
Hospital Admission in the Latent versus the Active Phase of Labor: Comparison of Perinatal Outcomes

Abstract
:1. Introduction
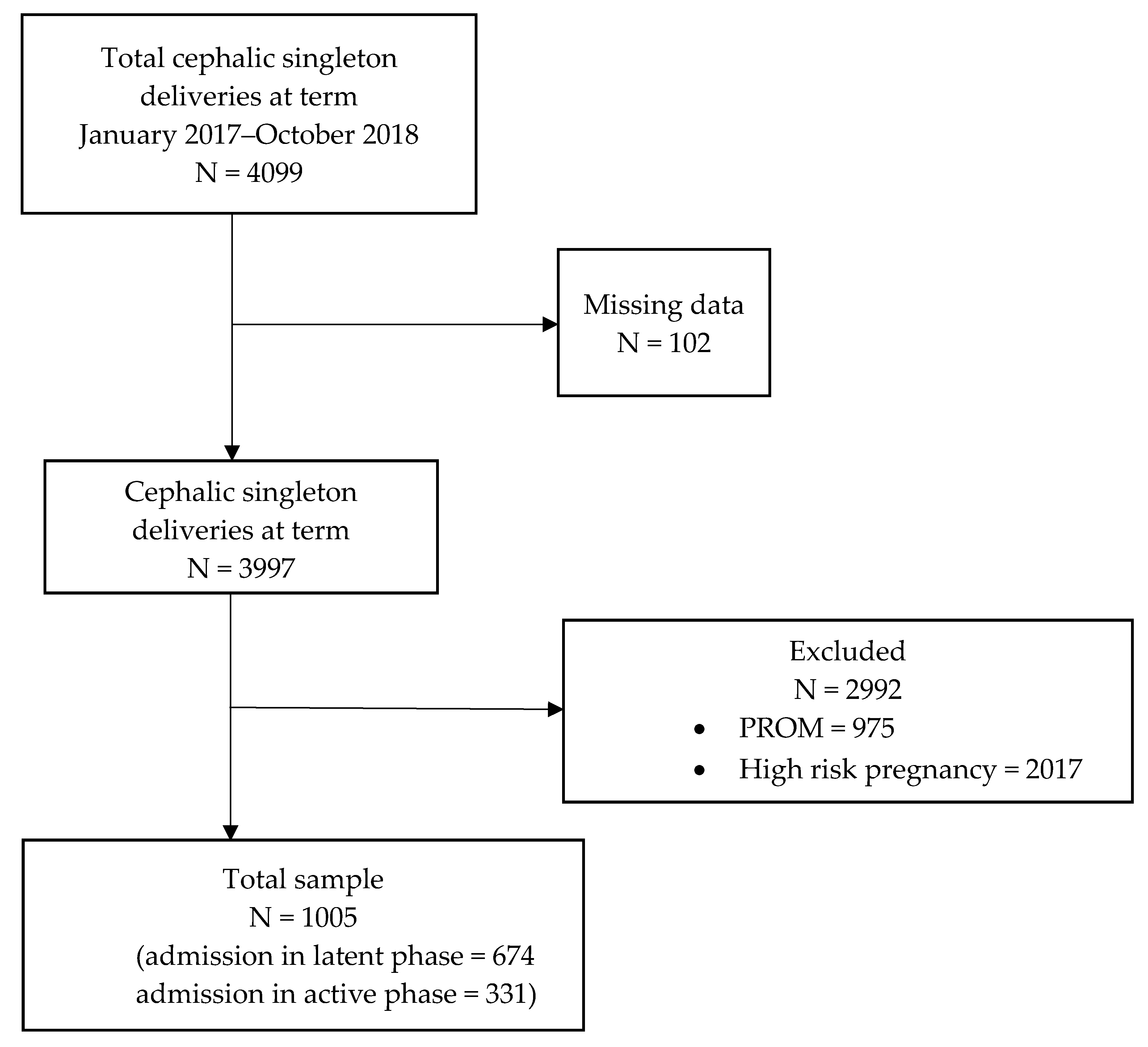
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ACOG. Committee Opinion No. 766: Approaches to Limit Intervention During Labor and Birth. Obstet. Gynecol. 2019, 133, e20–e28. [Google Scholar]
- Hemminki, E.; Simukka, R. The timing of hospital admission and progress of labour. Eur. J. Obstet. Gynecol. Reprod. Biol. 1986, 22, 85–94. [Google Scholar] [CrossRef]
- Rosenbloom, J.I.; Woolfolk, C.L.; Wan, L.; Stout, M.J.; Tuuli, M.G.; Macones, G.A.; Cahill, A.G. The Transition from Latent to Active Labor and Adverse Obstetrical Outcomes. Am. J. Obstet. Gynecol. 2019, 221, 487.e1–487.e8. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, E.; Souter, V.L.; Katon, J.K.; Sitcov, K. Cervical Dilation on Admission in Term, Spontaneous Labor and Maternal and Newborn Outcomes. Obstet. Gynecol. 2016, 127, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Wood, A.M.; Frey, H.A.; Tuuli, M.G.; Caughey, A.B.; Odibo, A.O.; Macones, G.A.; Cahill, A.G. Optimal Admission Cervical Dilation in Spontaneously Laboring Women. Am. J. Perinatol. 2016, 33, 188–194. [Google Scholar]
- Rota, A.; Antolini, L.; Colciago, E.; Nespoli, A.; Borrelli, S.E.; Fumagalli, S. Timing of hospital admission in labour: Latent versus active phase, mode of birth and intrapartum interventions. A correlational study. Women Birth 2018, 31, 313–318. [Google Scholar] [CrossRef]
- Neal, J.L.; Lamp, J.M.; Buck, J.S.; Lowe, N.K.; Gillespie, S.L.; Ryan, S.L. Outcomes of Nulliparous Women With Spontaneous Labor Onset Admitted to Hospitals in Preactive Versus Active Labor. J. Midwifery Womens Health 2014, 59, 28–34. [Google Scholar] [CrossRef] [Green Version]
- Mikolajczyk, R.T.; Zhan, J.; Grewal, J.; Chan, L.C.; Petersen, A.; Gross, M.M. Early versus Late Admission to Labor Affects Labor Progression and Risk of Cesarean Section in Nulliparous Women. Front. Med. 2016, 3, 26. [Google Scholar] [CrossRef] [Green Version]
- Iobst, S.E.; Breman, R.B.; Bingham, D.; Storr, C.L.; Zhu, S.; Johantgen, M. Associations among cervical dilatation at admission, intrapartum care, and birth mode in low-risk, nulliparous women. Birth 2019, 46, 253–261. [Google Scholar] [CrossRef]
- Holmes, P.; Oppenheimer, L.W.; Wen, S.W. The relationship between cervical dilatation at initial presentation in labour and subsequent intervention. BJOG 2001, 108, 1120–1124. [Google Scholar]
- Bailit, J.L.; Dierker, L.; Blanchard, M.H.; Mercer, B.M. Outcomes of Women Presenting in Active Versus Latent Phase of Spontaneous Labor. Obstet. Gynecol. 2005, 105, 77–79. [Google Scholar] [CrossRef]
- Tilden, E.L.; Lee, V.R.; Allen, A.J.; Griffin, E.E.; Caughey, A.B. Cost-Effectiveness Analysis of Latent versus Active Labor Hospital Admission for Medically Low-Risk, Term Women. Birth 2015, 42, 219–226. [Google Scholar] [CrossRef] [PubMed]
- McNiven, P.S.; Williams, J.I.; Hodnett, E.; Kaufman, K.; Hannah, M.E. An early labor assessment program: A randomized, controlled trial. Birth 1998, 25, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Incerti, M.; Locatelli, A.; Ghidini, A.; Ciriello, E.; Consonni, S.; Pezzullo, J.C. Variability in rate of cervical dilation in nulliparous women at term. Birth 2011, 38, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Intrapartum care for a positive childbirth experience. In WHO Guidelines; WHO: Geneva, Switzerland, 2018.
- Kobayashi, S.; Hanada, N.; Matsuzaki, M.; Takehara, K.; Ota, E.; Sasaki, H.; Nagata, C.; Mori, R. Assessment and support during early labour for improving birth outcomes. Cochrane Database Syst. Rev. 2017, 4, CD011516. [Google Scholar] [CrossRef]
- Salahuddin, M.; Mandell, D.J.; Lakey, D.L.; Eppes, C.S.; Patel, D.A. Maternal risk factor index and cesarean delivery among women with nulliparous, term, singleton, vertex deliveries, Texas, 2015. Birth 2019, 46, 182–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poobalan, A.S.; Aucott, L.S.; Gurung, T.; Smith, W.C.; Bhattacharya, S. Obesity as an independent risk factor for elective and emergency caesarean delivery in nulliparous women–systematic review and meta-analysis of cohort studies. Obes. Rev. 2009, 10, 28–35. [Google Scholar] [CrossRef]
- Remsberg, K.E.; McKeown, R.E.; McFarland, K.F.; Irwin, L.S. Diabetes in pregnancy and cesarean delivery. Diabetes Care 1999, 22, 1561–1567. [Google Scholar] [CrossRef]
- Boyle, A.; Reddy, U.M. Epidemiology of cesarean delivery: The scope of the problem. Semin. Perinatol. 2012, 36, 308–314. [Google Scholar] [CrossRef]
- Spong, C.Y.; Berghella, V.; Wenstrom, K.D.; Mercer, B.M.; Saade, G.R. Preventing the first cesarean delivery: Summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, and American College of Obstetricians and Gynecologists workshop. In reply. Obstet. Gynecol. 2013, 121, 687. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, J.C.; Kozhimannil, K.B.; McDermott, P.; Saade, G.R.; Srinivas, S.K.; Society for Maternal-Fetal Medicine Health Policy Committee. Comparing variation in hospital rates of cesarean delivery among low-risk women using 3 different measures. Am. J. Obstet. Gynecol. 2016, 214, 153–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, P.A.; Still, D.K.; Klein, M.C.; Singer, J.; Carty, E.A.; Liston, R.M.; Zupancic, J.A. Early Labor Assessment and Support at Home Versus Telephone Triage. Obstet. Gynecol. 2006, 108, 1463–1469. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Latent Phase (n = 674) | Active Phase (n =331) | p | |
|---|---|---|---|
| Maternal Age (years) | 30.87 ± 5.61 | 30.88 ± 5.46 | 0.98 |
| BMI ≥ 25 kg/m2 | 74 (11.0%) | 37 (11.2%) | 0.92 |
| Nationality | |||
| Italian | 464 (68.8%) | 204 (61.6%) | 0.02 |
| Foreigner | 210 (31.2%) | 127 (38.4%) | |
| Parity | |||
| Nulliparous | 375 (55.6%) | 102 (30.8%) | <0.01 |
| Multiparous | 299 (44.4%) | 229 (69.2%) | |
| Assisted Reproductive Technologies | 16 (2.4%) | 6 (1.8%) | 0.65 |
| Gestational age at delivery | 39.81 ± 1.78 | 39.71 ± 0.92 | 0.35 |
| Latent Phase (n = 674) | Active Phase (n =331) | p | Odds Ratio (95% CI) | |
|---|---|---|---|---|
| Nulliparous women | 375 | 102 | ||
| Maternal and delivery outcomes | ||||
| Epidural analgesia | 147 (39.2%) | 16 (15.7%) | <0.01 | 3.47 (1.96–6.14) |
| Augmentation of labor with oxytocin | 54 (14.4%) | 14 (13.7%) | 1.00 | 1.06 (0.56–1.99) |
| Cesarean delivery | 39 (10.4%) | 8 (7.8%) | 0.57 | 1.36 (0.61–3.02) |
| Vaginal delivery | 336 (89.6%) | 94 (92.2%) | 0.57 | 0.73 (0.33–1.62) |
| Major post-partum hemorrhage | 5 (1.3%) | 1 (1.0%) | 1.00 | 1.37 (0.16–11.82) |
| Hospital stays (days) | 3.01 ± 1.03 | 2.86 ± 1.39 | 0.14 | - |
| Neonatal outcomes | ||||
| Birthweight (g) | 3300± 347 | 3319 ± 345 | 0.58 | |
| Need for resuscitation | 1 (0.3%) | 0 | 1.00 | 0.82(0.03–20.32) |
| Cord pH | 7.25 ± 0.09 | 7.27 ± 0.09 | 0.06 | |
| Cord pH < 7.2 | 68 (18.1%) | 12 (11.8%) | 0.14 | 1.66 (0.86–3.21) |
| 1 min Apgar score < 7 | 4 (1.1%) | 0 | 0.58 | 2.48 (0.13–46.53) |
| NICU admission | 20 (5.3%) | 4 (3.9%) | 0.80 | 1.38 (0.46–4.13) |
| Multiparous women | 299 | 229 | ||
| Maternal and delivery outcomes | ||||
| Epidural analgesia | 43 (14.4%) | 14 (6.1%) | <0.01 | 2.58 (1.37–4.84) |
| Augmentation of labor with oxytocin | 18 (6.0%) | 5 (2.2%) | 0.03 | 2.87 (1.05–7.85) |
| Cesarean delivery | 3 (1.0%) | 2 (0.9%) | 1.00 | 1.15 (0.19–6.94) |
| Vaginal delivery | 296 (99.0%) | 227 (99.1%) | 1.00 | 0.87 (0.14–5.25) |
| Major post-partum hemorrhage | 6 (2.0%) | 5 (2.2%) | 1.00 | 0.91(0.28–3.04) |
| Hospital stays (days) | 3.54 ± 1.41 | 3.27 ± 1.51 | 0.07 | - |
| Neonatal outcomes | ||||
| Birthweight (g) | 3392 ± 371 | 3425 ± 353 | 0.22 | |
| Need for resuscitation | 0 | 1 (0.4%) | 0.43 | 0.25 (0.01–6.27) |
| Cord pH | 7.29 ± 0.09 | 7.29 ± 0.08 | 0.94 | |
| Cord pH < 7.2 | 37 (12.4%) | 30 (13.1%) | 0.90 | 0.94 (0.56–1.57) |
| 1 min Apgar score < 7 | 2 (0.7%) | 2 (0.9%) | 1.00 | 0.76 (1.11–5.47) |
| NICU admission | 13 (4.3%) | 12 (5.2%) | 0.68 | 0.82 (0.37–1.84) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seravalli, V.; Strambi, N.; Castellana, E.; Salamina, M.A.; Bettini, C.; Di Tommaso, M. Hospital Admission in the Latent versus the Active Phase of Labor: Comparison of Perinatal Outcomes. Children 2022, 9, 924. https://doi.org/10.3390/children9060924
Seravalli V, Strambi N, Castellana E, Salamina MA, Bettini C, Di Tommaso M. Hospital Admission in the Latent versus the Active Phase of Labor: Comparison of Perinatal Outcomes. Children. 2022; 9(6):924. https://doi.org/10.3390/children9060924
Chicago/Turabian StyleSeravalli, Viola, Noemi Strambi, Enrica Castellana, Maria Alessia Salamina, Chiara Bettini, and Mariarosaria Di Tommaso. 2022. "Hospital Admission in the Latent versus the Active Phase of Labor: Comparison of Perinatal Outcomes" Children 9, no. 6: 924. https://doi.org/10.3390/children9060924