Benedetta Lepore, Marco Castagnetti, Gianluigi Califano, and et al. 2022. "Review of a 25-Year Experience in the Management of Ovarian Masses in Neonates, Children and Adolescents: From Laparoscopy to Robotics and Indocyanine Green Fluorescence Technology" Children 9, no. 8: 1219. https://doi.org/10.3390/children9081219