
From Fetal to Neonatal Neuroimaging in TORCH Infections: A Pictorial Review

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. TORCH
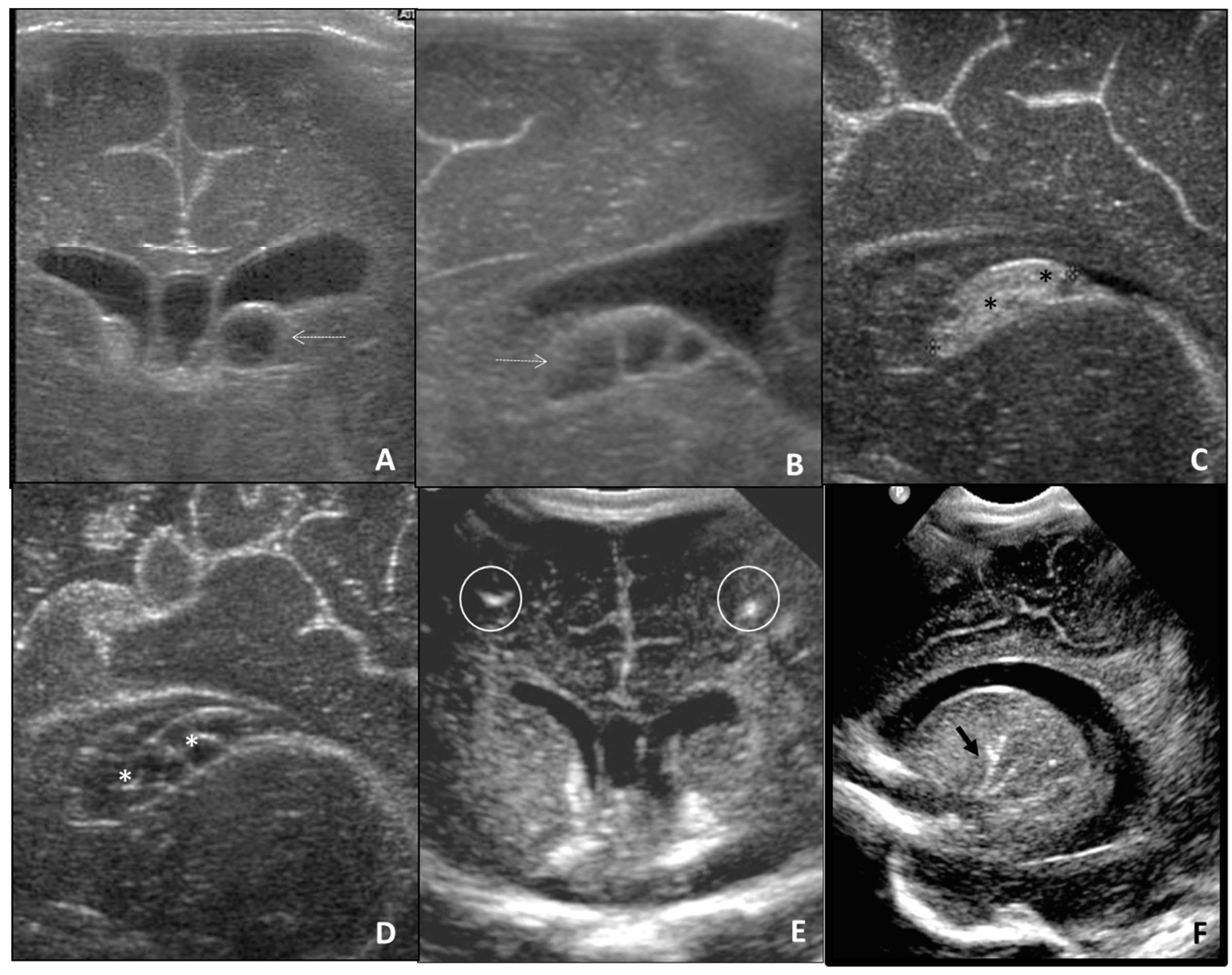
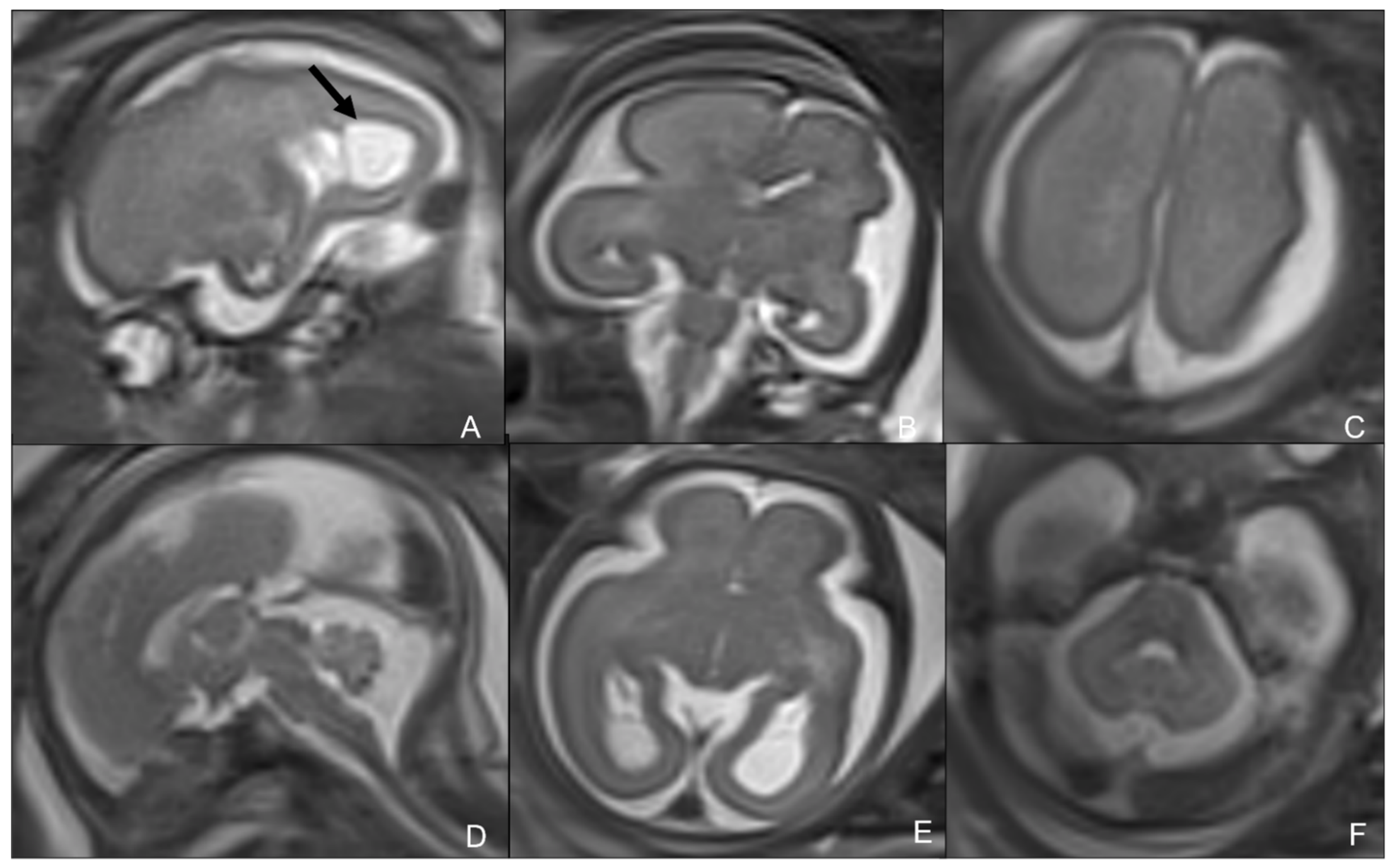
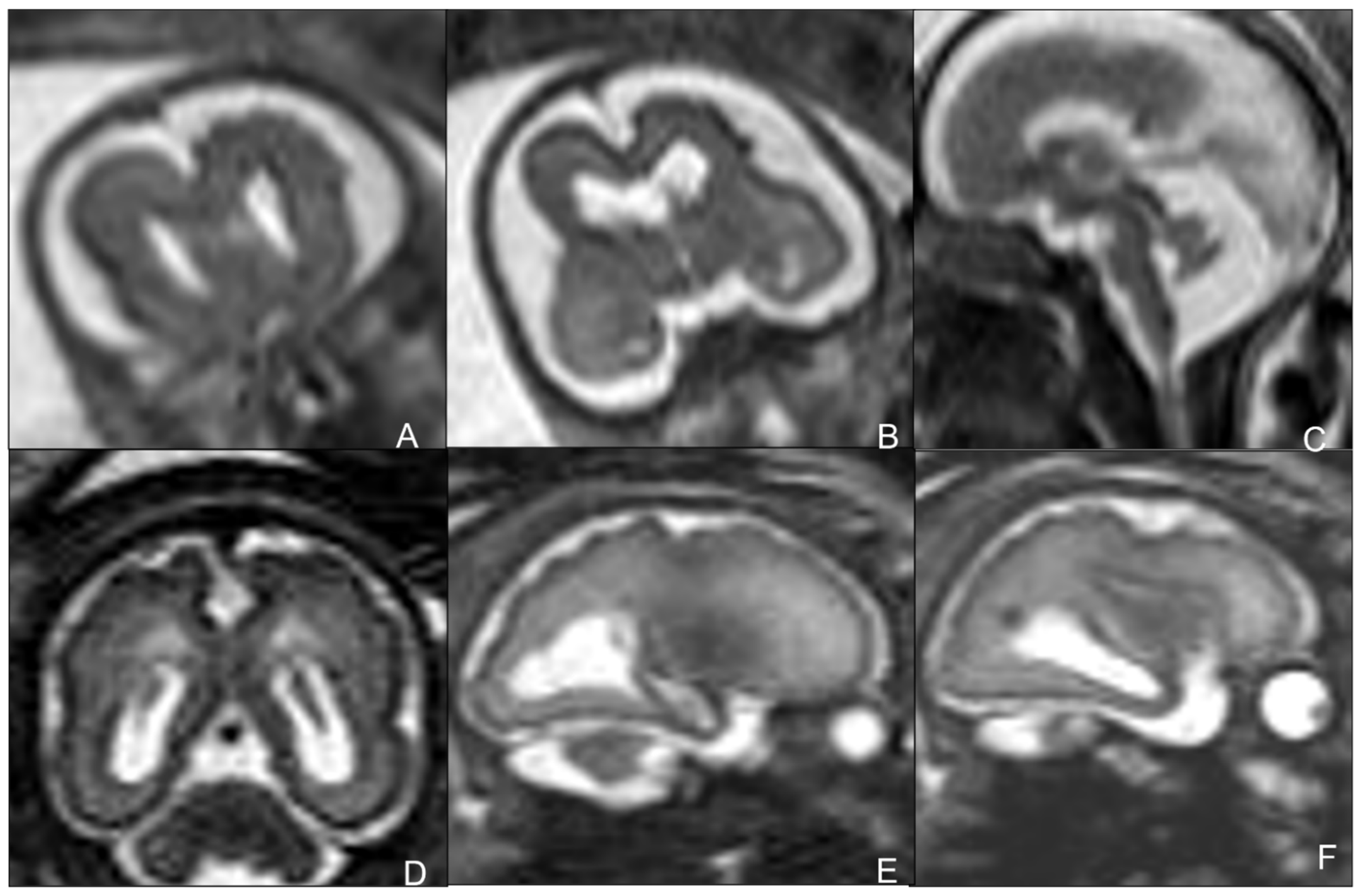
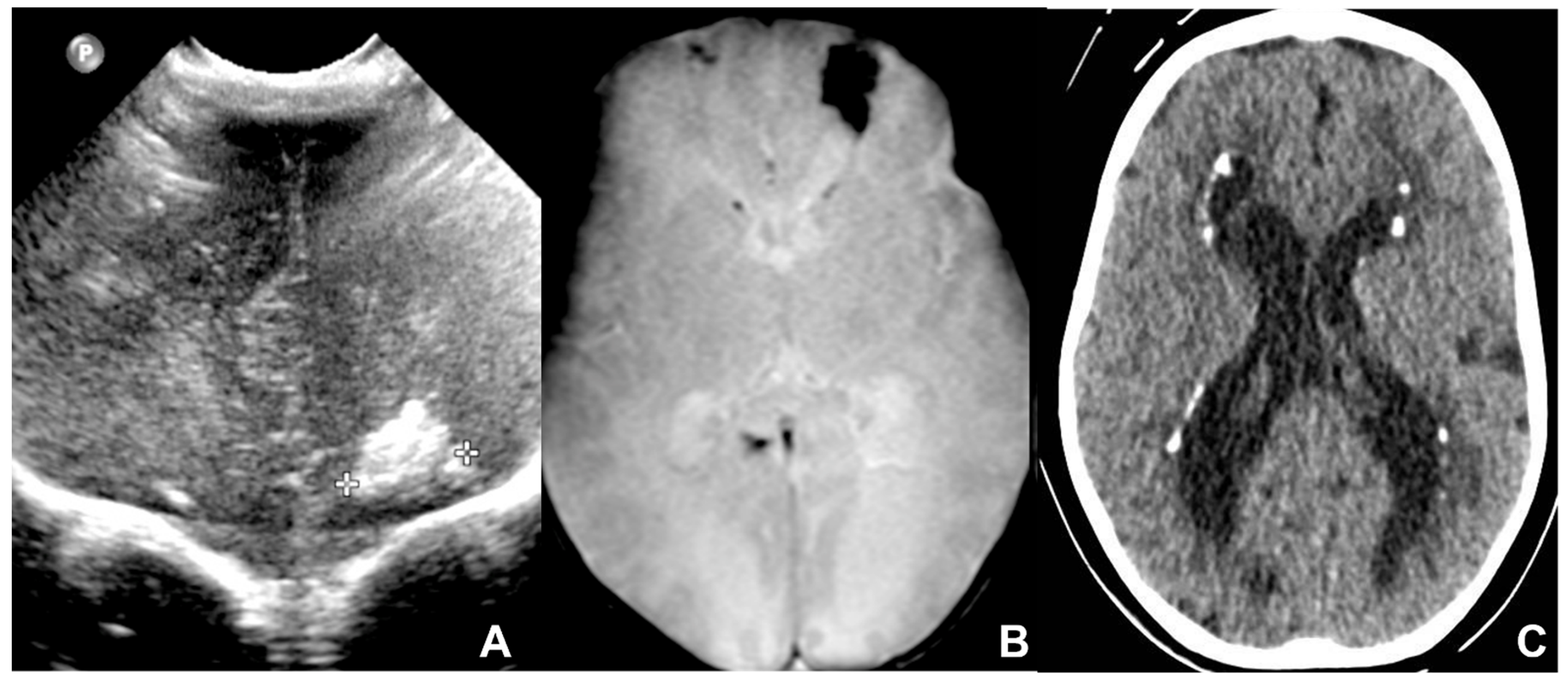
2.1. Cytomegalovirus Infection
2.2. Toxoplasmosis
2.3. Rubella
2.4. Herpes Simplex
2.5. Other and Emerging Viral Agents
Parvovirus
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CNS | central nervous system |
| TORCH | Toxoplasma gondii, others, rubella, cytomegalovirus, herpes |
| cUS | cerebral ultrasound |
| MR | magnetic resonance |
| cCMV | congenital cytomegalovirus |
| CMV | cytomegalovirus |
| WI | weighted image |
| GRE | gradient-echo |
| SWI | susceptibility-weighted imaging |
| CT | computed tomography |
| SEM | skin, eye, mouth |
| DWI | diffusion-weighted image |
| ASL | arterial spin labeling |
| HIV | human immunodeficiency virus |
| ZIKV | zika virus |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus-2 |
References
- Baldwin, S.; Whitley, R. Teratogen update: Intrauterine herpes simplex virus infection. Teratology 1989, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Megli, C.J.; Coyne, C.B. Infections at the maternal-fetal interface: An overview of pathogenesis and defense. Nat. Rev. Microbiol. 2022, 20, 67–82. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, J.P.; Richner, B.; Santy, K.; Lequin, M.H.; Poretti, A.; Filippi, C.G.; Huisman, T.A. Neuroimaging of pediatric intracranial infection—Part 2: TORCH, viral, fungal, and parasitic infections. J. Neuroimaging 2012, 22, e52–e63. [Google Scholar] [CrossRef] [PubMed]
- Stegmann, B.J.; Carey, J.C. TORCH Infections. Toxoplasmosis, Other (syphilis, varicella-zoster, parvovirus B19), Rubella, Cytomegalovirus (CMV), and Herpes infections. Curr. Womens Health Rep. 2002, 2, 253–258. [Google Scholar]
- Colonna, A.T.; Buonsenso, D.; Pata, D.; Salerno, G.; Chieffo, D.P.R.; Romeo, D.M.; Faccia, V.; Conti, G.; Molle, F.; Baldascino, A.; et al. Long-Term Clinical, Audiological, Visual, Neurocognitive and Behavioral Outcome in Children with Symptomatic and Asymptomatic Congenital Cytomegalovirus Infection Treated with Valganciclovir. Front. Med. 2020, 7, 268. [Google Scholar] [CrossRef]
- Maldonado, A.; Nizet, V.; Klein, J.O.; Remington, J.S.; Wilson, C.B. Current concepts of infections of the fetus and newborn infant. In Infectious Diseases of the Fetus and Newborn Infant, 7th ed.; Remington, J., Klein, J., Wilson, C., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2011; pp. 2–23. [Google Scholar]
- Barkovich, A.J.; Girard, N. Fetal brain infections. Childs Nerv. Syst. 2003, 19, 501–507. [Google Scholar] [CrossRef]
- Barkovich, A.; Raybaud, C. Pediatric Neuroimaging; LWW: Philadelphia, PA, USA, 2018. [Google Scholar]
- Manganaro, L.; Bernardo, S.; Antonelli, A.; Vinci, V.; Saldari, M.; Catalano, C. Fetal MRI of the central nervous system: State-of-the-art. Eur. J. Radiol. 2017, 93, 273–283. [Google Scholar] [CrossRef]
- Fink, K.R.; Thapa, M.M.; Ishak, G.E.; Pruthi, S. Neuroimaging of pediatric central nervous system cytomegalovirus infection. Radiographics 2010, 30, 1779–1796. [Google Scholar] [CrossRef]
- Vande Walle, C.; Keymeulen, A.; Schiettecatte, E.; Acke, F.; Dhooge, I.; Smets, K.; Herregods, N. Brain MRI findings in newborns with congenital cytomegalovirus infection: Results from a large cohort study. Eur. Radiol. 2021, 31, 8001–8010. [Google Scholar] [CrossRef]
- Diogo, M.C.; Glatter, S.; Binder, J.; Kiss, H.; Prayer, D. The MRI spectrum of congenital cytomegalovirus infection. Prenat. Diagn. 2020, 40, 110–124. [Google Scholar] [CrossRef]
- Giannattasio, A.; Bruzzese, D.; Di Costanzo, P.; Capone, E.; Romano, A.; D’Amico, A.; Bravaccio, C.; Grande, C.; Capasso, L.; Raimondi, F. Neuroimaging Profiles and Neurodevelopmental Outcome in Infants with Congenital Cytomegalovirus Infection. Pediatr. Infect. Dis. J. 2018, 37, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Gantt, S.; Bitnun, A.; Renaud, C.; Kakkar, F.; Vaudry, W. Diagnosis and management of infants with congenital cytomegalovirus infection. Paediatr. Child Health 2017, 22, 72–74. [Google Scholar] [CrossRef]
- Ssentongo, P.; Hehnly, C.; Birungi, P.; Roach, M.A.; Spady, J.; Fronterre, C.; Wang, M.; Murray-Kolb, L.E.; Al-Shaar, L.; Chinchilli, V.M.; et al. Congenital Cytomegalovirus Infection Burden and Epidemiologic Risk Factors in Countries with Universal Screening: A Systematic Review and Meta-analysis. JAMA Netw. Open. 2021, 4, e2120736. [Google Scholar] [CrossRef] [PubMed]
- Chiopris, G.; Veronese, P.; Cusenza, F.; Procaccianti, M.; Perrone, S.; Daccò, V.; Colombo, C.; Esposito, S. Congenital Cytomegalovirus Infection: Update on Diagnosis and Treatment. Microorganisms 2020, 8, 1516. [Google Scholar] [CrossRef]
- Barkovich, A.J.; Lindan, C.E. Congenital cyomegalovirus infection of the brain: Imaging analysis and embryologic considerations. AJNR Am. J. Neuroradiol. 1994, 15, 703–715. [Google Scholar] [PubMed]
- De Vrijer, B.; Crowley, D.; Cosma, D.; Muscedere, G.; Hammond, R. Congenital CMV infection presenting with massive intracerebral hemorrhage. Clin. Neuropathol. 2021, 40, 341–346. [Google Scholar] [CrossRef]
- Averill, L.W.; Kandula, V.V.; Akyol, Y.; Epelman, M. Fetal Brain Magnetic Resonance Imaging Findings In Congenital Cytomegalovirus Infection with Postnatal Imaging Correlation. Semin. Ultrasound CT MRI 2015, 36, 476–486. [Google Scholar] [CrossRef]
- Lanari, M.; Capretti, M.G.; Lazzarotto, T.; Gabrielli, L.; Rizzollo, S.; Mostert, M.; Manzoni, P. Neuroimaging in CMV congenital infected neonates: How and when. Early Hum. Dev. 2012, 88 (Suppl. S2), S3–S5. [Google Scholar] [CrossRef]
- Keymeulen, A.; De Leenheer, E.; Casaer, A.; Cossey, V.; Herregods, N.; Laroche, S.; Mahieu, L.; Van Mol, C.; Vanhaesebrouck, S.; Walle, C.V.; et al. Cranial ultrasound and MRI: Complementary or not in the diagnostic assessment of children with congenital CMV infection? Eur. J. Pediatr. 2021, 181, 911–920. [Google Scholar] [CrossRef]
- Smiljkovic, M.; Renaud, C.; Tapiero, B.; Lamarre, V.; Kakkar, F. Head ultrasound, CT or MRI? The choice of neuroimaging in the assessment of infants with congenital cytomegalovirus infection. BMC Pediatr. 2019, 19, 180. [Google Scholar] [CrossRef]
- Escobar Castellanos, M.; de la Mata Navazo, S.; Carrón Bermejo, M.; García Morín, M.; Martín, Y.R.; Lozano, J.S.; Herrero, M.M.; Valderrama, E.B.; de Castro, P.C.; López, M.V. Association between neuroimaging findings and neurological sequelae in patients with congenital cytomegalovirus infection. Neurologia 2019, 8. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, H.; Takahashi, H.; Kanda, Y.; Kitaoka, K.; Hara, M. Long-term Outcomes of Cochlear Implantation in Children with Congenital Cytomegalovirus Infection. Otol. Neurotol. 2017, 38, e190–e194. [Google Scholar] [CrossRef] [PubMed]
- Miller, T.E.; Weisz, B.; Yinon, Y.; Weissbach, T.; De Castro, H.; Avnet, H.; Hoffman, C.; Katorza, E.; Lipitz, S. Congenital Cytomegalovirus Infection Following Second and Third Trimester Maternal Infection Is Associated with Mild Childhood Adverse Outcome Not Predicted by Prenatal Imaging. J. Pediatric Infect. Dis. Soc. 2021, 10, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Zuber, P.; Jacquier, P. Epidemiology of toxoplasmosis: Worldwide status. Schweiz. Med. Wochenschr. 1995, 65, 19S–22S. [Google Scholar]
- Dunn, D.; Wallon, M.; Peyron, F.; Petersen, E.; Peckham, C.; Gilbert, R. Mother-to-child transmission of toxoplasmosis: Risk estimates for clinical counselling. Lancet 1999, 353, 1829–1833. [Google Scholar] [CrossRef]
- Martin, S. Congenital Toxoplasmosis. Neonatal Netw. 2001, 20, 23–30. [Google Scholar] [CrossRef]
- Orphanet: Toxoplasmosi Congenita. Available online: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=IT&Expert=858 (accessed on 13 December 2021).
- Capobiango, J.D.; Breganó, R.M.; Navarro, I.T.; Rezende Neto, C.P.; Casella, A.M.B.; Mori, F.M.R.L.; Pagliari, S.; Inoue, I.T.; Reiche, E.M.V. Congenital toxoplasmosis in a reference center of Paraná, Southern Brazil. Braz. J. Infect. Dis. 2014, 18, 364–371. [Google Scholar] [CrossRef]
- Sarvi, S.; Chegeni, T.N.; Sharif, M.; Montazeri, M.; Hosseini, S.A.; Amouei, A.; Hosseininejad, Z.; Anvari, D.; Saberi, R.; Gohardehi, S.; et al. Congenital toxoplasmosis among Iranian neonates: A systematic review and meta-analysis. Epidemiol Health 2019, 41, e2019021. [Google Scholar] [CrossRef]
- Rostami, A.; Karanis, P.; Fallahi, S. Advances in serological, imaging techniques and molecular diagnosis of Toxoplasma gondii infection. Infection 2018, 46, 303–315. [Google Scholar] [CrossRef]
- Diebler, C.; Dusser, A.; Dulac, O. Congenital toxoplasmosis. Clinical and neuroradiological evaluation of the cerebral lesions. Neuroradiology 1985, 27, 125–130. [Google Scholar] [CrossRef]
- Jacquemard F Ultrasonographic signs of congenital toxoplasmosis. Arch. Pediatr. 2003, 10 (Suppl. S1), 35–38.
- Lago, E.; Baldisserotto, M.; Filho, J.H.; Santiago, D.; Jungblut, R. Agreement between ultrasonography and computed tomography in detecting intracranial calcifications in congenital toxoplasmosis. Clin. Radiol. 2007, 62, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Triulzi, F.; Baldoli, C.; Parazzini, C.; Righini, A. Perinatal Neuroradiology; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Available online: https://www.orpha.net/data/patho/GB/uk-toxo.pdf (accessed on 13 December 2021).
- Peyron, F.; L’ollivier, C.; Mandelbrot, L.; Wallon, M.; Piarroux, R.; Kieffer, F.; Hadjadj, E.; Paris, L.; Garcia-Meric, P. Maternal and Congenital Toxoplasmosis: Diagnosis and Treatment Recommendations of a French Multidisciplinary Working Group. Pathogens 2019, 8, 24. [Google Scholar] [CrossRef] [PubMed]
- Dunay, I.R.; Gajurel, K.; Dhakal, R.; Liesenfeld, O.; Montoya, J.G. Treatment of Toxoplasmosis: Historical Perspective, Animal Models, and Current Clinical Practice. Clin. Microbiol. Rev. 2018, 31, e00057-17. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Pata, D.; Turriziani Colonna, A.; Iademarco, M.; De Santis, M.; Masini, L.; Conti, G.; Molle, F.; Baldascino, A.; Acampora, A.; et al. Spyramicine and Trimethoprim-Sulfamethoxazole Combination to Prevent Mother-To-Fetus Transmission of Toxoplasma gondii Infection in Pregnant Women: A 28-Years Single-center Experience. Pediatr. Infect. Dis. J. 2022, 41, e223–e227. [Google Scholar] [CrossRef]
- Valentini, P.; Buonsenso, D.; Barone, G.; Serranti, D.; Calzedda, R.; Ceccarelli, M.; Speziale, D.; Ricci, R.; Masini, L. Spiramycin/cotrimoxazole versus pyrimethamine/sulfonamide and spiramycin alone for the treatment of toxoplasmosis in pregnancy. J. Perinatol. 2015, 35, 90–94. [Google Scholar] [CrossRef]
- McLeod, R.; Boyer, K.; Karrison, T.; Kasza, K.; Swisher, C.; Roizen, N.; Jalbrzikowski, J.; Remington, J.; Heydemann, P.; Noble, A.G.; et al. Outcome of treatment for congenital toxoplasmosis, 1981–2004: The National Collaborative Chicago-Based, Congenital Toxoplasmosis Study. Clin. Infect. Dis. 2006, 42, 1383–1394. [Google Scholar] [CrossRef]
- Ghanaat, M.; Soleiman, A. Congenital rubella syndrome: Clinical and imaging features. J. Pediatr. Neurol. 2020, 18, 251–257. [Google Scholar] [CrossRef]
- Duszak, R.S. Congenital rubella syndrome—Major review. Optometry 2009, 80, 36–43. [Google Scholar] [CrossRef]
- Dontigny, L.; Arsenault, M.-Y.; Martel, M.-J.; Clinical Practice Obstetrics Committee. Rubella in pregnancy. J. Obstet. Gynaecol. Can. 2008, 30, 152–158. [Google Scholar] [CrossRef]
- Lambert, N.; Strebel, P.; Orenstein, W.; Icenogle, J.; Poland, G.A. Rubella. Lancet 2015, 385, 2297–2307. [Google Scholar] [CrossRef]
- Chapter 9: Manual for the Laboratory-Based Surveillance of Measles, Rubella, and Congenital Rubella Syndrome. Available online: https://www.who.int/publications/m/item/chapter-9-manual-for-the-laboratory-based-surveillance-of-measles-rubella-and-congenital-rubella-syndrome (accessed on 21 March 2022).
- Robertson, S.E.; Featherstone, D.A.; Gacic-Dobo, M.; Hersh, B.S. Rubella and congenital rubella syndrome: Global update. Rev. Panam. Salud Publica 2003, 14, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Agbede, O.O.; Adeyemi, O.O.; Olatinwo, A.W. Significance of IgG-Avidity in Antenatal Rubella Diagnosis. J. Family Reprod. Health 2013, 7, 131–137. [Google Scholar] [PubMed]
- Epelman, M.; Daneman, A.; Blaser, S.I.; Ortiz-Neira, C.; Konen, O.; Jarrín, J.; Navarro, O.M. Differential diagnosis of intracranial cystic lesions at head US: Correlation with CT and MR imaging. Radiographics 2006, 26, 173–196. [Google Scholar] [CrossRef]
- Beltinger, C.; Saule, H. Sonography of subependymal cysts in congenital rubella syndrome. Eur. J. Pediatr. 1988, 148, 206–207. [Google Scholar] [CrossRef]
- Yamashita, Y.; Matsuishi, T.; Murakami, Y.; Shoji, H.; Hashimoto, T.; Utsunomiya, H.; Araki, H. Neuroimaging findings (ultrasonography, CT, MRI) in 3 infants with congenital rubella syndrome. Pediatr. Radiol. 1991, 21, 547–549. [Google Scholar] [CrossRef]
- Sawlani, V.; Shankar, J.J.S.; White, C. Magnetic resonance imaging findings in a case of congenital rubella encephalitis. Can. J. Infect. Dis. Med. Microbiol. 2013, 24, e122–e123. [Google Scholar] [CrossRef]
- Townsend, J.J.; Wolinsky, J.S.; Baringer, J.R. The neuropathology of progressive rubella panencephalitis of late onset. Brain 1976, 99, 81–90. [Google Scholar] [CrossRef]
- Townsend, J.J.; Stroop, W.G.; Baringer, J.R.; Wolinsky, J.S.; McKerrow, J.H.; Berg, B.O. Neuropathology of progressive rubella panencephalitis after childhood rubella. Neurology 1982, 32, 185–190. [Google Scholar] [CrossRef]
- Marquez, L.; Levy, M.L.; Munoz, F.M.; Palazzi, D.L. A report of three cases and review of intrauterine herpes simplex virus infection. Pediatr. Infect. Dis. J. 2011, 30, 153–157. [Google Scholar] [CrossRef]
- Purewal, R.; Costello, L.; Garlapati, S.; Mitra, S.; Mitchell, M.; Moffett, K.S. Congenital Herpes Simplex Virus in the Newborn: A Diagnostic Dilemma. J. Pediatric Infect. Dis. Soc. 2016, 5, e21–e23. [Google Scholar] [CrossRef] [PubMed]
- James, S.H.; Kimberlin, D.W. Neonatal herpes simplex virus infection: Epidemiology and treatment. Clin. Perinatol. 2015, 42, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Samies, N.L.; James, S.H. Prevention and treatment of neonatal herpes simplex virus infection. Antivir. Res. 2020, 176, 104721. [Google Scholar] [CrossRef] [PubMed]
- Baskin, H.J.; Hedlund, G. Neuroimaging of herpesvirus infections in children. Pediatr. Radiol. 2007, 37, 949–963. [Google Scholar] [CrossRef]
- Pinninti, S.G.; Kimberlin, D.W. Neonatal herpes simplex virus infections. Semin. Perinatol. 2018, 42, 168–175. [Google Scholar] [CrossRef]
- Kubota, T.; Ito, M.; Maruyama, K.; Kato, Y.; Miyajima, Y.; Ogawa, A.; Kuno, K.; Okumura, A.; Watanabe, K. Serial diffusion-weighted imaging of neonatal herpes encephalitis: A case report. Brain Dev. 2007, 29, 171–173. [Google Scholar] [CrossRef]
- Okanishi, T.; Yamamoto, H.; Hosokawa, T.; Ando, N.; Nagayama, Y.; Hashimoto, Y.; Maihara, T.; Goto, T.; Kubota, T.; Kawaguchi, C.; et al. Diffusion-weighted MRI for early diagnosis of neonatal herpes simplex encephalitis. Brain Dev. 2015, 37, 423–431. [Google Scholar] [CrossRef]
- Wong, A.M.; Yeh, C.H.; Lin, J.J.; Liu, H.L.; Chou, I.J.; Lin, K.L.; Wang, H.S. Arterial spin-labeling perfusion imaging of childhood encephalitis: Correlation with seizure and clinical outcome. Neuroradiology 2018, 60, 961–970. [Google Scholar] [CrossRef]
- Soares, B.P.; Provenzale, J.M. Imaging of Herpesvirus Infections of the CNS. AJR Am. J. Roentgenol. 2016, 206, 39–48. [Google Scholar] [CrossRef]
- Muller, W.J. Treatment of perinatal viral infections to improve neurologic outcomes. Pediatr. Res. 2017, 81, 162–169. [Google Scholar] [CrossRef]
- Parmar, H.; Ibrahim, M. Pediatric intracranial infections. Neuroimaging Clin. N. Am. 2012, 22, 707–725. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.F.; Sobel, J.; Mazaki-Tovi, S.; Kusanovic, J.P.; Vaisbuch, E.; Kim, S.K.; Uldbjerg, N.; Romero, R. Listeriosis in human pregnancy: A systematic review. J. Perinat. Med. 2011, 39, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, I.; Garcia, J.; Meyers, M.L.; Feygin, T.; Bulas, D.I.; Mirsky, D.M. Imaging of congenital central nervous system infections. Pediatr Radiol 2018, 48, 513–523. [Google Scholar] [CrossRef] [PubMed]
- De Vries, L.S. Viral infections and the neonatal brain. Semin. Pediatric Neurol. 2019, 32, 100769. [Google Scholar] [CrossRef] [PubMed]
- Penner, J.; Hernstadt, H.; Burns, J.E.; Randell, P.; Lyall, H. Stop, think SCORTCH: Rethinking the traditional ‘TORCH’ screen in an era of re-emerging syphilis. Arch. Dis. Child. 2021, 106, 117–124. [Google Scholar] [CrossRef]
- Zare Mehrjardi, M.; Poretti, A.; Huisman, T.A.; Werner, H.; Keshavarz, E.; Araujo Júnior, E. Neuroimaging findings of congenital Zika virus infection: A pictorial essay. Jpn. J. Radiol. 2017, 35, 89–94. [Google Scholar] [CrossRef]
- Levine, D.; Jani, J.C.; Castro-Aragon, I.; Cannie, M. How Does Imaging of Congenital Zika Compare with Imaging of Other TORCH Infections? Radiology 2017, 285, 744–761. [Google Scholar] [CrossRef]
- Henderson, A.D.; Ventura, C.V.; Huisman, T.A.G.M.; Meoded, A.; Hazin, A.N.; van der Linden, V.; de Lima Petribu, N.C.; May, W.N. Characterization of Visual Pathway Abnormalities in Infants with Congenital Zika Syndrome Using Computed Tomography and Magnetic Resonance Imaging. J. Neuroophthalmol. 2021, 41, e598–e605. [Google Scholar] [CrossRef]
- Oladapo, O.T.; Souza, J.P.; De Mucio, B.; de León, R.G.P.; Perea, W.; Gülmezoglu, A.M. WHO interim guidance on pregnancy management in the context of Zika virus infection. Lancet Glob Health. 2016, 4, e510–e511. [Google Scholar] [CrossRef]
- Muldoon, K.M.; Fowler, K.B.; Pesch, M.H.; Schleiss, M.R. SARS-CoV-2: Is it the newest spark in the TORCH? J. Clin. Virol. 2020, 127, 104372. [Google Scholar] [CrossRef]
- Karimi-Zarchi, M.; Neamatzadeh, H.; Dastgheib, S.A.; Abbasi, H.; Mirjalili, S.R.; Behforouz, A.; Ferdosian, F.; Bahrami, R. Vertical Transmission of Coronavirus Disease 19 (COVID-19) from Infected Pregnant Mothers to Neonates: A Review. Fetal Pediatr. Pathol. 2020, 39, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Dashraath, P.; Wong, J.L.J.; Lim, M.X.K.; Lim, L.M.; Li, S.; Biswas, A.; Choolani, M.; Mattar, C.; Su, L.L. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am. J. Obstet. Gynecol. 2020, 222, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Pettirosso, E.; Giles, M.; Cole, S.; Rees, M. COVID-19 and pregnancy: A review of clinical characteristics, obstetric outcomes and vertical transmission. Aust. N. Z. J. Obstet. Gynaecol. 2020, 60, 640–659. [Google Scholar] [CrossRef]
- Favre, G.; Mazzetti, S.; Gengler, C.; Bertelli, C.; Schneider, J.; Laubscher, B.; Capoccia, R.; Pakniyat, F.; Ben Jazia, I.; Eggel-Hort, B.; et al. Decreased Fetal Movements: A Sign of Placental SARS-CoV-2 Infection with Perinatal Brain Injury. Viruses 2021, 13, 2517. [Google Scholar] [CrossRef] [PubMed]
- Miesbach, W.; Makris, M. COVID-19: Coagulopathy, risk of thrombosis, and the rationale for anticoagulation. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620938149. [Google Scholar] [CrossRef]
- Campi, F.; Longo, D.; Bersani, I.; Savarese, I.; Lucignani, G.; Haass, C.; Paolino, M.C.; Vadalà, S.; De Liso, P.; Di Capua, M.; et al. Neonatal Cerebral Venous Thrombosis following Maternal SARS-CoV-2 Infection in Pregnancy. Neonatology 2022, 25, 268–272. [Google Scholar] [CrossRef]
- Shuffrey, L.C.; Firestein, M.R.; Kyle, M.H.; Fields, A.; Alcántara, C.; Amso, D.; Austin, J.; Bain, J.M.; Barbosa, J.; Bence, M.; et al. Association of Birth During the COVID-19 Pandemic with Neurodevelopmental Status at 6 Months in Infants with and without In Utero Exposure to Maternal SARS-CoV-2 Infection. JAMA Pediatr. 2022, 176, e215563. [Google Scholar] [CrossRef]
- Cursi, L.; Calo Carducci, F.I.; Chiurchiu, S.; Romani, L.; Stoppa, F.; Lucignani, G.; Russo, C.; Longo, D.; Perno, C.F.; Cecchetti, C.; et al. Severe COVID-19 Complicated by Cerebral Venous Thrombosis in a Newborn Successfully Treated with Remdesivir, Glucocorticoids, and Hyperimmune Plasma. Int. J. Environ. Res. Public Health 2021, 18, 13201. [Google Scholar] [CrossRef]
- Questions and Answers: COVID-19 Vaccines and Pregnancy. Available online: https://apps.who.int/iris/bitstream/handle/10665/351855/WHO-2019-nCoV-FAQ-Pregnancy-Vaccines-2022.1-eng.pdf (accessed on 13 December 2021).
- Young, N.S.; Brown, K.E. Parvovirus B19. N. Engl. J. Med. 2004, 350, 586–597. [Google Scholar] [CrossRef]
- Enders, M.; Weidner, A.; Zoellner, I.; Searle, K.; Enders, G. Fetal morbidity and mortality after acute human parvovirus B19 infection in pregnancy: Prospective evaluation of 1018 cases. Prenat. Diagn. 2004, 24, 513–518. [Google Scholar] [CrossRef]
- Isumi, H.; Nunoue, T.; Nishida, A.; Takashima, S. Fetal brain infection with human parvovirus B19. Pediatr. Neurol. 1999, 21, 661–663. [Google Scholar] [CrossRef]
- Craze, J.L.; Salisbury, A.J.; Pike, M.G. Prenatal stroke associated with maternal parvovirus infection. Dev. Med. Child Neurol. 1996, 38, 84–85. [Google Scholar] [PubMed]
- Glenn, O.A.; Bianco, K.; Barkovich, A.J.; Callen, P.W.; Parer, J.T. Fetal cerebellar hemorrhage in parvovirus-associated non-immune hydrops fetalis. J. Matern. Fetal Neonatal Med. 2007, 20, 769–772. [Google Scholar] [CrossRef]
- Schulert, G.S.; Walsh, W.F.; Weitkamp, J.-H. Polymicrogyria and congenital parvovirus b19 infection. AJP Rep. 2011, 1, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Pistorius, L.R.; Smal, J.; De Haan, T.R.; Page-Christiaens, G.C.; Verboon-Maciolek, M.; Oepkes, D.; De Vries, L.S. Disturbance of cerebral neuronal migration following congenital parvovirus B19 infection. Fetal Diagn. Ther. 2008, 24, 491–494. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Calcifications | Ventricles | Cortex | White Matter | Other | |
|---|---|---|---|---|---|
| CMV | Periventricular, punctate | Ventriculomegaly | Polymicrogyria, lissencephaly, schizencephaly | Periventriculardelayed myelination, Germinolitic cysts, Temporal cyst | Hemorrhage (rare). Cerebellum hypoplasia |
| TOXOPLASMOSIS | Extensive and most commonly in basal ganglia, thalami, cerebral cortex, and periventricular tissue | Hydrocephalus, Hydranencephaly (rare) | Microcephaly, Macrocephaly, Porencephaly | Microcephaly, Macrocephaly, Porencephaly | Aqueduct occlusion/stenosis secondary to epididymitis |
| HSV | Less common | Ventriculomegaly, hydranencephaly | Microcephaly, Porencephaly | Microcephaly, Porencephaly | Corpus callosum agenesis, microphthalmia, meningeal involvement |
| RUBELLA | Basal ganglia and periventricular | Ventriculomegaly | Polymicrogyria | Extensive multifocal white matter hyperintensity, mainly in the frontal lobes | Subependymal cysts, leucostriate vasculopathy, myelination delay, cerebellar hypoplasia |
| PARVOVIRUS | Less common | Ventricular dilatation | Ischemic and hemorrhagic strokes, Polymicrogyria (rare), heterotopia (rare) | Ischemic and hemorrhagic strokes | Cerebral vasculitis, hydrops |
| SARS-COVID19 | / | Intraventricular hemorrhage | Parenchymal hemorrhage, cerebral ischemia | Periventricular leukomalacia, parenchymal hemorrhage, cerebral ischemia | Cerebral vein thrombosis |
| ZIKA VIRUS | Corticomedullary junction in frontal and parietal lobes, less frequently in the thalamus, basal ganglia, cortex, and periventricular regions | Ventriculomegaly | Microcephaly, polymicrogyria, gyral simplification, pachygyria-lissencephaly, opercular dysplasia, heterotopia | Microcephaly, delayed myelination, dysmyelination, hypoplasia of corticospinal tracts | Pseudocysts in the occipital horns, asymmetrical microphthalmia, cataracts, optic nerve atrophy, coloboma, lens defects, herniation of the orbital fat into the cranial vault, thin spinal cord |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucignani, G.; Guarnera, A.; Rossi-Espagnet, M.C.; Moltoni, G.; Antonelli, A.; Figà Talamanca, L.; Carducci, C.; Calo Carducci, F.I.; Napolitano, A.; Gandolfo, C.; et al. From Fetal to Neonatal Neuroimaging in TORCH Infections: A Pictorial Review. Children 2022, 9, 1210. https://doi.org/10.3390/children9081210
Lucignani G, Guarnera A, Rossi-Espagnet MC, Moltoni G, Antonelli A, Figà Talamanca L, Carducci C, Calo Carducci FI, Napolitano A, Gandolfo C, et al. From Fetal to Neonatal Neuroimaging in TORCH Infections: A Pictorial Review. Children. 2022; 9(8):1210. https://doi.org/10.3390/children9081210
Chicago/Turabian StyleLucignani, Giulia, Alessia Guarnera, Maria Camilla Rossi-Espagnet, Giulia Moltoni, Amanda Antonelli, Lorenzo Figà Talamanca, Chiara Carducci, Francesca Ippolita Calo Carducci, Antonio Napolitano, Carlo Gandolfo, and et al. 2022. "From Fetal to Neonatal Neuroimaging in TORCH Infections: A Pictorial Review" Children 9, no. 8: 1210. https://doi.org/10.3390/children9081210