
Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature

 ,
,  ,
,  , , ,
, , ,  , , ,
, , ,  , , , , ,
, , , , ,  , , ,
, , ,  , , , , ,
, , , , ,  , ,
, ,  and
and  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
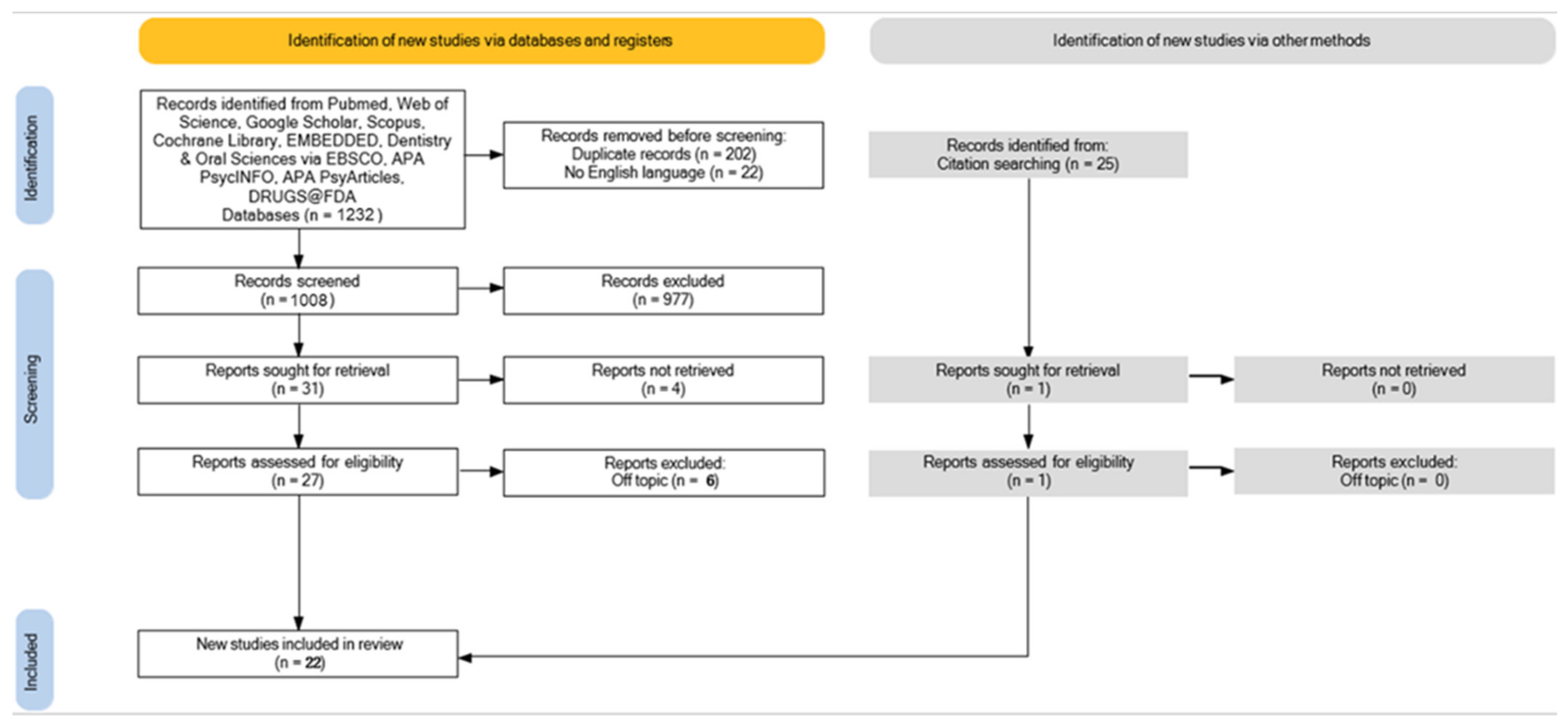
2.1. Search Processing
2.2. Inclusion Criteria
2.3. Data Processing
3. Results
Characteristics of Included Articles
4. Discussion
4.1. Microbiota and Orthodontics

| Authors | Type of Study | Object | Study Design and Timeline | Results |
|---|---|---|---|---|
| Shokeen, 2021 [42] | Longitudinal study | Study bacterial shift in aligner orthodontic therapy | Microbiome analysis of supragingival plaque (16S rRNA) collected from 12 subjects at baseline and at 1, 3, 6, and 12-months after. | Orthodontic therapy is a stressor for oral environment. Clear aligner showed improved oral health condition |
| Padala RG, 2019 [83] | Randomized clinical trial, split-mouth | Impact of fluoride in elastomeric appliances to control Streptococcus mutans in orthodontic subjects | 30 subjects, with 2 experimental periods of 3 weeks and a 3-week. Fluoridated elastics vs. non-fluoridated ones. | Fluoridated elastics were effective to decrease the Streptococcus mutans level in dental plaque. |
| Beerens MW, 2017 [79] | Cross-sectional study | Study caries risk assessment in orthodontic subjects | Dental plaque before debracketing and white spot lesions identified after debracketing. Microbiological analysis of the aciduric flora (Strept. mutans, Lactobacillus and Candida a.) | No significant differences between groups |
| Shimpo, 2022 [44] | Randomized control trial | Study the effectiveness of disinfection treatment, with the use of fluoride | White spot lesions identified by quantitative light-induced fluorescence, and bacteria by bacterial culture | Disinfection with PMTC and fluoride, shows efficacy in caries, when used on the tooth surface |
| Reichardt, 2019 [80] | Pilot study | Study qualitative and quantitative bacterial shift after insertion of orthodontic devices | Total 10 patients (12–15 years old). Microbiological samples at T0 and 1 week after at premolars and molars of the right upper side. Microbial evaluations by mass spectrometry | The orthodontic therapy leads to important shift in the oral bacteria, with gingivitis and raised risk of decay |
| Gujar, 2019 [82] | Clinical trial | Quantify orange and red bacteria in subjects with orthodontic aligners therapy, fixed labial, and lingual appliances | Total 60 patients, 20 treated with aligners, 20 with labial fixed appliances, and 20 with lingual fixed appliances. After a month brackets and aligners removed and DNA-DNA hybridization | After 1 month: bacterial contamination was major on brackets than aligners; in lingual fixed appliances was major than in labial-fixed appliances. |
| Ko-Adams, 2020 [81] | Clinical trial | In early orthodontic patients study the Streptococcus Mutans level, aerobic and facultative anaerobe bacterial PC quantitative | Plaque samples to evaluate the amount of Streptococcus Mutans and PCs from 17 patients after 1 month. | Statistically significant reduction in Streptococcus Mutans but not in PCs, and is highly variable across individuals |
| Ali, 022 [78] | Double-blind, randomized clinical trial study | Study the effectiveness of nano-silver, chlorhexidine, or fluoride mouthwashes on white spot lesions | Clinical examination of white spot lesions in 42 patients; 3 groups made to divide the type of brushing during the orthodontic therapy | Statistically significant discrepancies through the 3 groups. White spot lesions in the nanosilver group are lower than CHX and fluoride group |
4.2. Microbiota and Remineralization
4.3. Microbiota and Dental Demineralization
4.4. Microbiota and the Influence of Probiotics and Prebiotics on Dental Remineralization
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AT | ALIGNERS THERAPY |
| CHX | chlorhexidine |
| CPP-ACP | phosphopeptides-amorphous calcium phosphate |
| CT | computer tomography scan |
| DC | dental caries |
| DMFT | the sum of the number of decayed, missing due to caries, and filled teeth in the permanent teeth |
| DNA | deoxyribonucleic acid |
| ECC | early childhood caries |
| ER-YAG LASER | yttrio-aluminum-garnet laser |
| FT | FIXED THERAPY |
| HOMINGS | human oral microbe identification |
| GI | gastrointestinal system |
| Illumina MiSeq | a benchtop instrument that utilizes a single-lane flow cell and a reagent cartridge supplied in kit form |
| Lactobacillus spp. | Lactobacillus species |
| MB | microbiota |
| MIH | molar-incisor hypomineralization |
| MM | microbiome |
| OM | oral microbiota |
| PCA | principal component analysis |
| pH | potential of hydrogen |
| RCTs | randomized controlled trials |
| RNA | ribonucleic acid |
| RTI | respiratory tract infections |
| S. mutans | Streptococcus mutans |
| SSK12 | Streptococcus salivarius K12 |
| WSL | white spot lesion |
References
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of Dental Caries in Primary and Permanent Teeth in Children and Young Adults. J. Clin. Microbiol. 2008, 46, 1407–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sender, R.; Fuchs, S.; Milo, R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLoS Biol. 2016, 14, e1002533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inchingolo, A.D.; Cazzolla, A.P.; Di Cosola, M.; Greco Lucchina, A.; Santacroce, L.; Charitos, I.A.; Topi, S.; Malcangi, G.; Hazballa, D.; Scarano, A.; et al. The Integumentary System and Its Microbiota between Health and Disease. J. Biol. Regul. Homeost. Agents 2021, 35, 303–321. [Google Scholar] [CrossRef] [PubMed]
- Piombo, E.; Abdelfattah, A.; Droby, S.; Wisniewski, M.; Spadaro, D.; Schena, L. Metagenomics Approaches for the Detection and Surveillance of Emerging and Recurrent Plant Pathogens. Microorganisms 2021, 9, 188. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-H.; Chung, S.W.; Auh, Q.-S.; Hong, S.-J.; Lee, Y.-A.; Jung, J.; Lee, G.-J.; Park, H.J.; Shin, S.-I.; Hong, J.-Y. Progress in Oral Microbiome Related to Oral and Systemic Diseases: An Update. Diagnostics 2021, 11, 1283. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, G.; Lau, H.C.-H.; Yu, J. Metagenomic Sequencing for Microbial DNA in Human Samples: Emerging Technological Advances. Int. J. Mol. Sci. 2022, 23, 2181. [Google Scholar] [CrossRef]
- Fiehn, O.; Kloska, S.; Altmann, T. Integrated Studies on Plant Biology Using Multiparallel Techniques. Curr. Opin. Biotechnol. 2001, 12, 82–86. [Google Scholar] [CrossRef]
- Fiehn, O. Combining Genomics, Metabolome Analysis, and Biochemical Modelling to Understand Metabolic Networks. Comp. Funct. Genom. 2001, 2, 155–168. [Google Scholar] [CrossRef] [Green Version]
- Goodacre, R.; Vaidyanathan, S.; Dunn, W.B.; Harrigan, G.G.; Kell, D.B. Metabolomics by Numbers: Acquiring and Understanding Global Metabolite Data. Trends Biotechnol. 2004, 22, 245–252. [Google Scholar] [CrossRef]
- Weckwerth, W. Metabolomics in Systems Biology. Annu. Rev. Plant Biol. 2003, 54, 669–689. [Google Scholar] [CrossRef]
- Santacroce, L.; Inchingolo, F.; Topi, S.; Del Prete, R.; Di Cosola, M.; Charitos, I.A.; Montagnani, M. Potential Beneficial Role of Probiotics on the Outcome of COVID-19 Patients: An Evolving Perspective. Diabetes Metab. Syndr. 2021, 15, 295–301. [Google Scholar] [CrossRef]
- Reitano, E.; de’Angelis, N.; Gavriilidis, P.; Gaiani, F.; Memeo, R.; Inchingolo, R.; Bianchi, G.; de’Angelis, G.L.; Carra, M.C. Oral Bacterial Microbiota in Digestive Cancer Patients: A Systematic Review. Microorganisms 2021, 9, 2585. [Google Scholar] [CrossRef]
- Segata, N.; Haake, S.K.; Mannon, P.; Lemon, K.P.; Waldron, L.; Gevers, D.; Huttenhower, C.; Izard, J. Composition of the Adult Digestive Tract Bacterial Microbiome Based on Seven Mouth Surfaces, Tonsils, Throat and Stool Samples. Genome Biol. 2012, 13, R42. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, T.S.; Hayward, M.R.; Coelho, L.P.; Li, S.S.; Costea, P.I.; Voigt, A.Y.; Wirbel, J.; Maistrenko, O.M.; Alves, R.J.; Bergsten, E.; et al. Extensive Transmission of Microbes along the Gastrointestinal Tract. eLife 2019, 8, e42693. [Google Scholar] [CrossRef]
- Pacifici, L.; Santacroce, L.; Dipalma, G.; Haxhirexha, K.; Topi, S.; Cantore, S.; Altini, V.; Pacifici, A.; Vito, D.D.; Pettini, F.; et al. Gender Medicine: The Impact of Probiotics on Male Patients. Clin. Ter. 2021, 172, 8–15. [Google Scholar]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhang, D.; Jia, H.; Feng, Q.; Wang, D.; Liang, D.; Wu, X.; Li, J.; Tang, L.; Li, Y.; et al. The Oral and Gut Microbiomes Are Perturbed in Rheumatoid Arthritis and Partly Normalized after Treatment. Nat. Med. 2015, 21, 895–905. [Google Scholar] [CrossRef]
- Metabolic and Community Synergy of Oral Bacteria in Colorectal Cancer MSphere. Available online: https://journals.asm.org/doi/10.1128/mSphere.00102-16 (accessed on 20 May 2022).
- Zeller, G.; Tap, J.; Voigt, A.Y.; Sunagawa, S.; Kultima, J.R.; Costea, P.I.; Amiot, A.; Böhm, J.; Brunetti, F.; Habermann, N.; et al. Potential of Fecal Microbiota for Early-Stage Detection of Colorectal Cancer. Mol. Syst. Biol. 2014, 10, 766. [Google Scholar] [CrossRef]
- Vanhée, T.; Poncelet, J.; Cheikh-Ali, S.; Bottenberg, P. Prevalence, Caries, Dental Anxiety and Quality of Life in Children with MIH in Brussels, Belgium. J. Clin. Med. 2022, 11, 3065. [Google Scholar] [CrossRef]
- Margolis, H.C.; Moreno, E.C. Composition of Pooled Plaque Fluid from Caries-Free and Caries-Positive Individuals Following Sucrose Exposure. J. Dent. Res. 1992, 71, 1776–1784. [Google Scholar] [CrossRef]
- Signorini, L.; Ballini, A.; Arrigoni, R.; De Leonardis, F.; Saini, R.; Cantore, S.; De Vito, D.; Coscia, M.F.; Dipalma, G.; Santacroce, L.; et al. Evaluation of a Nutraceutical Product with Probiotics, Vitamin D, Plus Banaba Leaf Extracts (Lagerstroemia Speciosa) in Glycemic Control. Endocr Metab. Immune. Disord. Drug. Targets 2021, 21, 1356–1365. [Google Scholar] [CrossRef]
- Signorini, L.; De Leonardis, F.; Santacroce, L.; Haxhirexha, K.; Topi, S.; Fumarola, L.; Dipalma, G.; Coscia, M.F.; Inchingolo, F. Probiotics May Modulate the Impact of Aging on Adults. J. Biol. Regul. Homeost Agents 2020, 34, 1601–1606. [Google Scholar] [CrossRef]
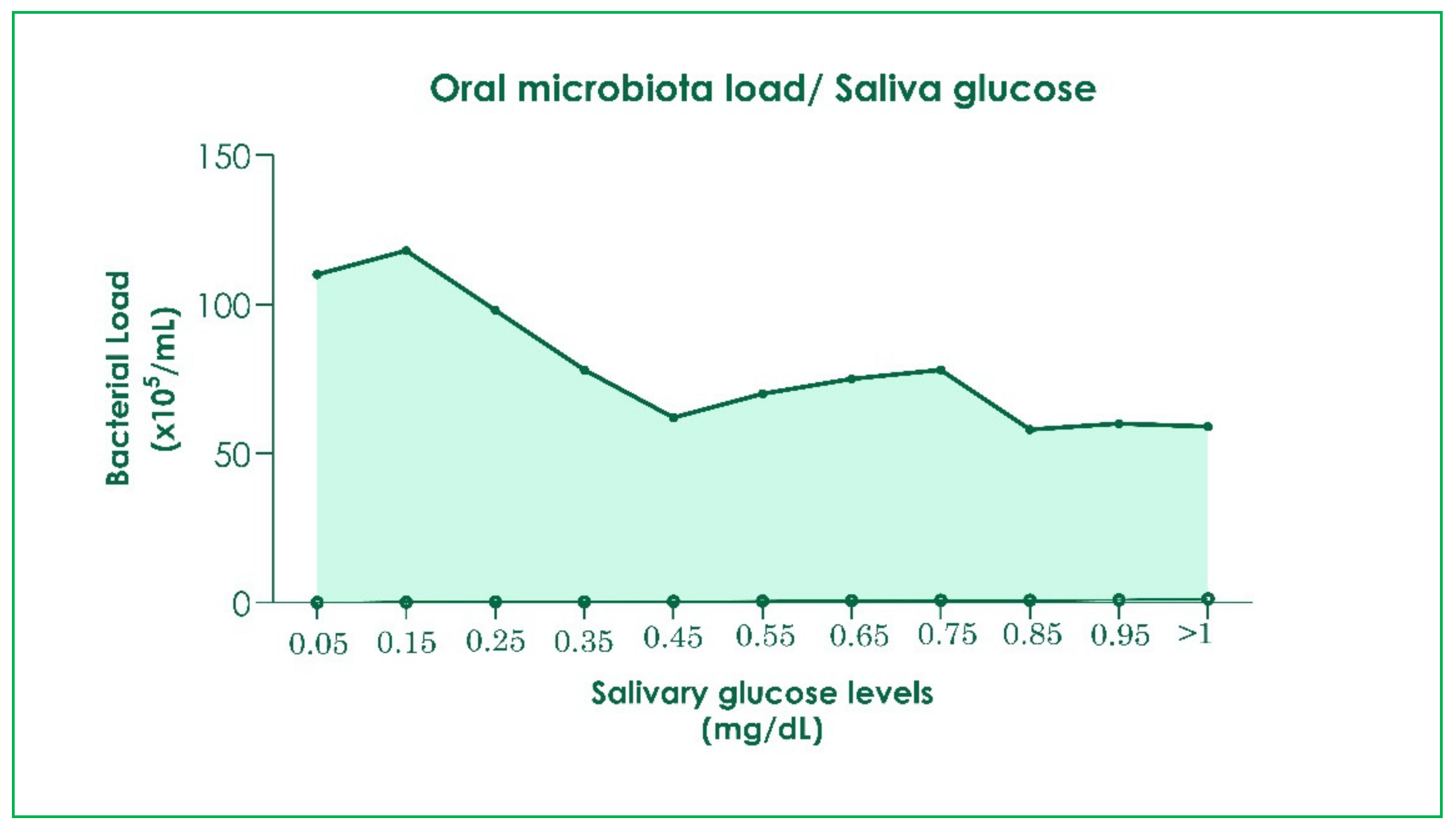
- Goodson, J.M.; Hartman, M.-L.; Shi, P.; Hasturk, H.; Yaskell, T.; Vargas, J.; Song, X.; Cugini, M.; Barake, R.; Alsmadi, O.; et al. The Salivary Microbiome Is Altered in the Presence of a High Salivary Glucose Concentration. PLoS ONE 2017, 12, e0170437. [Google Scholar] [CrossRef] [Green Version]
- Isacco, C.G.; Ballini, A.; De Vito, D.; Nguyen, K.C.D.; Cantore, S.; Bottalico, L.; Quagliuolo, L.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; et al. Rebalancing the Oral Microbiota as an Efficient Tool in Endocrine, Metabolic and Immune Disorders. Endocr Metab. Immune Disord. Drug Targets 2021, 21, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Al-Zyoud, W.; Hajjo, R.; Abu-Siniyeh, A.; Hajjaj, S. Salivary Microbiome and Cigarette Smoking: A First of Its Kind Investigation in Jordan. Int. J. Environ. Res. Public Health 2020, 17, 256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contaldo, M.; Fusco, A.; Stiuso, P.; Lama, S.; Gravina, A.G.; Itro, A.; Federico, A.; Itro, A.; Dipalma, G.; Inchingolo, F.; et al. Oral Microbiota and Salivary Levels of Oral Pathogens in Gastro-Intestinal Diseases: Current Knowledge and Exploratory Study. Microorganisms 2021, 9, 1064. [Google Scholar] [CrossRef] [PubMed]
- Santacroce, L.; Sardaro, N.; Topi, S.; Pettini, F.; Bottalico, L.; Cantore, S.; Cascella, G.; Del Prete, R.; Dipalma, G.; Inchingolo, F. The Pivotal Role of Oral Microbiota in Health and Disease. J. Biol. Regul. Homeost. Agents 2020, 34, 733–737. [Google Scholar] [CrossRef] [PubMed]
- Nakajo, K.; Takahashi, N.; Beighton, D. Resistance to Acidic Environments of Caries-Associated Bacteria: Bifidobacterium Dentium and Bifidobacterium Longum. Caries Res. 2010, 44, 431–437. [Google Scholar] [CrossRef]
- Pacifici, A.; Pacifici, L.; Nuzzolese, M.; Cascella, G.; Ballini, A.; Santacroce, L.; Dipalma, G.; Aiello, E.; Amantea, M.; Saini, R.; et al. The Alteration of Stress-Related Physiological Parameters after Probiotics Administration in Oral Surgeons with Different Degrees of Surgical Experience. Clin. Ter. 2020, 171, e197–e208. [Google Scholar] [CrossRef]
- Harper, D.S.; Loesche, W.J. Growth and Acid Tolerance of Human Dental Plaque Bacteria. Arch. Oral Biol. 1984, 29, 843–848. [Google Scholar] [CrossRef] [Green Version]
- Inchingolo, F.; Santacroce, L.; Ballini, A.; Topi, S.; Dipalma, G.; Haxhirexha, K.; Bottalico, L.; Charitos, I.A. Oral Cancer: A Historical Review. Int. J. Environ. Res. Public Health 2020, 17, 3168. [Google Scholar] [CrossRef]
- Horiuchi, M.; Washio, J.; Mayanagi, H.; Takahashi, N. Transient Acid-Impairment of Growth Ability of Oral Streptococcus, Actinomyces, and Lactobacillus: A Possible Ecological Determinant in Dental Plaque. Oral Microbiol. Immunol. 2009, 24, 319–324. [Google Scholar] [CrossRef]
- Obesity Alters Gut Microbial Ecology PNAS. Available online: https://www.pnas.org/doi/full/10.1073/pnas.0504978102 (accessed on 21 May 2022).
- Ballini, A.; Scacco, S.; Boccellino, M.; Santacroce, L.; Arrigoni, R. Microbiota and Obesity: Where Are We Now? Biology 2020, 9, 415. [Google Scholar] [CrossRef]
- Association between Diabetes-Related Factors and Clinical Periodontal Parameters in Type-2 Diabetes Mellitus BMC Oral Health Full Text. Available online: https://bmcoralhealth.biomedcentral.com/articles/10.1186/1472-6831-13-64 (accessed on 21 May 2022).
- Inchingolo, F.; Santacroce, L.; Cantore, S.; Ballini, A.; Del Prete, R.; Topi, S.; Saini, R.; Dipalma, G.; Arrigoni, R. Probiotics and EpiCor® in Human Health. J. Biol. Regul. Homeost. Agents 2019, 33, 1973–1979. [Google Scholar] [CrossRef]
- Cialiè Rosso, M.; Stilo, F.; Squara, S.; Liberto, E.; Mai, S.; Mele, C.; Marzullo, P.; Aimaretti, G.; Reichenbach, S.E.; Collino, M.; et al. Exploring Extra Dimensions to Capture Saliva Metabolite Fingerprints from Metabolically Healthy and Unhealthy Obese Patients by Comprehensive Two-Dimensional Gas Chromatography Featuring Tandem Ionization Mass Spectrometry. Anal. Bioanal. Chem. 2021, 413, 403–418. [Google Scholar] [CrossRef]
- DiCraciun, C.-I.; Neag, M.-A.; Catinean, A.; Mitre, A.-O.; Rusu, A.; Bala, C.; Roman, G.; Buzoianu, A.-D.; Muntean, D.-M.; Craciun, A.-E. The Relationships between Gut Microbiota and Diabetes Mellitus, and Treatments for Diabetes Mellitus. Biomedicines 2022, 10, 308. [Google Scholar] [CrossRef]
- Topi, S.; Santacroce, L.; Bottalico, L.; Ballini, A.; Inchingolo, A.D.; Dipalma, G.; Charitos, I.A.; Inchingolo, F. Gastric Cancer in History: A Perspective Interdisciplinary Study. Cancers 2020, 12, 264. [Google Scholar] [CrossRef] [Green Version]
- Albhaisi, Z.; Al-Khateeb, S.N.; Abu Alhaija, E.S. Enamel Demineralization during Clear Aligner Orthodontic Treatment Compared with Fixed Appliance Therapy, Evaluated with Quantitative Light-Induced Fluorescence: A Randomized Clinical Trial. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 594–601. [Google Scholar] [CrossRef]
- Shokeen, B.; Viloria, E.; Duong, E.; Rizvi, M.; Murillo, G.; Mullen, J.; Shi, B.; Dinis, M.; Li, H.; Tran, N.C.; et al. The Impact of Fixed Orthodontic Appliances and Clear Aligners on the Oral Microbiome and the Association with Clinical Parameters: A Longitudinal Comparative Study. Am. J. Orthod. Dentofac. Orthop. 2022, 161, e475–e485. [Google Scholar] [CrossRef]
- Ballini, A.; Gnoni, A.; De Vito, D.; Dipalma, G.; Cantore, S.; Gargiulo Isacco, C.; Saini, R.; Santacroce, L.; Topi, S.; Scarano, A.; et al. Effect of Probiotics on the Occurrence of Nutrition Absorption Capacities in Healthy Children: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Eur. Rev. Med. Pharm. Sci. 2019, 23, 8645–8657. [Google Scholar] [CrossRef]
- Shimpo, Y.; Nomura, Y.; Sekiya, T.; Arai, C.; Okada, A.; Sogabe, K.; Hanada, N.; Tomonari, H. Effects of the Dental Caries Preventive Procedure on the White Spot Lesions during Orthodontic Treatment—An Open Label Randomized Controlled Trial. J. Clin. Med. 2022, 11, 854. [Google Scholar] [CrossRef]
- Lombardo, L.; Ortan, Y.Ö.; Gorgun, Ö.; Panza, C.; Scuzzo, G.; Siciliani, G. Changes in the Oral Environment after Placement of Lingual and Labial Orthodontic Appliances. Prog. Orthod. 2013, 14, 28. [Google Scholar] [CrossRef] [Green Version]
- Mummolo, S.; Tieri, M.; Tecco, S.; Mattei, A.; Albani, F.; Giuca, M.R.; Marzo, G. Clinical Evaluation of Salivary Indices and Levels of Streptococcus Mutans and Lactobacillus in Patients Treated with Occlus-o-Guide. Eur. J. Paediatr. Dent. 2014, 15, 367–370. [Google Scholar]
- Al-Batayneh, O.B.; Jbarat, R.A.; Al-Khateeb, S.N. Effect of Application Sequence of Fluoride and CPP-ACP on Remineralization of White Spot Lesions in Primary Teeth: An in-Vitro Study. Arch. Oral Biol. 2017, 83, 236–240. [Google Scholar] [CrossRef]
- Apriani, A.; Widyarman, A.; Budiyanti, E.; Roeslan, B. Caries Activity and Ph Level Changes after Fluoride Varnish and Casein Phosphopeptides-Amorphous Calcium Phosphate Application on Children’s Saliva. Contemp. Clin. Dent. 2020, 11, 126. [Google Scholar] [CrossRef]
- Dipalma, G.; Inchingolo, A.D.; Inchingolo, F.; Charitos, I.A.; Di Cosola, M.; Cazzolla, A.P. Focus on the Cariogenic Process: Microbial and Biochemical Interactions with Teeth and Oral Environment. J. Biol. Regul. Homeost. Agents 2021, 35. [Google Scholar] [CrossRef]
- Montemurro, N.; Perrini, P.; Marani, W.; Chaurasia, B.; Corsalini, M.; Scarano, A.; Rapone, B. Multiple Brain Abscesses of Odontogenic Origin. May Oral Microbiota Affect Their Development? A Review of the Current Literature. Appl. Sci. 2021, 11, 3316. [Google Scholar] [CrossRef]
- Cury, J.A.; Tenuta, L.M.A. How to Maintain a Cariostatic Fluoride Concentration in the Oral Environment. Adv. Dent. Res. 2008, 20, 13–16. [Google Scholar] [CrossRef]
- Kozmos, M.; Virant, P.; Rojko, F.; Abram, A.; Rudolf, R.; Raspor, P.; Zore, A.; Bohinc, K. Bacterial Adhesion of Streptococcus mutans to Dental Material Surfaces. Molecules 2021, 26, 1152. [Google Scholar] [CrossRef]
- Devine, D.A.; Marsh, P.D. Prospects for the Development of Probiotics and Prebiotics for Oral Applications. J. Oral Microbiol. 2009, 1, 1949. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Saini, R.; Pettini, F.; Fotopoulou, E.A.; Saini, S.R.; Georgakopoulos, I.P.; Dipalma, G.; Gargiulo Isacco, C.; Inchingolo, F. Effect of Activated Charcoal Probiotic Toothpaste Containing Lactobacillus Paracasei and Xylitol on Dental Caries: A Randomized and Controlled Clinical Trial. J. Biol. Regul. Homeost. Agents 2019, 33, 977–981. [Google Scholar] [PubMed]
- Huang, X.; Zhang, K.; Deng, M.; Exterkate, R.A.M.; Liu, C.; Zhou, X.; Cheng, L.; Ten Cate, J.M. Effect of Arginine on the Growth and Biofilm Formation of Oral Bacteria. Arch. Oral Biol. 2017, 82, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Zaura, E.; Twetman, S. Critical Appraisal of Oral Pre- and Probiotics for Caries Prevention and Care. Caries Res. 2019, 53, 514–526. [Google Scholar] [CrossRef] [PubMed]
- Casu, C.; Mosaico, G.; Natoli, V.; Scarano, A.; Lorusso, F.; Inchingolo, F. Microbiota of the Tongue and Systemic Connections: The Examination of the Tongue as an Integrated Approach in Oral Medicine. Hygiene 2021, 1, 56–68. [Google Scholar] [CrossRef]
- Ballini, A.; Santacroce, L.; Cantore, S.; Bottalico, L.; Dipalma, G.; Topi, S.; Saini, R.; De Vito, D.; Inchingolo, F. Probiotics Efficacy on Oxidative Stress Values in Inflammatory Bowel Disease: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Endocr. Metab. Immune. Disord. Drug Targets 2019, 19, 373–381. [Google Scholar] [CrossRef]
- Gargiulo Isacco, C.; Ballini, A.; De Vito, D.; Michele Inchingolo, A.; Cantore, S.; Paduanelli, G.; Cao Diem Nguyen, K.; Danilo Inchingolo, A.; Dipalma, G.; Inchingolo, F. Probiotics in Health and Immunity: A First Step toward Understanding the Importance of Microbiota System in Translational Medicine. In Prebiotics and Probiotics—Potential Benefits in Nutrition and Health; Franco-Robles, E., Ramírez-Emiliano, J., Eds.; IntechOpen: London UK, 2020; ISBN 978-1-78985-921-8. [Google Scholar]
- Oral Microbiome and Preterm Birth: Correlation or Coincidence? A Narrative Review. Open Access Maced. J. Med. Sci. 2020, 14, 123–132.
- Campanella, V.; Syed, J.; Santacroce, L.; Saini, R.; Ballini, A.; Inchingolo, F. Oral Probiotics Influence Oral and Respiratory Tract Infections in Pediatric Population: A Randomized Double-Blinded Placebo-Controlled Pilot Study. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 8034–8041. [Google Scholar]
- Inchingolo, A.D.; Malcangi, G.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; De Leonardis, N.; et al. Benefits and Implications of Resveratrol Supplementation on Microbiota Modulations: A Systematic Review of the Literature. Int. J. Mol. Sci. 2022, 23, 4027. [Google Scholar] [CrossRef]
- Sang-Ngoen, T.; Czumbel, L.M.; Sadaeng, W.; Mikó, A.; Németh, D.I.; Mátrai, P.; Hegyi, P.; Tóth, B.; Csupor, D.; Kiss, I.; et al. Orally Administered Probiotics Decrease Aggregatibacter Actinomycetemcomitans but Not Other Periodontal Pathogenic Bacteria Counts in the Oral Cavity: A Systematic Review and Meta-Analysis. Front. Pharm. 2021, 12, 682656. [Google Scholar] [CrossRef]
- Burton, J.P.; Wescombe, P.A.; Macklaim, J.M.; Chai, M.H.C.; MacDonald, K.; Hale, J.D.F.; Tagg, J.; Reid, G.; Gloor, G.B.; Cadieux, P.A. Persistence of the Oral Probiotic Streptococcus Salivarius M18 Is Dose Dependent and Megaplasmid Transfer Can Augment Their Bacteriocin Production and Adhesion Characteristics. PLoS ONE 2013, 8, e65991. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Santacroce, L.; Cantore, S.; Bottalico, L.; Dipalma, G.; Vito, D.D.; Saini, R.; Inchingolo, F. Probiotics Improve Urogenital Health in Women. Open Access Maced. J. Med. Sci. 2018, 6, 1845–1850. [Google Scholar] [CrossRef] [Green Version]
- Wescombe, P.A.; Heng, N.C.K.; Burton, J.P.; Chilcott, C.N.; Tagg, J.R. Streptococcal Bacteriocins and the Case for Streptococcus Salivarius as Model Oral Probiotics. Future Microbiol. 2009, 4, 819–835. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; Signorini, L.; Inchingolo, A.D.; Saini, R.; Gnoni, A.; Scacco, S.; Cantore, S.; Dipalma, G.; Inchingolo, F.; Santacroce, L. Probiotics May Improve Serum Folate Availability in Pregnant Women: A Pilot Study. Open Access Maced. J. Med. Sci. 2020, 8, 1124–1130. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; De Vito, D.; Abbinante, A.; Altini, V.; Dipalma, G.; Inchingolo, F.; Saini, R. Clinical Results of Improvement in Periodontal Condition by Administration of Oral Probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1329–1334. [Google Scholar]
- Ballini, A.; Dipalma, G.; Isacco, C.G.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; Nguyễn, K.C.D.; Scacco, S.; Calvani, M.; Boddi, A.; et al. Oral Microbiota and Immune System Crosstalk: A Translational Research. Biology 2020, 9, E131. [Google Scholar] [CrossRef]
- Nunpan, S.; Suwannachart, C.; Wayakanon, K. Effect of Prebiotics-Enhanced Probiotics on the Growth of Streptococcus Mutans. Int. J. Microbiol. 2019, 2019, 4623807. [Google Scholar] [CrossRef] [Green Version]
- Burton, J.P.; Wescombe, P.A.; Moore, C.J.; Chilcott, C.N.; Tagg, J.R. Safety Assessment of the Oral Cavity Probiotic Streptococcus Salivarius K12. Appl. Environ. Microbiol. 2006, 72, 3050–3053. [Google Scholar] [CrossRef] [Green Version]
- Dobson, A.; Crispie, F.; Rea, M.C.; O’Sullivan, O.; Casey, P.G.; Lawlor, P.G.; Cotter, P.D.; Ross, P.; Gardiner, G.E.; Hill, C. Fate and Efficacy of Lacticin 3147-Producing Lactococcus Lactis in the Mammalian Gastrointestinal Tract: Lacticin-Producing L. Lactis in the Gastrointestinal Tract. FEMS Microbiol. Ecol. 2011, 76, 602–614. [Google Scholar] [CrossRef] [Green Version]
- Heng, N.C.K.; Haji-Ishak, N.S.; Kalyan, A.; Wong, A.Y.C.; Lovrić, M.; Bridson, J.M.; Artamonova, J.; Stanton, J.-A.L.; Wescombe, P.A.; Burton, J.P.; et al. Genome Sequence of the Bacteriocin-Producing Oral Probiotic Streptococcus Salivarius Strain M18. J. Bacteriol. 2011, 193, 6402–6403. [Google Scholar] [CrossRef] [Green Version]
- Inchingolo, F.; Dipalma, G.; Cirulli, N.; Cantore, S.; Saini, R.S.; Altini, V.; Santacroce, L.; Ballini, A.; Saini, R. Microbiological results of improvement in periodontal condition by administration of oral probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1323–1328. [Google Scholar]
- Dierksen, K.P.; Moore, C.J.; Inglis, M.; Wescombe, P.A.; Tagg, J.R. The Effect of Ingestion of Milk Supplemented with Salivaricin A-Producing Streptococcus Salivarius on the Bacteriocin-like Inhibitory Activity of Streptococcal Populations on the Tongue. FEMS Microbiol. Ecol. 2007, 59, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Santacroce, L.; Charitos, I.A.; Ballini, A.; Inchingolo, F.; Luperto, P.; De Nitto, E.; Topi, S. The Human Respiratory System and Its Microbiome at a Glimpse. Biology 2020, 9, E318. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 10, n71. [Google Scholar] [CrossRef]
- Ali, A.; Ismail, H.; Amin, K. Effect of Nanosilver Mouthwash on Prevention of White Spot Lesions in Patients Undergoing Fixed Orthodontic Treatment—A Randomized Double-Blind Clinical Trial. J. Dent. Sci. 2022, 17, 249–255. [Google Scholar] [CrossRef]
- Beerens, M.W.; ten Cate, J.M.; van der Veen, M.H. Microbial Profile of Dental Plaque Associated to White Spot Lesions in Orthodontic Patients Immediately after the Bracket Removal. Arch. Oral Biol. 2017, 78, 88–93. [Google Scholar] [CrossRef]
- Reichardt, E.; Geraci, J.; Sachse, S.; Rödel, J.; Pfister, W.; Löffler, B.; Wagner, Y.; Eigenthaler, M.; Wolf, M. Qualitative and Quantitative Changes in the Oral Bacterial Flora Occur Shortly after Implementation of Fixed Orthodontic Appliances. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 735–744. [Google Scholar] [CrossRef]
- Ko-Adams, C.; Cioffi, I.; Dufour, D.; Nainar, S.M.H.; Lévesque, C.M.; Gong, S.-G. Short-Term Effects of Fixed Orthodontic Appliance on Concentrations of Mutans Streptococci and Persister Cells in Adolescents. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 385–391. [Google Scholar] [CrossRef]
- Gujar, A.N.; Al-Hazmi, A.; Raj, A.T.; Patil, S. Microbial Profile in Different Orthodontic Appliances by Checkerboard DNA-DNA Hybridization: An in-Vivo Study. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 49–58. [Google Scholar] [CrossRef]
- Salehi, B.; Kregiel, D.; Mahady, G.; Sharifi-Rad, J.; Martins, N.; Rodrigues, C.F. Management of Streptococcus mutans-Candida spp. Oral Biofilms’ Infections: Paving the Way for Effective Clinical Interventions. J. Clin. Med. 2020, 9, 517. [Google Scholar] [CrossRef] [Green Version]
- Rosier, B.T.; Palazón, C.; García-Esteban, S.; Artacho, A.; Galiana, A.; Mira, A. A Single Dose of Nitrate Increases Resilience Against Acidification Derived From Sugar Fermentation by the Oral Microbiome. Front. Cell. Infect. Microbiol. 2021, 11, 692883. [Google Scholar] [CrossRef]
- Kim, Y.-R.; Nam, S.-H. A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of a Mouthwash Containing Glycyrrhiza Uralensis Extract for Preventing Dental Caries. Int. J. Environ. Res. Public Health 2021, 19, 242. [Google Scholar] [CrossRef] [PubMed]
- Padala, R.G.; Peddu, R.; Nuvusetty, B.; Mallavarapu, K.; Banswada, S.R.; Mood, T.N. Effect of Fluoride-Releasing Elastomers on Mutans Streptococci in Dental Plaque: An In Vivo Study. J. Contemp. Dent. Pract. 2019, 20, 1061–1066. [Google Scholar] [PubMed]
- Nascimento, M.M.; Alvarez, A.J.; Huang, X.; Browngardt, C.; Jenkins, R.; Sinhoreti, M.C.; Ribeiro, A.P.D.; Dilbone, D.A.; Richards, V.P.; Garrett, T.J.; et al. Metabolic Profile of Supragingival Plaque Exposed to Arginine and Fluoride. J. Dent. Res. 2019, 98, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; He, J.; Wang, L.; Zhou, S.; Peng, X.; Huang, S.; Zheng, L.; Cheng, L.; Hao, Y.; Li, J.; et al. Ecological Effect of Arginine on Oral Microbiota. Sci. Rep. 2017, 7, 7206. [Google Scholar] [CrossRef] [Green Version]
- Koruyucu, M.; BiRant, S.; Topçuoğlu, N.; Kulekci, G.; Seymen, F. Investigation of The Clinical and Microbiological Effects of Different Toothpastes: In-Vivo Study. Cumhur. Dent. J. 2020, 23, 21–30. [Google Scholar] [CrossRef]
- Villinski, J.R.; Bergeron, C.; Cannistra, J.C.; Gloer, J.B.; Coleman, C.M.; Ferreira, D.; Azelmat, J.; Grenier, D.; Gafner, S. Pyrano-Isoflavans from Glycyrrhiza Uralensis with Antibacterial Activity against Streptococcus Mutans and Porphyromonas Gingivalis. J. Nat. Prod. 2014, 77, 521–526. [Google Scholar] [CrossRef]
- Nascimento, M.M.; Alvarez, A.J.; Huang, X.; Hanway, S.; Perry, S.; Luce, A.; Richards, V.P.; Burne, R.A. Arginine Metabolism in Supragingival Oral Biofilms as a Potential Predictor of Caries Risk. JDR Clin. Transl. Res. 2019, 4, 262–270. [Google Scholar] [CrossRef]
- Kuribayashi, M.; Kitasako, Y.; Matin, K.; Sadr, A.; Shida, K.; Tagami, J. Intraoral PH Measurement of Carious Lesions with QPCR of Cariogenic Bacteria to Differentiate Caries Activity. J. Dent. 2012, 40, 222–228. [Google Scholar] [CrossRef]
- Geiger, A.M.; Gorelick, L.; Gwinnett, A.J.; Benson, B.J. Reducing White Spot Lesions in Orthodontic Populations with Fluoride Rinsing. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 403–407. [Google Scholar] [CrossRef]
- Roveri, N.; Battistella, E.; Bianchi, C.L.; Foltran, I.; Foresti, E.; Iafisco, M.; Lelli, M.; Naldoni, A.; Palazzo, B.; Rimondini, L. Surface Enamel Remineralization: Biomimetic Apatite Nanocrystals and Fluoride Ions Different Effects. J. Nanomater. 2009, 2009, 746383. [Google Scholar] [CrossRef] [Green Version]
- Orsini, G.; Procaccini, M.; Manzoli, L.; Giuliodori, F.; Lorenzini, A.; Putignano, A. A Double-Blind Randomized-Controlled Trial Comparing the Desensitizing Efficacy of a New Dentifrice Containing Carbonate/Hydroxyapatite Nanocrystals and a Sodium Fluoride/Potassium Nitrate Dentifrice: A New Dentifrice Desensitizing Efficacy. J. Clin. Periodontol. 2010, 37, 510–517. [Google Scholar] [CrossRef]
- Orsini, G.; Procaccini, M.; Manzoli, L.; Sparabombe, S.; Tiriduzzi, P.; Bambini, F.; Putignano, A. A 3-Day Randomized Clinical Trial to Investigate the Desensitizing Properties of Three Dentifrices. J. Periodontol. 2013, 84, e65–e73. [Google Scholar] [CrossRef]
- Rimondini, L.; Palazzo, B.; Iafisco, M.; Canegallo, L.; Demarosi, F.; Merlo, M.; Roveri, N. The Remineralizing Effect of Carbonate-Hydroxyapatite Nanocrystals on Dentine. Mater. Sci. Forum Mater Sci. Forum 2007, 539, 602–605. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Gallo, S.; Lelli, M.; Tarterini, F.; Giglia, F.; Scribante, A. SEM/EDS Evaluation of the Mineral Deposition on a Polymeric Composite Resin of a Toothpaste Containing Biomimetic Zn-Carbonate Hydroxyapatite (MicroRepair®) in Oral Environment: A Randomized Clinical Trial. Polymers 2021, 13, 2740. [Google Scholar] [CrossRef]
- Zubadalashvili, N.G.; Makhviladze, M.A.; Diasamidze, M.T.; Abdulashvili, N.N. The Comparative Study of Linex and Lacto-G in Treatment of Adult Patients with Disbacteriosis. Georgian Med. News 2009, 170, 38–42. [Google Scholar]
- Tamboli, C.P.; Neut, C.; Desreumaux, P.; Colombel, J.F. Dysbiosis in Inflammatory Bowel Disease. Gut 2004, 53, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Hawrelak, J.A.; Myers, S.P. The Causes of Intestinal Dysbiosis: A Review. Altern. Med. Rev. 2004, 9, 180–197. [Google Scholar]
- Torrazza, R.M.; Ukhanova, M.; Wang, X.; Sharma, R.; Hudak, M.L.; Neu, J.; Mai, V. Intestinal Microbial Ecology and Environmental Factors Affecting Necrotizing Enterocolitis. PLoS ONE 2013, 8, e83304. [Google Scholar] [CrossRef] [Green Version]
- De Vrese, M.; Marteau, P.R. Probiotics and Prebiotics: Effects on Diarrhea. J. Nutr. 2007, 137, 803S–811S. [Google Scholar] [CrossRef] [Green Version]
- Koning, C.J.M.; Jonkers, D.M.A.E.; Stobberingh, E.E.; Mulder, L.; Rombouts, F.M.; Stockbrügger, R.W. The Effect of a Multispecies Probiotic on the Intestinal Microbiota and Bowel Movements in Healthy Volunteers Taking the Antibiotic Amoxycillin. Am. J. Gastroenterol. 2008, 103, 178–189. [Google Scholar] [CrossRef]
- Gill, H.; Prasad, J. Probiotics, Immunomodulation, and Health Benefits. Adv. Exp. Med. Biol. 2008, 606, 423–454. [Google Scholar] [CrossRef]
- Vangay, P.; Ward, T.; Gerber, J.S.; Knights, D. Antibiotics, Pediatric Dysbiosis, and Disease. Cell Host Microbe 2015, 17, 553–564. [Google Scholar] [CrossRef] [Green Version]
- The Oral Microflora. M.R.Milward School of Dentistry—PDF Free Download. Available online: https://docplayer.net/23903060-The-oral-microflora-m-r-milward-school-of-dentistry.html (accessed on 19 May 2022).
- Norris, V.; Chen, M.; Goldberg, M.; Voskuil, J.; McGurk, G.; Holland, I.B. Calcium in Bacteria: A Solution to Which Problem? Mol. Microbiol. 1991, 5, 775–778. [Google Scholar] [CrossRef]
- Rose, R.K. The Role of Calcium in Oral Streptococcal Aggregation and the Implications for Biofilm Formation and Retention. Biochim. Biophys. Acta 2000, 1475, 76–82. [Google Scholar] [CrossRef]
- Dominguez, D.C. Calcium Signalling in Bacteria. Mol. Microbiol. 2004, 54, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Rose, R.K.; Dibdin, G.H.; Shellis, R.P. A Quantitative Study of Calcium Binding and Aggregation in Selected Oral Bacteria. J. Dent. Res. 1993, 72, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Correia, M.F.; Tenuta, L.M.A.; Del Bel Cury, A.A.; Cury, J.A. Mineral Ions in the Fluid of Biofilms Formed on Enamel and Dentine Shortly after Sugar Challenge. Caries Res. 2012, 46, 408–412. [Google Scholar] [CrossRef]
- Chemical Interactions between the Tooth and Oral Fluids—Research—Aarhus University. Available online: https://pure.au.dk/portal/en/publications/chemical-interactions-between-the-tooth-and-oral-fluids(56fed3c0-b5c4-11db-bee9-02004c4f4f50).html (accessed on 19 May 2022).
- Domon-Tawaraya, H.; Nakajo, K.; Washio, J.; Ashizawa, T.; Ichino, T.; Sugawara, H.; Fukumoto, S.; Takahashi, N. Divalent Cations Enhance Fluoride Binding to Streptococcus Mutans and Streptococcus Sanguinis Cells and Subsequently Inhibit Bacterial Acid Production. Caries Res. 2013, 47, 141–149. [Google Scholar] [CrossRef]
- Shishniashvili, T.; Suladze, T.; Makhviladze, M.; Kalandaze, M.; Margvelashvili, V. Dental Diseases and Intestinal Dysbiosis Among Children. J. Clin. Pediatric Dent. 2018, 42, 217–220. [Google Scholar] [CrossRef]
- Hernández, M.; Planells, P.; Martínez, E.; Mira, A.; Carda-Diéguez, M. Microbiology of Molar–Incisor Hypomineralization Lesions. A Pilot Study. J. Oral Microbiol. 2020, 12, 1766166. [Google Scholar] [CrossRef]
- Leitão, T.J.; Cury, J.A.; Tenuta, L.M.A. Kinetics of Calcium Binding to Dental Biofilm Bacteria. PLoS ONE 2018, 13, e0191284. [Google Scholar] [CrossRef] [Green Version]
- Senneby, A.; Davies, J.; Svensäter, G.; Neilands, J. Acid Tolerance Properties of Dental Biofilms in Vivo. BMC Microbiol. 2017, 17, 165. [Google Scholar] [CrossRef]
- Zhou, J.; Jiang, N.; Wang, Z.; Li, L.; Zhang, J.; Ma, R.; Nie, H.; Li, Z. Influences of PH and Iron Concentration on the Salivary Microbiome in Individual Humans with and without Caries. Appl. Environ. Microbiol. 2017, 83, e02412-16. [Google Scholar] [CrossRef] [Green Version]
- Valenti, C.; Pagano, S.; Bozza, S.; Ciurnella, E.; Lomurno, G.; Capobianco, B.; Coniglio, M.; Cianetti, S.; Marinucci, L. Use of the Er:YAG Laser in Conservative Dentistry: Evaluation of the Microbial Population in Carious Lesions. Materials 2021, 14, 2387. [Google Scholar] [CrossRef]
- Jia, G.; Zhi, A.; Lai, P.F.H.; Wang, G.; Xia, Y.; Xiong, Z.; Zhang, H.; Che, N.; Ai, L. The Oral Microbiota–Ia Mechanistic Role for Systemic Diseases. Br. Dent. J. 2018, 224, 447–455. [Google Scholar] [CrossRef]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The Oral Microbiota: Dynamic Communities and Host Interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, X.; Li, H.; Ni, C.; Du, Z.; Yan, F. Human Oral Microbiota and Its Modulation for Oral Health. Biomed. Pharm. 2018, 99, 883–893. [Google Scholar] [CrossRef]
- Mira, A.; Simon-Soro, A.; Curtis, M.A. Role of Microbial Communities in the Pathogenesis of Periodontal Diseases and Caries. J. Clin. Periodontol. 2017, 44, S23–S38. [Google Scholar] [CrossRef] [Green Version]
- Lygidakis, N.A.; Dimou, G.; Briseniou, E. Molar-Incisor-Hypomineralisation (MIH). Retrospective Clinical Study in Greek Children. I. Prevalence and Defect Characteristics. Eur. Arch Paediatr. Dent. 2008, 9, 200–206. [Google Scholar] [CrossRef]
- Elcock, C.; Smith, R.N.; Simpson, J.; Abdellatif, A.; Bäckman, B.; Brook, A.H. Comparison of Methods for Measurement of Hypoplastic Lesions. Eur. J. Oral Sci. 2006, 114, 365–369. [Google Scholar] [CrossRef]
- Weerheijm, K.L.; Groen, H.J.; Beentjes, V.E.; Poorterman, J.H. Prevalence of Cheese Molars in Eleven-Year-Old Dutch Children. ASDC J. Dent. Child. 2001, 68, 229, 256–262. [Google Scholar]
- Weerheijm, K.L.; Duggal, M.; Mejàre, I.; Papagiannoulis, L.; Koch, G.; Martens, L.C.; Hallonsten, A.-L. Judgement Criteria for Molar Incisor Hypomineralisation (MIH) in Epidemiologic Studies: A Summary of the European Meeting on MIH Held in Athens, 2003. Eur. J. Paediatr. Dent. 2003, 4, 110–113. [Google Scholar]
- Mathu-Muju, K.; Wright, J.T. Diagnosis and Treatment of Molar Incisor Hypomineralization. Compend. Contin. Educ. Dent. 2006, 27, 604–610. [Google Scholar]
- Hernández, M.; Boj, J.-R.; Espasa, E.; Peretz, B. First Permanent Molars and Permanent Incisors Teeth by Tooth Prevalence of Molar–Incisor–Hypomineralisation in a Group of Spanish Schoolchildren. Acta Stomatol. Croat. 2018, 52, 4–11. [Google Scholar] [CrossRef]
- Weerheijm, K.L.; Jälevik, B.; Alaluusua, S. Molar-Incisor Hypomineralisation. Caries. Res. 2001, 35, 390–391. [Google Scholar] [CrossRef]
- Elhennawy, K.; Schwendicke, F. Managing Molar-Incisor Hypomineralization: A Systematic Review. J. Dent. 2016, 55, 16–24. [Google Scholar] [CrossRef]
- Silva, M.J.; Scurrah, K.J.; Craig, J.M.; Manton, D.J.; Kilpatrick, N. Etiology of Molar Incisor Hypomineralization—A Systematic Review. Community Dent. Oral Epidemiol. 2016, 44, 342–353. [Google Scholar] [CrossRef]
- Crombie, F.; Manton, D.; Kilpatrick, N. Aetiology of Molar-Incisor Hypomineralization: A Critical Review. Int. J. Paediatr. Dent. 2009, 19, 73–83. [Google Scholar] [CrossRef]
- Elhennawy, K.; Manton, D.J.; Crombie, F.; Zaslansky, P.; Radlanski, R.J.; Jost-Brinkmann, P.-G.; Schwendicke, F. Structural, Mechanical and Chemical Evaluation of Molar-Incisor Hypomineralization-Affected Enamel: A Systematic Review. Arch. Oral Biol. 2017, 83, 272–281. [Google Scholar] [CrossRef]
- Simón-Soro, A.; Belda-Ferre, P.; Cabrera-Rubio, R.; Alcaraz, L.D.; Mira, A. A Tissue-Dependent Hypothesis of Dental Caries. Caries Res. 2013, 47, 591–600. [Google Scholar] [CrossRef]
- Subgingival Microbiota in Health Compared to Periodontitis and the Influence of Smoking—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4356944/ (accessed on 19 May 2022).
- Chan, Y.; Chien, R. Identification and Analyses of Periodontal Pathogens in Taiwan by Microbiological Tests. Chin. J. Microbiol. Immunol. 1994, 27, 59–69. [Google Scholar]
- Siqueira, J.F.; Rôças, I.N. Catonella Morbi and Granulicatella Adiacens: New Species in Endodontic Infections. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Chu, M.; Huang, Z.; Yang, X.; Ran, S.; Hu, B.; Zhang, C.; Liang, J. Variations in Oral Microbiota Associated with Oral Cancer. Sci. Rep. 2017, 7, 11773. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Tsuruda, K.; Iwamoto, Y.; Kato, F.; Odaki, T.; Yamane, N.; Hori, Y.; Harashima, Y.; Sakoda, A.; Tagaya, A.; et al. Significant Increase of Oral Bacteria in the Early Pregnancy Period in Japanese Women. J. Investig. Clin. Dent. 2017, 8, e12189. [Google Scholar] [CrossRef]
- Borgo, P.V.; Rodrigues, V.A.A.; Feitosa, A.C.R.; Xavier, K.C.B.; Avila-Campos, M.J. Association between Periodontal Condition and Subgingival Microbiota in Women during Pregnancy: A Longitudinal Study. J. Appl. Oral Sci. 2014, 22, 528–533. [Google Scholar] [CrossRef]
- Kumar, P.S. Sex and the Subgingival Microbiome: Do Female Sex Steroids Affect Periodontal Bacteria? Periodontol 2000 2013, 61, 103–124. [Google Scholar] [CrossRef]
- Tinanoff, N.; Baez, R.J.; Diaz Guillory, C.; Donly, K.J.; Feldens, C.A.; McGrath, C.; Phantumvanit, P.; Pitts, N.B.; Seow, W.K.; Sharkov, N.; et al. Early Childhood Caries Epidemiology, Aetiology, Risk Assessment, Societal Burden, Management, Education, and Policy: Global Perspective. Int. J. Paediatr. Dent. 2019, 29, 238–248. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Barbieri, S.; Bruni, A.; Sinesi, A.; Ricci, M.; Trombini, J.; et al. Assessment of Genetical, Pre, Peri and Post Natal Risk Factors of Deciduous Molar Hypomineralization (DMH), Hypomineralized Second Primary Molar (HSPM) and Molar Incisor Hypomineralization (MIH): A Narrative Review. Children 2021, 8, 432. [Google Scholar] [CrossRef]
- Lif Holgerson, P.; Harnevik, L.; Hernell, O.; Tanner, A.C.R.; Johansson, I. Mode of Birth Delivery Affects Oral Microbiota in Infants. J. Dent. Res. 2011, 90, 1183–1188. [Google Scholar] [CrossRef] [Green Version]
- Paster, B.J.; Dewhirst, F.E. Molecular Microbial Diagnosis. Periodontology 2009, 51, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Penders, J.; Thijs, C.; Vink, C.; Stelma, F.F.; Snijders, B.; Kummeling, I.; van den Brandt, P.A.; Stobberingh, E.E. Factors Influencing the Composition of the Intestinal Microbiota in Early Infancy. Pediatrics 2006, 118, 511–521. [Google Scholar] [CrossRef] [Green Version]
- Dominguez-Bello, M.G.; Costello, E.K.; Contreras, M.; Magris, M.; Hidalgo, G.; Fierer, N.; Knight, R. Delivery Mode Shapes the Acquisition and Structure of the Initial Microbiota across Multiple Body Habitats in Newborns. Proc. Natl. Acad. Sci. USA 2010, 107, 11971–11975. [Google Scholar] [CrossRef] [Green Version]
- Marsh, P.D. Microbial Ecology of Dental Plaque and Its Significance in Health and Disease. Adv. Dent. Res. 1994, 8, 263–271. [Google Scholar] [CrossRef]
- Jenkinson, H.F. Beyond the Oral Microbiome. Environ. Microbiol. 2011, 13, 3077–3087. [Google Scholar] [CrossRef]
- Carlsson, J. Bacterial Metabolism in Dental Biofilms. 1997. Available online: https://journals.sagepub.com/doi/abs/10.1177/08959374970110012001 (accessed on 19 May 2022).
- Bowden, G.H.W. Which Bacteria Are Cariogenic in Humans. In Dental Caries Vol. 1: Markers of High and Low Risk Groups and Individuals; Johnson, N.M., Ed.; Cambridge University Press: Cambridge, UK, 1991; pp. 266–286. [Google Scholar]
- Stephan, R.M. Intra-Oral Hydrogen-Ion Concentrations Associated With Dental Caries Activity. J. Dent. Res. 1944, 23, 257–266. [Google Scholar] [CrossRef]
- Marsh, P.D. Are Dental Diseases Examples of Ecological Catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef]
- Hamilton, I.R.; Buckley, N.D. Adaptation by Streptococcus Mutans to Acid Tolerance. Oral Microbiol. Immunol. 1991, 6, 65–71. [Google Scholar] [CrossRef]
- Svensäter, G.; Larsson, U.B.; Greif, E.C.; Cvitkovitch, D.G.; Hamilton, I.R. Acid Tolerance Response and Survival by Oral Bacteria. Oral Microbiol. Immunol. 1997, 12, 266–273. [Google Scholar] [CrossRef]
- Foster, J.W.; Hall, H.K. Adaptive Acidification Tolerance Response of Salmonella Typhimurium. J. Bacteriol. 1990, 172, 771–778. [Google Scholar] [CrossRef] [Green Version]
- Foster, J.W.; Moreno, M. Inducible Acid Tolerance Mechanisms in Enteric Bacteria. Novartis Found. Symp. 1999, 221, 55–69; discussion 70–74. [Google Scholar] [CrossRef]
- Gahan, C.G.; O’Driscoll, B.; Hill, C. Acid Adaptation of Listeria Monocytogenes Can Enhance Survival in Acidic Foods and during Milk Fermentation. Appl. Environ. Microbiol. 1996, 62, 3128–3132. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, N.; Xiao, J.-Z.; Miyaji, K.; Yaeshiima, T.; Hiramatsu, A.; Iwatsuki, K.; Kokubo, S.; Hosono, A. Selection of Acid Tolerant Bifidobacteria and Evidence for a Low-PH-Inducible Acid Tolerance Response in Bifidobacterium Longum. J. Dairy Res. 2004, 71, 340–345. [Google Scholar] [CrossRef]
- Belli, W.A.; Marquis, R.E. Adaptation of Streptococcus Mutans and Enterococcus Hirae to Acid Stress in Continuous Culture. Appl. Environ. Microbiol. 1991, 57, 1134–1138. [Google Scholar] [CrossRef] [Green Version]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [CrossRef] [Green Version]
- Moynihan, P.J.; Kelly, S.A.M. Effect on Caries of Restricting Sugars Intake: Systematic Review to Inform WHO Guidelines. J. Dent. Res. 2014, 93, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Hemadi, A.S.; Huang, R.; Zhou, Y.; Zou, J. Salivary Proteins and Microbiota as Biomarkers for Early Childhood Caries Risk Assessment. Int. J. Oral Sci. 2017, 9, e1. [Google Scholar] [CrossRef] [Green Version]
- Conrads, G.; de Soet, J.J.; Song, L.; Henne, K.; Sztajer, H.; Wagner-Döbler, I.; Zeng, A.-P. Comparing the Cariogenic Species Streptococcus Sobrinus and S. mutans on Whole Genome Level. J. Oral. Microbiol. 2014, 6, 26189. [Google Scholar] [CrossRef] [Green Version]
- Velazquez-Enriquez, U.; Scougall-Vilchis, R.J.; Contreras-Bulnes, R.; Flores-Estrada, J.; Uematsu, S.; Yamaguchi, R. Quantitative Analysis of S. mutans and S. Sobrinus Cultivated Independently and Adhered to Polished Orthodontic Composite Resins. J. Appl. Oral Sci. 2012, 20, 544–549. [Google Scholar] [CrossRef]
- Tanner, A.C.R.; Kressirer, C.A.; Rothmiller, S.; Johansson, I.; Chalmers, N.I. The Caries Microbiome: Implications for Reversing Dysbiosis. Adv. Dent. Res. 2018, 29, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Tanzer, J.M.; Livingston, J.; Thompson, A.M. The Microbiology of Primary Dental Caries in Humans. J. Dent. Educ. 2001, 65, 1028–1037. [Google Scholar] [CrossRef]
- Bacterial Biofilms: From the Natural Environment to Infectious Diseases Nature Reviews Microbiology. Available online: https://www.nature.com/articles/nrmicro821 (accessed on 19 May 2022).
- Bowen, W.H.; Burne, R.A.; Wu, H.; Koo, H. Oral Biofilms: Pathogens, Matrix, and Polymicrobial Interactions in Microenvironments. Trends Microbiol. 2018, 26, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.; Coelho, A.; Lima, R.; Amaro, I.; Paula, A.; Marto, C.M.; Sousa, J.; Spagnuolo, G.; Marques Ferreira, M.; Carrilho, E. Efficacy and Patient’s Acceptance of Alternative Methods for Caries Removal-a Systematic Review. J. Clin. Med. 2020, 9, E3407. [Google Scholar] [CrossRef] [PubMed]
- Montedori, A.; Abraha, I.; Orso, M.; D’Errico, P.G.; Pagano, S.; Lombardo, G. Lasers for Caries Removal in Deciduous and Permanent Teeth. Cochrane Database Syst. Rev. 2016, 9, CD010229. [Google Scholar] [CrossRef] [PubMed]
- Pagano, S.; Lombardo, G.; Orso, M.; Abraha, I.; Capobianco, B.; Cianetti, S. Lasers to Prevent Dental Caries: A Systematic Review. BMJ Open 2020, 10, e038638. [Google Scholar] [CrossRef]
- Santos, G.M.; Pacheco, R.L.; Bussadori, S.K.; Santos, E.M.; Riera, R.; de Oliveira Cruz Latorraca, C.; Mota, P.; Benavent Caldas Bellotto, E.F.; Martimbianco, A.L.C. Effectiveness and Safety of Ozone Therapy in Dental Caries Treatment: Systematic Review and Meta-Analysis. J. Evid.-Based Dent. Pract. 2020, 20, 101472. [Google Scholar] [CrossRef]
- Bowen, W.H. Dental Caries—Not Just Holes in Teeth! A Perspective. Mol. Oral Microbiol. 2016, 31, 228–233. [Google Scholar] [CrossRef]
- Kallis, A.; Tolidis, K.; Gerasimou, P.; Dionysopoulos, D. Qualitative Evaluation of Hybrid Layer Formation Using Er:YAG Laser in QSP Mode for Tooth Cavity Preparations. Lasers Med. Sci. 2019, 34, 23–34. [Google Scholar] [CrossRef]
- Abbasi, M.; Nakhostin, A.; Namdar, F.; Chiniforush, N.; Hasani Tabatabaei, M. The Rate of Demineralization in the Teeth Prepared by Bur and Er:YAG Laser. J. Lasers Med. Sci. 2018, 9, 82–86. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, M.C.; Llama-Palacios, A.; Blanc, V.; León, R.; Herrera, D.; Sanz, M. Structure, Viability and Bacterial Kinetics of an in Vitro Biofilm Model Using Six Bacteria from the Subgingival Microbiota. J. Periodontal. Res. 2011, 46, 252–260. [Google Scholar] [CrossRef]
- Wang, X.; Willing, M.C.; Marazita, M.L.; Wendell, S.; Warren, J.J.; Broffitt, B.; Smith, B.; Busch, T.; Lidral, A.C.; Levy, S.M. Genetic and Environmental Factors Associated with Dental Caries in Children: The Iowa Fluoride Study. Caries Res. 2012, 46, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Jalasvuori, H.; Haukioja, A.; Tenovuo, J. Probiotic Lactobacillus Reuteri Strains ATCC PTA 5289 and ATCC 55730 Differ in Their Cariogenic Properties in Vitro. Arch. Oral Biol. 2012, 57, 1633–1638. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal Microbiome of Reproductive-Age Women. Proc. Natl. Acad. Sci. USA 2011, 108, 4680–4687. [Google Scholar] [CrossRef] [Green Version]
- Alves, K.M.R.P.; Franco, K.S.; Sassaki, K.T.; Buzalaf, M.A.R.; Delbem, A.C.B. Effect of Iron on Enamel Demineralization and Remineralization in Vitro. Arch. Oral Biol. 2011, 56, 1192–1198. [Google Scholar] [CrossRef]
- Wang, R.; Kaplan, A.; Guo, L.; Shi, W.; Zhou, X.; Lux, R.; He, X. The Influence of Iron Availability on Human Salivary Microbial Community Composition. Microb. Ecol. 2012, 64, 152–161. [Google Scholar] [CrossRef] [Green Version]
- Duran-Pinedo, A.E.; Frias-Lopez, J. Beyond Microbial Community Composition: Functional Activities of the Oral Microbiome in Health and Disease. Microbes Infect. 2015, 17, 505–516. [Google Scholar] [CrossRef] [Green Version]
- Buzalaf, M.A.R.; de Moraes Italiani, F.; Kato, M.T.; Martinhon, C.C.R.; Magalhães, A.C. Effect of Iron on Inhibition of Acid Demineralisation of Bovine Dental Enamel in Vitro. Arch. Oral Biol. 2006, 51, 844–848. [Google Scholar] [CrossRef]
- Kato, M.T.; Sales-Peres, S.H.D.C.; Buzalaf, M.A.R. Effect of Iron on Acid Demineralisation of Bovine Enamel Blocks by a Soft Drink. Arch. Oral Biol. 2007, 52, 1109–1111. [Google Scholar] [CrossRef]
- Martinhon, C.C.R.; Italiani, F.D.M.; Padilha, P.D.M.; Bijella, M.F.T.B.; Delbem, A.C.B.; Buzalaf, M.A.R. Effect of Iron on Bovine Enamel and on the Composition of the Dental Biofilm Formed “in Situ”. Arch. Oral Biol. 2006, 51, 471–475. [Google Scholar] [CrossRef]
- Pecharki, G.D.; Cury, J.A.; Paes Leme, A.F.; Tabchoury, C.P.M.; Del Bel Cury, A.A.; Rosalen, P.L.; Bowen, W.H. Effect of Sucrose Containing Iron (II) on Dental Biofilm and Enamel Demineralization in Situ. Caries Res. 2005, 39, 123–129. [Google Scholar] [CrossRef]
- Sales-Peres, S.H.C.; Pessan, J.P.; Buzalaf, M.A.R. Effect of an Iron Mouthrinse on Enamel and Dentine Erosion Subjected or Not to Abrasion: An in Situ/Ex Vivo Study. Arch. Oral Biol. 2007, 52, 128–132. [Google Scholar] [CrossRef]
- Iron and Dental Caries—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/3165568/ (accessed on 19 May 2022).
- Kojima, Y.; Ohshima, T.; Seneviratne, C.J.; Maeda, N. Combining Prebiotics and Probiotics to Develop Novel Synbiotics That Suppress Oral Pathogens. J. Oral Biosci. 2016, 58, 27–32. [Google Scholar] [CrossRef]
- Probiotics: Health Benefits in the Mouth—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/20178208/ (accessed on 19 May 2022).
- A Preliminary Study of the Synbiotic Effects of Konjac Glucomannan Hydrolysates (GMH) and Lactobacilli on the Growth of the Oral Bacterium Streptococcus Mutans Emerald Insight. Available online: https://www.emerald.com/insight/content/doi/10.1108/00346651111151357/full/html (accessed on 19 May 2022).
- Gibson, G.R.; Probert, H.M.; Loo, J.V.; Rastall, R.A.; Roberfroid, M.B. Dietary Modulation of the Human Colonic Microbiota: Updating the Concept of Prebiotics. Nutr. Res. Rev. 2004, 17, 259–275. [Google Scholar] [CrossRef] [Green Version]
- Kilian, M.; Chapple, I.L.C.; Hannig, M.; Marsh, P.D.; Meuric, V.; Pedersen, A.M.L.; Tonetti, M.S.; Wade, W.G.; Zaura, E. The Oral Microbiome—an Update for Oral Healthcare Professionals. Br. Dent. J. 2016, 221, 657–666. [Google Scholar] [CrossRef]
- Nyvad, B.; Fejerskov, O. Scanning Electron Microscopy of Early Microbial Colonization of Human Enamel and Root Surfaces in Vivo. Scand. J. Dent. Res. 1987, 95, 287–296. [Google Scholar] [CrossRef]
- Bermudez-Brito, M.; Plaza-Díaz, J.; Muñoz-Quezada, S.; Gómez-Llorente, C.; Gil, A. Probiotic Mechanisms of Action. Ann. Nutr. Metab. 2012, 61, 160–174. [Google Scholar] [CrossRef]
- Pujia, A.M.; Costacurta, M.; Fortunato, L.; Merra, G.; Cascapera, S.; Calvani, M.; Gratteri, S. The Probiotics in Dentistry: A Narrative Review. Eur. Rev. Med. Pharm. Sci. 2017, 21, 1405–1412. [Google Scholar]
- Viral and Bacterial Interactions in the Upper Respiratory Tract—ubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/23326226/ (accessed on 19 May 2022).
- De Martino, M.; Ballotti, S. The Child with Recurrent Respiratory Infections: Normal or Not? Pediatr. Allergy Immunol. 2007, 18, 13–18. [Google Scholar] [CrossRef]
- Insights into the Interaction between Influenza Virus and Pneumococcus—PMC. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1539103/ (accessed on 19 May 2022).
- Vesa, S.; Kleemola, M.; Blomqvist, S.; Takala, A.; Kilpi, T.; Hovi, T. Epidemiology of Documented Viral Respiratory Infections and Acute Otitis Media in a Cohort of Children Followed from Two to Twenty-Four Months of Age. Pediatr. Infect. Dis. J. 2001, 20, 574–581. [Google Scholar] [CrossRef]
- Mummolo, S.; D’Ercole, S.; Marchetti, E.; Campanella, V.; Martinelli, D.; Marzo, G.; Tripodi, D. Oral Antiseptic and Periodontitis: A Clinical and Microbiological Study. Oral Health Dent. Manag. 2014, 13, 698–702. [Google Scholar]
- Nicholson, K.G.; McNally, T.; Silverman, M.; Simons, P.; Stockton, J.D.; Zambon, M.C. Rates of Hospitalisation for Influenza, Respiratory Syncytial Virus and Human Metapneumovirus among Infants and Young Children. Vaccine 2006, 24, 102–108. [Google Scholar] [CrossRef]
- Massin, M.M.; Montesanti, J.; Gérard, P.; Lepage, P. Spectrum and Frequency of Illness Presenting to a Pediatric Emergency Department. Acta Clin. Belg. 2006, 61, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Pietruszewska, W.; Barańska, M.; Wielgat, J. Place of Phytotherapy in the Treatment of Acute Infections of Upper Respiratory Tract and Upper Gastrointestinal Tract. Otolaryngol. Pol. 2018, 72, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Cabral, C.; Ingram, J.; Lucas, P.J.; Redmond, N.M.; Kai, J.; Hay, A.D.; Horwood, J. Influence of Clinical Communication on Parents’ Antibiotic Expectations for Children With Respiratory Tract Infections. Ann. Fam. Med. 2016, 14, 141–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Embryotoxicity Assays for Leached Components from Dental Restorative Materials Reproductive Biology and Endocrinology Full Text. Available online: https://rbej.biomedcentral.com/articles/10.1186/1477-7827-9-136 (accessed on 19 May 2022).
- Andrews, T.; Thompson, M.; Buckley, D.I.; Heneghan, C.; Deyo, R.; Redmond, N.; Lucas, P.J.; Blair, P.S.; Hay, A.D. Interventions to Influence Consulting and Antibiotic Use for Acute Respiratory Tract Infections in Children: A Systematic Review and Meta-Analysis. PLoS ONE 2012, 7, e30334. [Google Scholar] [CrossRef] [Green Version]
- Lange, K.; Buerger, M.; Stallmach, A.; Bruns, T. Effects of Antibiotics on Gut Microbiota. Dig. Dis. 2016, 34, 260–268. [Google Scholar] [CrossRef]
- Szajewska, H.; Konarska, Z.; Kołodziej, M. Probiotic Bacterial and Fungal Strains: Claims with Evidence. Dig. Dis. 2016, 34, 251–259. [Google Scholar] [CrossRef]
- Di Pierro, F.; Colombo, M.; Giuliani, M.G.; Danza, M.L.; Basile, I.; Bollani, T.; Conti, A.M.; Zanvit, A.; Rottoli, A.S. Effect of Administration of Streptococcus Salivarius K12 on the Occurrence of Streptococcal Pharyngo-Tonsillitis, Scarlet Fever and Acute Otitis Media in 3 Years Old Children. Eur. Rev. Med. Pharm. Sci. 2016, 20, 4601–4606. [Google Scholar]
- Fooks, L.J.; Gibson, G.R. Probiotics as Modulators of the Gut Flora. Br. J. Nutr. 2002, 88 (Suppl. S1), S39–S49. [Google Scholar] [CrossRef] [Green Version]
- Ozen, M.; Kocabas Sandal, G.; Dinleyici, E.C. Probiotics for the Prevention of Pediatric Upper Respiratory Tract Infections: A Systematic Review. Expert Opin. Biol. Ther. 2015, 15, 9–20. [Google Scholar] [CrossRef]
- Lactobacillus Reuteri DSM 17938 Shortens Acute Infectious Diarrhea in a Pediatric Outpatient Setting—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/25986615/ (accessed on 19 May 2022).
- Ojetti, V.; Petruzziello, C.; Migneco, A.; Gnarra, M.; Gasbarrini, A.; Franceschi, F. Effect of Lactobacillus Reuteri (DSM 17938) on Methane Production in Patients Affected by Functional Constipation: A Retrospective Study. Eur. Rev. Med. Pharm. Sci. 2017, 21, 1702–1708. [Google Scholar]
- Santagati, M.; Scillato, M.; Patanè, F.; Aiello, C.; Stefani, S. Bacteriocin-Producing Oral Streptococci and Inhibition of Respiratory Pathogens. FEMS Immunol. Med. Microbiol. 2012, 65, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Gabryszewski, S.J.; Bachar, O.; Dyer, K.D.; Percopo, C.M.; Killoran, K.E.; Domachowske, J.B.; Rosenberg, H.F. Lactobacillus-Mediated Priming of the Respiratory Mucosa Protects against Lethal Pneumovirus Infection. J. Immunol. 2011, 186, 1151–1161. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}



| Articles screening strategy | KEYWORDS: A: “microbio*”; B: “oral microbiota”; C: “demineralization”; Boolean Indicators: (“A” AND “C”) AND (“B” AND “C”). Timespan: from January 2017 up to April 2022. Electronic Databases: PubMed, Web of Science, Google Scholar, Scopus, Cochrane Library, EMBEDDED, Dentistry & Oral Sciences Source via EBSCO, APA PsycINFO, APA PsyArticles, DRUGS@FDA |
| Authors | Type of Study | Object | Study Design and Timeline | Results |
|---|---|---|---|---|
| Yu-Rin Kim et al. [85] | A Randomized, Double-Blind, Placebo-Controlled Clinical Trial | Dental plaque pH variations after Glycyrrhiza Uralensis mouthwash. | Total of 60 patients, (30 case group and 30 control group), treated with placebo mouthwash. Mouthwash administered one time a day/5 days. | Glycyrrhiza Uralensis mouthwash is useful to prevent dental caries. |
| Bob T. et al. [84] | Blinded crossover study | Effect of nitrate on reduction of oral pH by sugar fermentation | Total 12 subjects subjected to nitrate-rich supplement dissolved in mineral water and a nitrate-poor placebo dissolved in mineral water vs. placebo. | pH buffering effect of nitrate when sugars were fermented in vivo due to lactate usage by nitrate reducing bacteria, including Rothia and Neisseria. |
| Anie Apriani et al. [48] | Perspective study | Casein CPP-ACP and fluoride varnish effect on saliva pH and caries activity | 60 children patients, 30 patients were treated with casein CPP-ACP and 30 patients with fluoride varnish | No statistical differences were found between the two groups. |
| Rahul G. Padala et al. [86] | Perspective case-control study | to verify the impact of Fluoride-releasing elastic modules on Streptococcus Mutans in oral cavity | Fluoride-releasing elastic modules were placed on brackets 12-11-33 and fluoride-free elastic modules were positioned on brackets 21-22-43 in 30 orthodontic patients. During each appointment, they were analyzed and replaced. | It was reported a considerable reduction was demonstrated (p < 0.001) of S. mutans count on Fluoride-releasing modules compared to non-fluoridates ones. |
| M.M. Nascimento et al. [87] | Randomized double-blind clinical trial | to evaluate the trend of plaque metabolic profile using arginine and fluoride. | 83 patients’ plaque data were selected on tooth surfaces with and without caries. Taxonomic profiles and analyses on plaque metabolism, arginine catabolism, and acidogenicity were performed. | Biofilm pH homeostasis is improved due to Arginine metabolism. Fluoride improves resistance of enamel and dentine to acidic pH. |
| Xin Zheng et al. [88] | Clinical Trial | to evaluate Fluoride and Arginine toothpaste impact on oral microbiome. | 42 patients divided in 2 groups had to clean their teeth 2 times a day for 3 minutes with and without Fluoride and Arginine toothpaste in 1 month. | Fluoride and arginine work together to maintain an oral microbial balance and prevent dental cavities. |
| Mine Koruyuc al. [89] | Randomized Clinical Trial | Non-fluoride toothpastes were compared to fluoride toothpastes about clinical, antibacterial, and microbiological effects. | 80 patients, aged from 3 to 12 years old, were randomly assigned to four groups and evaluated for 1 month. 2 groups used fluoride toothpaste and 2 groups used non-fluoride toothpaste. These groups were analyzed with statistical analysis | Streptococci Mutans levels decreased statistically significantly (p 0.05) in the I, II and III groups during one month; but no considerable variations were found between two groups |
| Azheen Ali et al. [78] | Randomized double-blind clinical trial | to examine the effect of nano-silver CHX or fluoride mouthwashes on WSLs during orthodontic treatment. | 42 patients were separated into three groups (14 patients each) based on the mouthwash (nano-silver, CHX, or fluoride), with 3 months and 6 months of follow-up | WSLs in the nanosilver group is evidently less relevant than in the CHX and fluoride group. |
| Authors | Type of Study | Object | Study Design and Timeline | Results |
|---|---|---|---|---|
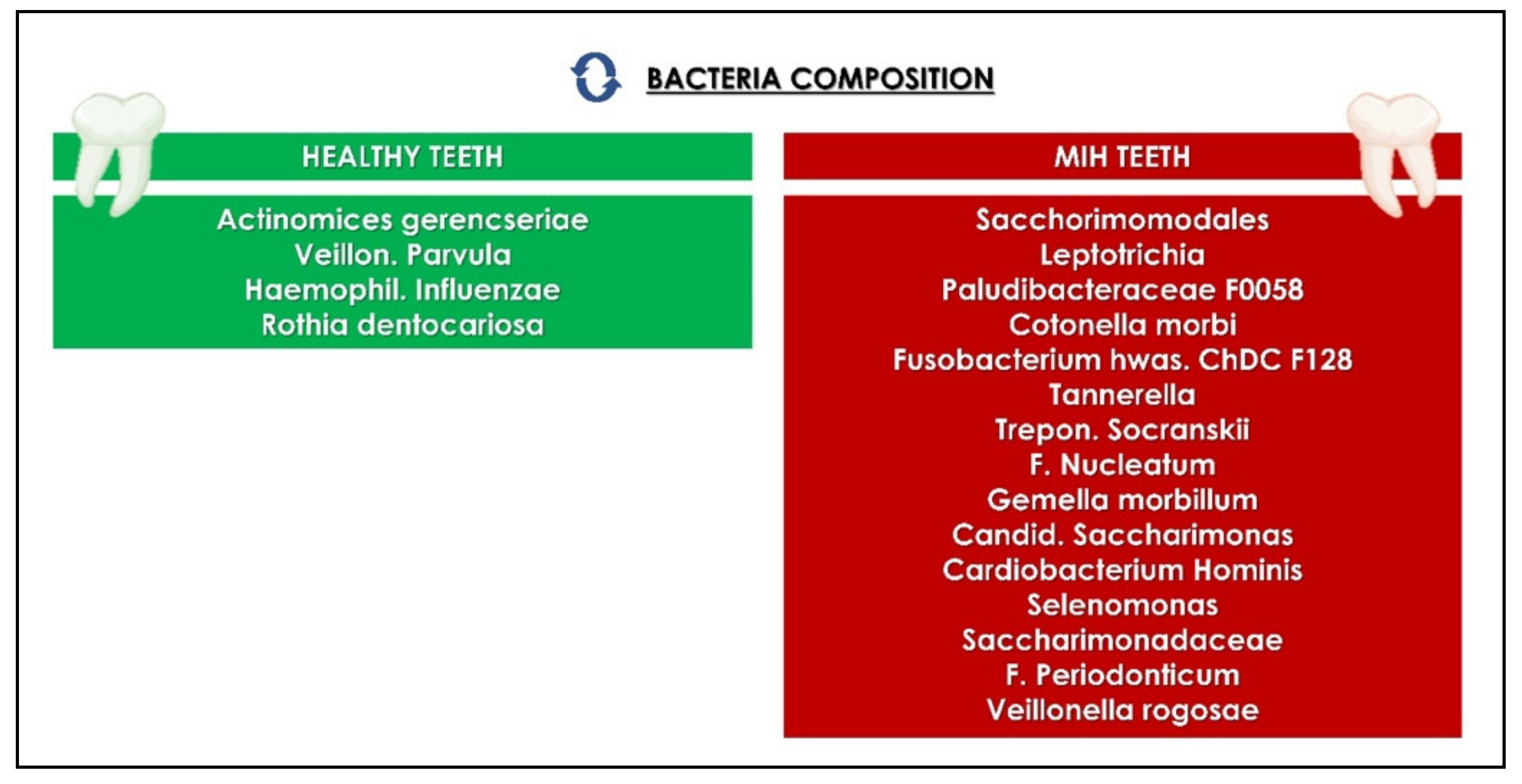
| Hernández et al., 2020 [116] | Randomized study | Association of the microbiome and dental molar–incisor hypomineralization | Patients with molar–incisor hypomineralization supragingival samples from healthy and MIH. Marker: 16S rRNA gene | The increased protein content of MIH teeth encourage proteolytic bacteria colonization, promote caries, raise the risk of other oral disorders. |
| Shishniashvili et al., 2018 [115] | Randomized study | The link between tooth enamel mineralization, oral mucosal diseases, and varying levels of GI imbalance. | Patients with caries, acute or chronic candidiasis and proven dysbiosis. | The degree of dental hard tissue demineralization is influenced by GI microbiota dysbiosis. |
| Leitão et al., 2018 [117] | Randomized study | The determination of calcium kinetics, binding, and release to/from Streptococcus mutans. | Calcium in S. mutans Ingbrit 1600 pellets treated with PIPES buffer, 1 or 10 mM Ca | The relevance of the calcium bacterial reservoir may decrease the power for tooth demineralization when released from the bacterial reservoirs |
| Senneby et al., 2017 [118] | In vivo study | Intra-individual variability in biofilm acid tolerance between different tooth surfaces and inter-individual variance and acid tolerance stability over time. | Plaque biofilm sampling by 40 adolescents | Biofilm acid tolerance showed short-term stability and low variance between multiple sites in the same individual. |
| Zhou et al., 2016 [119] | In vivo study | Variations of oral microbial communities by patients with and without caries | Saliva from patients with and without caries | The microbial community structure was influenced by salivary pH and iron content. |
| Valenti et al., 2021 [120] | Randomized study | Effects of the erbium:yttrio-aluminum-granate (Er:YAG) laser on dental diseases and on bacterial composition | Adults with active deep dental illnesses received CT and Er:YAG therapy. | Er:YAG laser demonstrated to be able to reduce microbial loads, aimed to pediatric and complicated patients |
| Authors | Type of Study | Object | Study Design and Timeline | Results |
|---|---|---|---|---|
| Nunpan et al. 2019 [70] | Randomized study | The prebiotic’s effect on Lactobacillus acidophilus’s inhibition on Streptococcus mutans (A32-2) and prevent dental caries. | S. mutans A32-2-S. mutans clinical strain obtained from highly active carious individuals | S. mutans’ growth rate was significantly inhibited when cocultured with L. acidophilus and the appropriate dose of prebiotics. |
| Campanella et al. 2018 [61] | Randomized double-blinded placebo-controlled pilot study | The therapeutic benefit of oral probiotics on acute oral and respiratory tract infections in pediatric patients | Total 40 subjects with recent oral and respiratory tract infections. The probiotics were compared to placebo. | Major advantages of probiotics in reducing infections in the oral and respiratory tracts without the use of any drugs. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. https://doi.org/10.3390/children9071014
Inchingolo AD, Malcangi G, Semjonova A, Inchingolo AM, Patano A, Coloccia G, Ceci S, Marinelli G, Di Pede C, Ciocia AM, et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children. 2022; 9(7):1014. https://doi.org/10.3390/children9071014
Chicago/Turabian StyleInchingolo, Alessio Danilo, Giuseppina Malcangi, Alexandra Semjonova, Angelo Michele Inchingolo, Assunta Patano, Giovanni Coloccia, Sabino Ceci, Grazia Marinelli, Chiara Di Pede, Anna Maria Ciocia, and et al. 2022. "Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature" Children 9, no. 7: 1014. https://doi.org/10.3390/children9071014