
The Predictive Value of Radiographs and the Pirani Score for Later Additional Surgery in Ponseti-Treated Idiopathic Clubfeet, an Observational Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
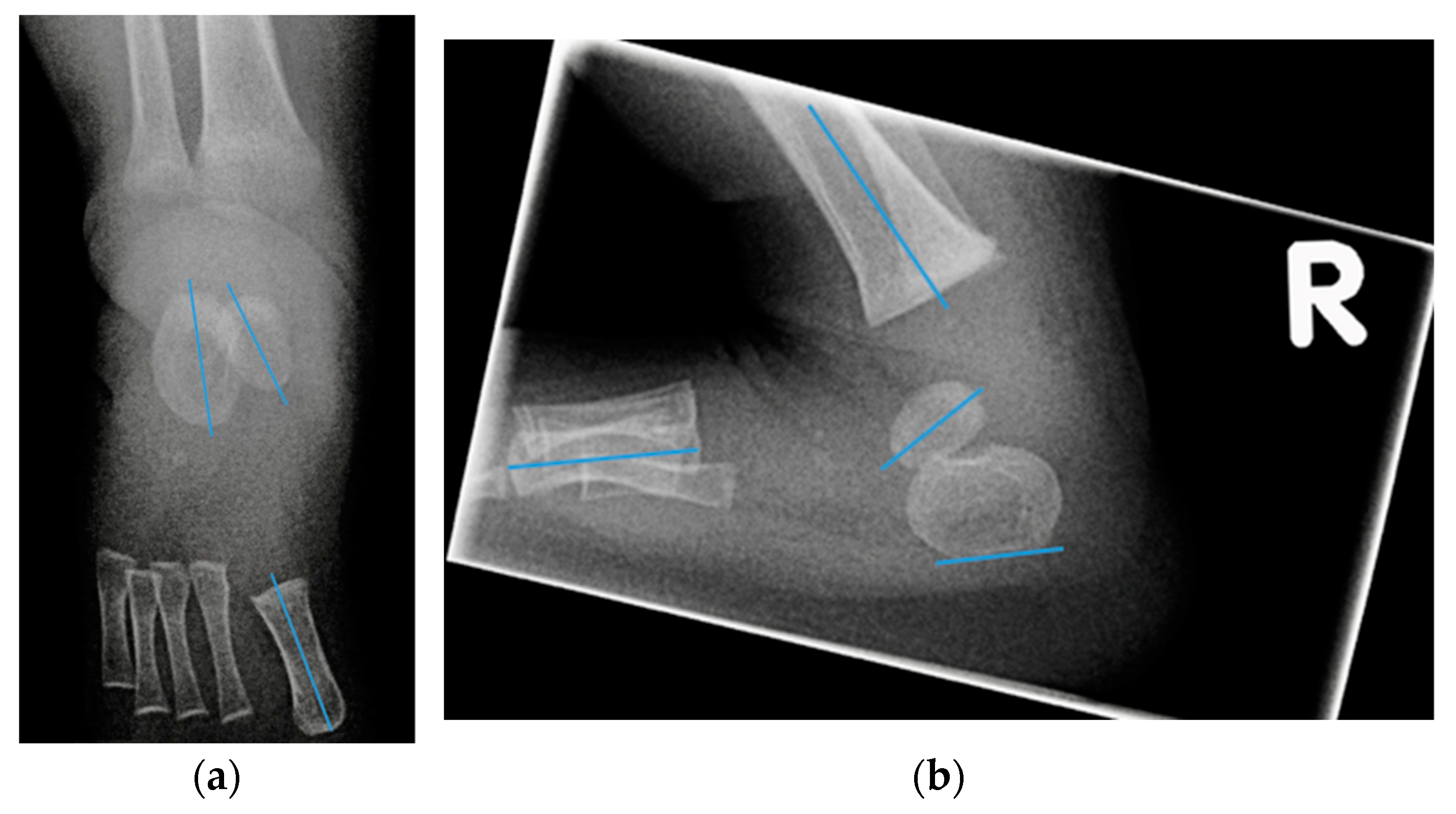
2.2. Radiographs
- Talocalcaneal angle (AP talocalcaneal): the angle between the long axes of the talus and calcaneus. This measurement describes the eversion of the calcaneus under the talus. A small value indicates hindfoot varus [9].
- Talo first metatarsal angle (AP talo 1st MT): the angle between the long axis of the talus and 1st metatarsal. This measurement describes forefoot abduction or adduction [9].
- Lateral tibial calcaneal angle (lat tibiocalcaneal): the angle between longitudinal axis of the tibia and the plantar aspect of the calcaneus. This measurement describes equinus deformity.
- Lateral talo first metatarsal angle (lat talo 1st MT): the angle between the long axis of the talus and the first metatarsal. This measurement describes the presence of cavus deformity.
- Lateral calcaneal 1st metatarsal angle (lat calcaneal 1st MT): the angle between the plantar aspect of the calcaneus and the long axis of the first metatarsal. This measurement also describes the presence of cavus deformity.
- Foot dorsiflexion between the tibia and a radiolucent wooden board in maximum dorsiflexion (lat foot dorsiflexion). This measurement describes equinus.
2.3. Need for Additional Surgery
2.4. Parent Satisfaction
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Need for Additional Surgery
3.3. Radiographs
3.4. Parent Satisfaction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponseti, I.V. Congenital Clubfoot: Fundamentals of Treatment; Oxford University Press: Oxford, UK, 1996; ISBN 0192627651. [Google Scholar]
- Gelfer, Y.; Wientroub, S.; Hughes, K.; Fontalis, A.; Eastwood, D.M. Congenital Talipes Equinovarus Ponseti Method. Bone Jt. J. 2019, 101-B, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.M.; Sangiorgio, S.N.; Ebramzadeh, E.; Zionts, L.E. Relapse Rates in Patients with Clubfoot Treated Using the Ponseti Method Increase with Time: A Systematic Review. JBJS Rev. 2019, 7, e6. [Google Scholar] [CrossRef] [PubMed]
- Van Schelven, H.; Moerman, S.; Van Der Steen, M.; Besselaar, A.T.; Greve, C. Prognostic Factors for Recurrent Idiopathic Clubfoot Deformity: A Systematic Literature Review and Meta-Analysis. Acta Orthop. 2021, 93, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Pirani, S.; Outerbridge, H.; Moran, M.; Sawatski, B. A Method of Evaluating the Virgin Clubfoot with Substantial Interobserver Reliability; POSNA: Miami, FL, USA, 1995. [Google Scholar]
- Dyer, P.J. The Role of the Pirani Scoring System in the Management of Club Foot by the Ponseti Method. J. Bone Jt. Surg. Br. Vol. 2006, 88, 1082–1084. [Google Scholar] [CrossRef]
- Haft, G.F.; Walker, C.G.; Crawford, H.A. Early Clubfoot Recurrence after Use of the Ponseti Method in a New Zealand Population. J. Bone Jt. Surg. Ser. A 2007, 89, 487–493. [Google Scholar] [CrossRef] [Green Version]
- Zhao, D.; Li, H.; Zhao, L.; Kuo, K.N.; Yang, X.; Wu, Z.; Liu, J.; Zhu, J. Prognosticating Factors of Relapse in Clubfoot Management by Ponseti Method. J. Pediatr. Orthop. 2018, 38, 514–520. [Google Scholar] [CrossRef]
- Simons, G.W. Analytical Radiography of Club Feet. J. Bone Jt. Surg. 1977, 59, 485–489. [Google Scholar] [CrossRef]
- Kang, S.; Park, S.S. Lateral Tibiocalcaneal Angle as a Determinant for Percutaneous Achilles Tenotomy for Idiopathic Clubfeet. J. Bone Jt. Surg. Am. Vol. 2014, 97, 1246–1254. [Google Scholar] [CrossRef]
- O’Halloran, C.P.; Halanski, M.A.; Nemeth, B.A.; Zimmermann, C.C.; Noonan, K.J. Can Radiographs Predict Outcome in Patients with Idiopathic Clubfeet Treated with the Ponseti Method? J. Pediatr. Orthop. 2015, 35, 734–738. [Google Scholar] [CrossRef]
- Richards, B.S.; Faulks, S.; Razi, O.; Moualeu, A.; Jo, C.-H. Nonoperatively Corrected Clubfoot at Age 2 Years. J. Bone Jt. Surg. 2017, 99, 155–160. [Google Scholar] [CrossRef]
- Besselaar, A.T.; Sakkers, R.J.B.; Schuppers, H.A.; Witbreuk, M.M.E.H.; Zeegers, E.V.C.M.; Visser, J.D.; Boekestijn, R.A.; Margés, S.D.; Van der Steen, M.C.; Burger, K.N.J. Guideline on the Diagnosis and Treatment of Primary Idiopathic Clubfoot. Acta Orthop. 2017, 88, 305–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simons, G.W. Complete Subtalar Release in Clubfeet. J. Bone Jt. Surg. 1985, 7, 1056–1065. [Google Scholar] [CrossRef]
- Simons, G.W. A Standardized Method for the Radiographic Evaluation of Clubfeet. Clin. Orthop. Relat. Res. 1978, 135, 107–118. [Google Scholar] [CrossRef]
- Shabtai, L.; Hemo, Y.; Yavor, A.; Gigi, R.; Wientroub, S.; Segev, E. Radiographic Indicators of Surgery and Functional Outcome in Ponseti-Treated Clubfeet. Foot Ankle Int. 2015, 37, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Bhatia, M.; Nair, N.S. Talo-Calcaneal Relationship in Clubfoot. J. Pediatr. Orthop. 2001, 21, 60–64. [Google Scholar] [CrossRef]
- Roye, B.D.; Vitale, M.G.; Gelijns, A.C.; Roye, D.P. Patient-Based Outcomes after Clubfoot Surgery. J. Pediatr. Orthop. 2001, 21, 42–49. [Google Scholar] [CrossRef]
- Wijnen, W.; Witlox, A.; Mesters, I.; Bosma, H.; vsn Rhijn, L.; Staal, H. Patient Reported Outcom Measurement (PROM’s) for Children (of Paediatric Patients) with Clubfeet. Ned. Tijdschr. Orthop. 2017, 24, 111–113. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Liu, Y.; Li, Y.; Yuan, Z.; Xu, H.; Canavese, F. Early Radiographic Changes in the Lateral Talocalcaneal Angle Following Achilles Tenotomy in Children With Idiopathic Clubfoot. Foot Ankle Int. 2020, 41, 350–355. [Google Scholar] [CrossRef]
- Zimmerman, C.C.; Nemeth, B.A.; Noonan, K.J.; Vanderbilt, T.P.; Winston, M.J.; O’Halloran, C.P.; Sund, S.A.; Hetzel, S.J.; Halanski, M.A. Reliability of Radiographic Measures in Infants with Clubfoot Treated with the Ponseti Method. J. Child. Orthop. 2015, 9, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Pavone, V.; Vescio, A.; Caldaci, A.; Culmone, A.; Sapienza, M.; Rabito, M.; Canavese, F.; Testa, G. Sport Ability during Walking Age in Clubfoot-Affected Children after Ponseti Method: A Case-Series Study. Children 2021, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Radler, C.; Mindler, G.T. Treatment of Severe Recurrent Clubfoot. Foot Ankle Clin. 2015, 20, 563–586. [Google Scholar] [CrossRef] [PubMed]
- Stouten, J.H.; Besselaar, A.T.; Van Der Steen, M.C. Identification and Treatment of Residual and Relapsed Idiopathic Clubfoot in 88 Children. Acta Orthop. 2018, 89, 448–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sriharsha, Y.; Balaji, G.; Bharathi, D.; Patro, D.K. Do the Clinical Scores (Pirani and Dimeglio Scores) Correlate with the Radiological Parameters in Idiopathic Club Foot in Infants? A Cross-Sectional Study. J. Pediatr. Orthop. Part B 2021, 30, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Zionts, L.E.; Ebramzadeh, E.; Morgan, R.D.; Sangiorgio, S.N. Sixty Years on: Ponseti Method for Clubfoot Treatment Produces High Satisfaction despite Inherent Tendency to Relapse. J. Bone Jt. Surg. Am. Vol. 2018, 100, 721–728. [Google Scholar] [CrossRef]
- Dietz, F.R.; Tyler, M.C.; Leary, K.S.; Damiano, P.C. Evaluation of a Disease-Specific Instrument for Idiopathic Clubfoot Outcome. Clin. Orthop. Relat. Res. 2009, 467, 1256–1262. [Google Scholar] [CrossRef] [Green Version]
- McCahill, J.L.; Stebbins, J.; Harlaar, J.; Prescott, R.; Theologis, T.; Lavy, C. Foot Function during Gait and Parental Perceived Outcome in Older Children with Symptomatic Club Foot Deformity. Bone Jt. Open 2020, 1, 384–391. [Google Scholar] [CrossRef]


{kind=link}
| Children (n = 50) | Clubfoot (n = 72) | |
|---|---|---|
| Female, n (%) | 14 (28%) | |
| Unilateral, n (%) | 28 (56%) | |
| Dimeglio score before first cast, median (IQR) a | 10 (7–12) | |
| Pirani score before first cast | 3.8 (3.4–4.1) | |
| Pirani score before tenotomy b | 1.4 (1.1–1.7) | |
| Pirani score before radiograph c | 0.3 (0.1–0.5) | |
| Initial tenotomy performed, n (%) | 55 (76%) | |
| Age at initial tenotomy, weeks | 8.3 (7.0–9.5) | |
| Age at radiograph, weeks | 14.0 (13.6–14.4) |
| Mean Angle | 95% CI of Mean | ICC Average Measure | |
|---|---|---|---|
| AP talocalcaneal | 16.0 | 13.3–18.7 | 0.80 (0.68–0.88) |
| AP talo 1st MT | 9.7 | 6.8–12.5 | 0.09 (−0.37–0.41) |
| Lat tibiocalcaneal | 59.1 | 55.4–62.8 | 0.99 (0.98–0.99) |
| Lat talocalcaneal | 31.2 | 28.5–33.9 | 0.94 (0.90–0.96) |
| Lat talo 1st MT | −26.9 | −31.3–22.5 | 0.89 (0.80–0.94) |
| Lat calaneal 1st MT | 13.4 | 11.0–15.7 | 0.85 (0.76–0.91) |
| Lat foot dorsiflexion | 45.7 | 41.7–49.7 | 0.99 (0.99–1.00) |
| No Additional Surgery | Additional Surgery | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Excellent (n = 45) | Good (n = 9) Fair (n = 18) | t Test | Univariate Logistic Regression | ||||||
| Mean | SD | Mean | SD | p | B | S.E. | Exp (B) | p | |
| AP talocalcaneal | 16.4 | 11.0 | 15.4 | 12.2 | 0.75 | −0.00 | 0.02 | 1.0 | 0.73 |
| Lat tibiocalcaneal | 54.7 | 12.0 | 66.5 | 18.9 | <0.05 | 0.06 | 0.02 | 1.06 | 0.005 |
| Lat talocalcaneal | 33.6 | 11.3 | 27.1 | 10.5 | <0.05 | −0.06 | 0.03 | 0.95 | 0.025 |
| Lat talo 1st MT | −27.3 | 20.1 | −26.1 | 15.7 | 0.51 | 0.00 | 0.1 | 1.0 | 0.79 |
| Lat calaneal 1st MT | 13.7 | 8.4 | 12.8 | 11.8 | 0.75 | 0.0 | 0.03 | 0.99 | 0.72 |
| Lat foot dorsiflexion | 43.5 | 14.0 | 49.8 | 20.0 | 0.19 | 0.02 | 0.02 | 1.02 | 0.15 |
| Pirani score before the 1st cast | 3.6 | 1.5 | 4.1 | 1.4 | 0.09 | 0.30 | 0.18 | 1.35 | 0.099 |
| Pirani score before tenotomy | 1.0 | 0.6 | 1.9 | 1.2 | <0.05 | 1.27 | 0.50 | 3.56 | 0.011 |
| Pirani score before radiograph | 0.1 | 0.3 | 0.7 | 1.1 | <0.05 | 1.58 | 0.63 | 4.83 | 0.012 |
| Clubfeet Pirani = 0 n = 51 | Clubfeet Pirani > 0 n = 16 | ||
|---|---|---|---|
| Lat talocalcaneal (radiograph) | 32.9 (11.7) | 24.3 (9.2) | p < 0.01 |
| Lat tibiocalcaneal (radiograph) | 55.8 (12.8) | 71.3 (20.5) | p < 0.01 |
| Result excellent | 36 (71%) | 5 (31%) | |
| Result good | 4 (8%) | 4 (25%) | |
| Result fair | 11 (22%) | 7 (44%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moerman, S.; Zijlstra-Koenrades, N.; Reijman, M.; Kempink, D.R.J.; Bessems, J.H.J.M.; de Vos-Jakobs, S. The Predictive Value of Radiographs and the Pirani Score for Later Additional Surgery in Ponseti-Treated Idiopathic Clubfeet, an Observational Cohort Study. Children 2022, 9, 865. https://doi.org/10.3390/children9060865
Moerman S, Zijlstra-Koenrades N, Reijman M, Kempink DRJ, Bessems JHJM, de Vos-Jakobs S. The Predictive Value of Radiographs and the Pirani Score for Later Additional Surgery in Ponseti-Treated Idiopathic Clubfeet, an Observational Cohort Study. Children. 2022; 9(6):865. https://doi.org/10.3390/children9060865
Chicago/Turabian StyleMoerman, Sophie, Nienke Zijlstra-Koenrades, Max Reijman, Dagmar R. J. Kempink, Johannes H. J. M. Bessems, and Suzanne de Vos-Jakobs. 2022. "The Predictive Value of Radiographs and the Pirani Score for Later Additional Surgery in Ponseti-Treated Idiopathic Clubfeet, an Observational Cohort Study" Children 9, no. 6: 865. https://doi.org/10.3390/children9060865