
Comparison of Health Literacy Assessment Tools among Beijing School-Aged Children



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Settings
2.2. Measures
2.2.1. Health Literacy Assessment Tools
2.2.2. Upstream Factors
2.2.3. Developmental Outcomes
2.3. Statistical Analysis
2.4. Missing Data
3. Results
3.1. Sample Characteristics
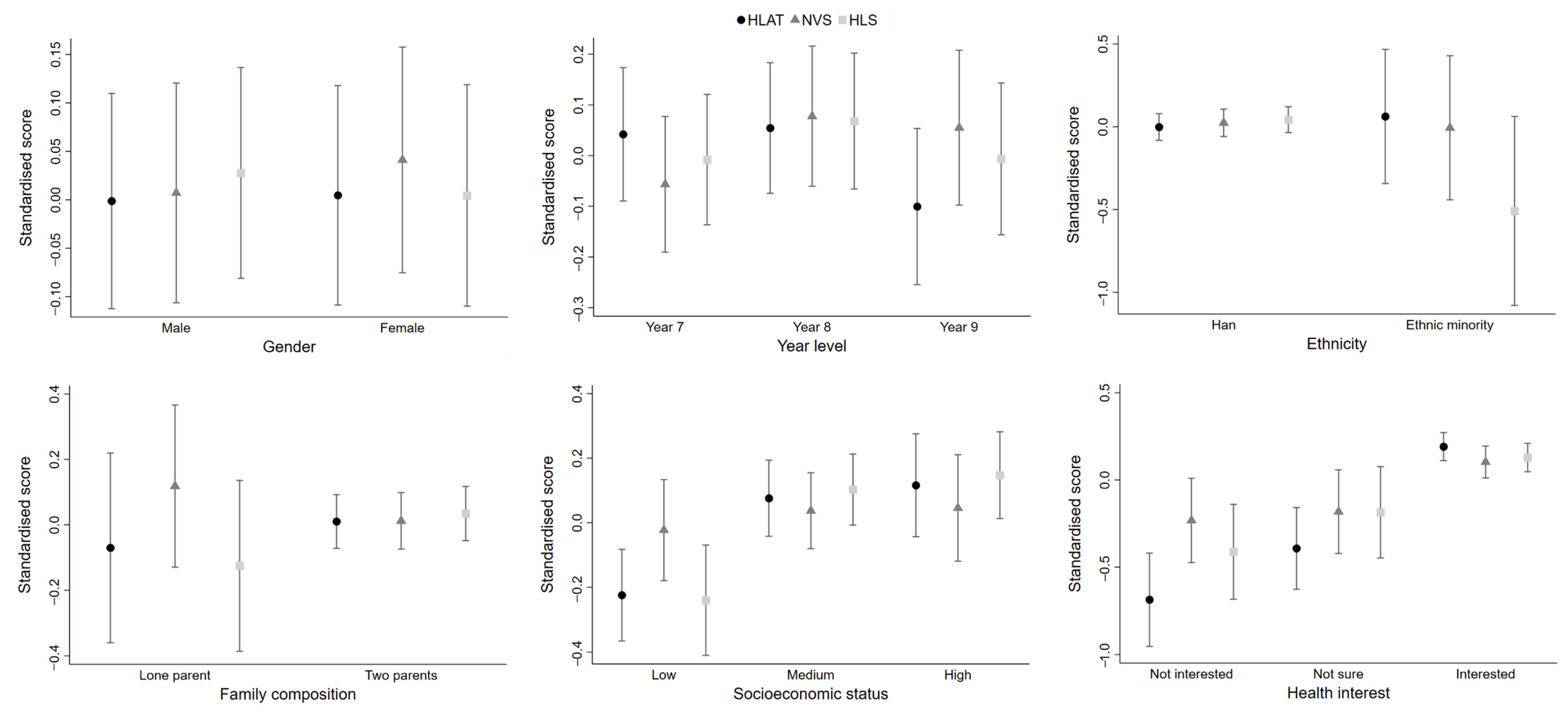
3.2. Distribution of Health Literacy by Socio-Demographics and Individual Characteristics
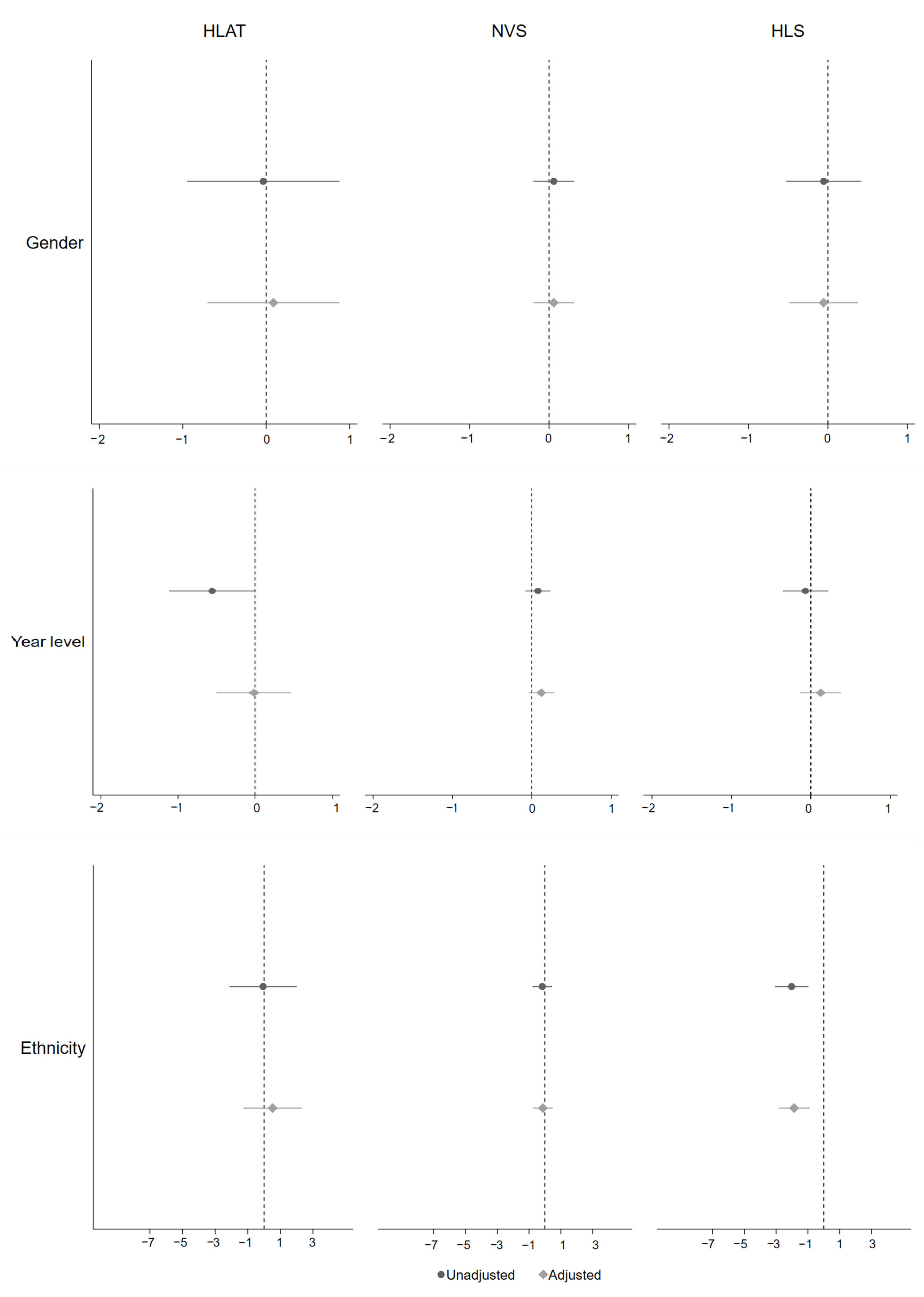
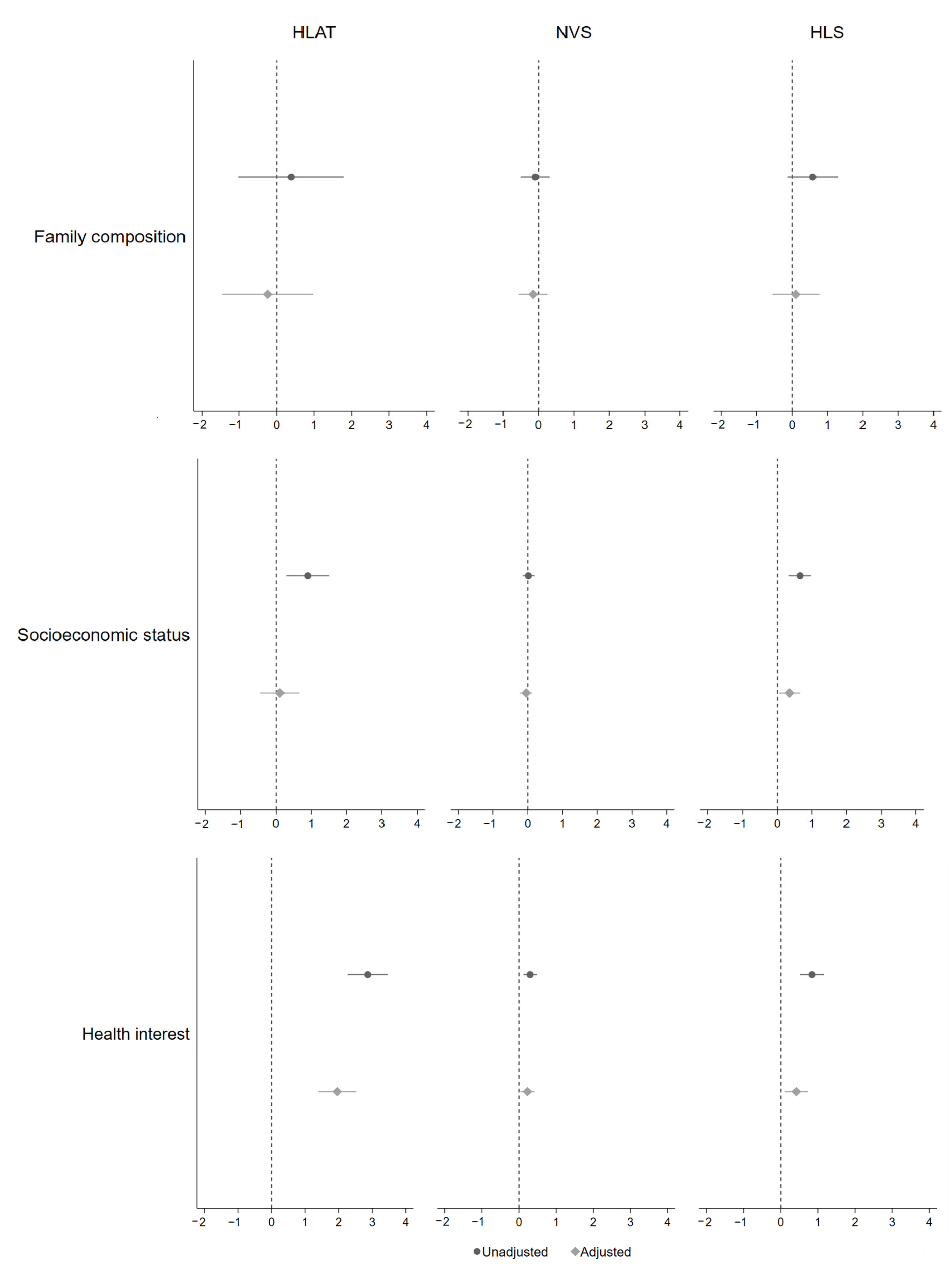
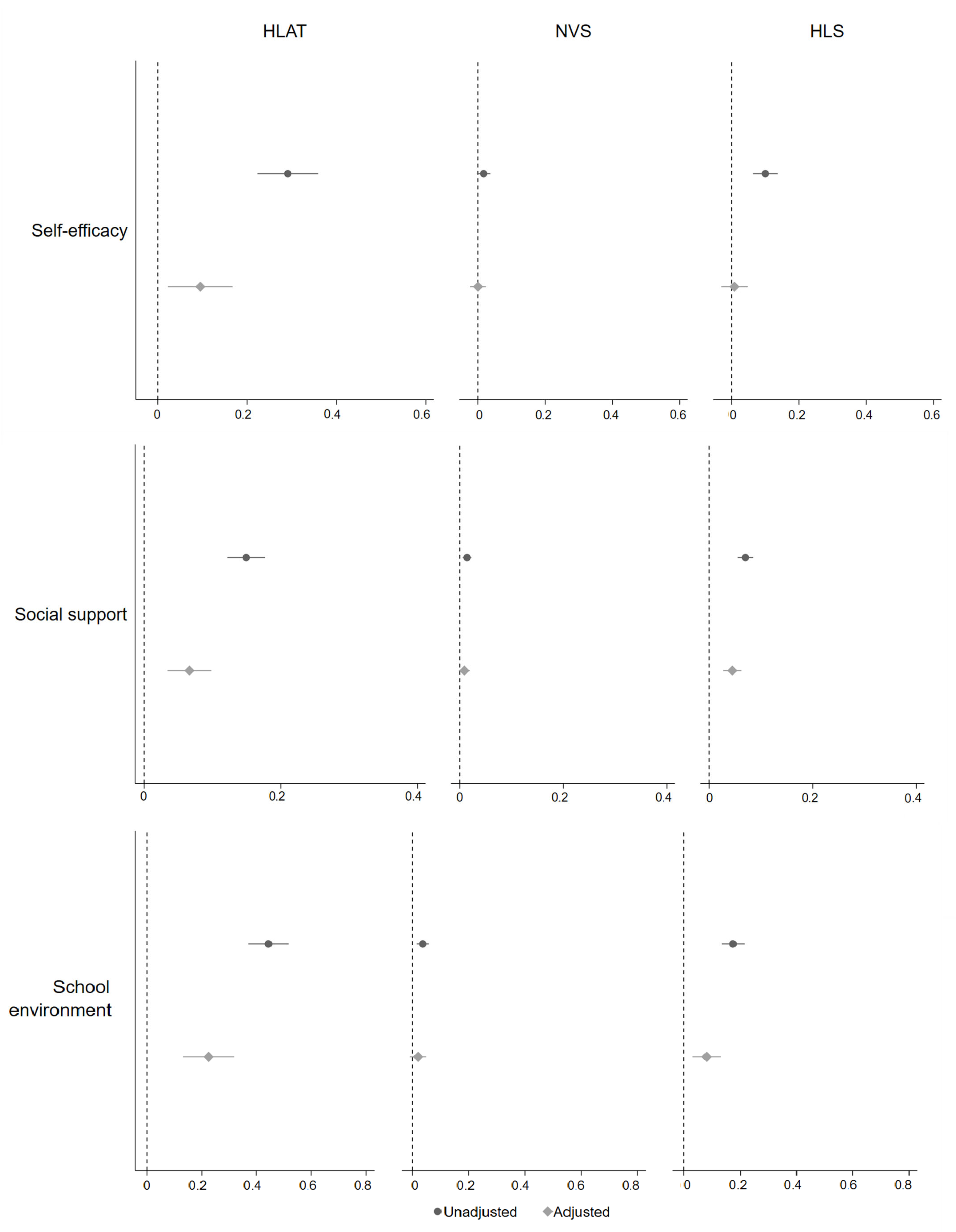
3.3. Association between Health Literacy and Its Upstream Factors
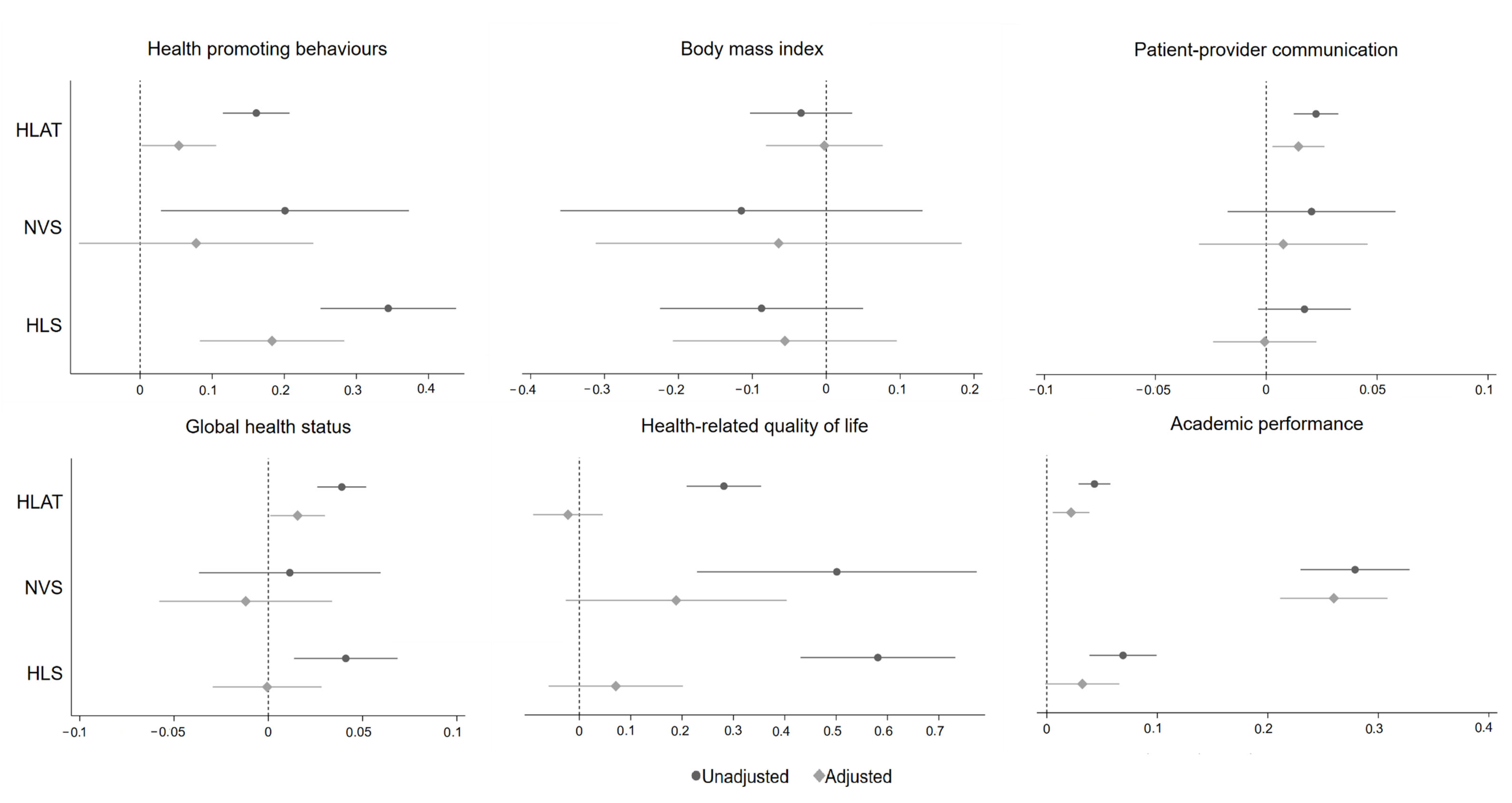
3.4. Association between Health Literacy and Developmental Outcomes
4. Discussion
4.1. Summary of Key Findings
4.2. Strengths and Limitations
4.3. Implications and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Construct | Measure | Example Item | Scoring | Coding | α |
|---|---|---|---|---|---|
| Upstream factors | |||||
| Gender | A single-item measurement of students’ sex | Are you male or female? | Gender was self-reported by students themselves. | Binary: male; female | - |
| Year level | A single-item measurement of students’ year level | What Year level are you in at school? | Year level was self-reported by students themselves. | Categorical: Year 7; Year 8; Year 9 | - |
| Ethnicity | A single-item measurement of students’ ethnicity | What is your ethnicity? | Ethnicity was self-reported by students themselves. | Binary: Han; ethnic minorities | - |
| Family composition | A single-item measurement of students’ family structure | Think of where you live most of the time. Who usually lives there with you? | Family structure was self-reported by students themselves. Intact families were defined as those in which participants indicated residing in a household with both biological parents, whereas other types of families were defined as those in which participants indicated residing in a household with either one of their parents, foster parents, step parents, a relative or who were living in a shared care institution. | Binary: Intact; other types | - |
| Family socioeconomic status | The 4-item Family Affluence Scale (FAS) | Do you have your own bedroom for yourself? | Students self-reported family affluence in terms of the number(s) of cars, computers, bedrooms and family holidays. The FAS total score range was 0–7. | Ordinal: low (0–3); medium (4–5); and high (6–7) | - |
| Health interest | A single-item measurement of students’ interest in health topics | How interested are you in learning about health? | Students self-reported interests in health topics. | Ordinal: not interested; not sure; interested | - |
| Self-efficacy | The 10-item General Self-Efficacy Scale (GSES) | I can always manage to solve difficult problems if I try hard enough. | Students self-reported personal belief in the ability to cope with a variety of challenges in life. The GSES total score range was 10–40. | Continuous | 0.89 |
| Social support | The 12-item Multidimensional Scale of Perceived Social Support (MSPSS) | My family really tries to help me. | Students self-reported support from family, friends and significant others. The MSPSS total score range was 12–84. | Continuous | 0.93 |
| School environment | The 10-item School Environment Scale (SES) | I feel safe at my school. | Students self-reported feelings about opportunities and rewards for pro-social involvement at school. The SES total score range was 10–40. | Continuous | 0.88 |
| Health literacy | |||||
| Health literacy | The 8-item Health Literacy Assessment Tool (HLAT-8) | When I have questions on diseases or health problems (e.g., headache, back pain, sport injury), I know where I can find information on these issues. | Students self-reported their ability to access, understand, evaluate, and communicate health information in everyday life. The HLAT total score range was 0–37. | Continuous | 0.79 |
| The 6-item Newest Vital Sign (NVS) | How many calories (Cal) will you consume if you ate the whole package of ice-cream? | Students completed a performance-based measure for reading comprehension and numeracy. The NVS total score range was 0–6. | Continuous | 0.54 | |
| The 16-item Health Literacy Survey (HLS) | On a scale from very easy to very difficult, how easy would you say it is to find information on treatments of illnesses that concern you? | Students self-reported their ability to access, understand, evaluate, and communicate health information in everyday life. The HLS total score range was 0–16. | Continuous | 0.82 | |
| Developmental outcomes | |||||
| Health-promoting behaviours | Five-item health behaviours | During the past 7 days, how often did you have breakfast? | Students self-reported five items derived from the global school-based student health survey, including breakfast eating, teeth brushing, cigarette smoking, alcohol drinking and physical activity. | Continuous | - |
| Body mass index | Two-item measurement of height and weight | How tall do you think you are? | Students self-reported their height and weight. Body mass index (BMI) was calculated using the following formula: BMI = weight (kg)/height (m)2. | Continuous | - |
| Global health status | A single-item measurement of students’ health status | In general, would you say your health is? | Global health status was self-reported by students themselves. | Ordinal: fair or poor; good; excellent or very good | - |
| Health-related quality of life | The 10-item KIDSCREEN-10 | Have you felt fit and well? | Students self-reported their health-related quality of life in the last week. | Continous | 0.79 |
| Health service use | A single-item measurement of students’ patient-provider communication | How many times have you raised a question during your doctor’s appointment in the last 12 months? | Students self-reported their frequency of patient-provider communication over the last 12 months. | Continuous | - |
| Academic performance | A single-item measurement of students’ academic performance | Think of your marks at school, if putting them all together, where were your marks like last year? | Students self-reported their academic performance in the last year. | Continuous | - |
| Variable | Frequency (%) |
|---|---|
| Gender | 0 |
| Year level | 0 |
| Ethnicity | 0 |
| Family composition | 1 (0.2) |
| Socioeconomic status | 0 |
| Health interest | 0 |
| Self-efficacy | 6 (0.9) |
| Social support | 6 (0.9) |
| School environment | 6 (0.9) |
| HLAT | 1 (0.2) |
| NVS | 17 (2.6) |
| HLS | 50 (7.7) |
| Health-promoting behaviours | 1 (0.2) |
| Body mass index | 23 (3.5) |
| Patient-provider communication | 26 (4.0) |
| Global health status | 0 |
| Health-related quality of life | 0 |
| Academic performance | 2 (0.3) |
| Variable | HLAT | NVS | HLS |
|---|---|---|---|
| Mean (±SD) | Mean (±SD) | Mean (±SD) | |
| Gender | |||
| Male | 26.36 (6.14) | 3.61 (1.69) | 13.75 (3.03) |
| Female | 26.31 (5.57) | 3.68 (1.57) | 13.67 (2.82) |
| Year | |||
| Year 7 | 26.78 (5.75) | 3.50 (1.61) | 13.70 (2.79) |
| Year 8 | 26.51 (5.39) | 3.74 (1.59) | 13.83 (2.93) |
| Year 9 | 25.65 (6.48) | 3.69 (1.71) | 13.62 (3.12) |
| Ethnicity | |||
| Han | 26.34 (5.89) | 3.64 (1.63) | 13.81 (2.83) |
| Ethnic minority | 26.27 (5.96) | 3.60 (1.73) | 11.97 (4.21) |
| Family composition | |||
| Lone parent | 25.99 (6.79) | 3.78 (1.62) | 13.18 (3.23) |
| Two parents | 26.38 (5.76) | 3.63 (1.64) | 13.78 (2.90) |
| Socioeconomic status | |||
| Low | 25.15 (5.79) | 3.61 (1.66) | 12.89 (3.44) |
| Medium | 26.70 (5.90) | 3.67 (1.63) | 14.00 (2.75) |
| High | 26.96 (5.82) | 3.63 (1.64) | 14.12 (2.47) |
| Health interest | |||
| Not interested | 22.01 (7.16) | 3.27 (1.73) | 12.51 (3.52) |
| Not sure | 24.13 (5.85) | 3.30 (1.68) | 13.09 (3.47) |
| Interested | 27.52 (5.12) | 3.76 (1.60) | 14.04 (2.65) |
| HLAT | NVS | HLS | ||||
|---|---|---|---|---|---|---|
| Unadjusted β (95% CI) | Adjusted β (95% CI) | Unadjusted β (95% CI) | Adjusted β (95% CI) | Unadjusted β (95% CI) | Adjusted β (95% CI) | |
| Gender | −0.04 (−0.95, 0.88) | 0.09 (−0.71, 0.88) | 0.06 (−0.2, 0.32) | 0.06 (−0.2, 0.32) | −0.05 (−0.53, 0.42) | −0.06 (−0.49, 0.38) |
| Year level | −0.56 (−1.11, 0.00) | −0.02 (−0.50, 0.47) | 0.08 (−0.08, 0.24) | 0.12 (−0.03, 0.28) | −0.06 (−0.35, 0.22) | 0.13 (−0.13, 0.38) |
| Ethnicity | −0.06 (−2.12, 2.01) | 0.52 (−1.26, 2.31) | −0.16 (−0.78, 0.45) | −0.13 (−0.73, 0.48) | −2.02 (−3.08, −0.97) | −1.86 (−2.84, −0.89) |
| Family composition | 0.38 (−1.02, 1.79) | −0.24 (−1.46, 0.98) | −0.09 (−0.50, 0.31) | −0.15 (−0.56, 0.25) | 0.58 (−0.14, 1.3) | 0.11 (−0.56, 0.78) |
| Socioeconomic status | 0.89 (0.28, 1.51) | 0.10 (−0.45, 0.65) | 0.01 (−0.16, 0.19) | −0.05 (−0.23, 0.13) | 0.65 (0.33, 0.97) | 0.35 (0.05, 0.65) |
| Health interest | 2.86 (2.27, 3.46) | 1.96 (1.39, 2.53) | 0.30 (0.12, 0.48) | 0.23 (0.04, 0.42) | 0.84 (0.51, 1.17) | 0.42 (0.11, 0.73) |
| Self-efficacy | 0.29 (0.22, 0.36) | 0.10 (0.02, 0.17) | 0.02 (0.00, 0.04) | 0.00 (−0.02, 0.02) | 0.10 (0.06, 0.14) | 0.01 (−0.03, 0.05) |
| Social support | 0.15 (0.12, 0.18) | 0.07 (0.03, 0.10) | 0.01 (0.01, 0.02) | 0.01 (0.00, 0.02) | 0.07 (0.05, 0.09) | 0.04 (0.03, 0.06) |
| School environment | 0.44 (0.37, 0.52) | 0.23 (0.13, 0.32) | 0.04 (0.01, 0.06) | 0.02 (−0.01, 0.05) | 0.17 (0.13, 0.22) | 0.08 (0.03, 0.13) |
| Health-Promoting Behaviours | Body Mass Index | Patient-Provider Communication | ||||
|---|---|---|---|---|---|---|
| Unadjusted β (95% CI) | Adjusted β (95% CI) | Unadjusted β (95% CI) | Adjusted β (95% CI) | Unadjusted β (95% CI) | Adjusted β (95% CI) | |
| HLAT | 0.16 (0.12, 0.21) | 0.05 (0.00, 0.11) | −0.03 (−0.10, 0.04) | 0.00 (−0.08, 0.08) | 0.02 (0.01, 0.03) | 0.01 (0.00, 0.03) |
| NVS | 0.20 (0.03, 0.37) | 0.08 (−0.08, 0.24) | −0.11 (−0.36, 0.13) | −0.06 (−0.31, 0.18) | 0.02 (−0.02, 0.06) | 0.01 (−0.03, 0.05) |
| HLS | 0.34 (0.25, 0.44) | 0.18 (0.08, 0.28) | −0.09 (−0.22, 0.05) | −0.06 (−0.21, 0.10) | 0.02 (0, 0.04) | 0.00 (−0.02, 0.02) |
| Global Health Status | Health-Related Quality of Life | Academic Performance | ||||
| Unadjusted β (95% CI) | Adjusted β (95% CI) | Unadjusted β (95% CI) | Adjusted β (95% CI) | Unadjusted β (95% CI) | Adjusted β (95% CI) | |
| HLAT | 0.04 (0.03, 0.05) | 0.02 (0.00, 0.03) | 0.28 (0.21, 0.35) | −0.02 (−0.09, 0.05) | 0.04 (0.03, 0.06) | 0.02 (0.01, 0.04) |
| NVS | 0.01 (−0.04, 0.06) | −0.01 (−0.06, 0.03) | 0.50 (0.23, 0.77) | 0.19 (−0.03, 0.40) | 0.28 (0.23, 0.33) | 0.26 (0.21, 0.31) |
| HLS | 0.04 (0.01, 0.07) | 0.00 (−0.03, 0.03) | 0.58 (0.43, 0.73) | 0.07 (−0.06, 0.20) | 0.07 (0.04, 0.10) | 0.03 (0.00, 0.07) |
References
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Paakkari, L.; Okan, O. COVID-19: Health literacy is an underestimated problem. Lancet Public Health 2020, 5, e249–e250. [Google Scholar] [CrossRef]
- Sentell, T.; Vamos, S.; Okan, O. Interdisciplinary Perspectives on Health Literacy Research Around the World: More Important Than Ever in a Time of COVID-19; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2020. [Google Scholar]
- Habersaat, K.B.; Betsch, C.; Danchin, M.; Sunstein, C.R.; Böhm, R.; Falk, A.; Brewer, N.T.; Omer, S.B.; Scherzer, M.; Sah, S. Ten considerations for effectively managing the COVID-19 transition. Nat. Hum. Behav. 2020, 4, 677–687. [Google Scholar] [CrossRef]
- Rajah, R.; Hassali, M.A.A.; Murugiah, M.K. A systematic review of the prevalence of limited health literacy in Southeast Asian countries. Public Health 2019, 167, 8–15. [Google Scholar] [CrossRef]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [Green Version]
- The Lancet Child Adolescent Health. Universal health coverage and the forgotten generation. Lancet Child Adolesc. Health 2019, 3, 749. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Kasemsap, K. Challenges and implications of health literacy in global health care. In Advanced Methodologies and Technologies in Medicine and Healthcare; IGI Global: Pennsylvania, PA, USA, 2019; pp. 185–197. [Google Scholar]
- World Health Organisation. Shanghai Declaration on Promoting Health in the 2030 Agenda for Sustainable Development; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Pleasant, A.; O’Leary, C.; Carmona, R. Health Literacy: Global Advances with a Focus Upon the Shanghai Declaration on Promoting Health in the 2030 Agenda for Sustainable Development. Stud. Health Technol. Inform. 2020, 269, 481–496. [Google Scholar] [CrossRef]
- Bröder, J.; Okan, O.; Bauer, U.; Schlupp, S.; Pinheiro, P. Advancing perspectives on health literacy in childhood and youth. Health Promot. Int. 2020, 35, 575–585. [Google Scholar] [CrossRef]
- Sansom-Daly, U.M.; Lin, M.; Robertson, E.G.; Wakefield, C.E.; McGill, B.C.; Girgis, A.; Cohn, R.J. Health literacy in adolescents and young adults: An updated review. J. Adolesc. Young Adult Oncol. 2016, 5, 106–118. [Google Scholar] [CrossRef]
- Guo, S. Understanding and Measuring Health Literacy among Secondary Students in Beijing and Melbourne. Ph.D. Thesis, The University of Melbourne, Melbourne, Australia, 2018. [Google Scholar]
- Heckman, J.; Masterov, D. The productivity argument for investing in young children. Rev. Agric. Econ. 2007, 29, 446–493. [Google Scholar] [CrossRef]
- Guo, S.; Yu, X.; Okan, O. Moving health literacy research and practice towards a vision of equity, precision and transparency. Int. J. Environ. Res. Public Health 2020, 17, 7650. [Google Scholar] [CrossRef]
- Nutbeam, D.; Lloyd, J.E. Understanding and Responding to Health Literacy as a Social Determinant of Health. Annu. Rev. Public Health 2021, 42, 159–173. [Google Scholar] [CrossRef]
- Fretian, A.; Bollweg, T.M.; Okan, O.; Pinheiro, P.; Bauer, U. Exploring Associated Factors of Subjective Health Literacy in School-Aged Children. Int. J. Environ. Res. Public Health 2020, 17, 1720. [Google Scholar] [CrossRef] [Green Version]
- Stormacq, C.; Van den Broucke, S.; Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot. Int. 2019, 34, e1–e17. [Google Scholar] [CrossRef]
- Mantwill, S.; Monestel-Umaña, S.; Schulz, P.J. The relationship between health literacy and health disparities: A systematic review. PLoS ONE 2015, 10, e0145455. [Google Scholar] [CrossRef] [Green Version]
- Schillinger, D. The Intersections between social determinants of health, health literacy, and health disparities. Stud. Health Technol. Inform. 2020, 269, 22–41. [Google Scholar]
- Smith, J.A.; Griffiths, K.; Nash, R.; Elmer, S.; Ireland, S.; Wright, C.J.C.; Gupta, H. Equity and health literacy: Using emerging evidence to inform the development of the National Preventive Health Strategy. Health Promot. J. Aust. 2021, 32, 3–4. [Google Scholar] [CrossRef]
- Nutbeam, D.; Levin-Zamir, D.; Rowlands, G. Health Literacy and Health Promotion in Context; SAGE Publications Sage UK: London, UK, 2018. [Google Scholar]
- Pleasant, A.; McKinney, J.; Rikard, R.V. Health Literacy Measurement: A Proposed Research Agenda. J. Health Commun. 2011, 16, 11–21. [Google Scholar] [CrossRef] [Green Version]
- McCormack, L.; Haun, J.; Sørensen, K.; Valerio, M. Recommendations for Advancing Health Literacy Measurement. J. Health Commun. 2013, 18, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sørensen, K.; Bitzer, E.-M. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health 2017, 17, 361. [Google Scholar]
- Manganello, J.A. Health literacy and adolescents: A framework and agenda for future research. Health Educ. Res. 2008, 23, 840–847. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Toward an experimental ecology of human development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Higgins, J.W.; Begoray, D.; MacDonald, M. A Social Ecological Conceptual Framework for Understanding Adolescent Health Literacy in the Health Education Classroom. Am. J. Commun. Psychol. 2009, 44, 350–362. [Google Scholar] [CrossRef]
- Guo, S.; Naccarella, L.; Yu, X.; Armstrong, R.; Browne, G.; Shi, Y.; Davis, E. Health literacy and its mediating role in predicting health behaviors among Chinese secondary students. Asia Pac J. Public Health 2021, 33, 76–83. [Google Scholar] [CrossRef]
- Guo, S.; Yu, X.; Davis, E.; Armstrong, R.; Naccarella, L. Health literacy: An interactive outcome among secondary students in Beijing. Health Lit. Res. Pract. 2021, 5, e1–e14. [Google Scholar] [CrossRef]
- Guo, S.; Yu, X.; Davis, E.; Armstrong, R.; Riggs, E.; Naccarella, L. Adolescent Health Literacy in Beijing and Melbourne: A Cross-Cultural Comparison. Int. J. Environ. Res. Public Health 2020, 17, 1242. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.L.; Teufel, J.A.; Birch, D.A. Early Adolescents Perceptions of Health and Health Literacy. J. Sch. Health 2007, 77, 7–15. [Google Scholar] [CrossRef]
- Olyani, S.; Gholian Aval, M.; Tehrani, H.; Mahdiadeh, M. School-based mental health literacy educational interventions in adolescents: A systematic review. J. Health Lit. 2021, 6, 69–77. [Google Scholar]
- Okan, O.; Lopes, E.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L.J.B.P.H. Generic health literacy measurement instruments for children and adolescents: A systematic review of the literature. BMC Public Health 2018, 18, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, S.; Armstrong, R.; Waters, E.; Sathish, T.; Alif, S.M.; Browne, G.R.; Yu, X. Quality of health literacy instruments used in children and adolescents: A systematic review. BMJ Open 2018, 8, e020080. [Google Scholar] [CrossRef] [PubMed]
- Abdillah, I.L.; Lusmilasari, L.; Hartini, S. Instruments to Measure Health Literacy among Children: A Scoping Review. Jurnal Promosi Kesehatan Indonesia 2021, 16, 79–87. [Google Scholar] [CrossRef]
- Zhang, S.-c.; Li, D.-l.; Yang, R.; Wan, Y.-h.; Tao, F.-b.; Fang, J. The association between health literacy and psychosomatic symptoms of adolescents in China: A cross-sectional study. BMC Public Health 2019, 19, 1259. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.; Yang, T.; Wang, S.; Zhang, X. Study on student health literacy gained through health education in elementary and middle schools in China. Health Educ. J. 2012, 71, 452–460. [Google Scholar] [CrossRef]
- Ye, X.-H.; Yang, Y.; Gao, Y.-H.; Chen, S.-D.; Xu, Y. Status and determinants of health literacy among adolescents in Guangdong, China. Asian Pac. J. Cancer Prev. APJCP 2014, 15, 8735–8740. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Xie, T.; Zhang, N. Chinese Students’ Health Literacy Level and Its Associated Factors: A Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 204. [Google Scholar] [CrossRef]
- Guo, S.; Davis, E.; Armstrong, R.; Yu, X.; Naccarella, L. A pilot study of adolescent health literacy research in Melbourne: Implementation and reflections. Health Promot. J. Aust. 2020, 32, 128–132. [Google Scholar] [CrossRef]
- Ilaka, O. A Comparison of Health Literacy Measurement Tools for a Sample of College Students; University at Albany, State University of New York: Albany, NY, USA, 2018. [Google Scholar]
- Shigaki, C.L.; Kruse, R.L.; Mehr, D.R.; Ge, B. The REALM vs. NVS: A comparison of health literacy measuRes. in patients with diabetes. Ann. Behav. Sci. Med. Educ. 2012, 18, 9–13. [Google Scholar] [CrossRef]
- Barber, M.N.; Staples, M.; Osborne, R.H.; Clerehan, R.; Elder, C.; Buchbinder, R. Up to a quarter of the Australian population may have suboptimal health literacy depending upon the measurement tool: Results from a population-based survey. Health Promot. Int. 2009, 24, 252–261. [Google Scholar] [CrossRef] [Green Version]
- Chinese National SSCH Association. Chinese National Survey on Student’s Constitution and Health; China College and University Press: Beijing, China, 2002. [Google Scholar]
- Song, Y.; Ji, C.-Y. Sexual intercourse and high-risk sexual behaviours among a national sample of urban adolescents in China. J. Public Health 2010, 32, 312–321. [Google Scholar] [CrossRef] [Green Version]
- Charter, R.A. Sample size requirements for precise estimates of reliability, generalizability, and validity coefficients. J. Clin. Exp. Neuropsychol. 1999, 21, 559–566. [Google Scholar] [CrossRef]
- Golob, T.F. Structural equation modeling for travel behavior research. Transp. Res. B Meth 2003, 37, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Abel, T.; Hofmann, K.; Ackermann, S.; Bucher, S.; Sakarya, S. Health literacy among young adults: A short survey tool for public health and health promotion research. Health Promot. Int. 2015, 30, 725–735. [Google Scholar] [CrossRef] [Green Version]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick assessment of literacy in primary care: The newest vital sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Rouquette, A.; Nadot, T.; Labitrie, P.; Van den Broucke, S.; Mancini, J.; Rigal, L.; Ringa, V. Validity and measurement invariance across sex, age, and education level of the French short versions of the European Health Literacy Survey Questionnaire. PLoS ONE 2018, 13, e0208091. [Google Scholar] [CrossRef]
- Guo, S.; Davis, E.; Yu, X.; Naccarella, L.; Armstrong, R.; Abel, T.; Browne, G.; Shi, Y. Measuring functional, interactive and critical health literacy of Chinese secondary school students: Reliable, valid and feasible? Glob Health Promot. 2018, 25, 6–14. [Google Scholar] [CrossRef]
- Rouquette, A.; Rigal, L.; Mancini, J.; Guillemin, F.; Van den Broucke, S.; Allaire, C.; Azogui-Levy, S.; Ringa, V.; Hassler, C. Health Literacy throughout adolescence: Invariance and validity study of three measurement scales in the general population. Patient Educ. Couns. 2021, 105, 996–1003. [Google Scholar] [CrossRef]
- Warsh, J.; Chari, R.; Badaczewski, A.; Hossain, J.; Sharif, I. Can the newest vital sign be used to assess health literacy in children and adolescents? Clin. Pediatr. 2014, 53, 141–144. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, M.; Villberg, J.; Torsheim, T.; Tynjälä, J.; Lv, Y.; Kannas, L. Reliability and validity of family affluence scale (FAS II) among adolescents in Beijing, China. Child Indic. Res. 2012, 5, 235–251. [Google Scholar] [CrossRef]
- Schwarzer, R.; Jerusalem, M. The general self-efficacy scale (GSE). Anxiety Stress Coping 2010, 12, 329–345. [Google Scholar]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Glaser, R.R.; Horn, M.L.V.; Arthur, M.W.; Hawkins, J.D.; Catalano, R.F. Measurement properties of the Communities That Care® Youth Survey across demographic groups. J. Quant. Criminol. 2005, 21, 73–102. [Google Scholar] [CrossRef]
- Health Organization; Centres for Disease Control and Prevention (CDC). Global School-based Stu-dent Health Survey (GSHS). Available online: https://ncvc.dspacedirect.org/handle/20.500.11990/1425 (accessed on 10 April 2022).
- Sherry, B.; Jefferds, M.E.; Grummer-Strawn, L.M. Accuracy of Adolescent Self-report of Height and Weight in Assessing Overweight Status: A Literature Review. Arch. Pediatrics Adolesc. Med. 2007, 161, 1154–1161. [Google Scholar] [CrossRef]
- Waters, E.B.; Salmon, L.A.; Wake, M.; Wright, M.; Hesketh, K.D. The health and well-being of adolescents: A school-based population study of the self-report Child Health Questionnaire. J. Adolesc. Health 2001, 29, 140–149. [Google Scholar] [CrossRef]
- Haddock, C.K.; Poston, W.S.; Pyle, S.A.; Klesges, R.C.; Vander Weg, M.W.; Peterson, A.; Debon, M. The validity of self-rated health as a measure of health status among young military personnel: Evidence from a cross-sectional survey. Health Qual. Life Outcomes 2006, 4, 57. [Google Scholar] [CrossRef] [Green Version]
- Ravens-Sieberer, U.; Erhart, M.; Rajmil, L.; Herdman, M.; Auquier, P.; Bruil, J.; Power, M.; Duer, W.; Abel, T.; Czemy, L. Reliability, construct and criterion validity of the KIDSCREEN-10 score: A short measure for children and adolescents’ well-being and health-related quality of life. Qual. Life Res. 2010, 19, 1487–1500. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-Y.; Lei, Y.-T.; Song, Y.; Lu, R.-R.; Duan, J.-L.; Prochaska, J.J. Gender differences in suicidal ideation and health-risk behaviors among high school students in Beijing, China. J. Glob. Health 2019, 9, 010604. [Google Scholar] [CrossRef]
- Yaddanapudi, L.N. The American Statistical Association statement on P-values explained. J. Anaesthesiol. Clin. Pharm. 2016, 32, 421–423. [Google Scholar] [CrossRef]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Rubin, D. Multiple Imputation for Nonresponse in Surveys; Wiley: New York, NY, USA, 1987. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 17; StataCorp LLC.: College Station, TX, USA, 2021. [Google Scholar]
- Fleary, S.A.; Joseph, P.; Pappagianopoulos, J.E. Adolescent health literacy and health behaviors: A systematic review. J. Adolesc. 2018, 62, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Torppa, M.; Paakkari, O.-P.; Välimaa, R.; Ojala, K.; Tynjälä, J. Does health literacy explain the link between structural stratifiers and adolescent health? Eur. J. Public Health 2019, 29, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Santha, A.; Bittlingmayer, U.H.; Bollweg, T.M.; Gerdes, J.; Okan, O.; Okcu, G.; Pinheiro, P.; Osipov, I.; Sahrai, D. Health Literacy and its Determinants in 11- and 12-year-old School Children in Germany. In New Approaches to Health Literacy. Linking Different Perspectives; Saboga-Nunes, L., Bittlingmayer, U.H., Okan, O.D.S., Eds.; Springer: Wiesbaden, Germany, 2020. [Google Scholar]
- Rademakers, J.; Hahnraths, M.T.H.; van Schayck, O.C.P.; Heijmans, M. Children’s Health Literacy in Relation to Their BMI z-Score, Food Intake, and Physical Activity: A Cross-Sectional Study among 8–11-Year-Old Children in The Netherlands. Children 2022, 9, 925. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.O.; Fahland, R.A.; Franze, M.; Splieth, C.; Thyrian, J.R.; Plachta-Danielzik, S.; Hoffmann, W.; Kohlmann, T. Health-related behaviour, knowledge, attitudes, communication and social status in school children in Eastern Germany. Health Educ. Res. 2010, 25, 542–551. [Google Scholar] [CrossRef]
- Sukys, S.; Trinkuniene, L.; Tilindiene, I. Subjective health literacy among school-aged children: First evidence from Lithuania. Int. J. Environ. Res. Public Health 2019, 16, 3397. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Ren, Q.; Jiang, C.; Wang, L. Academic stress and depression of Chinese adolescents in junior high schools: Moderated mediation model of school burnout and self-esteem. J. Affect. Disord. 2021, 295, 384–389. [Google Scholar] [CrossRef]
- Cheng, T.L.; Dreyer, B.P.; Jenkins, R.e.R. Introduction: Child Health Disparities and Health Literacy. Pediatrics 2009, 124, S161–S162. [Google Scholar] [CrossRef]
- Sun, S.; Huang, J.; Hudson, D.L.; Sherraden, M. Cash transfers and health. Annu. Rev. Public Health 2021, 42, 363–380. [Google Scholar] [CrossRef]
- Smith, C.; Goss, H.R.; Issartel, J.; Belton, S. Health Literacy in Schools? A Systematic Review of Health-Related Interventions Aimed at Disadvantaged Adolescents. Children 2021, 8, 176. [Google Scholar] [CrossRef]
- Shih, S.-F.; Liu, C.-H.; Liao, L.-L.; Osborne, R.H. Health literacy and the determinants of obesity: A population-based survey of sixth grade school children in Taiwan. BMC Public Health 2016, 16, 280. [Google Scholar] [CrossRef] [Green Version]
- Olyani, S.; Tehrani, H.; Esmaily, H.; Rezaii, M.M.; Vahedian-Shahroodi, M. Assessment of health literacy with the Newest Vital Sign and its correlation with body mass index in female adolescent students. Int. J. Adolesc. Med. Health 2020, 32. [Google Scholar] [CrossRef]
- Qi, S.; Qin, Z.; Wang, N.; Tse, L.A.; Qiao, H.; Xu, F. Association of academic performance, general health with health-related quality of life in primary and high school students in China. Health Qual. Life Outcomes 2020, 18, 339. [Google Scholar] [CrossRef]
- He, J.; Chen, X.; Fan, X.; Cai, Z.; Huang, F. Is there a relationship between body mass index and academic achievement? A meta-analysis. Public Health 2019, 167, 111–124. [Google Scholar] [CrossRef]
- St Leger, L. Schools, health literacy and public health: Possibilities and challenges. Health Promot. Int. 2001, 16, 197–205. [Google Scholar] [CrossRef]
- Deal, T.B.; Hodges, B. Role of 21st Century Schools in Promoting Health Literacy; National Education Association Health Information Network: Washington, DC, USA, 2009; pp. 1–10. [Google Scholar]
- Nash, R.; Patterson, K.; Flittner, A.; Elmer, S.; Osborne, R. School-Based Health Literacy Programs for Children (2–16 Years): An International Review. J. Sch. Health 2021, 91, 632–649. [Google Scholar] [CrossRef]
- Elmer, S.; Nash, R.; Kemp, N.; Coleman, C.; Wyss, M.; Roach, J. HealthLit4Kids: Supporting schools to be health literacy responsive organisations. Health Promot. J. Austr. 2021, 32, 17–28. [Google Scholar] [CrossRef]
- Blume, M.; Rattay, P.; Hoffmann, S.; Spallek, J.; Sander, L.; Herr, R.; Richter, M.; Moor, I.; Dragano, N.; Pischke, C.; et al. Health Inequalities in Children and Adolescents: A Scoping Review of the Mediating and Moderating Effects of Family Characteristics. Int. J. Environ. Res. Public Health 2021, 18, 7739. [Google Scholar] [CrossRef]
- Gibney, S.; Bruton, L.; Ryan, C.; Doyle, G.; Rowlands, G. Increasing Health Literacy May Reduce Health Inequalities: Evidence from a National Population Survey in Ireland. Int. J. Environ. Res. Public Health 2020, 17, 5891. [Google Scholar] [CrossRef]
- Aghazadeh, S.A.; Aldoory, L. ‘Health literacy for all’: Exploring the feasibility of an intervention to reduce health disparities among rural children. J. Appl. Commun. Res. 2020, 48, 478–495. [Google Scholar] [CrossRef]





| Variable | Frequency (%)/Mean (±SD) |
|---|---|
| Sociodemographics and individual characteristics | |
| Gender | |
| Male | 357 (54.9) |
| Female | 293 (45.1) |
| Year level | |
| Year 7 | 232 (35.7) |
| Year 8 | 215 (33.1) |
| Year 9 | 203 (31.2) |
| Ethnicity | |
| Han | 617 (94.9) |
| Ethnic minority | 33 (5.1) |
| Family composition | |
| Lone parent | 77 (11.9) |
| Two parents | 572 (88.1) |
| Socioeconomic status | |
| Low | 180 (27.7) |
| Medium | 301 (46.3) |
| High | 169 (26.0) |
| Health interest | |
| Not interested | 88 (13.5) |
| Not sure | 85 (13.1) |
| Interested | 477 (73.4) |
| Self-efficacy | 26.85 (6.37) |
| Social support | 62.79 (15.26) |
| School environment | 30.48 (5.59) |
| Health literacy | |
| HLAT | 26.34 (5.89) |
| NVS | 3.64 (1.64) |
| HLS | 13.72 (2.94) |
| Developmental outcomes | |
| Health-promoting behaviours | 28.04 (3.65) |
| Body mass index | 21.21 (5.02) |
| Patient-provider communication | |
| 0 times | 332 (53.2) |
| 1–2 times | 221 (35.4) |
| 3–5 times | 51 (8.2) |
| 6 times or more | 20 (3.2) |
| Global health status | |
| Poor | 9 (1.4) |
| Fair | 215 (33.1) |
| Good | 227 (34.9) |
| Very good | 125 (19.2) |
| Excellent | 74 (11.4) |
| Health-related quality of life | 37.49 (5.78) |
| Academic performance | |
| Very poor | 69 (10.6) |
| Poor | 139 (21.5) |
| Average | 197 (30.4) |
| Good | 186 (28.7) |
| Very good | 57 (8.8) |
| Gender | YL | Ethnicity | FC | SES | HI | SEF | SS | SCE | HLAT | NVS | HLS | HPB | BMI | PC | GHS | HRQOL | AP | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | 1.00 | |||||||||||||||||
| YL | 0.00 | 1.00 | ||||||||||||||||
| Ethnicity | −0.01 | 0.03 | 1.00 | |||||||||||||||
| FC | 0.03 | 0.00 | −0.08 | 1.00 | ||||||||||||||
| SES | 0.02 | −0.01 | 0.06 | 0.06 | 1.00 | |||||||||||||
| HI | 0.03 | −0.08 | −0.04 | 0.00 | 0.04 | 1.00 | ||||||||||||
| SEF | −0.11 * | −0.11 * | −0.01 | 0.05 | 0.17 * | 0.17 * | 1.00 | |||||||||||
| SS | 0.02 | −0.06 | 0.03 | 0.10 * | 0.18 * | 0.25 * | 0.41 * | 1.00 | ||||||||||
| SCE | 0.03 | −0.16 * | −0.03 | 0.03 | 0.13 * | 0.22 * | 0.45 * | 0.55 * | 1.00 | |||||||||
| HLAT | −0.00 | −0.04 | 0.03 | 0.00 | 0.15 * | 0.29 * | 0.38 * | 0.44 * | 0.42 * | 1.00 | ||||||||
| NVS | 0.01 | 0.03 | 0.02 | −0.02 | 0.02 | 0.11 * | 0.10 * | 0.17 * | 0.11 * | 0.20 * | 1.00 | |||||||
| HLS | −0.03 | 0.01 | −0.07 | 0.06 | 0.11 * | 0.16 * | 0.25 * | 0.37 * | 0.32 * | 0.43 * | 0.14 * | 1.00 | ||||||
| HPB | −0.07 | −0.08 | −0.04 | 0.05 | 0.12 * | 0.17 * | 0.30 * | 0.28 * | 0.32 * | 0.29 * | 0.07 | 0.32 * | 1.00 | |||||
| BMI | −0.10 * | 0.07 | 0.01 | 0.05 | −0.03 | −0.06 | −0.04 | −0.03 | −0.05 | −0.05 | −0.05 | −0.03 | −0.09 * | 1.00 | ||||
| PC | 0.05 | 0.01 | 0.02 | 0.04 | 0.12 * | 0.16 * | 0.12 * | 0.14 * | 0.09 * | 0.15 * | 0.06 | 0.11 * | 0.06 | −0.03 | 1.00 | |||
| GHS | −0.14 * | −0.10 * | −0.04 | 0.11 * | 0.10 * | 0.14 * | 0.25 * | 0.23 * | 0.19 * | 0.24 * | 0.02 | 0.23 * | 0.18 * | −0.12 * | −0.05 | 1.00 | ||
| HRQOL | −0.12 * | −0.15 * | −0.04 | 0.05 | 0.18 * | 0.20 * | 0.35 * | 0.59 * | 0.48 * | 0.35 * | 0.14 * | 0.34 * | 0.32 * | −0.06 | 0.06 | 0.34 * | 1.00 | |
| AP | 0.08 | −0.01 | 0.04 | −0.01 | 0.16 * | 0.10 * | 0.20 * | 0.24 * | 0.21 * | 0.22 * | 0.39 * | 0.18 * | 0.17 * | −0.09 * | 0.12 * | 0.03 | 0.22 * | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, S.; Yu, X.; Davis, E.; Armstrong, R.; Naccarella, L. Comparison of Health Literacy Assessment Tools among Beijing School-Aged Children. Children 2022, 9, 1128. https://doi.org/10.3390/children9081128
Guo S, Yu X, Davis E, Armstrong R, Naccarella L. Comparison of Health Literacy Assessment Tools among Beijing School-Aged Children. Children. 2022; 9(8):1128. https://doi.org/10.3390/children9081128
Chicago/Turabian StyleGuo, Shuaijun, Xiaoming Yu, Elise Davis, Rebecca Armstrong, and Lucio Naccarella. 2022. "Comparison of Health Literacy Assessment Tools among Beijing School-Aged Children" Children 9, no. 8: 1128. https://doi.org/10.3390/children9081128