
Qualitative and Arts-Based Evidence from Children Participating in a Pilot Randomised Controlled Study of School-Based Arts Therapies †


Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology
2.2. Study Design
2.3. Study Procedure
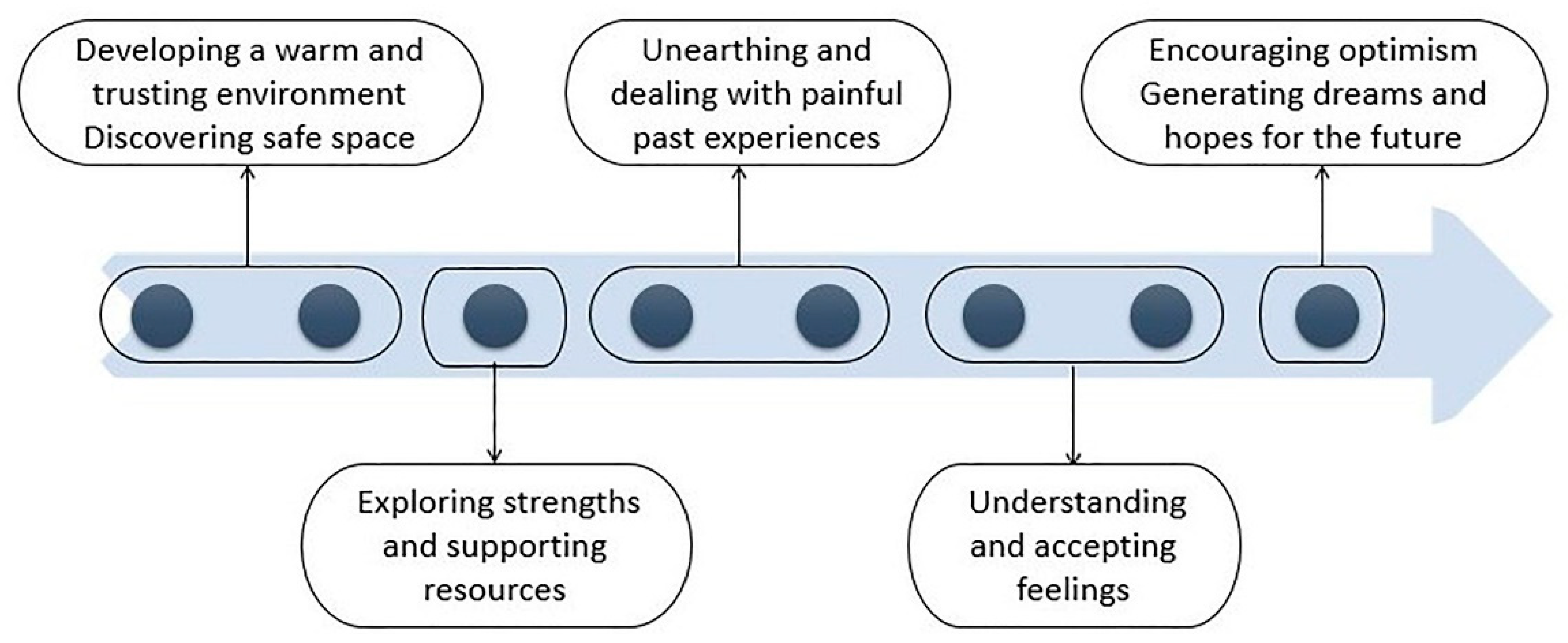
2.4. Arts Therapies Intervention
2.5. Methods of Data Collection and Analysis
2.5.1. Interviews with Children
2.5.2. Children’s Arts Work
3. Findings
3.1. Interviews with Children
3.1.1. Helpful Elements of Arts Therapies for Children’s Mental Health and Well-Being
Engagement with the Arts and Self-Expression
“I was sharing things that I was not used to share with anyone else.”(9 years-old-dance movement therapy)
“I made it [the character] look like crazy, you know, like my auntie used to be before she passed away. I want to be like my auntie so this [character] was actually me.”(9 years-old-art therapy)
“One of my favourite [role-play] was the pirates on the island, where we could choose to fight with the pirates on the boat if we wanted, or stay still on the island.”(9 years-old-dance movement therapy)
“I could tell my own story through my own puppet, but nobody knows if it’s a true story or if I made it all up.”(8 years-old-dramatherapy)
“I placed all my family in my sand tray, some trees around and a lake that I go with my parents to relax and spend the weekend sometimes […] the sense of the sand was very relaxing, reminded me of our weekends away.”(10 years-old-art therapy)
Safe Space
“We all know that it’s not like gossip what we say and we have to protect each other.”(9 years-old-music therapy)
“It was easy to share when I choose the people I want to share with and I know that we all do the same […] confidentiality was very helpful.”(9 years-old-dance movement therapy)
“I liked the sessions that started and finished with the same song to know that I am not in the class anymore, and to prepare me to go back to the class. The song in the end was my favourite; it made me happier and ready to go back to class.”(8 years-old-music therapy)
Stress Relief
“When I feel upset I focus on my breath and it helps me calm down.”(9 years-old-dance movement therapy)
“It made feel less stressed than I was used to be. I am still stressed in the inside but not on the outside anymore. Before I would be stressed in the inside and also the outside.”(10 years-old-art therapy)
“It made me sleep better because I felt less stressed.”(10 years-old-dramatherapy)
“I try to relax for ten minutes before I go to bed and I sleep better than before.”(9 years-old-dance movement therapy)
Empowerment
“My dream is to become a head teacher, that’s the wish I wrote down on my dreamcatcher and I hope this dream will come true one day […] to help other children feel good, take good grades, have fun at school and be fair.”(10 years-old-art therapy)
“I had a vision of myself as a volcano which has superpowers. When I’m angry, I look like the fire. When I’m calm, I look like the water. When I’m in the middle, I look like the clouds. I notice non-stop different things in my mind; water, fire, clouds… but most of the time I feel like the fire.”(10 years-old-art therapy)
“When we were sharing the boat of our difficulties, I was thinking that things will get better and I felt better.”(9 years-old-art therapy)
Coping Mechanisms
“I used to be really angry, I wanted to destroy everything. I had never listened in my life, never. I couldn’t even concentrate.”(10 years-old-art therapy)
“I’m fighting less with my brothers, and I control my anger. I try not to respond immediately when something happens and take my own time when I need it.”(10 years-old-dance movement therapy)
“When I am frustrated, I know that there are better ways than being mad at other people when they haven’t really done anything and it’s not their fault.”(9 years-old-dramatherapy)
“I got to forget about all the bad things, or most of the bad things in my mind.”(9 years-old-dramatherapy)
“I feel happier coming to school.”(7 years-old-music therapy)
3.1.2. Unhelpful Elements of Arts Therapies for Children’s Mental Health and Well-Being
Lack of Time
“I could spend hours, no, I could spend days in each craft we did. I didn’t want to feel in a rush.”(8 years-old-art therapy)
Lack of Group Cohesion
“I didn’t feel comfortable to share around S, we fight a lot in the class and I can’t concentrate when he is around.”(10 years-old-art therapy)
“It was when we did the mirroring that D said “I don’t want to do this, I don’t like that” but I think he just didn’t want to be a partner with me […] I didn’t feel good about it.”(9 years-old-dance movement therapy)
“It was so annoying and frustrating when R and E were shouting at each other so loud that I couldn’t focus for the rest of the time.”(10 years-old-dramatherapy)
Small Number of Sessions and High Number of Children
“I felt very sad because the sessions were over. I was crying without reason.”(9 years-old-dance movement therapy)
“I felt upset because I didn’t want to let it go.”(7 years-old-music therapy)
“I would prefer smaller numbers [of children], like five of us in each group.”(8 years-old-dance movement therapy)
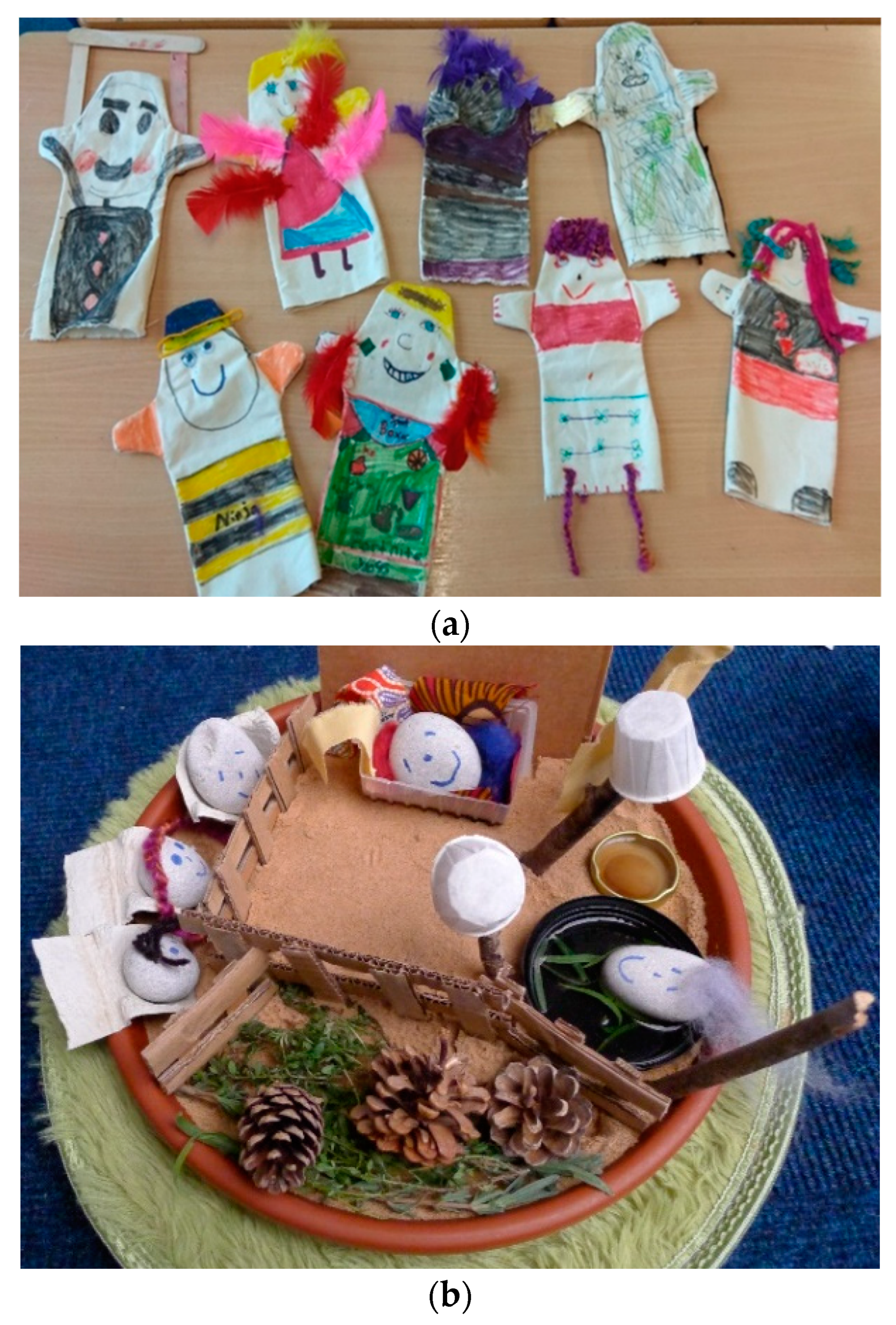
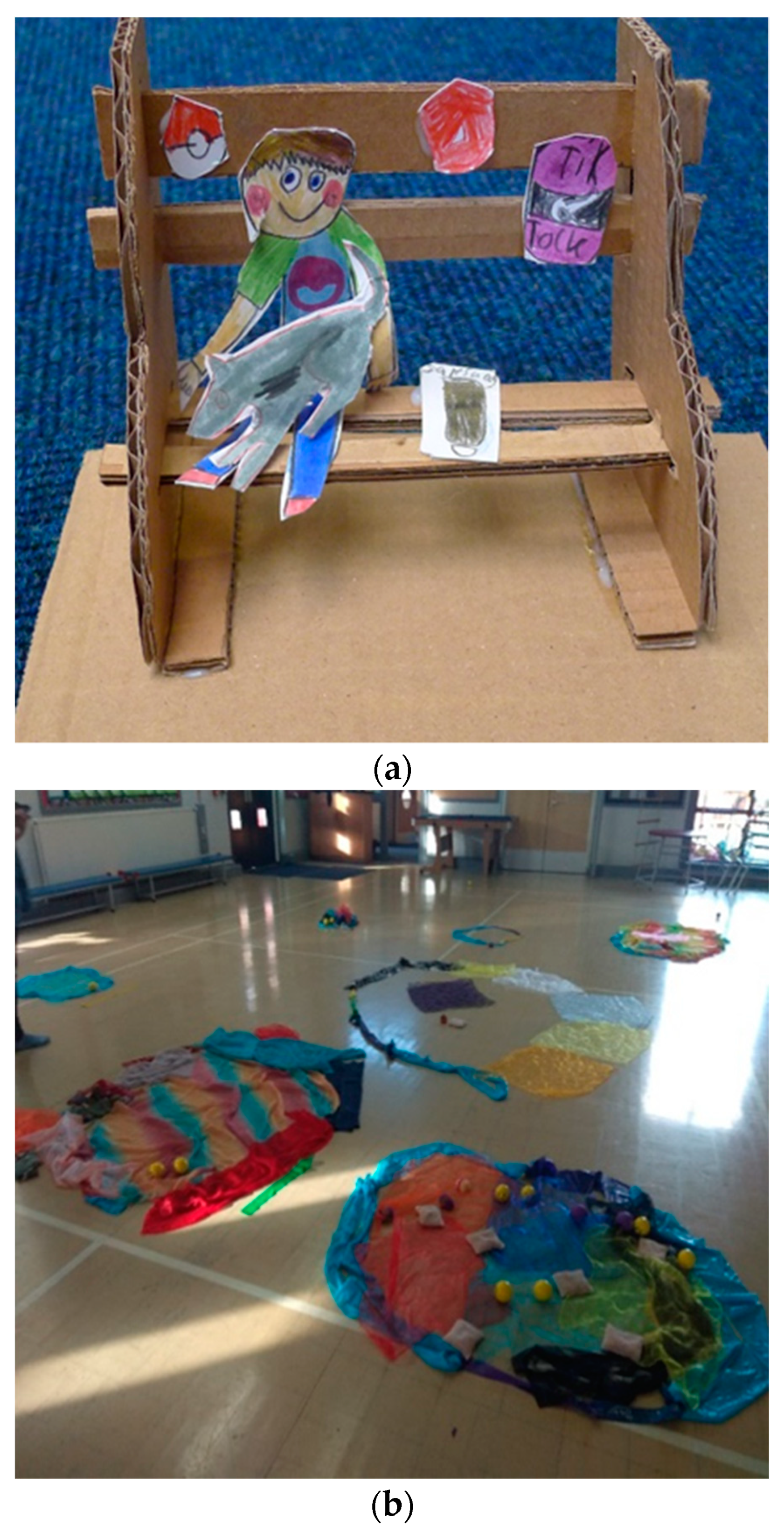
3.2. Children’s Arts Work
3.2.1. Themes of Children’s Arts Work
3.2.2. Aesthetic Qualities of Children’s Arts Work
4. Discussion
4.1. Overview of Findings
4.2. Improving the Quality of Group Arts Therapies
4.3. Strenghts and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://sdgs.un.org/publications/transforming-our-world-2030-agenda-sustainable-development-17981 (accessed on 1 June 2022).
- World Health Organization. Prevention of Mental Disorders: Effective Interventions and Policy Options; WHO Department of Mental Health and Substance Abuse, Prevention Research Centre: Nijmegen, Maastricht, 2004. Available online: https://www.who.int/mental_health/evidence/en/prevention_of_mental_disorders_sr.pdf (accessed on 1 June 2022).
- Place2Be. School Staff Witness an Increase in Pupil Anxiety, Low Self-Esteem and Depression. 2022. Available online: https://www.childrensmentalhealthweek.org.uk/news/school-staff-witness-an-increase-in-pupil-anxiety-low-self-esteem-and-depression/ (accessed on 1 June 2022).
- UK Parliament. Children and Young People’s Mental Health. House of Commons, Health and Social Care Committee. 2021. Available online: https://committees.parliament.uk/publications/8153/documents/83622/default/ (accessed on 1 June 2022).
- Children’s Commissioner. The State of Children’s Mental Health Services 2020/21. 2021. Available online: cco-the-state-of-childrens-mental-health-services-2020-21.pdf (accessed on 1 June 2022).
- NHS Confederation. Reaching the Tipping Point: Children and Young People’s Mental Health. Available online: https://www.nhsconfed.org/sites/default/files/2021-08/Reaching%20the%20tipping%20point%20Final.pdf (accessed on 1 June 2022).
- Children’s Society. The Good Childhood Report 2020. 2020. Available online: https://www.childrenssociety.org.uk/sites/default/files/2020-11/Good-Childhood-Report-2020.pdf (accessed on 1 June 2022).
- EBPU Bridging Research and Practice in Child Mental Health: Key Findings. Evidence Based Practice Unit. EBPU Key Findings. 2021. Available online: annafreud.org (accessed on 1 June 2022).
- Gislason, M.K.; Kennedy, A.M.; Witham, S.M. The interplay between social and ecological determinants of mental health for children and youth in the climate crisis. Int. J. Environ. Res. Public Health 2021, 18, 4573. [Google Scholar] [CrossRef] [PubMed]
- Marks, E.; Hickman, C.; Pihkala, P.; Clayton, S.; Lewandowski, E.R.; Mayall, E.E.; Wray, B.; Mellor, C.; van Susteren, L. Young people’s voices on climate anxiety, government betrayal and moral injury: A global phenomenon. Lancet Planet. Health 2021, 5, e863–e873. [Google Scholar] [CrossRef]
- Kavanagh, J.; Oliver, S.; Caird, J.; Tucker, H.; Greaves, A.; Harden, A.; Oakley, A.; Lorenc, T.; Thomas, J. Inequalities and the Mental Health of Young People: A Systematic Review of Secondary School-Based Cognitive Behavioural Interventions; EPPI-Centre, Social Science Research Unit; Institute of Education London: London, UK, 2009. [Google Scholar]
- Greenberg, M.T. School-based prevention: Current status and future challenges. Eff. Educ. 2010, 2, 27–52. [Google Scholar] [CrossRef]
- Capp, C. Our community, our schools: A case study of program design for school-based mental health services. Child. Sch. 2015, 37, 241–248. [Google Scholar] [CrossRef]
- Goldie, I.; Elliott, I.; Regan, M.; Bernal, L.; Makurah, L. Mental Health and Prevention: Taking Local Action. London: Mental Health Foundation. 2016. Available online: https://www.mentalhealth.org.uk/sites/default/files/mental-health-and-prevention-taking-local-action-for-better-mental-health-july-2016.pdf (accessed on 1 June 2022).
- Deboys, R.; Holttum, S.; Wright, K. Processes of change in school-based art therapy with children: A systematic qualitative study. Int. J. Art Ther. 2017, 22, 118–131. [Google Scholar] [CrossRef]
- DoH & DfE. Transforming Children and Young People’s Mental Health Provision: A Green Paper. 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/664855/Transforming_children_and_young_people_s_mental_health_provision.pdf (accessed on 1 June 2022).
- NHS England. The Five Year Forward View Mental Health Taskforce: Public Engagement Findings. 2015. Available online: https://www.england.nhs.uk/mentalhealth/wp-content/uploads/sites/29/2015/09/fyfv-mental-hlth-taskforce.pdf (accessed on 1 June 2022).
- Kearney, C.A. Getting Your Child to Say “Yes” to School: A Guide for Parents of Youth with School Refusal Behavior; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Children’s Commissioner for England. Annual Report and Accounts. 2017. Available online: https://www.childrenscommissioner.gov.uk/wpcontent/uploads/2017/07/Annual-Report-and-Accounts-version-2017.pdf (accessed on 1 June 2022).
- Moula, Z.; Powell, J.; Karkou, V. An investigation of the effectiveness of arts therapies interventions on measures of quality of life and wellbeing: A pilot randomized controlled study in primary schools. Front. Psychol. 2020, 11, 586134. [Google Scholar] [CrossRef]
- Children’s Society. The Good Childhood Report 2018; The Children’s Society: London, UK, 2018; Available online: https://www.childrenssociety.org.uk/sites/default/files/good_childhood_summary_2018.pdf (accessed on 1 June 2022).
- Karkou, V.; Sanderson, P. Arts Therapies: A Research Based Map of the Field; Elsevier: Edinburgh, UK, 2006. [Google Scholar]
- Karkou, V. Arts Therapies in Schools: Research and Practice; Jessica Kingsley Publishers: London, UK, 2010. [Google Scholar]
- Carr, C.E.; Tsiris, G.; Swijghuisen Reigersberg, M. Understanding the present, re-visioning the future: An initial mapping of music therapists in the United Kingdom. Br. J. Music Ther. 2017, 31, 68–85. [Google Scholar] [CrossRef]
- British Association of Art Therapists (BAAT). Editorial: The state-of-the-art, building a positive future for art therapy through systematic research. Int. J. Art Ther. 2018, 24, 53–55. [Google Scholar]
- Zubala, A.; Karkou, V. Dance movement psychotherapy practice in the UK: Findings from the arts therapies survey 2011. Body Mov. Danc. Psychother. 2014, 10, 21–38. [Google Scholar] [CrossRef] [Green Version]
- Uttley, L.; Scope, A.; Stevenson, M.; Rawdin, A.; Taylor Buck, E.; Sutton, A.; Wood, C. Systematic review and economic modelling of the clinical effectiveness and cost effectiveness of art therapy among people with non-psychotic mental healthdisorders. Health Technol. Assess. 2015, 19, 18. [Google Scholar] [CrossRef] [Green Version]
- Moula, Z.; Karkou, V.; Powell, J. A pilot randomised controlled trial of child-focused process and outcome evaluation of arts therapies at primary mainstream schools: Study protocol. Int. J. Arts Health 2019, 13, 1703198. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.B.; Onwuegbuzie, A.J.; Turner, L.A. Toward a definition of mixed methods research. J. Mix. Methods Res. 2007, 1, 112–133. [Google Scholar] [CrossRef]
- Howe, K.R. Against the quantitative-qualitative incompatibility thesis or dogmas die hard. Educ. Res. 1988, 17, 10–16. [Google Scholar] [CrossRef]
- Creswell, J.W. A Concise Introduction to Mixed Methods Research; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Brierley, J.A. The role of a pragmatist paradigm when adopting mixed methods in behavioural accounting research. Int. J. Behav. Account. Financ. 2017, 6, 140–154. [Google Scholar] [CrossRef]
- Onwuegbuzie, A.J.; Johnson, R.B. The validity issue in mixed research. Res. Sch. 2006, 13, 48–63. [Google Scholar]
- Teddlie, C.; Tashakkori, A. Foundations of Mixed Methods Research: Integrating Quantitative and Qualitative: Approaches in the Social and Behavioral Sciences; SAGE Publications: London, UK, 2009. [Google Scholar]
- Yvonne Feilzer, M. Doing mixed methods research pragmatically: Implications for the rediscovery of pragmatism as a research paradigm. J. Mix. Methods Res. 2010, 4, 6–16. [Google Scholar] [CrossRef]
- National Institute for Health Research. Programme Development Grants: Guidance Information for Applications. RP-DG-0517-1. 2017. Available online: https://www.nihr.ac.uk/funding-and-support/documents/funding-for-research-studies/research-programmes (accessed on 1 June 2022).
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Br. Med. J. 2008, 29, a1655. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef]
- Moula, Z. Child-Focused Process and Outcome Evaluation of Arts Therapies for Children in Primary Schools. Ph.D. Thesis, Edge Hill University, Ormskirk, UK, 2020. [Google Scholar]
- Moula, Z. A systematic review of the effectiveness of art therapy delivered in school-based settings to children aged 5–12 years. Int. J. Art Ther. 2020, 25, 88–89. [Google Scholar] [CrossRef]
- Moula, Z.; Aithal, S.; Karkou, V.; Powell, J. A systematic review of child-focused outcomes and assessments of arts therapies delivered in primary mainstream schools. J. Child. Youth Serv. Rev. 2020, 112, 104928. [Google Scholar] [CrossRef]
- Omylinska-Thurston, J.; Karkou, V.; Parsons, A.; Nair, K.; Starkey, J.; Dubrow-Marshall, L.; Thurston, S.; Dudley-Swarbrick, I.; Sharma, S. Arts for the Blues: The development of a new evidence-based creative group psychotherapy for depression. Couns. Psychother. Res. 2021, 21, 3. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Hervey, L.W. Artistic Inquiry in Dance/Movement Therapy: Creative Research Alternatives; Thomas: Springfield, IL, USA, 2006. [Google Scholar]
- McNiff, S. Art-Based Research; Jessica Kingsley Publishers: London, UK, 2009. [Google Scholar]
- McDonald, A.; Holttum, S.; Drey, N. Primary-school-based art therapy: Exploratory study of changes in children’s social, emotional and mental health. Int. J. Art Ther. 2019, 24, 125–138. [Google Scholar] [CrossRef]
- Jones, P. The Arts Therapies: A Revolution in Healthcare; Routledge Publications: New York, NY, USA, 2005. [Google Scholar]
- Sutherland, J.; Waldman, G.; Collins, C. Art therapy connection: Encouraging troubled youth to stay in school and succeed. J. Am. Art Ther. Assoc. 2010, 27, 69–74. [Google Scholar] [CrossRef]
- Harpazi, S.; Regev, D.; Snir, S.; Raubach-Kaspy, R. Perceptions of Art Therapy in Adolescent Clients Treated Within the School System. Front. Psychol. 2020, 11, 518304. [Google Scholar] [CrossRef]
- Maslow, A.H. Towards a Psychology of Being; D. Van Nostrand Company: New York, NY, USA, 1962. [Google Scholar]
- May, R. The Courage to Create; WW Norton & Company: New York, NY, USA, 1994. [Google Scholar]
- Zimmerman, M.A. Empowerment theory: Psychological, organizational, and community levels of analysis. In Handbook of Community Psychology; Rappaport, J., Seidman, E., Eds.; Springer: New York, NY, USA, 2000; pp. 43–63. [Google Scholar] [CrossRef]
- Seligman, M.E.; Csikszentmihalyi, M. Positive Psychology: An Introduction; Springer: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. 2008, 49, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Regev, D.; Green-Orlovish, A.; Shir, S. Art therapy in schools: The therapist’s perspective. Arts Psychother. 2015, 45, 47–55. [Google Scholar] [CrossRef]
- Danieli, Y.; Snir, S.; Regev, D.; Adoni-Kroyanker, M. Suitability of the art therapy room and changes in outcome measures in the education system. Int. J. Art Ther. 2019, 24, 68–75. [Google Scholar] [CrossRef]
- Lohan, M.; Aventin, Á.; Maguire, L.; Curran, R.; McDowell, C.; Agus, A.; O’Halloran, P. Recruitment, Randomisation, Allocation and Retention. NIHR J. Public Health Res. 2017. Available online: https://www.ncbi.nlm.nih.gov/books/NBK425194/ (accessed on 1 June 2022).
- Parsons, A.; Omylinska-Thurston, J.; Karkou, V.; Harlow, J.; Haslam, S.; Hobson, J.; Nair, K.; Dubrow-Marshall, L.; Thurston, S.; Griffin, J. Arts for the Blues—A new creative psychological therapy for depression. Br. J. Guid. Couns. 2019, 48, 1633459. [Google Scholar] [CrossRef]
- Haslam, S.; Parsons, A.; Omylinska-Thurston, J.; Nair, K.; Harlow, J.; Lewis, J.; Thurston, S.; Griffin, J.; Dubrow-Marshall, L.; Karkou, V. Arts for the Blues—A new creative psychological therapy for depression: A pilot workshop report. Perspect. Public Health 2019, 139, 137–146. [Google Scholar] [CrossRef]
- Atkinson, P.; Coffey, A.; Delamont, S. Key Themes in Qualitative Research: Continuities and Changes; AltaMira Press: New York, NY, USA, 2003. [Google Scholar]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0; The Cochrane Collaboration, 2011. Available online: www.handbook.cochrane.org(accessed on 1 June 2022).




{kind=link}
{kind=link}
{kind=link}
| Type of Arts Therapies | No. of Children Recruited | No. of Children Completed | Dropouts (Group) | Dropout Reason |
|---|---|---|---|---|
| Art therapy | 16 | 14 | 2 (control group) | 1 hospitalisation 1 left school |
| Dramatherapy | 16 | 14 | 2 (1 from each group) | 2 did not want to keep missing the PE classes |
| Dance movement therapy | 16 | 16 | N/A | N/A |
| Music therapy | 14 | 12 | 2 (intervention group) | 1 left school 1 did not want to keep missing the assemblies |
| Total | 62 | 56 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moula, Z.; Powell, J.; Karkou, V. Qualitative and Arts-Based Evidence from Children Participating in a Pilot Randomised Controlled Study of School-Based Arts Therapies. Children 2022, 9, 890. https://doi.org/10.3390/children9060890
Moula Z, Powell J, Karkou V. Qualitative and Arts-Based Evidence from Children Participating in a Pilot Randomised Controlled Study of School-Based Arts Therapies. Children. 2022; 9(6):890. https://doi.org/10.3390/children9060890
Chicago/Turabian StyleMoula, Zoe, Joanne Powell, and Vicky Karkou. 2022. "Qualitative and Arts-Based Evidence from Children Participating in a Pilot Randomised Controlled Study of School-Based Arts Therapies" Children 9, no. 6: 890. https://doi.org/10.3390/children9060890