
Impact of Intubator’s Training Level on First-Pass Success of Endotracheal Intubation in Acute Care Settings: A Four-Center Retrospective Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
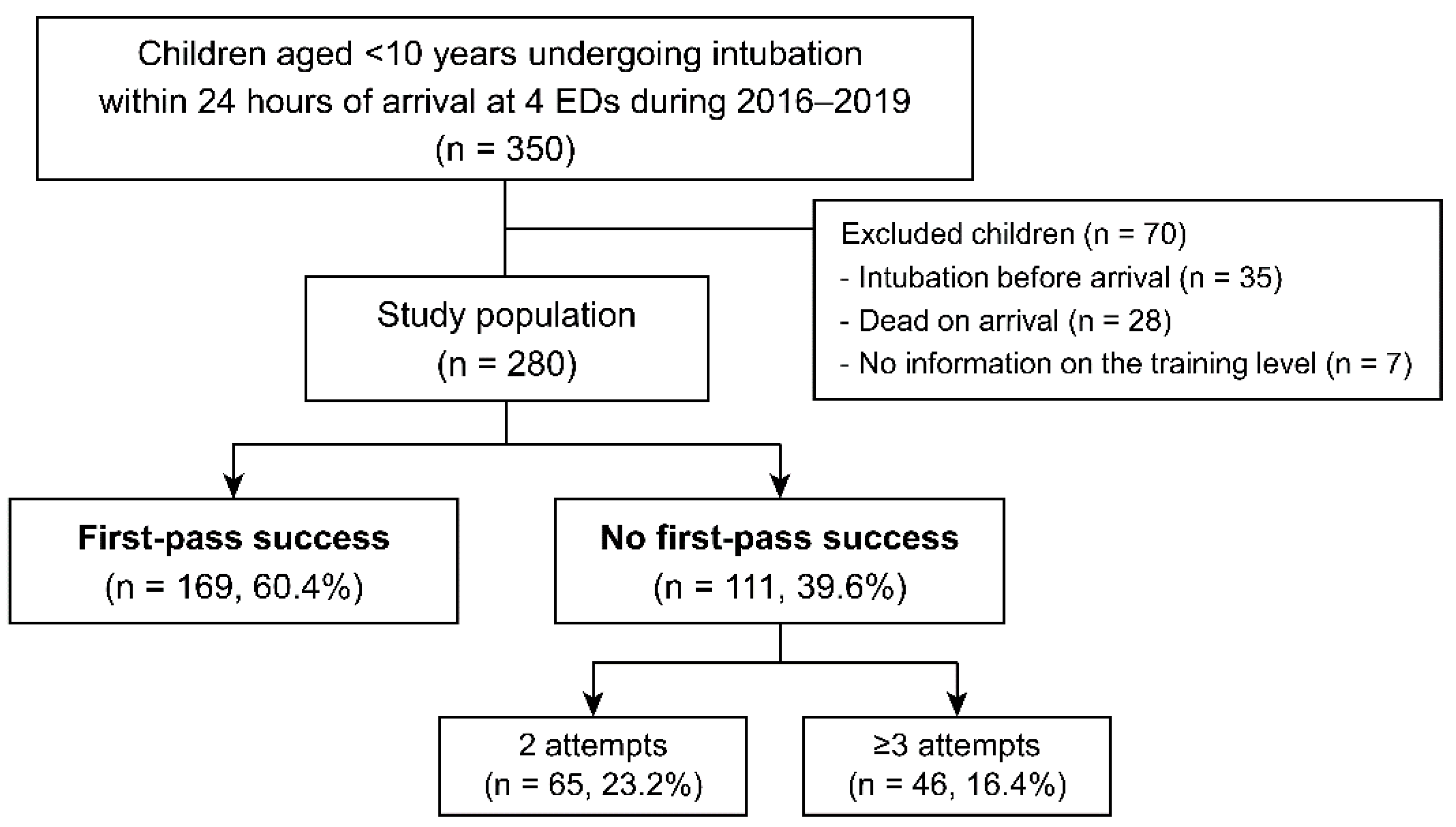
2.2. Study Population
2.3. Definitions
2.4. Data Collection
2.5. Statistical Analyses
3. Results
3.1. Patient-Level Variables
3.2. Intubator-Level Variables
3.3. Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choi, H.J.; Je, S.M.; Kim, J.H.; Kim, E. The factors associated with successful paediatric endotracheal intubation on the first attempt in emergency departments: A 13-emergency-department registry study. Resuscitation 2012, 83, 1363–1368. [Google Scholar] [CrossRef] [PubMed]
- Pallin, D.J.; Dwyer, R.C.; Walls, R.M.; Brown, C.A., 3rd. Techniques and Trends, Success Rates, and Adverse Events in Emergency Department Pediatric Intubations: A Report from the National Emergency Airway Registry. Ann. Emerg. Med. 2016, 67, 610–615.e611. [Google Scholar] [CrossRef] [PubMed]
- Kerrey, B.T.; Rinderknecht, A.S.; Geis, G.L.; Nigrovic, L.E.; Mittiga, M.R. Rapid sequence intubation for pediatric emergency patients: Higher frequency of failed attempts and adverse effects found by video review. Ann. Emerg. Med. 2012, 60, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, T.; Gibo, K.; Hagiwara, Y.; Okubo, M.; Brown, D.F.; Brown, C.A., 3rd; Hasegawa, K. Factors Associated with First-Pass Success in Pediatric Intubation in the Emergency Department. West J. Emerg. Med. 2016, 17, 129–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, R.C., Jr.; Giuliano, J.S., Jr.; Sullivan, J.E.; Brown, C.A., 3rd; Walls, R.M.; Nadkarni, V.; Nishisaki, A. Level of trainee and tracheal intubation outcomes. Pediatrics 2013, 131, e821–e828. [Google Scholar] [CrossRef] [Green Version]
- Brown, C.A., 3rd; Kaji, A.H.; Fantegrossi, A.; Carlson, J.N.; April, M.D.; Kilgo, R.W.; Walls, R.M. Video Laryngoscopy Compared to Augmented Direct Laryngoscopy in Adult Emergency Department Tracheal Intubations: A National Emergency Airway Registry (NEAR) Study. Acad. Emerg. Med. 2020, 27, 100–108. [Google Scholar] [CrossRef]
- Carroll, C.L.; Spinella, P.C.; Corsi, J.M.; Stoltz, P.; Zucker, A.R. Emergent endotracheal intubations in children: Be careful if it’s late when you intubate. Pediatr. Crit. Care Med. 2010, 11, 343–348. [Google Scholar] [CrossRef]
- Rinderknecht, A.S.; Mittiga, M.R.; Meinzen-Derr, J.; Geis, G.L.; Kerrey, B.T. Factors associated with oxyhemoglobin desaturation during rapid sequence intubation in a pediatric emergency department: Findings from multivariable analyses of video review data. Acad. Emerg. Med. 2015, 22, 431–440. [Google Scholar] [CrossRef]
- Eich, C.; Timmermann, A.; Russo, S.G.; Cremer, S.; Nickut, A.; Strack, M.; Weiss, M.; Müller, M.P. A controlled rapid-sequence induction technique for infants may reduce unsafe actions and stress. Acta Anaesthesiol. Scand. 2009, 53, 1167–1172. [Google Scholar] [CrossRef]
- Kanaris, C.; Murphy, P.C. Fifteen-minute consultation: Intubation of the critically ill child presenting to the emergency department. Arch. Dis. Child Educ. Pract. Ed. 2021. [Google Scholar] [CrossRef]
- West, J.R.; O’Keefe, B.P.; Russell, J.T. Predictors of first pass success without hypoxemia in trauma patients requiring emergent rapid sequence intubation. Trauma Surg. Acute Care Open 2021, 6, e000588. [Google Scholar] [CrossRef] [PubMed]
- Sagarin, M.J.; Chiang, V.; Sakles, J.C.; Barton, E.D.; Wolfe, R.E.; Vissers, R.J.; Walls, R.M. Rapid sequence intubation for pediatric emergency airway management. Pediatr. Emerg. Care 2002, 18, 417–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, T.; Park, J.; Je, S. Pediatric Korean Triage and Acuity Scale. Pediatr. Emerg. Med. J. 2015, 2, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Ko, Y.; Kim, J.H.; Hwang, K.; Lee, J.; Huh, Y. Comparison of Base Deficit and Vital Signs as Criteria for Hemorrhagic Shock Classification in Children with Trauma. Yonsei Med. J. 2021, 62, 352–358. [Google Scholar] [CrossRef]
- Lee, J.H.; Turner, D.A.; Kamat, P.; Nett, S.; Shults, J.; Nadkarni, V.M.; Nishisaki, A.; for the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) & the National Emergency Airway Registry for Children (NEAR4KIDS). The number of tracheal intubation attempts matters! A prospective multi-institutional pediatric observational study. BMC Pediatrics 2016, 16, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, G.; von Ungern-Sternberg, B.S.; Engelhardt, T. Pediatric airway management. Curr. Opin. Anaesthesiol. 2021, 34, 276–283. [Google Scholar] [CrossRef]
- Miller, K.A.; Nagler, J. Advances in Emergent Airway Management in Pediatrics. Emerg. Med. Clin. N. Am. 2019, 37, 473–491. [Google Scholar] [CrossRef]
- Nagler, J.; Auerbach, M.; Monuteaux, M.C.; Cheek, J.A.; Babl, F.E.; Oakley, E.; Nguyen, L.; Rao, A.; Dalton, S.; Lyttle, M.D.; et al. Exposure and confidence across critical airway procedures in pediatric emergency medicine: An international survey study. Am. J. Emerg. Med. 2021, 42, 70–77. [Google Scholar] [CrossRef]
- Mills, D.M.; Wu, C.L.; Williams, D.C.; King, L.; Dobson, J.V. High-fidelity simulation enhances pediatric residents’ retention, knowledge, procedural proficiency, group resuscitation performance, and experience in pediatric resuscitation. Hosp. Pediatr. 2013, 3, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Ruetzler, K.; Roessler, B.; Potura, L.; Priemayr, A.; Robak, O.; Schuster, E.; Frass, M. Performance and skill retention of intubation by paramedics using seven different airway devices—A manikin study. Resuscitation 2011, 82, 593–597. [Google Scholar] [CrossRef]
- Roy, K.M.; Miller, M.P.; Schmidt, K.; Sagy, M. Pediatric residents experience a significant decline in their response capabilities to simulated life-threatening events as their training frequency in cardiopulmonary resuscitation decreases. Pediatr. Crit. Care Med. 2011, 12, e141–e144. [Google Scholar] [CrossRef] [PubMed]
- Andreatta, P.B.; Dooley-Hash, S.L.; Klotz, J.J.; Hauptman, J.G.; Biddinger, B.; House, J.B. Retention Curves for Pediatric and Neonatal Intubation Skills After Simulation-Based Training. Pediatr. Emerg. Care 2016, 32, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Kendirli, T.; Caltik, A.; Duman, M.; Yilmaz, H.L.; Yildizdaş, D.; Boşnak, M.; Tekin, D.; Atay, N. Effect of pediatric advanced life support course on pediatric residents’ intubation success. Pediatr. Int. 2011, 53, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.A.; Monuteaux, M.C.; Nagler, J. Technical factors associated with first-pass success during endotracheal intubation in children: Analysis of videolaryngoscopy recordings. Emerg. Med. J. 2021, 38, 125–131. [Google Scholar] [CrossRef]


{kind=link}
| Author | Study Design/Setting | Factors for FPS * | Training Level | Intubator’s Specialty and Remarks |
|---|---|---|---|---|
| Choi et al. [1] | Prospective, 13 EDs in Korea, 2006–2010, n = 281, age <10 year (median, 23.8 mo; ≤2 year, 50.2%) | FPS, 67.6% EM (2.94; 1.38–6.26) | Not related | EM (72.2%) and PED (24.9%) ≥3 attempts, 12.8%; RSI, 12.1%; and trauma, 28.5% |
| Kerrey et al. [3] | Video review, single ED in the U.S., Apr 2009–Mar 2010, n = 114, age not specified (median, 2.4 year) | FPS, 51.8% Attending (10.20; 2.10–50.90) | Partially related; only 2 specialties (PEM attending or anesthesiologist) | PED residents (42.9%), PEM attendings/fellows (16.1%/18.8%), and EM residents (13.4%) ≥3 attempts, 26.3%; RSI, 100%; and trauma, 18.4% |
| Goto et al. [4] | Prospective, 17 EDs in Japan, 2010–2014, n = 293, age ≤18 year (median, 6 year) | FPS, 60.1% EM (3.21; 1.78–5.83), age ≥10 year (2.45; 1.23–4.87), and RSI (2.17; 1.31–3.57) In <10 year: EM (4.08;1.92–8.63) and RSI (3.05; 1.63–5.70) | Partially related; only 1 specialty (EM in PGY ≥3) | EM (43.3%) and PED (15.4%) ≥3 attempts, 16.0%; RSI, 25.9%; and trauma, 23.5% |
| Pallin et al. [2] | Prospective, 10 EDs in the U.S., 2002–2012, n = 1053, age <16 year (median, 7 year) | FPS, 83.2% Video laryngoscopy (3.40; 1.50–7.60), infants (0.39; 0.26–0.58), and girls (0.57; 0.46–0.73) If excluding “crash airways”: above 3 factors plus RSI (3.40; 1.50–7.40) | Not related | EM (83.6%), PED (6.5%), and PEM (3.6%) ≥3 attempts, unknown; RSI, 80.5%; and trauma, 50.3% |
| Sanders et al. [5] | Prospective, 15 ICUs in the U.S., 2010–2011, n = 1265, age not specified (median, 1 year) | FPS, 60.3% Fellow (4.29; 3.24–5.68; vs. resident) | Partially related; only 1 specialty (pediatrics) | PED (100%) ≥3 attempts, unknown; RSI, unknown; and trauma, 2.4% |
| Variable | Total (n = 280) | FPS (n = 169) | Non-FPS (n = 111) | p |
|---|---|---|---|---|
| Age (month) | 16.5 (5.0–52.3) | 23.0 (7.0–59.5) | 11.0 (4.0–37.0) | 0.018 |
| Infants | 117 (41.8) | 61 (36.1) | 56 (50.5) | 0.017 |
| Girls | 121 (43.2) | 73 (43.2) | 48 (43.2) | 0.994 |
| Overall comorbidity | 168 (60.0) | 100 (59.2) | 68 (61.3) | 0.727 |
| Critical comorbidity * | 28 (10.0) | 14 (8.3) | 14 (12.6) | 0.238 |
| High acuity | 133 (47.5) | 86 (50.9) | 47 (42.3) | 0.161 |
| Trauma | 26 (9.3) | 17 (10.1) | 9 (8.1) | 0.582 |
| Crash airway | 84 (30.0) | 57 (33.7) | 27 (24.3) | 0.093 |
| Hypotension † | 64 (22.9) | 38 (22.5) | 26 (23.4) | 0.855 |
| Tachycardia † | 178 (69.8) § | 106 (71.1) | 72 (67.9) | 0.581 |
| Tachypnea † | 57 (25.7) § | 36 (29.0) | 21 (21.4) | 0.198 |
| Desaturation † | 148 (53.0) § | 89 (53.0) | 59 (53.2) | 0.977 |
| Altered mental status † | 110 (39.4) § | 69 (40.8) | 41 (37.3) | 0.553 |
| Indications for intubation | 0.030 | |||
| Respiratory compromise | 131 (46.8) | 70 (41.4) | 61 (55.0) | |
| Altered mental status | 76 (27.1) | 47 (27.8) | 29 (26.1) | |
| Cardiac arrest | 44 (15.7) | 28 (16.6) | 16 (14.4) | |
| Shock or others ‡ | 29 (10.4) | 24 (14.2) | 5 (4.5) |
| Variable | Total (n = 280) | FPS (n = 169) | Non-FPS (n = 111) | p |
|---|---|---|---|---|
| Experienced intubators | 234 (83.6) | 147 (87.0) | 87 (78.4) | 0.057 |
| Specialty of intubators | 0.166 | |||
| Emergency medicine | 92 (33.0) * | 62 (36.9) * | 30 (27.0) | 0.086 § |
| Pediatrics | 167 (59.9) * | 93 (55.4) * | 74 (66.7) | |
| Others | 20 (7.2) *,† | 13 (7.7) *,† | 7 (6.3) | |
| RSI | 46 (16.4) | 26 (15.4) | 20 (18.0) | 0.561 |
| Induction agents | 149 (53.2) | 81 (47.9) | 68 (61.3) | 0.029 |
| Etomidate | 21 (7.5) | 15 (8.9) | 6 (5.4) | 0.002 |
| Ketamine | 22 (7.9) | 17 (10.1) | 5 (4.5) | |
| Fentanyl | 17 (6.1) | 5 (3.0) | 12 (10.8) | |
| Benzodiazepine | 89 (31.8) | 44 (26.0) | 45 (40.5) | |
| None | 131 (46.8) | 88 (52.1) | 43 (38.7) | |
| NMBAs | 57 (20.4) | 30 (17.8) | 27 (24.3) | 0.182 |
| Succinylcholine | 15 (5.4) | 9 (5.3) | 6 (5.4) | NA |
| Rocuronium | 3 (1.1) | 1 (0.6) | 2 (1.8) | |
| Vecuronium | 39 (13.9) | 20 (11.8) | 19 (17.1) | |
| None | 223 (79.6) | 139 (82.2) | 84 (75.7) | |
| Locations of intubation | NA | |||
| Emergency department | 200 (71.9) ‡ | 121 (72.5) ‡ | 79 (71.2) | |
| Intensive care unit | 73 (26.3) ‡ | 45 (26.9) ‡ | 28 (25.2) | |
| Ward | 5 (1.8) ‡ | 1 (0.6) ‡ | 4 (3.6) |
| Variable | Total (n = 280) | FPS (n = 169) | Non-FPS (n = 111) | p |
|---|---|---|---|---|
| Desaturation | 76 (27.1) | 17 (10.1) | 59 (53.2) | <0.001 |
| Overall success | 277 (98.9) | 169 (100.0) | 108 (97.3) | 0.061 |
| Total no. of attempts | 1.0 (1.0–2.0) | 1.0 (1.0–1.0) | 2.0 (2.0–3.0) | <0.001 |
| ED-success time (min) | 73.5 (22.0–267.8) | 49.0 (18.5–208.5) | 94.0 (32.0–313.0) | 0.008 |
| Rescue airway | 4 (1.4) | 0 (0) | 4 (3.6) | 0.024 |
| Cardiac arrest | 48 (17.1) | 31 (18.3) | 17 (15.3) | 0.511 |
| Ventilator days | 4.0 (1.0–9.0) | 3.0 (1.0–8.0) | 4.0 (2.0–11.0) | 0.217 |
| In-hospital mortality | 50 (17.9) | 31 (18.3) | 19 (17.1) | 0.793 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Jung, J.-Y.; Park, J.-W.; Lee, S.-U.; Son, M.-H.; Lee, J.-Y. Impact of Intubator’s Training Level on First-Pass Success of Endotracheal Intubation in Acute Care Settings: A Four-Center Retrospective Study. Children 2022, 9, 960. https://doi.org/10.3390/children9070960
Kim J-H, Jung J-Y, Park J-W, Lee S-U, Son M-H, Lee J-Y. Impact of Intubator’s Training Level on First-Pass Success of Endotracheal Intubation in Acute Care Settings: A Four-Center Retrospective Study. Children. 2022; 9(7):960. https://doi.org/10.3390/children9070960
Chicago/Turabian StyleKim, Jung-Heon, Jae-Yun Jung, Joong-Wan Park, Se-Uk Lee, Meong-Hi Son, and Jeong-Yong Lee. 2022. "Impact of Intubator’s Training Level on First-Pass Success of Endotracheal Intubation in Acute Care Settings: A Four-Center Retrospective Study" Children 9, no. 7: 960. https://doi.org/10.3390/children9070960