
Oxidative and Inflammatory Markers Are Higher in Full-Term Newborns Suffering Funisitis, and Higher Oxidative Markers Are Associated with Admission


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Samples
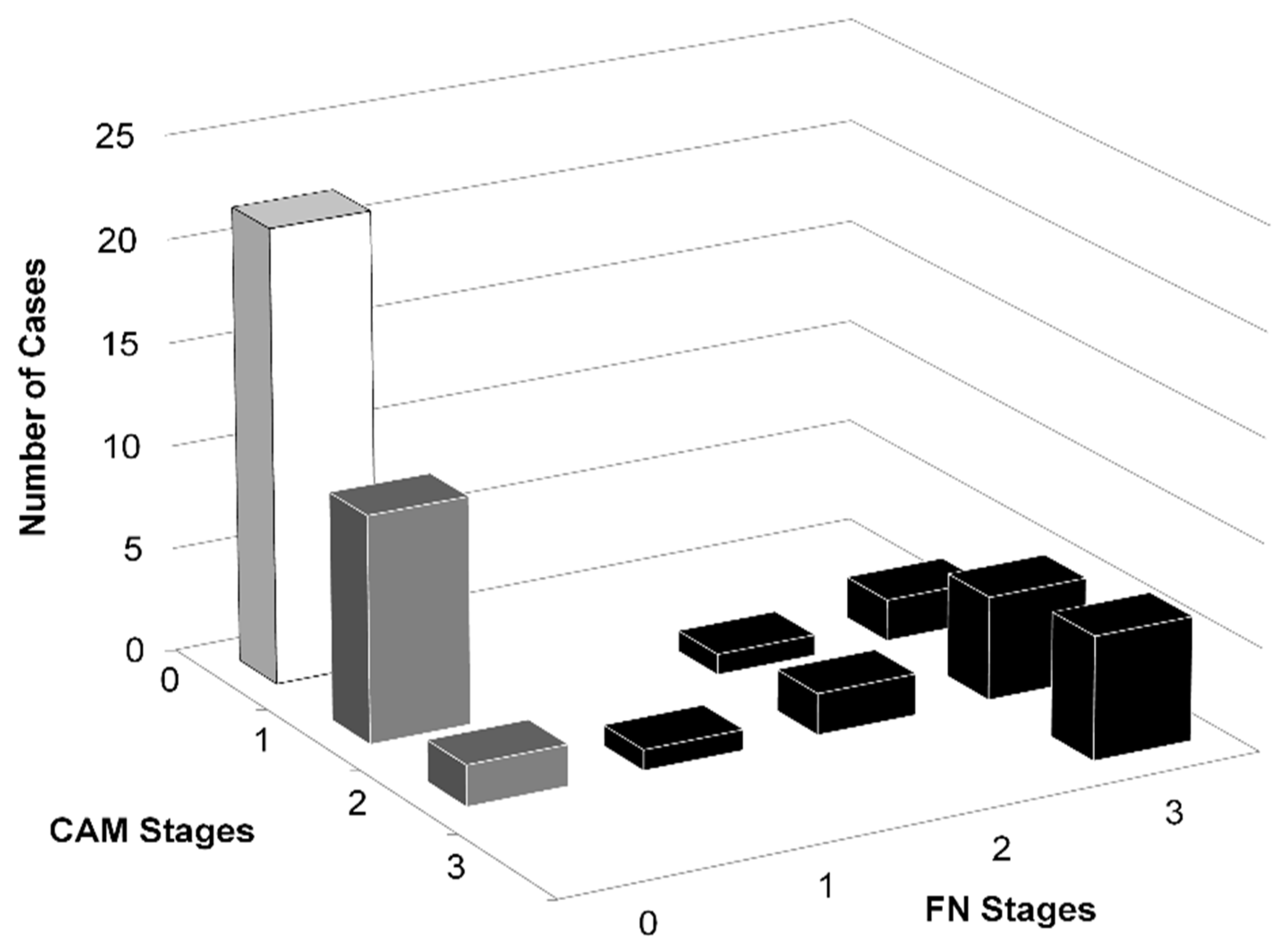
2.3. Histological Classification
2.4. Methods
2.4.1. Serum Total Hydroperoxide (TH) Measurement
2.4.2. Serum Biological Antioxidative Potential (BAP) Measurement
2.4.3. Calculation of the Serum Oxidative Stress Index (OSI)
2.4.4. Serum Total NO Concentration Measurement
2.4.5. Serum Cytokines Measurement
2.4.6. Serum C5a Measurement
2.5. Statistical Analysis
3. Results
3.1. Histological Classification
3.2. Population Studied
3.3. Characteristics and Clinical Courses of the Patients Studied
3.4. Comparison among Funisitis, Chorioamnionitis, and Control Groups
3.4.1. Oxidative Markers
3.4.2. Cytokines and C5a
3.4.3. Correlations
3.5. Comparison between Infants Admitted and Non-Admitted to the NICU
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Redline, R.W. Inflammatory Responses in the Placenta and Umbilical Cord. Semin. Fetal Neonatal Med. 2006, 11, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Espinoza, J.; Chaiworapongsa, T.; Kalache, K. Infection and Prematurity and the Role of Preventive Strategies. Semin Neonatol 2002, 7, 259–274. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Andrews, W.W.; Hauth, J.C. Choriodecidual Infection and Preterm Birth. Nutr. Rev. 2002, 60, S19–S25. [Google Scholar] [CrossRef] [PubMed]
- Blanc, W.A. Pathology of the Placenta, Membranes, and Umbilical Cord in Bacterial, Fungal, and Viral Infections in Man. Perinat. Dis. 1981, 22, 67–132. [Google Scholar]
- Silveira, R.C.; Procianoy, R.S. Evaluation of Interleukin-6, Tumour Necrosis Factor-Alpha and Interleukin-1beta for Early Diagnosis of Neonatal Sepsis. Acta Paediatr. 1999, 88, 647–650. [Google Scholar] [CrossRef]
- Witt, A.; Berger, A.; Gruber, C.J.; Petricevic, L.; Apfalter, P.; Husslein, P. IL-8 Concentrations in Maternal Serum, Amniotic Fluid and Cord Blood in Relation to Different Pathogens within the Amniotic Cavity. J. Perinat. Med. 2005, 33, 22–26. [Google Scholar] [CrossRef]
- Shimoya, K.; Matsuzaki, N.; Taniguchi, T.; Jo, T.; Saji, F.; Kitajima, H.; Fujimura, M.; Nakayama, M.; Tanizawa, O. Interleukin-8 in Cord Sera: A Sensitive and Specific Marker for the Detection of Preterm Chorioamnionitis. J. Infect. Dis. 1992, 165, 957–960. [Google Scholar] [CrossRef]
- Yoon, B.H.; Romero, R.; Jun, J.K.; Park, K.H.; Park, J.D.; Ghezzi, F.; Kim, B.I. Amniotic Fluid Cytokines (Interleukin-6, Tumor Necrosis Factor-Alpha, Interleukin-1 Beta, and Interleukin-8) and the Risk for the Development of Bronchopulmonary Dysplasia. Am. J. Obstet. Gynecol. 1997, 177, 825–830. [Google Scholar] [CrossRef]
- Yoon, B.H.; Romero, R.; Yang, S.H.; Jun, J.K.; Kim, I.O.; Choi, J.H.; Syn, H.C. Interleukin-6 Concentrations in Umbilical Cord Plasma Are Elevated in Neonates with White Matter Lesions Associated with Periventricular Leukomalacia. Am. J. Obstet. Gynecol. 1996, 174, 1433–1440. [Google Scholar] [CrossRef]
- Døllner, H.; Vatten, L.; Halgunset, J.; Rahimipoor, S.; Austgulen, R. Histologic Chorioamnionitis and Umbilical Serum Levels of Pro-Inflammatory Cytokines and Cytokine Inhibitors. BJOG 2002, 109, 534–539. [Google Scholar] [CrossRef]
- Daoud, G.A.; Suzuki, Y.; Yamamoto, T.; Suzumori, K.; Togari, H. Reduced Nitric Oxide in Amniotic Fluid of Patients with Chorioamnionitis. Fetal Diagn. Ther. 2006, 21, 77–80. [Google Scholar] [CrossRef]
- Chan, C.J.; Summers, K.L.; Chan, N.G.; Hardy, D.B.; Richardson, B.S. Cytokines in Umbilical Cord Blood and the Impact of Labor Events in Low-Risk Term Pregnancies. Early Hum. Dev. 2013, 89, 1005–1010. [Google Scholar] [CrossRef]
- Kasztelewicz, B.; Piotrowska, E.; Tołłoczko, J.; Borszewska-Kornacka, M.K.; Gregorek, H.; Dzierżanowska-Fangrat, K. Assessment of Interleukin-17A, C5a and RANTES for Early Diagnosis of Neonatal Sepsis—A Preliminary Study. Cent. Eur. J. Immunol. 2016, 41, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Moore, T.A.; Ahmad, I.M.; Zimmerman, M.C. Oxidative Stress and Preterm Birth: An Integrative Review. Biol. Res. Nurs. 2018, 20, 497–512. [Google Scholar] [CrossRef]
- Henderson, R.; Kim, S.; Lee, E. Use of Melatonin as Adjunctive Therapy in Neonatal Sepsis: A Systematic Review and Meta-Analysis. Complement. Ther. Med. 2018, 39, 131–136. [Google Scholar] [CrossRef]
- Kato, S.; Hussein, M.H.; Kakita, H.; Goto, T.; Daoud, G.A.; Kato, T.; Sugiura, T.; Nobata, M.; Nakajima, Y.; Endo, T.; et al. Edaravone, a Novel Free Radical Scavenger, Reduces High-Mobility Group Box 1 and Prolongs Survival in a Neonatal Sepsis Model. Shock 2009, 32, 586–592. [Google Scholar] [CrossRef]
- Carvalho, C.G.; Procianoy, R.S.; Neto, E.C.; Silveira, R.C. Preterm Neonates with Respiratory Distress Syndrome: Ventilator-Induced Lung Injury and Oxidative Stress. J. Immunol. Res. 2018, 2018, 6963754. [Google Scholar] [CrossRef] [Green Version]
- Sanodze, N.; Uberi, N.; Uberi, E.; Kulumbegov, B. Parameters of Oxidative Metabolism in Neonates Suffering from Sepsis and Anemia. Georgian Med. News 2006, 140, 65–67. [Google Scholar]
- Kakita, H.; Hussein, M.H.; Daoud, G.A.; Kato, T.; Murai, H.; Sugiura, T.; Mizuno, K.; Yamada, Y.; Ito, T.; Fukuda, S.; et al. Total Hydroperoxide and Biological Antioxidant Potentials in a Neonatal Sepsis Model. Pediatr. Res. 2006, 60, 675–679. [Google Scholar] [CrossRef] [Green Version]
- Dohi, K.; Satoh, K.; Ohtaki, H.; Shioda, S.; Miyake, Y.; Shindo, M.; Aruga, T. Elevated Plasma Levels of Bilirubin in Patients with Neurotrauma Reflect Its Pathophysiological Role in Free Radical Scavenging. In Vivo 2005, 19, 855–860. [Google Scholar]
- Kakita, H.; Hussein, M.H.; Yamada, Y.; Henmi, H.; Kato, S.; Kobayashi, S.; Ito, T.; Kato, I.; Fukuda, S.; Suzuki, S.; et al. High Postnatal Oxidative Stress in Neonatal Cystic Periventricular Leukomalacia. Brain Dev. 2009, 31, 641–648. [Google Scholar] [CrossRef]
- Hussein, M.H.; Daoud, G.A.; Kakita, H.; Kato, S.; Goto, T.; Kamei, M.; Goto, K.; Nobata, M.; Ozaki, Y.; Ito, T.; et al. High Cerebrospinal Fluid Antioxidants and Interleukin 8 Are Protective of Hypoxic Brain Damage in Newborns. Free Radic. Res. 2010, 44, 422–429. [Google Scholar] [CrossRef]
- Buonocore, G.; Perrone, S.; Longini, M.; Terzuoli, L.; Bracci, R. Total Hydroperoxide and Advanced Oxidation Protein Products in Preterm Hypoxic Babies. Pediatr. Res. 2000, 47, 221–224. [Google Scholar] [CrossRef] [Green Version]
- Morgan, E.; Varro, R.; Sepulveda, H.; Ember, J.A.; Apgar, J.; Wilson, J.; Lowe, L.; Chen, R.; Shivraj, L.; Agadir, A.; et al. Cytometric Bead Array: A Multiplexed Assay Platform with Applications in Various Areas of Biology. Clin. Immunol. 2004, 110, 252–266. [Google Scholar] [CrossRef]
- Zilow, E.P.; Hauck, W.; Linderkamp, O.; Zilow, G. Alternative Pathway Activation of the Complement System in Preterm Infants with Early Onset Infection. Pediatr. Res. 1997, 41, 334–339. [Google Scholar] [CrossRef]
- Friel, J.K.; Friesen, R.W.; Harding, S.V.; Roberts, L.J. Evidence of Oxidative Stress in Full-Term Healthy Infants. Pediatr. Res. 2004, 56, 878–882. [Google Scholar] [CrossRef] [Green Version]
- Victor, V.M.; Rocha, M.; De la Fuente, M. Immune Cells: Free Radicals and Antioxidants in Sepsis. Int. Immunopharmacol. 2004, 4, 327–347. [Google Scholar] [CrossRef]
- Saugstad, O.D. Mechanisms of Tissue Injury by Oxygen Radicals: Implications for Neonatal Disease. Acta Paediatr. 1996, 85, 1–4. [Google Scholar] [CrossRef]
- Ohman, L.; Tullus, K.; Katouli, M.; Burman, L.G.; Stendahl, O. Correlation between Susceptibility of Infants to Infections and Interaction with Neutrophils of Escherichia Coli Strains Causing Neonatal and Infantile Septicemia. J. Infect. Dis. 1995, 171, 128–133. [Google Scholar] [CrossRef]
- Andrades, M.; Ritter, C.; Moreira, J.C.F.; Dal-Pizzol, F. Oxidative Parameters Differences during Non-Lethal and Lethal Sepsis Development. J. Surg. Res. 2005, 125, 68–72. [Google Scholar] [CrossRef]
- Bavunoglu, I.; Genc, H.; Konukoglu, D.; Cicekci, H.; Sozer, V.; Gelisgen, R.; Uzun, H. Oxidative Stress Parameters and Inflammatory and Immune Mediators as Markers of the Severity of Sepsis. J. Infect. Dev. Ctries. 2016, 10, 1045–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, B.P. Cellular Defenses against Damage from Reactive Oxygen Species. Physiol. Rev. 1994, 74, 139–162. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, K.; Basu, S.; Das, B.K.; Bhatia, B.D. Lipid Peroxidation and Antioxidants in Neonatal Septicemia. J. Trop. Pediatr. 2006, 52, 372–375. [Google Scholar] [CrossRef] [Green Version]
- Hamed, S.A.; Hamed, E.A.; Abdella, M.M. Septic Encephalopathy: Relationship to Serum and Cerebrospinal Fluid Levels of Adhesion Molecules, Lipid Peroxides and S-100B Protein. Neuropediatrics 2009, 40, 66–72. [Google Scholar] [CrossRef]
- Huet, O.; Obata, R.; Aubron, C.; Spraul-Davit, A.; Charpentier, J.; Laplace, C.; Nguyen-Khoa, T.; Conti, M.; Vicaut, E.; Mira, J.-P.; et al. Plasma-Induced Endothelial Oxidative Stress Is Related to the Severity of Septic Shock. Crit. Care Med. 2007, 35, 821–826. [Google Scholar] [CrossRef]
- Dinkova-Kostova, A.T.; Holtzclaw, W.D.; Cole, R.N.; Itoh, K.; Wakabayashi, N.; Katoh, Y.; Yamamoto, M.; Talalay, P. Direct Evidence That Sulfhydryl Groups of Keap1 Are the Sensors Regulating Induction of Phase 2 Enzymes That Protect against Carcinogens and Oxidants. Proc. Natl. Acad. Sci. USA 2002, 99, 11908–11913. [Google Scholar] [CrossRef] [Green Version]
- Poggi, C.; Dani, C. Sepsis and Oxidative Stress in the Newborn: From Pathogenesis to Novel Therapeutic Targets. Oxid. Med. Cell. Longev. 2018, 2018, 9390140. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Item | Control n = 22 | Chorioamnionitis n = 13 | Funisitis n = 17 |
|---|---|---|---|
| Female gender, n (%) | 12 (55.5%) | 7 (53.8%) | 5 (29.4%) |
| Gestational age (weeks) | 38.8 (37–41) | 40 (38–42) | 39.8 (37–41) |
| Birth (body) weight in grams, median (range) | 3026 (2466–3622) | 3142 (2514–3770) | 3151 (2524–3682) |
| Mode of delivery | |||
| Vaginal, n (%) | 11 (50.0%) | 8 (61.5%) | 8 (47.1%) |
| Cesarean section a, n (%) | 11 (50.0%) | 5 (38.5%) | 9 (52.9%) |
| Emergency cesarean section, n (%) | 0 (0.0%) | 0 (0.0%) | 4 (23.5%) |
| PROM b, n (%) | 2 (9.1%) | 2 (15.4%) | 4 (23.5%) |
| Maternal infection c, n (%) | 0 (0%) | 1 (7.7%) | 6 (35.3%) ‡ |
| Admission to the NICU, n (%) | 2 (9.1%) | 3 (23.1%) | 8 (47.1%) ‡ |
| Apgar score (1 min), median (range) | 8.3 (7–10) | 8.2 (7–9) | 7.5 (1–9) |
| Apgar score (5 min), median (range) | 9.0 (8–10) | 8.7 (8–10) | 8.7 (8–9) |
| Newborn CRP d (mg/dL), mean ± SEM | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.56 ± 0.32 † |
| Item | Control n = 22 | Chorioamnionitis n = 13 | Funisitis n = 17 |
|---|---|---|---|
| Indications for cesarean section, n | 11 | 5 | 9 |
| Previous cesarean section | 7 | 1 | 0 |
| Malposition and malpresentation | 3 | 1 | 2 |
| Fetal distress or non-assuring fetal status | 1 | 1 | 2 |
| Polyhydramnios | 1 | 1 | 0 |
| Postdated pregnancy | 0 | 1 | 1 |
| Contracted pelvis and birth canal | 0 | 2 | 0 |
| Cephalopelvic disproportion | 0 | 1 | 2 |
| Maternal asthma | 0 | 1 | 0 |
| Uterine myoma | 0 | 0 | 1 |
| Pregnancy-induced hypertension | 0 | 0 | 1 |
| Intra-uterine infection | 0 | 0 | 3 |
| Indication for admission to the NICU a, n | 2 | 4 | 11 |
| TTN b | 1 | 0 | 2 |
| MAS c | 0 | 2 | 4 |
| Apnea | 1 | 0 | 0 |
| Infection/sepsis | 0 | 1 | 5 |
| Hyperbilirubinemia | 0 | 1 | 0 |
| Mediators | Control | Chorioamnionitis | Funisitis | p Value |
|---|---|---|---|---|
| n = 22 | n = 13 | n = 17 | ||
| IL-10 (pg/mL) | 2.49 ± 1.48 | 2.05 ± 1.38 | 3.22 ± 1.66 | NS a |
| IFN-γ (pg/mL) | 0.89 ± 0.158 | 1.24 ± 0.28 | 0.765 ± 0.199 | NS |
| TNFα (pg/mL) | 0.426 ± 0.139 | 0.394 ± 0.087 | 0.410 ± 106 | NS |
| BAP (μmol/L) | 2480 ± 183 | 2518 ± 171 | 2837 ± 112 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamei, M.; Hussein, M.H.; Hattori, A.; Saleh, M.; Kakita, H.; Abdel-Hamid Daoud, G.; Ishiguro, A.; Namba, F.; Yazaki, M.; Goto, H.; et al. Oxidative and Inflammatory Markers Are Higher in Full-Term Newborns Suffering Funisitis, and Higher Oxidative Markers Are Associated with Admission. Children 2022, 9, 702. https://doi.org/10.3390/children9050702
Kamei M, Hussein MH, Hattori A, Saleh M, Kakita H, Abdel-Hamid Daoud G, Ishiguro A, Namba F, Yazaki M, Goto H, et al. Oxidative and Inflammatory Markers Are Higher in Full-Term Newborns Suffering Funisitis, and Higher Oxidative Markers Are Associated with Admission. Children. 2022; 9(5):702. https://doi.org/10.3390/children9050702
Chicago/Turabian StyleKamei, Michi, Mohamed Hamed Hussein, Ayako Hattori, Marwa Saleh, Hiroki Kakita, Ghada Abdel-Hamid Daoud, Akio Ishiguro, Fumihiko Namba, Makoto Yazaki, Haruo Goto, and et al. 2022. "Oxidative and Inflammatory Markers Are Higher in Full-Term Newborns Suffering Funisitis, and Higher Oxidative Markers Are Associated with Admission" Children 9, no. 5: 702. https://doi.org/10.3390/children9050702