1. Introduction
The main goal of bracing adolescent and juvenile idiopathic scoliosis (AJIS) during pubertal growth is to arrest the progression of the Cobb angle (CAP) [
1,
2,
3,
4]. There is no worldwide consensus on the type of brace and wear time. The Cheneau–Toulouse–Munster (CTM) brace is widely used in Europe with full-time wear. The effectiveness of full-time brace wear is approximately 80% for all types of idiopathic scoliosis [
1,
2,
3,
4].
Observational studies have shown that scoliosis behavior (worsening or stability) depends on the curve pattern, with thoracic curves being more evolutive than lumbar curves [
5,
6]. Sanders and Al proposed a modified Lenke classification (mLenke) separating non-surgical scoliosis in main thoracic curves (MT) and main lumbar curves (ML) [
6], the latter including both thoracolumbar and lumbar main curves.
According to Weinstein’s BrAIST study, the most common duration of brace wear is >18 h daily. However, the authors reported a 90% success rate for a minimum of 12.9 h of effective brace wear. [
7]
Often, the actual and prescribed times of brace wear per day may differ [
8]. Compliance is higher with part-time brace prescriptions: 65% compliance for 23 h prescriptions, 71% for 12 h prescriptions, and 94% for 8 h prescriptions [
9]. Katz et al. found similar success ratios of brace wear time between 23 h and 16 h in-brace prescriptions but found poorer results for a wearing time down to 12 h (71% of success) and <7 h (31%) with a Boston brace [
10]. However, the literature remains contradictory about this [
11,
12]. To the best of our knowledge, no studies have been published featuring a prescription of 12 h nighttime wear of the CTM brace.
We hypothesized that 12 h of nighttime CTM brace wear is effective in treating AJIS. The main objective was to describe brace efficacy based on different curve patterns and the Risser classification. Afterward, we aimed to identify clinical and radiological factors associated with good results.
2. Materials and Methods
2.1. Patients
This was a monocentric retrospective cohort study of consecutive patients treated in a pediatric orthopedic surgery unit between 2006 and 2017 by a single pediatric spine surgeon (JLC).
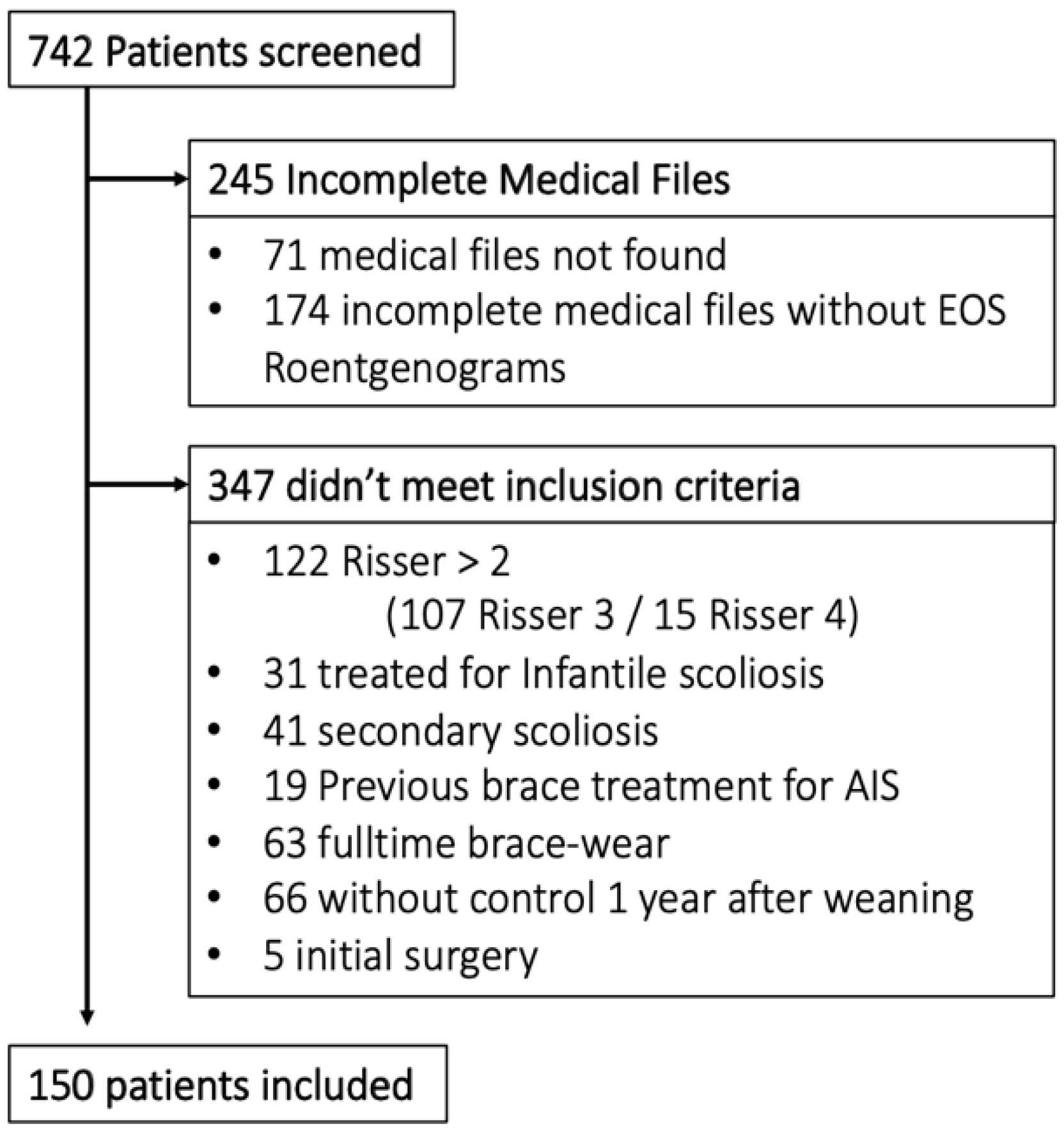
Inclusion criteria were: evolutive AJIS (CAP > 5° between 2 successive roentgenograms or Cobb angle >30° from the first visit), Risser sign = 0, 1 or 2, and initial prescription of part-time CTM brace. Incomplete medical files without available full spine roentgenograms, as well as clinical and radiological control 1 year after weaning, were excluded.
2.2. Treatment
The CTM Brace is a tailored, underarm, single piece, balanced, asymmetric brace with a pressure pad and expansion chambers composed of 4 mm polyethylene (
Figure 1).
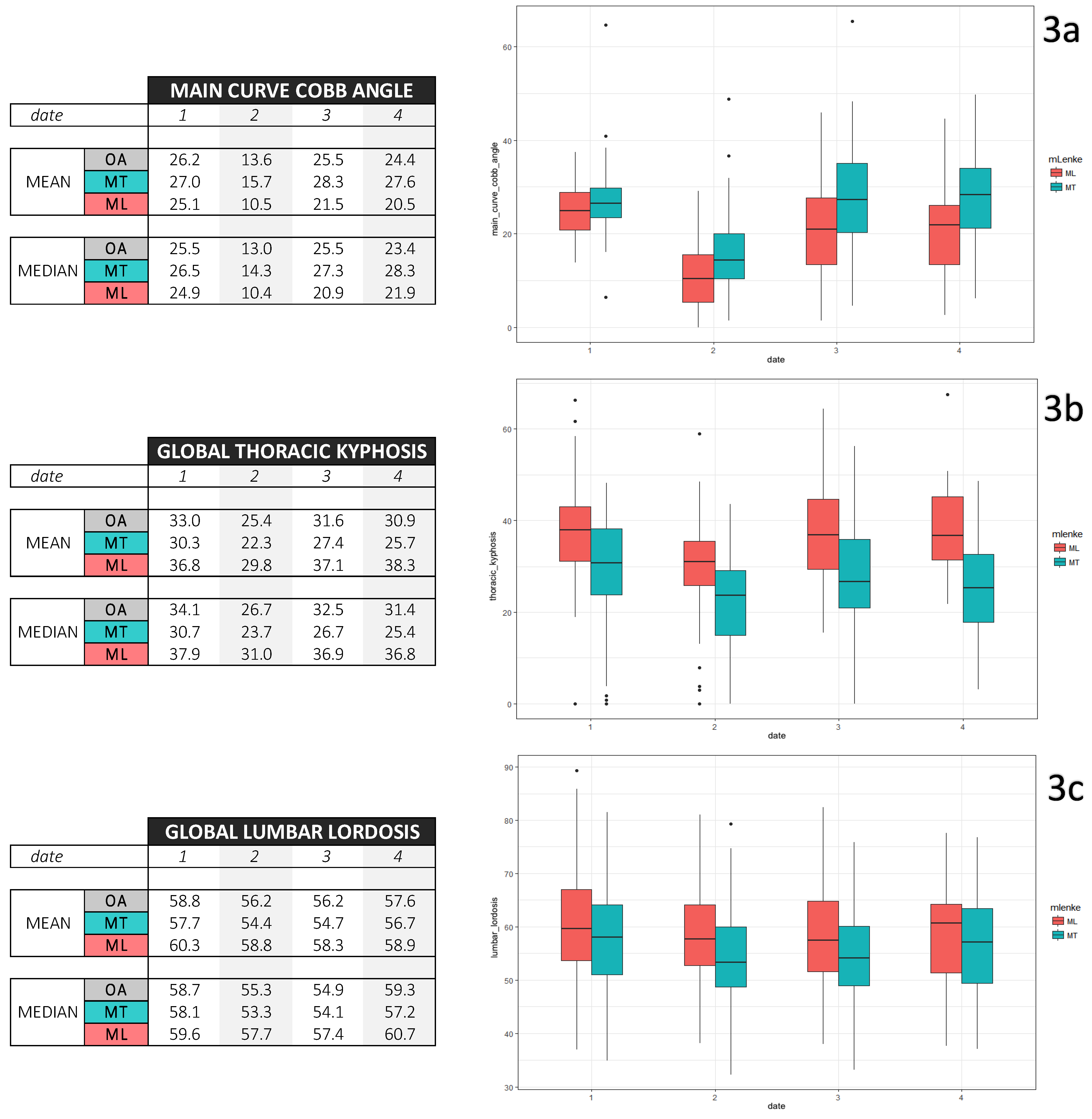
Data were collected at 4 dates:
- -
Date 1: Medical prescription, 3D scan body acquisition followed by brace-digitalized fabrication. Initial brace wear occurs at day 30 with a target of 12 h wear time out of 24, meaning all night and a small part of the day, usually the evening;
- -
Date 2: In-brace roentgenograms at Day 60, after foam pad adjunction to enhance correction;
- -
Date 3: Weaning, having a Risser test ≥ 4 and height stability;
- -
Date 4: Medical visit to evaluate brace efficiency with medical examination and roentgenograms, at least one year after weaning.
For brace renewal, delivery and foaming were simultaneous. Monitoring was shared as follows: orthotist visits every 2–3 months and medical visits every 6 months. No physiotherapy was prescribed.
2.3. Measures and X-ray Analysis
One experienced pediatric spine surgeon (JLC) performed clinical measurements in successive medical visits. These measurements included standing and sitting height, rib hump and lumbar prominence measured with lead wire, and inequality of leg length search for dates 1, 3 and 4. Non-compliance, such as failing to respect the 12 h wear time or not wearing the brace at all, was assessed through interrogation.
Full Spine Roentgenograms were taken on dates 1, 2 and 4 with EOS® technology on nude spine after a night without the brace, to avoid maintaining proprioceptive effect. In-brace full spine roentgenograms were taken on date 2.
An independent physician (GdC) performed digital measurements on “Keops Analyser” (Smaio, Lyon, France). This software has proved its superiority over direct measurements on X-rays [
13]. Data were classified in 3 categories: GLOBAL for global spine parameters, REGIONAL for scoliotic deformation pattern, and LOCAL for apex vertebrae.
Lumbar lordosis (LL) and thoracic kyphosis (TK) were measured using the Cobb method and represent angles of vertebral segments in lordosis or kyphosis, respectively, independently from predefined levels [
14]. The overcurve was defined as the proximal to the thoracic curve above the main thoracic and mid-thoracic above the main lumbar curves. Frontal C7 tilt was the angle between the vertical line passing through the center of the sacrum and the line passing through the center of C7 and the center of the sacrum. Sagittal C7 tilt angle was measured between the vertical line passing through the center of the sacrum and the line passing through the center of C7 and the center of the sacrum.
The acromio-femoral angle was the angle between the bi-coracoid line and the bi-femoral line, passing through the center of both femoral heads. The lateral displacement of the apical vertebra was measured as the distance from the apical vertebra and the midline passing through the center of the sacrum. Ilio-lumbar angle was measured between the bi-iliac line and the tangent of the most inclined lumbar vertebra. Wedging was measured as the angle between the superior and inferior vertebral plates. (
Supplemental file S1)
2.4. Main Outcome
The primary endpoint for brace success was defined if two criteria were present: (1) no indication for surgery and (2) the main curve CAP ≤ 5° between date 1 and date 4.
2.5. Statistical Analysis
Data were managed by an independent physician (GDC), and statistical analysis was carried out by an independent statistician (IB).
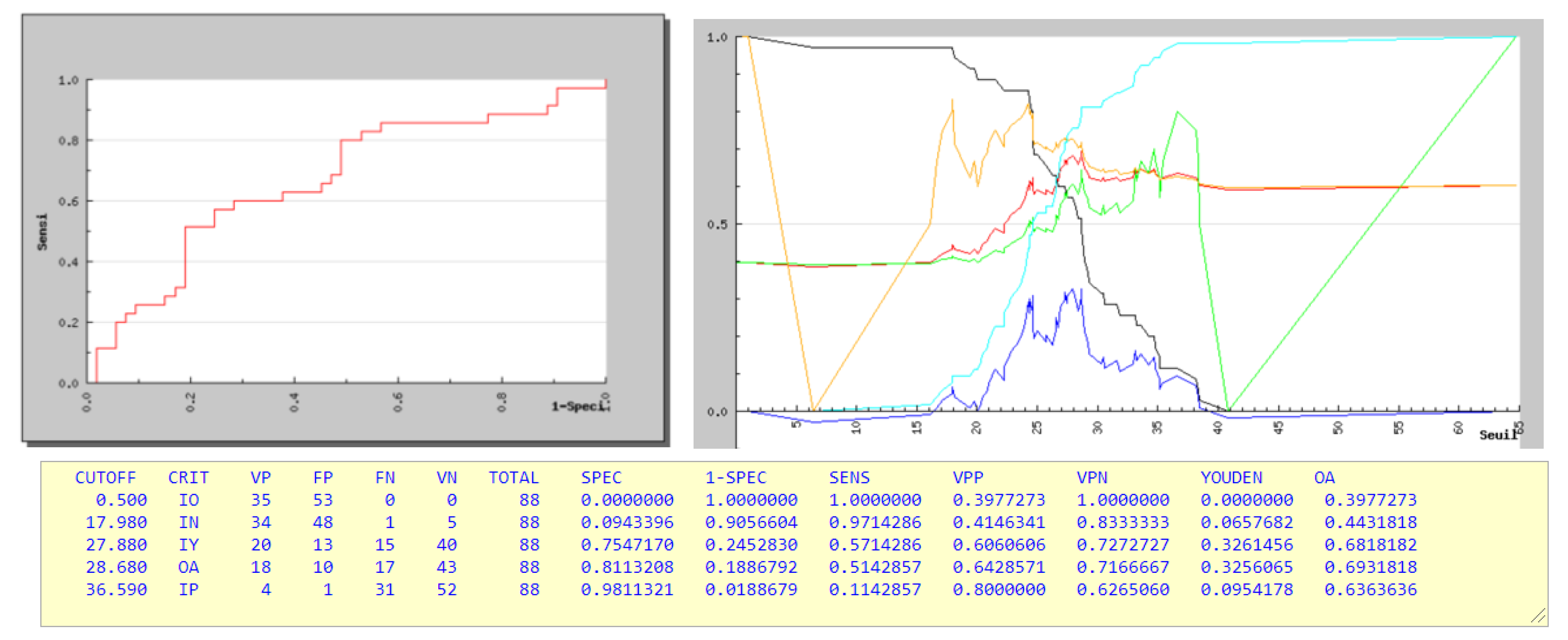
Chi squared and exact Fisher’s test were used to compare qualitative values, and a T-test was used for quantitative values after verification of normal distribution. Boxplots were made to describe repetitive measurements. To identify the cutoff values, ROC curves were realized. A logistic regression model was used for the primary outcome. Subgroup analysis was performed using the mLenke classification and Risser test.
The multiple regression model included potential influencing factors with clinical pertinence and p < 0.2 from univariate analysis. Odds ratios (OR) are presented with confidence interval 95% (CI) and p-values.
R software was used to perform calculations and diagnostic analysis was performed on Anger University software.
2.6. Ethical Statement
All procedures described in this article were in accordance with the ethical standards of the institutional review board (CNIL with number 2017728v0, 14 September 2017) and with the 1964 Helsinki Declaration and its later amendments. Formal consent from parents and patients was not necessary for the retrospective analysis of the anonymized data.
4. Discussion
Our study confirmed the efficiency of 12 h of nighttime brace wear, with higher success for ML curves [
14,
15].
The effectiveness of full-time CTM brace wear was reported in three different studies with 81 to 83% success [
2,
3,
4]. From our data, the overall success rate was 70%, but only 21 out of 150 patients (14%) underwent surgery or would need surgery in the future, with CA ≥45°. In turn, 86% of our cohort avoided surgery completely.
In the BrAIST study, the mean initial CA was 30°, and success was defined by CA ≤ 50° at skeletal maturity. A 90% success rate has been reported with a duration of daily brace wear between 12.9 and 17.6 h [
7]. With the same criteria of CA ≤ 50°, Thompson and Al found differences of success between MT (66%) and ML (85%) using TLSO full-time brace wear; these ratios of success are consistent with our results of 60% and 84% success with part-time bracing, while considering that we have used more severe criteria of success [
14].
Eight hours of hypercorrective brace wear (e.g., CAEN Brace) during the night has been prescribed for single curves with 66 to 75% success [
16,
17,
18,
19]. These results are comparable to our series of CTM braces, where we included both single and double curves. We emphasized nighttime because growth is higher during the night and because wearing a brace during the night is easier for a teenager than at school or during the daytime, in general.
We found better results for adolescent idiopathic scoliosis (70% success) than for juvenile idiopathic scoliosis compared to the Jarvis study (43% success for nighttime bracing). [
20] Boulot and Lateur recommend early treatment of AIS with nighttime bracing. [
3,
21] However, from our study, the earlier we treat with part-time bracing, the worse results we have, and our results are inferior to full-time brace wear for Risser stage 0–1 in MT and Risser stage 0 in ML. This result deserves caution since we tend to treat the more severe curves earlier.
Concerning the stage of growth, our data did not suggest that the Risser sign is a strong predictor of success. Thus, a more precise growth classification than the Risser sign should help define the protocol of brace wear, as well as find the curve acceleration phase. Correlations have been demonstrated using hand radiographs with the Tanner–Whitehouse-III or Greulich and Pyle atlas. Sander’s classification should also be useful [
6]. For clinical data, peak height velocity remains the best indicator, whereas the Tanner stage is an “invasive” examination for teenage girls in routine consultation.
For MT scoliosis, a Cobb angle of 28 degrees was the maximum limit when wearing a brace for 12 h overnight, which was consistent with Lateur’s study [
21] (
Figure 4).
Among less common predictors, the sitting height, thoracic rib hump, presence of high overcurve CA and main curve poor reduction in-brace were associated with failure for both MT and ML.
For MT, a good sagittal C7 tilt balance in-brace was associated with success. However, various patterns of the main thoracic curves are classified in the same gross group, with different responses to brace treatment [
22]. This finding suggests the brace prescriptor to use lateral bending with assessment of the sagittal alignment to obtain better CA reduction in brace [
23].
For ML, despite our small sample size, unbalanced frontal C7 tilt was correlated with failure. This imbalance is always on the same side as the lateral displacement of the apex vertebrae. This encourages us to use the lumbar shift with posterolateral force as much as possible for correcting lumbar and thoraco-lumbar curves.
For both groups, overcurve management is an obstacle to success, even with our underarm brace.
This study has several limitations. The sample size was limited; we were not able to include a considerable number of patients who had incomplete roentgenograms in their medical files. Moreover, we were not able to measure vertebral rotation. Furthermore, brace compliance was established only through patient and parent questioning and environment data, and no in-brace monitor was used.
Despite these limitations, our population is comparable to other studies. All clinical and radiological data has been analyzed with rigorous methodology: strict selection of cases, constant treatment protocol, x-rays under brace to check the effectiveness of the brace, and radiological results one year after brace weaning.


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}