
Outcome of Open Reduction Alone or with Concomitant Bony Procedures for Developmental Dysplasia of the Hip (DDH)

 ,
,
Abstract
:1. Introduction
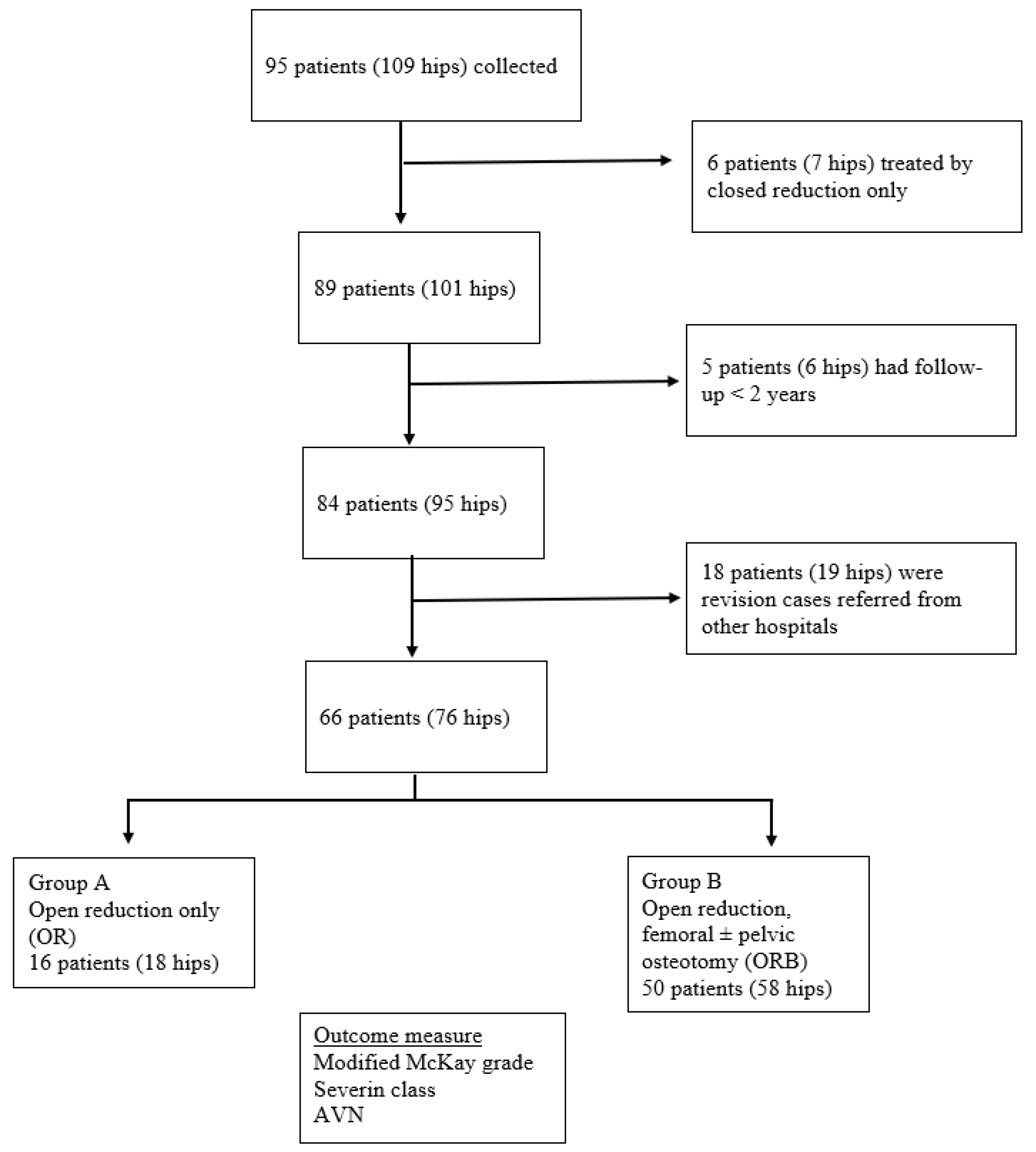
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boo, N.; Rajaram, T. Congenital dislocation of hips in Malaysian neonates. Singapore Med. J. 1989, 30, 71–368. [Google Scholar] [PubMed]
- Kotlarsky, P.; Haber, R.; Bialik, V.; Eidelman, M. Developmental dysplasia of the hip: What has changed in the last 20 years? World J. Orthop. 2015, 6, 886–901. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.F.; Kim, Y.-J. Surgical management of pediatric developmental dysplasia of the hip. J. Am. Acad. Orthop. Surg. 2016, 24, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Vaquero-Picado, A.; González-Morán, G.; Garay, E.G.; Moraleda, L. Developmental dysplasia of the hip: Update of management. EFORT Open Rev. 2019, 4, 548–556. [Google Scholar] [CrossRef]
- Holman, J.; Carroll, K.L.; Murray, K.A.; MacLeod, L.M.; Roach, J.W. Long-term follow-up of open reduction surgery for developmental dislocation of the hip. J. Pediatr. Orthop. 2012, 32, 121–124. [Google Scholar] [CrossRef]
- Weinstein, S.L.; Mubarak, S.J.; Wenger, D.R. Developmental hip dysplasia and dislocation: Part II. J. Bone Joint Surg. 2003, 85, 2024–2035. [Google Scholar] [CrossRef]
- Bhuyan, B.K. Outcome of one-stage treatment of developmental dysplasia of hip in older children. Indian J. Orthop. 2012, 46, 548–555. [Google Scholar] [CrossRef]
- Varner, K.E.; Incavo, S.J.; Haynes, R.J.; Dickson, J.A. Surgical treatment of developmental hip dislocation in children aged 1 to 3 years: A mean 18-year, 9-month follow-up study. Orthopedics 2010, 33, 1–5. [Google Scholar] [CrossRef]
- Yorgancıgil, H.; Aslan, A.; Demirci, D.; Atay, T. Effect of Age and Surgical Procedure on Clinical and Radiological Outcomes in Children with Developmental Dysplasia of the Hip: A Comparative Study. J. Acad. Res. Med. 2016, 6, 177–182. [Google Scholar] [CrossRef]
- Kothari, A.; Grammatopoulos, G.; Hopewell, S.; Theologis, T. How does bony surgery affect results of anterior open reduction in walking-age children with developmental hip dysplasia? Clin. Orthop. Relat. Res. 2016, 474, 1199–1208. [Google Scholar] [CrossRef]
- Wu, K.-W.; Wang, T.-M.; Huang, S.-C.; Kuo, K.N.; Chen, C.-W. Analysis of osteonecrosis following Pemberton acetabuloplasty in developmental dysplasia of the hip: Long-term results. J. Bone Joint Surg. 2010, 92, 2083–2094. [Google Scholar] [CrossRef] [PubMed]
- Asim, A.; Saw, A.; Nawar, M. Treatment of Developmental Dysplasia of the Hip: Shortand Mid-term Outcome. Malay. Orthop. J. 2011, 5, 17–20. [Google Scholar]
- Klisic, P.; Jankovic, L. Combined procedure of open reduction and shortening of the femur in treatment of congenital dislocation of the hips in older children. Clin. Orthop. Relat. Res. 1976, 119, 60–69. [Google Scholar] [CrossRef]
- Salter, R.B. Role of innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip in the older child. J. Bone Joint Surg. 1966, 48, 1413–1439. [Google Scholar] [CrossRef] [PubMed]
- Pemberton, P.A. Pericapsular osteotomy of the ilium for treatment of congenital subluxation and dislocation of the hip. J. Bone Joint Surg. 1965, 47, 65–86. [Google Scholar] [CrossRef] [PubMed]
- Mckay, D.W. A comparison of the innominate and the pericapsular osteotomy in the treatment of congenital dislocation of the hip. Clin. Orthop. Relat. Res. 1974, 98, 124–132. [Google Scholar] [CrossRef]
- Severin, E. Contribution to the knowledge of congenital dislocation of the hip joint. Acta Chir. Scand. 1941, 84, 163. [Google Scholar]
- Bucholz, R. Patterns of ischemic necrosis of the proximal femur in nonoperatively treated congenital hip disease. In The Hip Proceedings of the Sixth Open Scientific Meeting of the Hip Society; CV Mosby: Maryland Heights, MI, USA, 1978; pp. 43–63. [Google Scholar]
- El-Sayed, M.M. Single-stage open reduction, Salter innominate osteotomy, and proximal femoral osteotomy for the management of developmental dysplasia of the hip in children between the ages of 2 and 4 years. J. Pediatr. Orthop. B 2009, 18, 188–196. [Google Scholar] [CrossRef]
- Forlin, E.; Da Cunha, L.A.M.; Figueiredo, D.C. Treatment of developmental dysplasia of the hip after walking age with open reduction, femoral shortening, and acetabular osteotomy. Orthop. Clin. 2006, 37, 149–160. [Google Scholar] [CrossRef]
- Galpin, R.D.; Roach, J.; Wenger, D.; Herring, J.; Birch, J. One-stage treatment of congenital dislocation of the hip in older children, including femoral shortening. J. Bone Joint Surg. 1989, 71, 734–741. [Google Scholar] [CrossRef]
- Karakaş, E.; Baktir, A.; Argün, M.; Türk, C.Y. One-stage treatment of congenital dislocation of the hip in older children. J. Pediatr. Orthop. 1995, 15, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Umer, M.; Nawaz, H.; Kasi, P.M.; Ahmed, M. Outcome of triple procedure in older children with developmental dysplasia of hip (DDH). J. Pak. Med. Assoc. 2007, 57, 591. [Google Scholar] [PubMed]
- Li, Y.; Hu, W.; Xun, F.; Lin, X.; Li, J.; Yuan, Z.; Liu, Y.; Canavese, F.; Xu, H. Risk factors associated with unsatisfactory hip function in children with late-diagnosed developmental dislocation of the hip treated by open reduction. Orthop. Traumatol. Surg. Res. 2020, 106, 1373–1381. [Google Scholar] [CrossRef] [PubMed]
- Ning, B.; Yuan, Y.; Yao, J.; Zhang, S.; Sun, J. Analyses of outcomes of one-stage operation for treatment of late-diagnosed developmental dislocation of the hip: 864 hips followed for 3.2 to 8.9 years. BMC Musculoskelet. Disord. 2014, 15, 401. [Google Scholar] [CrossRef]
- Ganger, R.; Radler, C.; Petje, G.; Manner, H.M.; Kriegs-Au, G.; Grill, F. Treatment options for developmental dislocation of the hip after walking age. J. Pediatr Orthop. B. 2005, 14, 139–150. [Google Scholar] [CrossRef]
- Chen, Q.; Deng, Y.; Fang, B. Outcome of one-stage surgical treatment of developmental dysplasia of the hip in children from 1.5 to 6 years old. A retrospective study. Acta Orthop. Belg. 2015, 81, 375–383. [Google Scholar]
- Bursalı, A.; Tonbul, M. How are outcomes affected by combining the Pemberton and Salter osteotomies? Clin. Orthop. Relat. Res. 2008, 466, 837–846. [Google Scholar] [CrossRef]
- Eamsobhana, P.; Kamwong, S.; Sisuchinthara, T.; Jittivilai, T.; Keawpornsawan, K. The factor causing poor results in late developmental dysplasia of the hip (DDH). J. Med. Assoc. Thai. 2015, 98, S32–S37. [Google Scholar]
- Domzalski, M.; Synder, M. Avascular necrosis after surgical treatment for developmental dysplasia of the hip. Int. J. Orthop. 2004, 28, 65–68. [Google Scholar] [CrossRef]
- Kalamchi, A.; MacEwen, G.D. Avascular necrosis following treatment of congenital dislocation of the hip. J. Bone Joint Surg. 1980, 62, 876–888. [Google Scholar] [CrossRef]
- Kamath, S.U.; Bennet, G.C. Re-dislocation following open reduction for developmental dysplasia of the hip. Int. J. Orthop. 2005, 29, 191–194. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| OR (n = 16) | ORB (n = 50) | p-Value | |
|---|---|---|---|
| Age at surgery in years | |||
| (mean ± SD) | 1.5 ± 0.4 | 4.5 ± 2.5 | <0.05 |
| Age at final follow-up (mean ± SD) | 8.6 ± 4.6 | 13.0 ± 4.4 | <0.05 |
| Gender: N (%) | |||
| Male | 1 (1.5%) | 15 (22.7%) | 0.43 * |
| Female | 21 (41.2%) | 42 (63.6%) | |
| Laterality: N (%) | |||
| Left | 7 (10.6%) | 28 (10.6%) | 0.50 * |
| Right | 7 (56.9%) | 14 (21.2%) | |
| Bilateral | 2 (3.0 %) | 8 (12.1%) |
| Group | McKay Grading | Total | χ2 | p-Value | |
|---|---|---|---|---|---|
| Satisfactory | Unsatisfactory | ||||
| OR | 15 | 1 | 16 | ||
| (22.7%) | (1.5%) | (24.2%) | |||
| ORB | 33 | 17 | 50 | 4.71 | <0.05 * |
| (50.0% | (25.8%) | (75.8%) | |||
| Total | 48 | 18 | 66 | ||
| (72.7%) | (27.3%) | ||||
| Severin Class | |||||
| Satisfactory | Unsatisfactory | ||||
| OR | 11 | 5 | 16 | ||
| (16.7%) | (7.6%) | (24.2%) | |||
| ORB | 36 | 14 | 50 | 0.06 | 0.80 |
| (54.5%) | (21.2%) | (75.8%) | |||
| Total | 47 | 19 | 66 | ||
| (71.2%) | (28.8%) | ||||
| AVN | McKay Grading | Total | χ2 | p-Value | |
|---|---|---|---|---|---|
| Satisfactory | Unsatisfactory | ||||
| No AVN | 36 | 8 | 43 | ||
| (53.0%) | (12.1%) | (65.2%) | |||
| Grade 1 | 9 | 5 | 14 | 8.32 | <0.05 * |
| (13.6%) | (7.6%) | (21.2%) | |||
| Grade 2 | 4 (6.1%) | 3 (4.5%) | 7 (10.6%) | ||
| Grade 3 | 0 | 2 (3.0%) | 2 (3.0%) | ||
| Total | 48 | 18 | 66 | ||
| (72.7%) | (27.3%) | ||||
| Severin Class | |||||
| Satisfactory | Unsatisfactory | ||||
| No AVN | 36 | 7 | 43 | ||
| (54.5%) | (10.6%) | (65.2%) | |||
| Grade 1 | 6 | 8 | 14 | ||
| (9.1%) | (12.1%) | (21.2%) | 13.72 | <0.05 * | |
| Grade 2 | 5 | 2 | 7 | ||
| (7.6%) | (3.0%) | (10.6%) | |||
| Grade 3 | 0 | 2 | 2 | ||
| (3.0%) | (3.0%) | ||||
| Total | 47 | 19 | 66 | ||
| (71.2%) | (28.8%) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamil, K.; Saharuddin, R.; Abd Rasid, A.F.; Abd Rashid, A.H.; Ibrahim, S. Outcome of Open Reduction Alone or with Concomitant Bony Procedures for Developmental Dysplasia of the Hip (DDH). Children 2022, 9, 1213. https://doi.org/10.3390/children9081213
Jamil K, Saharuddin R, Abd Rasid AF, Abd Rashid AH, Ibrahim S. Outcome of Open Reduction Alone or with Concomitant Bony Procedures for Developmental Dysplasia of the Hip (DDH). Children. 2022; 9(8):1213. https://doi.org/10.3390/children9081213
Chicago/Turabian StyleJamil, Kamal, Rostam Saharuddin, Ahmad Fazly Abd Rasid, Abdul Halim Abd Rashid, and Sharaf Ibrahim. 2022. "Outcome of Open Reduction Alone or with Concomitant Bony Procedures for Developmental Dysplasia of the Hip (DDH)" Children 9, no. 8: 1213. https://doi.org/10.3390/children9081213