
High Prevalence of Astigmatism in Children after School Suspension during the COVID-19 Pandemic Is Associated with Axial Elongation

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Vision Screening Procedure
2.3. Data Analysis
3. Results
3.1. Demographic Characteristics and Refractive Status
3.2. Prevalence of Astigmatism
3.3. Astigmats vs. Non-Astigmats
3.4. Multiple Linear Regression Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hashemi, H.; Fotouhi, A.; Yekta, A.; Pakzad, R.; Ostadimoghaddam, H.; Khabazkhoob, M. Global and Regional Estimates of Prevalence of Refractive Errors: Systematic Review and Meta-Analysis. J. Curr. Ophthalmol. 2017, 30, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.-W.; Lam, A.K.-C.; Deng, L.; Kee, C.-S. Characteristics of Astigmatism as a Function of Age in a Hong Kong Clinical Population. Optom. Vis. Sci. 2012, 89, 984–992. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Maguire, M.G.; Ciner, E.; Kulp, M.T.; Cyert, L.A.; Quinn, G.E.; Orel-Bixler, D.; Moore, B.; Ying, G.S. Vision in Preschoolers (VIP) Study Group (2014) Risk Factors for Astigmatism in the Vision in Preschoolers (VIP) Study. Optom. Vis. Sci. 2014, 91, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Kleinstein, R.N.; Jones, L.A.; Hullett, S.; Kwon, S.; Lee, R.J.; Friedman, N.E.; Manny, R.E.; Mutti, D.O.; Yu, J.A.; Zadnik, K.; et al. Refractive Error and Ethnicity in Children. Arch. Ophthalmol. 2003, 121, 1141–1147. [Google Scholar] [CrossRef] [PubMed]
- McKean-Cowdin, R.; Varma, R.; Cotter, S.A.; Tarczy-Hornoch, K.; Borchert, M.S.; Lin, J.H.; Wen, G.; Azen, S.P.; Torres, M.; Tielsch, J.M.; et al. Risk Factors for Astigmatism in Preschool Children: The Multi-Ethnic Pediatric Eye Disease and Baltimore Pediatric Eye Disease Studies. Ophthalmology 2011, 118, 1974–1981. [Google Scholar] [CrossRef]
- Zhao, J.; Pan, X.; Sui, R.; Munoz, S.R.; Sperduto, R.D.; Leon, B.E. Refractive Error Study in Children: Results from Shunyi District, China. Am. J. Ophthalmol. 2000, 129, 427–435. [Google Scholar] [CrossRef]
- He, M.; Zeng, J.; Liu, Y.; Xu, J.; Pokharel, G.P.; Ellwein, L.B. Refractive Error and Visual Impairment in Urban Children in Southern China. Investig. Ophthalmol. Vis. Sci. 2004, 45, 793–799. [Google Scholar] [CrossRef]
- Wu, J.F.; Bi, H.S.; Wang, S.M.; Hu, Y.Y.; Wu, H.; Sun, W.; Lu, T.L.; Wang, X.R.; Jonas, J.B. Refractive Error, Visual Acuity and Causes of Vision Loss in Children in Shandong, China. The Shandong Children Eye Study. PLoS ONE 2013, 8, e82763. [Google Scholar] [CrossRef]
- Li, S.-M.; Liu, L.-R.; Li, S.-Y.; Ji, Y.-Z.; Fu, J.; Wang, Y.; Li, H.; Zhu, B.-D.; Yang, Z.; Li, L.; et al. Design, Methodology and Baseline Data of a School-Based Cohort Study in Central China: The Anyang Childhood Eye Study. Ophthalmic Epidemiol. 2013, 20, 348–359. [Google Scholar] [CrossRef]
- Han, B.; Zhou, W.; Liu, C.; Yang, Y.; Cheng, H.; Xu, X. Epidemiological Study on Visual Acuity and Refractive Status of Primary Students and Junior High School Students in Shenzhen. Int. J. Ophthalmol. Clin. Res. 2016, 16, 2103–2106. [Google Scholar]
- Tong, L.; Saw, S.-M.; CARKEET, A.; Chan, W.-Y.; Wu, H.-M.; Tan, D. Prevalence Rates and Epidemiological Risk Factors for Astigmatism in Singapore School Children. Optom. Vis. Sci. 2002, 79, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.Y.; Lam, C.H.-I.; Yu, W.Y.; Li, Z.C.; Chin, M.P.; Lakshmanan, Y.; Wong, F.S.Y.; Do, C.W.; Lee, P.H.; Chan, H.H.L. Childhood Exposure to Constricted Living Space: A Possible Environmental Threat for Myopia Development. Ophthalmic Physiol. Opt. 2017, 37, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Chen, A.; Zou, M.; Liu, Z.; Young, C.A.; Zheng, D.; Jin, G. Prevalence and Time Trends of Refractive Error in Chinese Children: A Systematic Review and Meta-Analysis. J. Glob. Health 2021, 11, 08006. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Cheung, S.S.L.; Chan, H.-N.; Zhang, Y.; Wang, Y.M.; Yip, B.H.; Kam, K.W.; Yu, M.; Cheng, C.-Y.; Young, A.L.; et al. Myopia Incidence and Lifestyle Changes among School Children during the COVID-19 Pandemic: A Population-Based Prospective Study. Br. J. Ophthalmol. 2021, bjophthalmol-2021-319307. [Google Scholar] [CrossRef]
- Wang, J.; Li, Y.; Musch, D.C.; Wei, N.; Qi, X.; Ding, G.; Li, X.; Song, L.; Zhang, Y.; Ning, Y.; et al. Progression of Myopia in School-Aged Children after COVID-19 Home Confinement. JAMA Ophthalmol. 2021, 139, 293–300. [Google Scholar] [CrossRef]
- Mu, J.; Zhong, H.; Liu, M.; Jiang, M.; Shuai, X.; Chen, Y.; Long, W.; Zhang, S. Trends in Myopia Development among Primary and Secondary School Students during the COVID-19 Pandemic: A Large-Scale Cross-Sectional Study. Front. Public Health 2022, 10, 859285. [Google Scholar] [CrossRef]
- Liang, Y.; Leung, T.-W.; Lian, J.T.; Kee, C.-S. Significant Increase in Astigmatism in Children after Study at Home during the COVID-19 Lockdown. Clin. Exp. Optom. 2022, 11, 19–26. [Google Scholar] [CrossRef]
- Liang, Y.; Kee, C.-S. Risk Factors for Myopia in 2 Hong Kong School Systems: A Pilot Study. Asia-Pac. J. Ophthalmol. 2022, 11, 19–26. [Google Scholar] [CrossRef]
- Thibos, L.N.; Wheeler, W.; Horner, D. Power Vectors: An Application of Fourier Analysis to the Description and Statistical Analysis of Refractive Error. Optom. Vis. Sci. 1997, 74, 367–375. [Google Scholar] [CrossRef]
- Chan, S.E.; Kuo, H.K.; Tsai, C.L.; Wu, P.C. Astigmatism in Chinese Primary School Children: Prevalence, Change, and Effect on Myopic Shift. Jpn. J. Ophthalmol. 2018, 62, 321–326. [Google Scholar] [CrossRef]
- Pi, L.-H.; Chen, L.; Liu, Q.; Ke, N.; Fang, J.; Zhang, S.; Xiao, J.; Ye, W.-J.; Xiong, Y.; Shi, H.; et al. Refractive Status and Prevalence of Refractive Errors in Suburban School-Age Children. Int. J. Med. Sci. 2010, 7, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Fan, D.S.; Lam, D.S.; Lam, R.F.; Lau, J.T.; Chong, K.S.; Cheung, E.Y.; Lai, R.Y.; Chew, S.J. Prevalence, Incidence, and Progression of Myopia of School Children in Hong Kong. Investig. Ophthalmol. Vis. Sci. 2004, 45, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.F.; Hsiao, C.K.; Tung, Y.L.; Lin, L.L.; Chen, C.J.; Hung, P.T. The Prevalence of Astigmatism in Taiwan Schoolchildren. Optom. Vis. Sci. 2004, 81, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Mao, J.; Luo, R.; Li, F.; Pokharel, G.P.; Ellwein, L.B. Accuracy of Noncycloplegic Autorefraction in School-Age Children in China. Optom. Vis. Sci. 2004, 81, 49–55. [Google Scholar] [CrossRef]
- Ma, D.; Wei, S.; Li, S.-M.; Yang, X.; Cao, K.; Hu, J.; Fan, S.; Zhang, L.; Wang, N. Progression of Myopia in a Natural Cohort of Chinese Children during COVID-19 Pandemic. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 2813–2820. [Google Scholar] [CrossRef]
- Mandel, Y.; Stone, R.A.; Zadok, D. Parameters Associated with the Different Astigmatism Axis Orientations. Investig. Ophthalmol. Vis. Sci. 2010, 51, 723–730. [Google Scholar] [CrossRef]
- Gwiazda, J.; Grice, K.; Held, R.; McLellan, J.; Thorn, F. Astigmatism and the Development of Myopia in Children. Vis. Res. 2000, 40, 1019–1026. [Google Scholar] [CrossRef]
- Guggenheim, J.A.; Farbrother, J.E. The Association between Spherical and Cylindrical Component Powers. Optom. Vis. Sci. 2004, 81, 62–63. [Google Scholar] [CrossRef]
- Feldkaemper, M.; Schaeffel, F. An Updated View on the Role of Dopamine in Myopia. Exp. Eye Res. 2013, 114, 106–119. [Google Scholar] [CrossRef]
- Tideman, J.W.; Polling, J.R.; Voortman, T.; Jaddoe, V.W.V.; Uitterlinden, A.G.; Hofman, A.; Vingerling, J.; Franco, O.H.; Klaver, C.C.W. Low Serum Vitamin D Is Associated with Axial Length and Risk of Myopia in Young Children. Eur. J. Epidemiol. 2016, 31, 491–499. [Google Scholar] [CrossRef]
- Guggenheim, J.A.; Northstone, K.; McMahon, G.; Ness, A.R.; Deere, K.; Mattocks, C.; Pourcain, B.S.; Williams, C. Time Outdoors and Physical Activity as Predictors of Incident Myopia in Childhood: A Prospective Cohort Study. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2856–2865. [Google Scholar] [CrossRef] [PubMed]
- Rose, K.A.; Morgan, I.G.; Ip, J.; Kifley, A.; Huynh, S.; Smith, W.; Mitchell, P. Outdoor Activity Reduces the Prevalence of Myopia in Children. Ophthalmology 2008, 115, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Farbrother, J.E.; Welsby, J.W.; Guggenheim, J.A. Astigmatic Axis Is Related to the Level of Spherical Ametropia. Optom. Vis. Sci. 2004, 81, 18–26. [Google Scholar] [CrossRef]
- Kuo, Y.C.; Wang, J.H.; Chiu, C.J. Comparison of Open-Field Autorefraction, Closed-Field Autorefraction, and Retinoscopy for Refractive Measurements of Children and Adolescents in Taiwan. J. Formos. Med. Assoc. 2020, 119, 1251–1258. [Google Scholar] [CrossRef] [PubMed]

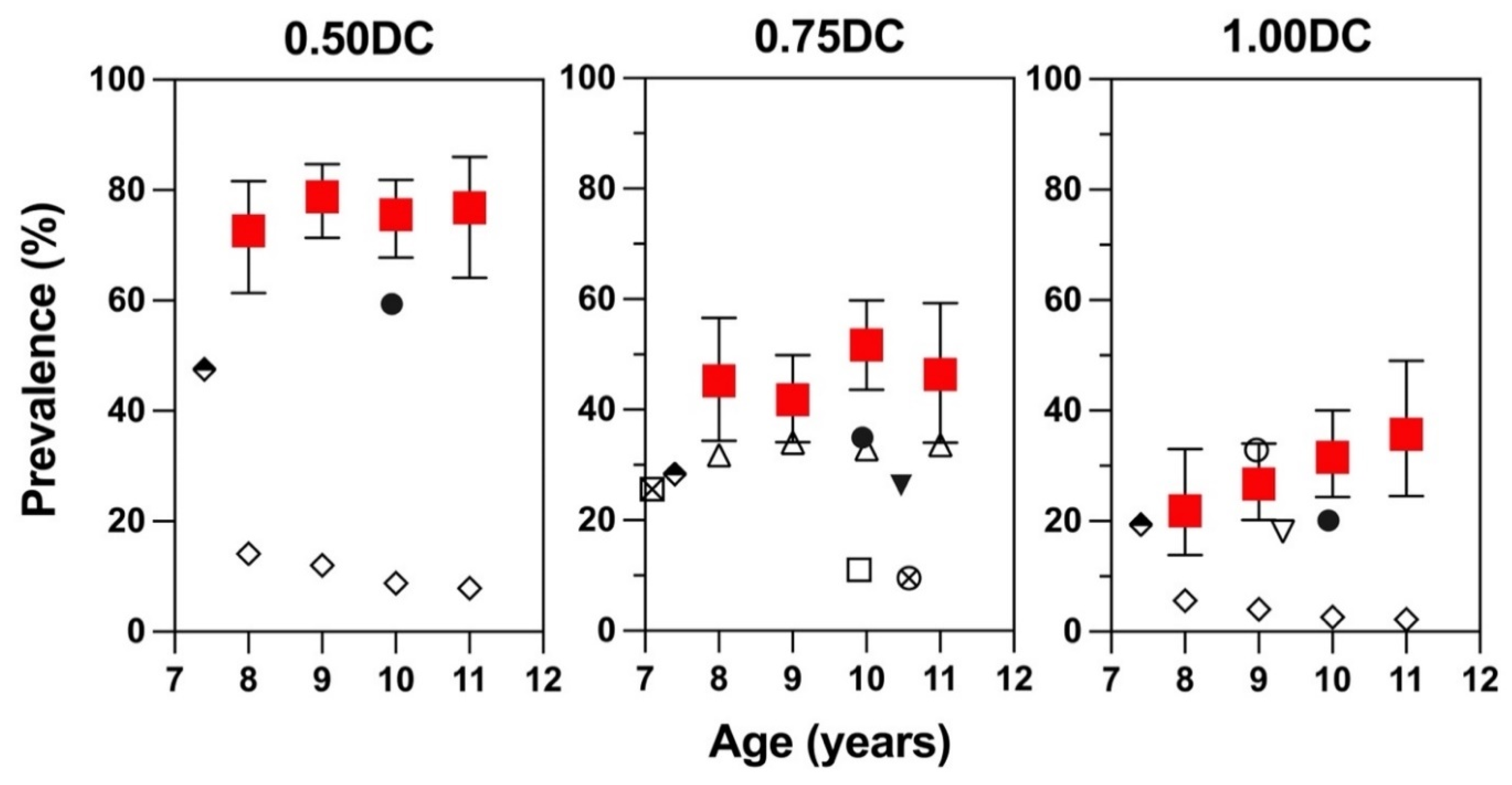
 ) with control data in Hong Kong ⚫ [12]; ▽ [22] and other Asian Chinese populations, including Singapore ⬘ [11], Taiwan [20], and Mainland China ⊗ [6]; ▼ [7]; △ [8]; ⊠ [9]; ☐ [10]; ◇ [21]. Only recent studies conducted on Asian Chinese population that consistently used either right eye or left eye to report the prevalence of astigmatism were included. Prevalence rates of various studies were stratified into three columns according to their definitions of astigmatism (Cyl ≥ 0.50, 0.75, and 1.00 DC). Note that data from Choi et al. 2017 [12] were not published but obtained via personal communication with the authors.
) with control data in Hong Kong ⚫ [12]; ▽ [22] and other Asian Chinese populations, including Singapore ⬘ [11], Taiwan [20], and Mainland China ⊗ [6]; ▼ [7]; △ [8]; ⊠ [9]; ☐ [10]; ◇ [21]. Only recent studies conducted on Asian Chinese population that consistently used either right eye or left eye to report the prevalence of astigmatism were included. Prevalence rates of various studies were stratified into three columns according to their definitions of astigmatism (Cyl ≥ 0.50, 0.75, and 1.00 DC). Note that data from Choi et al. 2017 [12] were not published but obtained via personal communication with the authors.
) with control data in Hong Kong ⚫ [12]; ▽ [22] and other Asian Chinese populations, including Singapore ⬘ [11], Taiwan [20], and Mainland China ⊗ [6]; ▼ [7]; △ [8]; ⊠ [9]; ☐ [10]; ◇ [21]. Only recent studies conducted on Asian Chinese population that consistently used either right eye or left eye to report the prevalence of astigmatism were included. Prevalence rates of various studies were stratified into three columns according to their definitions of astigmatism (Cyl ≥ 0.50, 0.75, and 1.00 DC). Note that data from Choi et al. 2017 [12] were not published but obtained via personal communication with the authors.
) with control data in Hong Kong ⚫ [12]; ▽ [22] and other Asian Chinese populations, including Singapore ⬘ [11], Taiwan [20], and Mainland China ⊗ [6]; ▼ [7]; △ [8]; ⊠ [9]; ☐ [10]; ◇ [21]. Only recent studies conducted on Asian Chinese population that consistently used either right eye or left eye to report the prevalence of astigmatism were included. Prevalence rates of various studies were stratified into three columns according to their definitions of astigmatism (Cyl ≥ 0.50, 0.75, and 1.00 DC). Note that data from Choi et al. 2017 [12] were not published but obtained via personal communication with the authors.

{kind=link}
{kind=link}
| Definitions | n | Astigmatism ≥ 0.50 D | Astigmatism ≥ 0.75 D | Astigmatism ≥ 1.00 D | ||||
|---|---|---|---|---|---|---|---|---|
| Prevalence (95% CI) | p Values | Prevalence (95% CI) | p Values | Prevalence (95% CI) | p Values | |||
| Total | 418 | 76.3 (72.0–80.4) | 46.5 (41.7–61.4) | 28.9 (24.6–33.5) | ||||
| Age | 8 | 73 | 72.6 (61.4–81.6) | 0.77 | 45.2 (34.4–56.6) | 0.40 | 21.9 (13.9–32.8) | 0.28 |
| 9 | 146 | 78.8 (71.4–84.7) | 41.8 (34.1–49.9) | 26.7 (20.2–34.4) | ||||
| 10 | 143 | 75.5 (67.8–81.9) | 51.7 (43.6–59.8) | 31.5 (24.4–39.5) | ||||
| 11 | 56 | 76.8 (64.1–86.0) | 46.4 (34.0–59.3) | 35.7 (24.5–48.8) | ||||
| Gender | Male | 234 | 76.5 (70.6–81.5) | 0.92 | 47.4 (41.1–53.8) | 0.64 | 29.1 (23.6–35.2) | 0.86 |
| Female | 184 | 76.1 (69.5–81.7) | 45.1 (38.1–52.3) | 28.3 (22.3–35.2) | ||||
| Astigmats (n = 195) | Non-Astigmats (n = 223) | p Values | |
|---|---|---|---|
| Age (years) | 9.48 ± 0.93 | 9.40 ± 0.93 | 0.927 |
| Gender | |||
| Males (%) | 57.2 | 54.9 | 0.636 |
| Spherical-equivalent Error (D) | −1.88 ± 1.67 | −1.35 ± 1.04 | <0.001 |
| Axial Length (mm) | 23.85 ± 1.18 | 23.58 ± 0.86 | <0.001 |
| Reading Time (hour) | 1.33 ± 0.87 | 1.32 ± 0.97 | 0.994 |
| Screen Time (hour) | 2.50 ± 1.82 | 2.47 ± 2.15 | 0.242 |
| Outdoor Activities Time (hour) | 1.42 ± 1.30 | 1.74 ± 1.67 | 0.044 |
| Beta | p-Value | |
|---|---|---|
| Cylindrical Error | ||
| Axial length | 0.181 | <0.001 |
| Reading hours | 0.003 | 0.946 |
| Screen hours | −0.011 | 0.584 |
| Outdoor hours | −0.017 | 0.498 |
| J0 Astigmatism | ||
| Axial length | 0.099 | <0.001 |
| Reading hours | −0.013 | 0.543 |
| Screen hours | −0.016 | 0.123 |
| Outdoor hours | −0.007 | 0.579 |
| J45 Astigmatism | ||
| Axial length | 0.002 | 0.872 |
| Reading hours | −0.01 | 0.443 |
| Screen hours | 0.017 | 0.013 |
| Outdoor hours | −0.011 | 0.161 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, S.-C.; Kee, C.-S.; Leung, T.-W. High Prevalence of Astigmatism in Children after School Suspension during the COVID-19 Pandemic Is Associated with Axial Elongation. Children 2022, 9, 919. https://doi.org/10.3390/children9060919
Wong S-C, Kee C-S, Leung T-W. High Prevalence of Astigmatism in Children after School Suspension during the COVID-19 Pandemic Is Associated with Axial Elongation. Children. 2022; 9(6):919. https://doi.org/10.3390/children9060919
Chicago/Turabian StyleWong, Suei-Cheng, Chea-Su Kee, and Tsz-Wing Leung. 2022. "High Prevalence of Astigmatism in Children after School Suspension during the COVID-19 Pandemic Is Associated with Axial Elongation" Children 9, no. 6: 919. https://doi.org/10.3390/children9060919