
Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report

 ,
,  , , ,
, , ,  , ,
, ,  , , ,
, , ,  ,
,  , , ,
, , ,  ,
,  , , , ,
, , , ,  and
and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
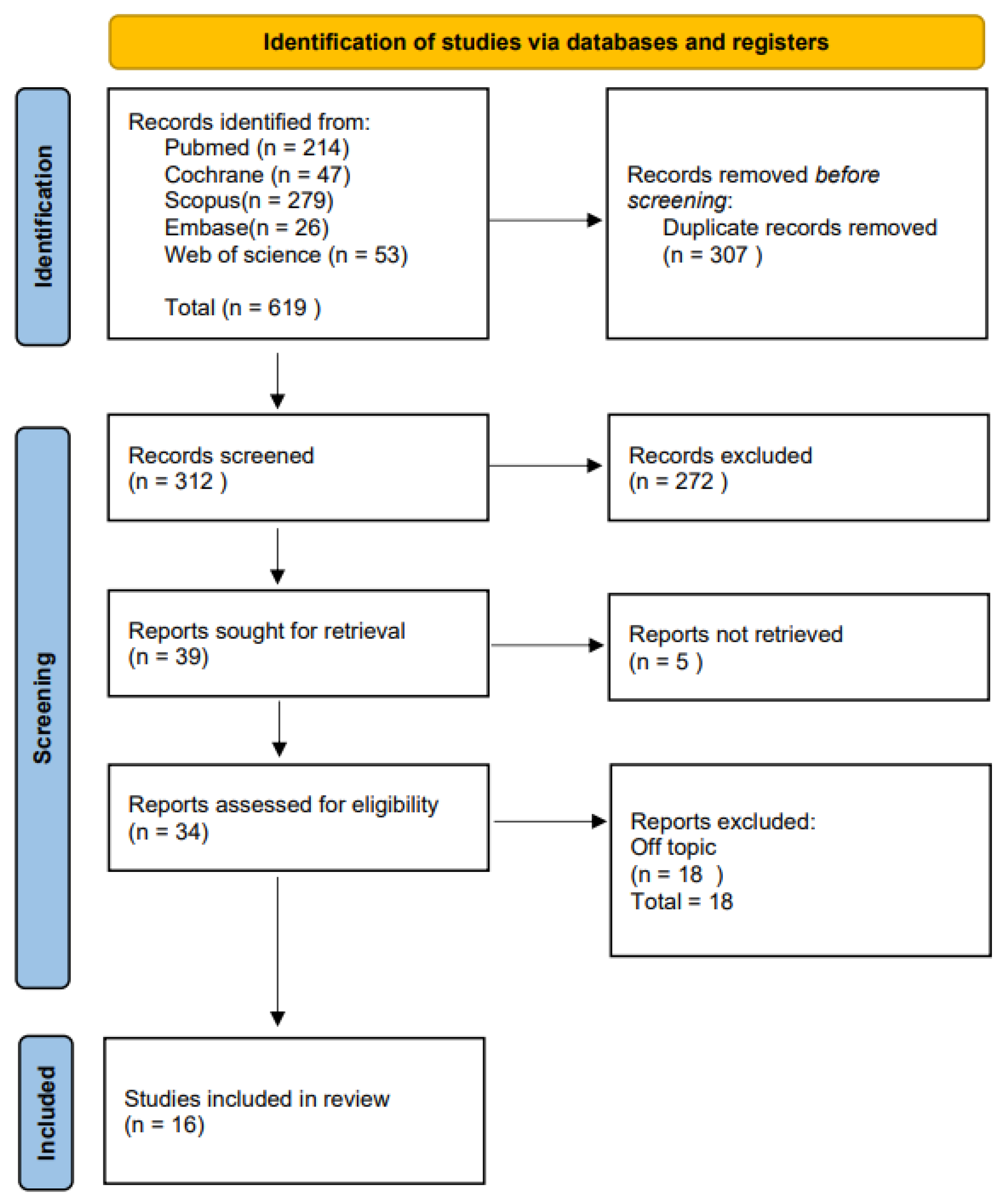
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Inclusion and Exclusion Criteria
2.4. Data Sources and Search Strategy
2.5. Data Collection
3. Results
Study Selection and Characteristics
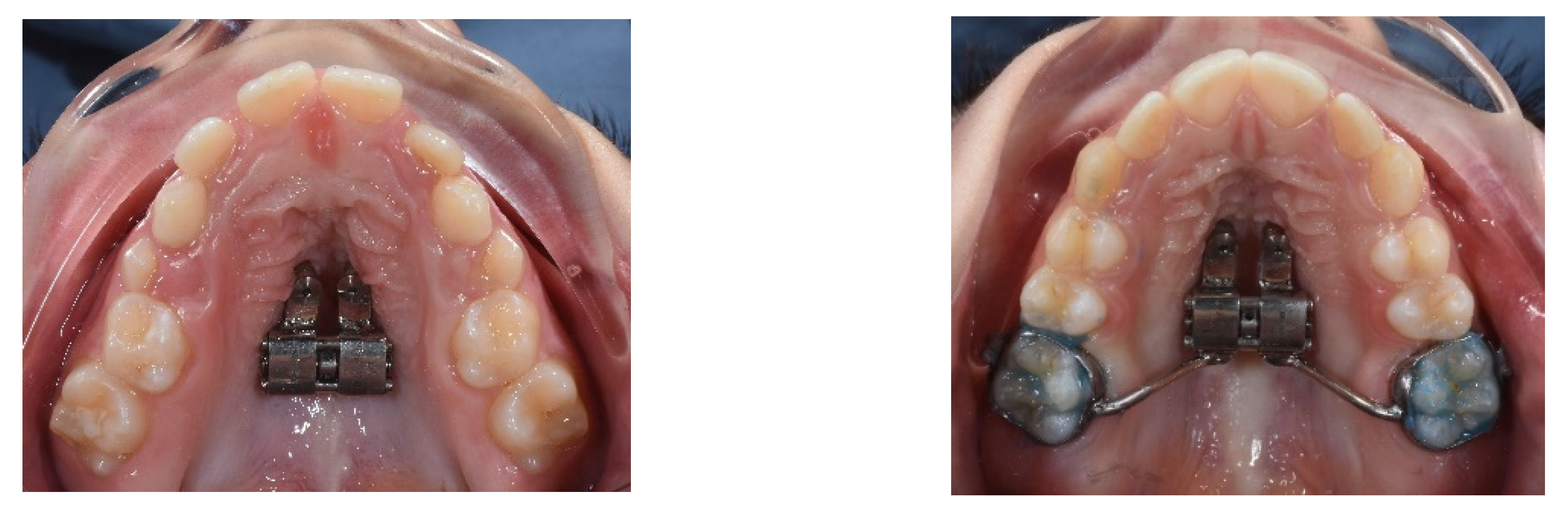
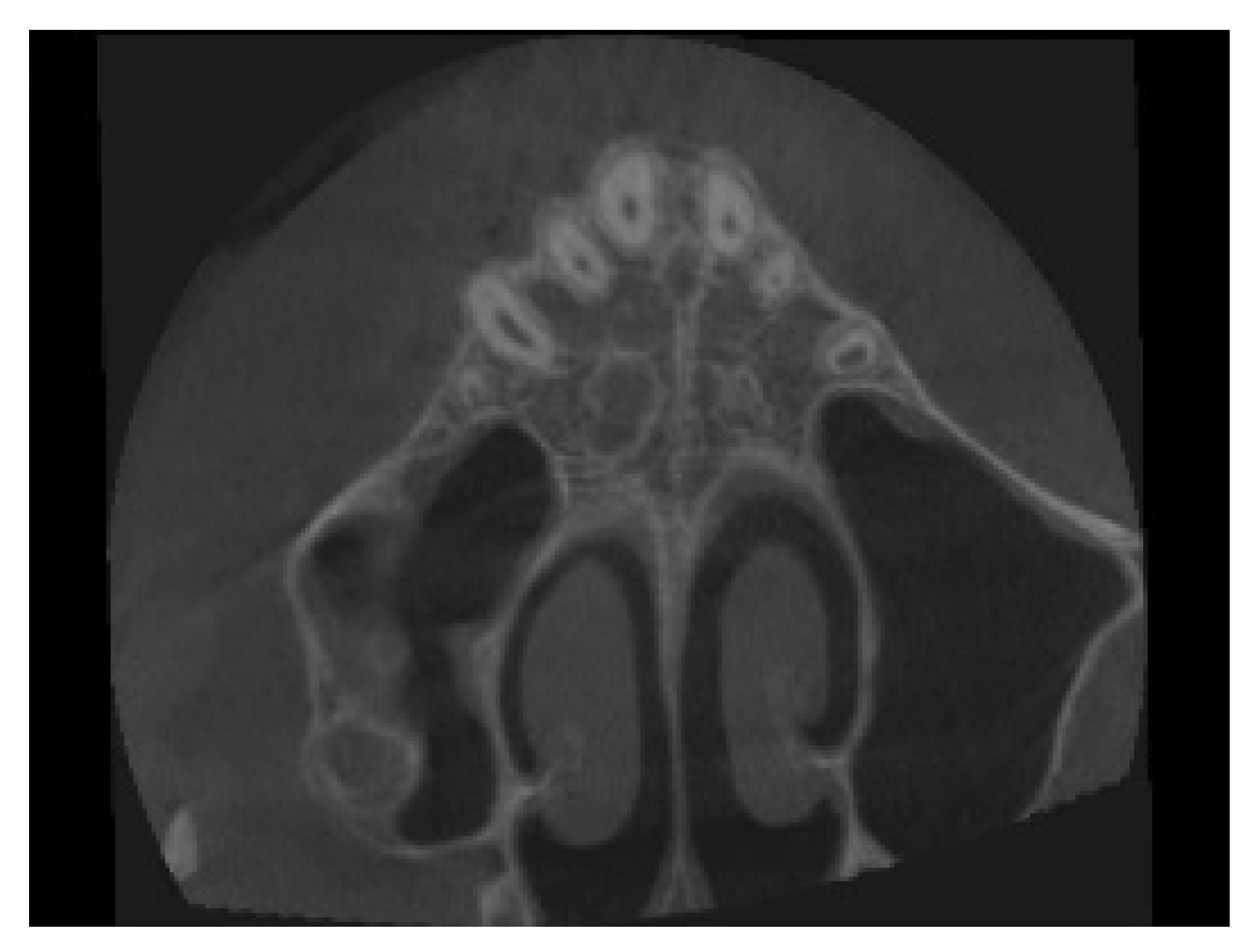
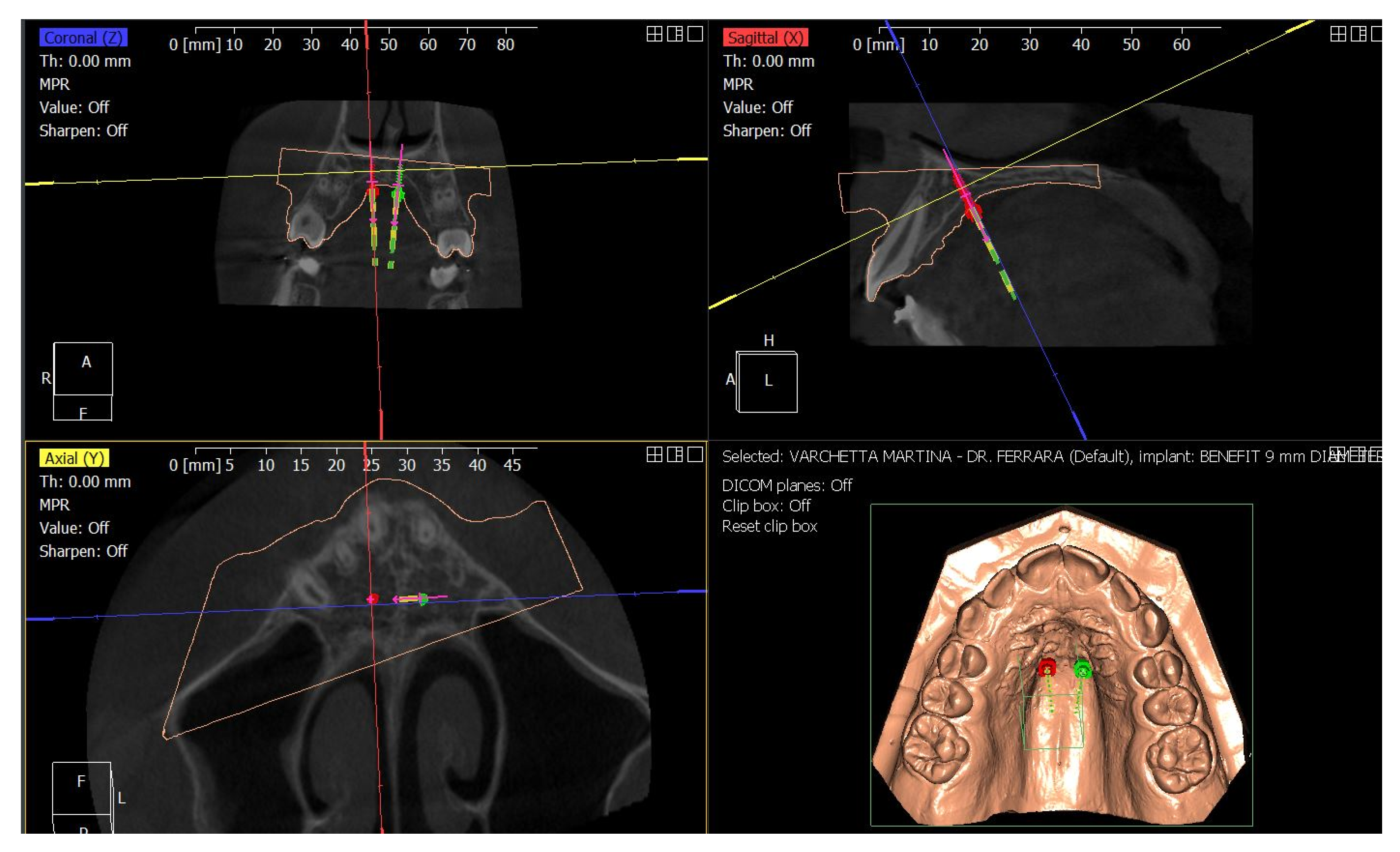
4. Case Report
4.1. Etiology and Diagnosis
4.2. Treatment Objectives
4.3. Treatment Strategy
4.4. Treatment Progress
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BB MARPE | Bone-born RME appliance |
| CBCT | Cone-beam computed tomography |
| MARPE | Miniscrew Anchored Rapid Palatal Expander |
| M-MW | Molar-maxillary width |
| MW | Maxillary-width |
| OSAS | Obstructive sleep apnea syndrome |
| PA | Posteroanterior |
| P-MW | Premolar-maxillary width |
| RME | Rapid maxillary expansion |
| TAD | Temporary anchorage device |
| TB RME | Tooth-borne RME appliance |
| TBB MARPE | Tooth–bone-borne MARPE appliance |
| TTB RME | Tooth-tissue-borne RME appliance |
| U6 | Upper first molar |
| L6 | Lower first molar |
References
- Proffit, W.R. Multicenter, Internet-Based Orthodontic Education: A Research Proposal. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 164–167. [Google Scholar] [CrossRef]
- Adina, S.; Dipalma, G.; Bordea, I.R.; Lucaciu, O.; Feurdean, C.; Inchingolo, A.D.; Septimiu, R.; Malcangi, G.; Cantore, S.; Martin, D.; et al. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef]
- Liu, S.; Xu, T.; Zou, W. Effects of Rapid Maxillary Expansion on the Midpalatal Suture: A Systematic Review. EORTHO 2015, 37, 651–655. [Google Scholar] [CrossRef] [Green Version]
- Farronato, P.P.; Pasciuti, G.E. Espansione Rapida del Palato: Terapia del Deficit. Available online: https://it.dental-tribune.com/news/espansione-rapida-del-palato-terapia-del-deficit-trasversale-scheletrico-del-mascellare-superiore/ (accessed on 21 March 2022).
- Dimonte, M.; Inchingolo, F.; Minonne, A.; Arditi, G.; Dipalma, G. Bone SPECT in Management of Mandibular Condyle Hyperplasia. Report of a Case and Review of Literature. Minerva Stomatol. 2004, 53, 281–285. [Google Scholar] [PubMed]
- Eguren, M. Midpalatal Suture Density Ratio after Rapid Maxillary Expansion Evaluated by Cone-Beam Computed Tomography. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 10. [Google Scholar] [CrossRef] [PubMed]
- Pasqua, B.D.P.M.; André, C.B.; Paiva, J.B.; Tarraf, N.E.; Wilmes, B.; Rino-Neto, J. Dentoskeletal Changes Due to Rapid Maxillary Expansion in Growing Patients with Tooth-Borne and Tooth-Bone-Borne Expanders: A Randomized Clinical Trial. Orthod. Craniofacial Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gokturk, M.; Yavan, M.A. Comparison of the Short-Term Effects of Tooth-Bone-Borne and Tooth-Borne Rapid Maxillary Expansion in Older Adolescents. J. Orofac. Orthop. 2022, 1–13. [Google Scholar] [CrossRef]
- Angelieri, F.; Cevidanes, L.H.S.; Franchi, L.; Gonçalves, J.R.; Benavides, E.; McNamara, J.A., Jr. Midpalatal Suture Maturation: Classification Method for Individual Assessment before Rapid Maxillary Expansion. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Stoilova-Todorova, M.G.; Krasteva, S.; Stoilov, G. Skeletal Age Assessment in Patients with Transverse Maxillary Deficit Undergoing Rapid Maxillary Expansion. J. IMAB 2018, 24, 2113–2118. [Google Scholar] [CrossRef] [Green Version]
- Schauseil, M.; Ludwig, B.; Zorkun, B.; Hellak, A.; Korbmacher-Steiner, H. Density of the Midpalatal Suture after RME Treatment—A Retrospective Comparative Low-Dose CT-Study. Head Face Med. 2014, 10, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franchi, L.; Baccetti, T.; Lione, R.; Fanucci, E.; Cozza, P. Modifications of Midpalatal Sutural Density Induced by Rapid Maxillary Expansion: A Low-Dose Computed-Tomography Evaluation. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 486–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baccetti, T.; Franchi, L.; Cameron, C.G.; McNamara, J.A., Jr. Treatment Timing for Rapid Maxillary Expansion. Angle Orthod. 2001, 71, 343–350. [Google Scholar] [PubMed]
- Angelieri, F.; Franchi, L.; Cevidanes, L.H.S.; McNamara, J.A., Jr. Diagnostic Performance of Skeletal Maturity for the Assessment of Midpalatal Suture Maturation. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 1010–1016. [Google Scholar] [CrossRef]
- Kapetanović, A.; Theodorou, C.; Bergé, S.; Schols, J.; Xi, T. Efficacy of Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in Late Adolescents and Adults: A Systematic Review and Meta-Analysis. Eur. J. Orthod. Eur. J. Orthod. 2021, 43, 313–323. [Google Scholar] [CrossRef]
- Gabriele, O.D.; Dallatana, G.; Riva, R.; Vasudavan, S.; Wilmes, B. The Easy Driver for Placement of Palatal Mini-Implants and a Maxillary Expander in a Single Appointment. J. Clin. Orthod. JCO 2017, 51, 728–737. [Google Scholar]
- Maino, B.G.; Paoletto, E.; Lombardo, L.; Siciliani, G. A Three-Dimensional Digital Insertion Guide for Palatal Miniscrew Placement. J. Clin. Orthod. JCO 2016, 50, 12–22. [Google Scholar]
- Patianna, A.G.; Ballini, A.; Meneghello, M.; Cantore, S.; Inchingolo, A.M.; Dipalma, G.; Inchingolo, A.D.; Inchingolo, F.; Malcangi, G.; Lucchese, A.; et al. Comparison of Conventional Orthognathic Surgery and “Surgery-First” Protocol: A New Weapon against Time. J. Biol. Regul. Homeost. Agents 2019, 33, 59–67. [Google Scholar]
- Laudadio, C.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Montenegro, V.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Management of Anterior Open-Bite in the Deciduous, Mixed and Permanent Dentition Stage: A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 271–281. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; De Vito, D.; Martelli, F.S.; Georgakopoulos, I.; Almasri, M.; Dibello, V.; Altini, V.; Farronato, G.; Dipalma, G.; et al. Characterization of Human Apical Papilla-Derived Stem Cells. J. Biol. Regul. Homeost. Agents 2017, 31, 901–910. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Gökçe, G.; Akan, B.; Veli, İ. A Postero-Anterior Cephalometric Evaluation of Different Rapid Maxillary Expansion Appliances. J. World Fed. Orthod. 2021, 10, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Akan, B.; Gökçe, G.; Şahan, A.O.; Veli, İ. Tooth-borne versus Tooth-bone-borne Rapid Maxillary Expanders According to a Stereophotogrammetric Evaluation of Facial Soft Tissues: A Randomized Clinical Trial. Orthod. Craniofac. Res. 2021, 24, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Canan, S.; Şenışık, N.E. Comparison of the Treatment Effects of Different Rapid Maxillary Expansion Devices on the Maxilla and the Mandible. Part 1: Evaluation of Dentoalveolar Changes. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 1125–1138. [Google Scholar] [CrossRef] [PubMed]
- Silveira, G.S.; Abreu, L.G.; Palomo, J.M.; da Matta Cid Pinto, L.S.; de Sousa, A.A.; Gribel, B.F.; Oliveira, D.D. Mini Hyrax vs Hyrax Expanders in the Rapid Palatal Expansion in Adolescents with Posterior Crossbite: A Randomized Controlled Clinical Trial. Prog Orthod. 2021, 22, 30. [Google Scholar] [CrossRef]
- Celenk-Koca, T.; Erdinc, A.E.; Hazar, S.; Harris, L.; English, J.D.; Akyalcin, S. Evaluation of Miniscrew-Supported Rapid Maxillary Expansion in Adolescents: A Prospective Randomized Clinical Trial. Angle Orthod. 2018, 88, 702–709. [Google Scholar] [CrossRef] [Green Version]
- Jia, H.; Zhuang, L.; Zhang, N.; Bian, Y.; Li, S. Comparison of Skeletal Maxillary Transverse Deficiency Treated by Microimplant-Assisted Rapid Palatal Expansion and Tooth-Borne Expansion during the Post-Pubertal Growth Spurt Stage. Angle Orthod. 2021, 91, 36–45. [Google Scholar] [CrossRef]
- Annarumma, F.; Posadino, M.; De Mari, A.; Drago, S.; Aghazada, H.; Gravina, G.M.; Qorri, E.; Silvestrini-Biavati, A.; Migliorati, M. Skeletal and Dental Changes after Maxillary Expansion with a Bone-Borne Appliance in Young and Late Adolescent Patients. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e363–e375. [Google Scholar] [CrossRef]
- Aljawad, H.; Lee, K.-M.; Lim, H.-J. Three-Dimensional Evaluation of Upper Airway Changes Following Rapid Maxillary Expansion: A Retrospective Comparison with Propensity Score Matched Controls. PLoS ONE 2021, 16, e0261579. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Ronsivalle, V.; Lagravere, M.; Leonardi, R.; Martina, S.; Isola, G. Transverse Dentoalveolar Response of Mandibular Arch after Rapid Maxillary Expansion (RME) with Tooth-Borne and Bone-Borne Appliances. Angle Orthod. 2020, 90, 680–687. [Google Scholar] [CrossRef]
- Torun, G.S. Soft Tissue Changes in the Orofacial Region after Rapid Maxillary Expansion: A Cone Beam Computed Tomography Study. J. Orofac. Orthop. 2017, 78, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Cheung, G.C.; Dalci, O.; Mustac, S.; Papageorgiou, S.N.; Hammond, S.; Darendeliler, M.A.; Papadopoulou, A.K. The Upper Airway Volume Effects Produced by Hyrax, Hybrid-Hyrax, and Keles Keyless Expanders: A Single-Centre Randomized Controlled Trial. Eur. J. Orthod. 2021, 43, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Kavand, G.; Lagravère, M.; Kula, K.; Stewart, K.; Ghoneima, A. Retrospective CBCT Analysis of Airway Volume Changes after Bone-Borne vs Tooth-Borne Rapid Maxillary Expansion. Angle Orthod. 2019, 89, 566–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lotfi, V.; Ghoneima, A.; Lagravere, M.; Kula, K.; Stewart, K. Three-Dimensional Evaluation of Airway Volume Changes in Two Expansion Activation Protocols. Int. Orthod. 2018, 16, 144–157. [Google Scholar] [CrossRef] [PubMed]
- Alcin, R.; Malkoç, S. Does Mini-Implant-Supported Rapid Maxillary Expansion Cause Less Root Resorption than Traditional Approaches? A Micro-Computed Tomography Study. Korean J. Orthod. 2021, 51, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Chun, J.-H.; de Castro, A.C.R.; Oh, S.; Kim, K.-H.; Choi, S.-H.; Nojima, L.I.; Nojima, M.d.C.G.; Lee, K.-J. Skeletal and Alveolar Changes in Conventional Rapid Palatal Expansion (RPE) and Miniscrew-Assisted RPE (MARPE): A Prospective Randomized Clinical Trial Using Low-Dose CBCT. BMC Oral Health 2022, 22, 114. [Google Scholar] [CrossRef]
- Yildirim, M.; Akin, M. Comparison of Root Resorption after Bone-Borne and Tooth-Borne Rapid Maxillary Expansion Evaluated with the Use of Microtomography. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 182–190. [Google Scholar] [CrossRef]
- Negrisoli, S.; Angelieri, F.; Gonçalves, J.R.; da Silva, H.D.P.; Maltagliati, L.Á.; Raphaelli Nahás-Scocate, A.C. Assessment of the Bone Thickness of the Palate on Cone-Beam Computed Tomography for Placement of Miniscrew-Assisted Rapid Palatal Expansion Appliances. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 849–857. [Google Scholar] [CrossRef]
- Suzuki, H.; Moon, W.; Previdente, L.H.; Suzuki, S.S.; Garcez, A.S.; Consolaro, A. Miniscrew-Assisted Rapid Palatal Expander (MARPE): The Quest for Pure Orthopedic Movement. Dent. Press J. Orthod. 2016, 21, 17–23. [Google Scholar] [CrossRef]
- Beretta, M.; Poli, P.P.; Maiorana, C. Accuracy of Computer-Aided Template-Guided Oral Implant Placement: A Prospective Clinical Study. J. Periodontal Implant Sci. 2014, 44, 184–193. [Google Scholar] [CrossRef] [Green Version]
- Brunetto, D.P.; Sant’Anna, E.F.; Machado, A.W.; Moon, W. Non-Surgical Treatment of Transverse Deficiency in Adults Using Microimplant-Assisted Rapid Palatal Expansion (MARPE). Dent. Press J. Orthod. 2017, 22, 110–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bazargani, F.; Feldmann, I.; Bondemark, L. Three-Dimensional Analysis of Effects of Rapid Maxillary Expansion on Facial Sutures and Bones: A Systematic Review. Angle Orthod. 2013, 83, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Garrett, B.J.; Caruso, J.M.; Rungcharassaeng, K.; Farrage, J.R.; Kim, J.S.; Taylor, G.D. Editor’s Summary, Q & A, Reviewer’s Critique: Skeletal Effects to the Maxilla after Rapid Maxillary Expansion Assessed with Cone-Beam Computed Tomography. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 8–9. [Google Scholar] [CrossRef]
- Garib, D.G.; Henriques, J.F.C.; Janson, G.; Freitas, M.R.; Coelho, R.A. Rapid Maxillary Expansion—Tooth Tissue-Borne Versus Tooth-Borne Expanders: A Computed Tomography Evaluation of Dentoskeletal Effects. Angle Orthod. 2005, 75, 548–557. [Google Scholar] [CrossRef]
- An, J.-S.; Seo, B.-Y.; Ahn, S.-J. Differences in Dentoskeletal and Soft Tissue Changes Due to Rapid Maxillary Expansion Using a Tooth-Borne Expander between Adolescents and Adults: A Retrospective Observational Study. Korean J. Orthod. 2022, 52, 131–141. [Google Scholar] [CrossRef]
- Yi, F.; Liu, S.; Lei, L.; Liu, O.; Zhang, L.; Peng, Q.; Lu, Y. Changes of the Upper Airway and Bone in Microimplant-Assisted Rapid Palatal Expansion: A Cone-Beam Computed Tomography (CBCT) Study. XST 2020, 28, 271–283. [Google Scholar] [CrossRef]
- Cirulli, N.; Ballini, A.; Cantore, S.; Farronato, D.; Inchingolo, F.; Dipalma, G.; Gatto, M.; Bonetti, G.A. Mixed Dentition Space Analysis of a Southern Italian Population: New Regression Equations for Unerupted Teeth. J. Biol. Regul. Homeost. Agents 2015, 29, 515–520. [Google Scholar]
- Cantore, S.; Ballini, A.; Farronato, D.; Malcangi, G.; Dipalma, G.; Assandri, F.; Garagiola, U.; Inchingolo, F.; De Vito, D.; Cirulli, N. Evaluation of an Oral Appliance in Patients with Mild to Moderate Obstructive Sleep Apnea Syndrome Intolerant to Continuous Positive Airway Pressure Use: Preliminary Results. Int. J. Immunopathol. Pharm. 2016, 29, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Malcangi, G.; Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Garibaldi, M.; Inchingolo, A.M.; Piras, F.; Cardarelli, F.; Settanni, V.; et al. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Cozzani, M.; Sadri, D.; Nucci, L.; Jamilian, P.; Pirhadirad, A.P.; Jamilian, A. The Effect of Alexander, Gianelly, Roth, and MBT Bracket Systems on Anterior Retraction: A 3-Dimensional Finite Element Study. Clin. Oral Investig. 2020, 24, 1351–1357. [Google Scholar] [CrossRef]
- Melsen, B. Palatal Growth Studied on Human Autopsy Material. A Histologic Microradiographic Study. Am. J. Orthod. 1975, 68, 42–54. [Google Scholar] [CrossRef]
- Copello, F.M.; Marañón-Vásquez, G.A.; Brunetto, D.P.; Caldas, L.D.; Masterson, D.; Maia, L.C.; Sant’Anna, E.F. Is the Buccal Alveolar Bone Less Affected by Mini-Implant Assisted Rapid Palatal Expansion than by Conventional Rapid Palatal Expansion?—A Systematic Review and Meta-Analysis. Orthod. Craniofac. Res. 2020, 23, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of Children with Removable Functional Appliance with Microchip Integrated during Covid-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar] [CrossRef]
- Di Venere, D.; Nardi, G.M.; Lacarbonara, V.; Laforgia, A.; Stefanachi, G.; Corsalini, M.; Grassi, F.R.; Rapone, B.; Pettini, F. Early Mandibular Canine-Lateral Incisor Transposition: Case Report. Oral Implant. 2017, 10, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Di Venere, D.; Pettini, F.; Nardi, G.M.; Laforgia, A.; Stefanachi, G.; Notaro, V.; Rapone, B.; Grassi, F.R.; Corsalini, M. Correlation between Parodontal Indexes and Orthodontic Retainers: Prospective Study in a Group of 16 Patients. Oral Implant. 2017, 10, 78–86. [Google Scholar] [CrossRef]
- Di Venere, D.; Corsalini, M.; Nardi, G.M.; Laforgia, A.; Grassi, F.R.; Rapone, B.; Pettini, F. Obstructive Site Localization in Patients with Obstructive Sleep Apnea Syndrome: A Comparison between Otolaryngologic Data and Cephalometric Values. Oral Implant. 2017, 10, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Ceci, S.; Patano, A.; Inchingolo, A.M.; Montenegro, V.; Di Pede, C.; Malcangi, G.; Marinelli, G.; Coloccia, G.; Garibaldi, M.; et al. Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP® Devices: A Retrospective Study. Appl. Sci. 2022, 12, 3259. [Google Scholar] [CrossRef]
- Patano, A.; Cirulli, N.; Beretta, M.; Plantamura, P.; Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Marinelli, G.; Scarano, A.; et al. Education Technology in Orthodontics and Paediatric Dentistry during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6056. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Cozzani, M.; Nucci, L.; Lupini, D.; Dolatshahizand, H.; Fazeli, D.; Barzkar, E.; Naeini, E.; Jamilian, A. The Ideal Insertion Angle after Immediate Loading in Jeil, Storm, and Thunder Miniscrews: A 3D-FEM Study. Int. Orthod. 2020, 18, 503–508. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef] [PubMed]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/ Year | Study Design | Sample Size | Data Collection | Average Age (Years Old) | Type of Appliance | Protocol of Expansion | Features of the Screw | Amout of Expansion Achieved (mm) | Outcomes | Retention Period |
|---|---|---|---|---|---|---|---|---|---|---|
| Gökçe, 2021 | Retrospective | 54 (25 M, 29 F) | Pretreatment (T0) and posttreatment (T1) Postero Anterior cephalometric radiographs | 13.28 ± 1.20 (TBB) 13.08 ± 1.06 (TTB) 12.05 ± 1.35 (TB) | -TBB -TTB -TB | First week 2 turns/day and then 1 turn/day 1 turn = 0.25 mm | 9 mm Hyrax expansion screw (G&H Orthodontics, Franklin, IN, USA) | Intermolar width: TB = 5.5 mm TTB = 4.47 mm BB = 6.71 mm | Skeletal changes are more evident in TTB and TBB groups | 3 months |
| Yildirim, 2018 | Observational | 20 (11 F, 9 M) | Micro CT device on premolar teeth after expansion and extraction | 11–16 (mean age 14.31 ± 1.36) | BB and TTB in the same patient using modified device | N.D. | Hyrax screw | N.D. | Root resorptions are more frequent in the TTB group, mostly in the apical and middle thirds | 3 months |
| Canan, 2017 | RCT | 47 (25 F, 22 M) | Superimposition of 3D digital maxillary dental models; OHIP-14 questionnaire to value quality of life | 12.63 ± 1.36 (TB) 12.92 ± 1.07 (BB) 13.41 ± 0.88 (HB) | -TB -BB -TBB | 2 turns/day 1 turn = 0.25 mm | 9 mm Hyrax; Lewa-Dental, Remchingen, Germany) | Mean turns = 26; Mean screw expansion = 6.5 mm | Dentoalveolar maxillary expansion with mild relapse in all groups; Lower expansion of the BB on the right side; Spontaneous interdental expansion in the mandibular dentitions | 6 months |
| Silveira, 2021 | RCT | 34 | Digitally superimposed pre-treatment and post-retention 3D intraoral scans on the palatal rugae using the software 3DSlicer | 11–16 year | -Hyrax (TB) -Mini-hyrax (TB) | 2 turns/day 1 turn = 0.25 mm | −8 mm mini expander jackscrew (Dynaflex, Saint Ann, USA) −9 mm Hyrax jackscrew (Morelli, Sorocaba, Brazil) | Mean turns = 30; Mean screw expansion = 7.5 mm | No significant differences in dental effects, impact on quality of life and pain perception | 6 months |
| Kavand, 2019 | Retrospective | 36 | CBCT at T0 before expansion and T1 post retention | 14.7 years (BB) 14.4 years (TB) | -BB -TB | 2 turns/day 1 turn = 0.25 mm | Jackscrew (Palex II Extra-Mini Expander, Su mmit Orthodontic Services, Munroe Falls, OH, USA) | Mean palatal width expansion TB = 1.5 ± 0.4 BB = 2.2 ± 0.3 mm | Increased volume of nasal cavity and nasopharynx; Increased maxillary dental and skeletal width in both groups; Buccal tipping of maxillary molars in TB. | 3 months |
| Alcin, 2021 | RCT | 20 (12 F, 8 M) | Micro-CT of maxillary first premolars | 12–15 | -TBB -TB -Acrylic-bonded TB -Full-coverage TB | 1turn/day 1 turn = 0.25 mm | Hyrax screw | Mean turns = 34; | All expansion appliances cause root resorption, mostly on the buccal surface; TBB causes lesser root resorption than TB appliances. | 3 months |
| Celenk-Koca, 2018 | RCT | 40 TB group: 12 F, 8 M; BB group 13 F, 7 M | CBCT evaluation of: -transverse skeletal widths; -buccal bone thickness; -tooth inclination -root length | 13.84 ± 1.36 (TB) 13.81 ± 1.23 (BB) | -TB -BB | 2 turns/day 1 turn = 0.25 mm | Hyrax screw | Molar width: TB = 4.2 + 1.7 BB = 4.5 + 1.3 | BB increased the maxillary suture opening more than 2.5 times than TB and did not result in any dental side effects | 6 months |
| Annarumma, 2021 | Retrospective | 24 (12 M, 12 F) | CBCT evaluation of: -maxillary width; -inclination of the alveolar process; -tooth inclination; -vertical dental height; -periodontal tissues | 13.9 | -BB on 4 miniscrews | 2 turns/day | Hyrax screw on BB | mean expansion screw = 8.12 ± 2.98 mm | BB expansion was effective with negligible dental effects | 12 months |
| Aljawad, 2021 | Case-control retrospective study | 33 17 TB 16 control group | Upper airway dimensions (CBCT) | mean age 12.6 ± 1.8 | -TB | 2 turns/day 1 turn = 0.25 mm | Hyrax screw (Dentaurum, Ispringen, Germany) | N.D. | RME causes an increase in upper airway dimensions | 3 months |
| Torun, 2017 | Retrospective study | 28 (10 M, 18 F) | Measurements of soft tissue with CBCT at T0, T1 | 13.91 ± 1.8 | TB | 2 turns/day 1 turn = 0.25 mm | Hyrax screw (Dentaurum, Ispringen, Germany) | Mean Screw expansion: 9–10 mm | significant changes in facial soft tissues P < 0.001 | 6 months |
| Lotfi, 2018 | Retrospective study | 20 (8 M, 12 F) | Measurements of upper airway volume changes with CBCT at T0, T1 | 12. 3 ± 1.9 | -TB | 2 turns/day | Hyrax screw | N.D | Significant changes in nasal cavity volume | 6 months |
| Chun, 2022 | Prospective RCT | 40 TB group: 20 (6 M, 14 F) MARPE group (8 M, 12 F) | CBCT evaluation of: -skeletal changes; -dentoalveolar changes; -periodontal changes | 14.0 ± 4.3 years | -TB -MARPE | 1 turn/day for 35 days 1 turn = 0.20 mm | Hyrax expander (Dentaurum, Ispringen, Germany) | 7 mm screw expansion | Greater increase in nasal width in the molar region (M-NW) and greater palatine foramen (GPF) in the MARPE group compared to the TB group; Similar dentoalveolar changes except for the maxillary width (PM-MW, M-MW). The MARPE group presented greater bilateral first premolar (PM-MW) and molar (M-MW) maxillary width in relation to the TB group; Lesser buccal displacement of the anchor teeth in the MARPE group. | 3 months |
| Jia, 2021 | Prospective RCT | 60 MARPE 30 TB 30 | CBCT and dental cast | 14.8 ± 1.5 (TB) 15.1 ± 1.6 (MARPE) | -MARPE -TB | 2 turns/day 1 turn = 0.25 | MARPE TTB: jackscrew (length: 12 mm; anatomic expander type: ‘‘s;’’ Forestadent, Pforzheim, Germany) TB HYRAX: jackscrew (anatomic expander type; Forestadent) | Mean expansion at maxillary basal bone TTB: 4.53 TB: 4.53 | MARPE enabled more predictable and greater skeletal expansion, less buccal tipping and alveolar height loss on anchorage teeth. | 3 months |
| Akan, 2021 | RCT | 32 16 TB 16 TBB | Changes in soft tissues before RME (T0) and post-retention (T1) evaluated by stereophotogra mmetry | 13.4 ± 1.3 | -TB -TBB | First week 2 turns/day and then 1 turn /day 1 turn = 0.25 mm | TB:Hyrax screw (Dentaurum, Ispringen, Germany) MARPE TTB mini-screws 2 mm diameter and 9 mm length (Benefit mini-implants; PSM Medical Solutions) | Mean numbers of activations were 25.25 ± 4.42 turns in hyrax group and 24.88 ± 3.40 turns in hybrid hyrax group. | Both appliances had effects on soft tissue profile; Anterior face height and lower face height increased in both groups; Upper lip length increased by 0.36 mm in theTBB group and 0.10 mm in the TB group. | 3 months |
| Lo Giudice, 2020 | Retrospective study | 33 | Linear and angular measurements in the coronal view to assess buccal inclinations and widths of mandibular posterior units. | 14.4 ± 1.3 (TB) 14.7 ± 1.4 (BB) | -TB -BB | 2 turns/day 1 turn = 0.25 mm | Hyrax miniscrew (Palex II ExtraMini Expander, Su mmit Orthodontic Services, Munroe Falls, OH, USA; Figure 1B) | 16–26 width TB = 4.20 ± 1.39 BB = 3.02 ± 1.48 | A clinically significant gain of space in the mandibular arch should not be expected after RME | 6 months |
| Cheung, 2021 | RCT | 44 | Measurements of upper airway volume changes with CBCT at T0, T1 | ND | -TB -TBB | 2 turns/day 1 turn = 0.25 mm | Hyrax screw (Hyrax, Dentaurum, Ispringen, Germany) Keles keyless expander (Keles, Istanbul, Turkey) | N.D. | No statistically significant difference across the TB and TBB | 6 months |
| Measurements | Norm | Pre-Treatment | Post-Treatment |
|---|---|---|---|
| Anterior Cranial Base(S-N) | 74.5 ± 3 | 66 | 66.5 |
| Facial Axis (BaN-PTGn) | 90° ± 3 | 84.4° | 85.8° |
| Mandibular Lenght (Goc-Me) | 74.5 ± 5 | 61.9 | 64 |
| Posterior Cranial Base (S-Ar) | 34 ± 3 | 30.9 | 31.4 |
| Height Mandibular Ramus (Ar-Goc) | 47.5 ± 5 | 33.9 | 38.3 |
| Saddle angle: (N-S-Ar) | 123° ± 5 | 120.4° | 118.8° |
| Articular angle (S-Ar-Goc) | 143° ± 7 | 150.1° | 149.6° |
| Gonial angle (Ar-Goc-Me) | 130° ± 7 | 128.6° | 129.1° |
| Upper gonial angle (Ar-Goc-N) | 52° ± 3 | 53° | 52.4° |
| Lower gonial angle (Me-Goc-N) | 70° ± 2 | 75.6° | 76.7° |
| Anterior facial height (N-Me) | 113 ± 7 | 105.2 | 108.9 |
| Posterior facial height (S-Goc) | 77.5 ± 7.5 | 62.6 | 67.3 |
| Jarabak Facial Proportion % | 61% ± 3 | 59.5% | 61.8% |
| SNA | 82° ± 2 | 80.9° | 79.7° |
| SNB | 80° ± 2 | 75.1° | 76° |
| ANB | 2° ± 2 | 5.8° | 3.7° |
| U1—palatal plane | 110° ± 2 | 112.7° | 111.2° |
| IMPA | 90° ± 3 | 96.9° | 97.8° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.D.; Ferrara, I.; Viapiano, F.; Netti, A.; Campanelli, M.; Buongiorno, S.; Latini, G.; Carpentiere, V.; Ciocia, A.M.; Ceci, S.; et al. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children 2022, 9, 1046. https://doi.org/10.3390/children9071046
Inchingolo AD, Ferrara I, Viapiano F, Netti A, Campanelli M, Buongiorno S, Latini G, Carpentiere V, Ciocia AM, Ceci S, et al. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children. 2022; 9(7):1046. https://doi.org/10.3390/children9071046
Chicago/Turabian StyleInchingolo, Alessio Danilo, Irene Ferrara, Fabio Viapiano, Anna Netti, Merigrazia Campanelli, Silvio Buongiorno, Giulia Latini, Vincenzo Carpentiere, Anna Maria Ciocia, Sabino Ceci, and et al. 2022. "Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report" Children 9, no. 7: 1046. https://doi.org/10.3390/children9071046