
The Efficacy of CPAP in Neonates with Meconium Aspiration Syndrome: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Registration
2.2. Search Methods
2.3. Selection of Studies
2.4. Outcomes
2.5. Data Extraction
2.6. Bias Risk Assessment
2.7. Statistical Analysis
3. Results
3.1. Selection of RCTs
3.2. Characteristics of Included RCTs
3.3. Risk of Bias in the Included RCTs
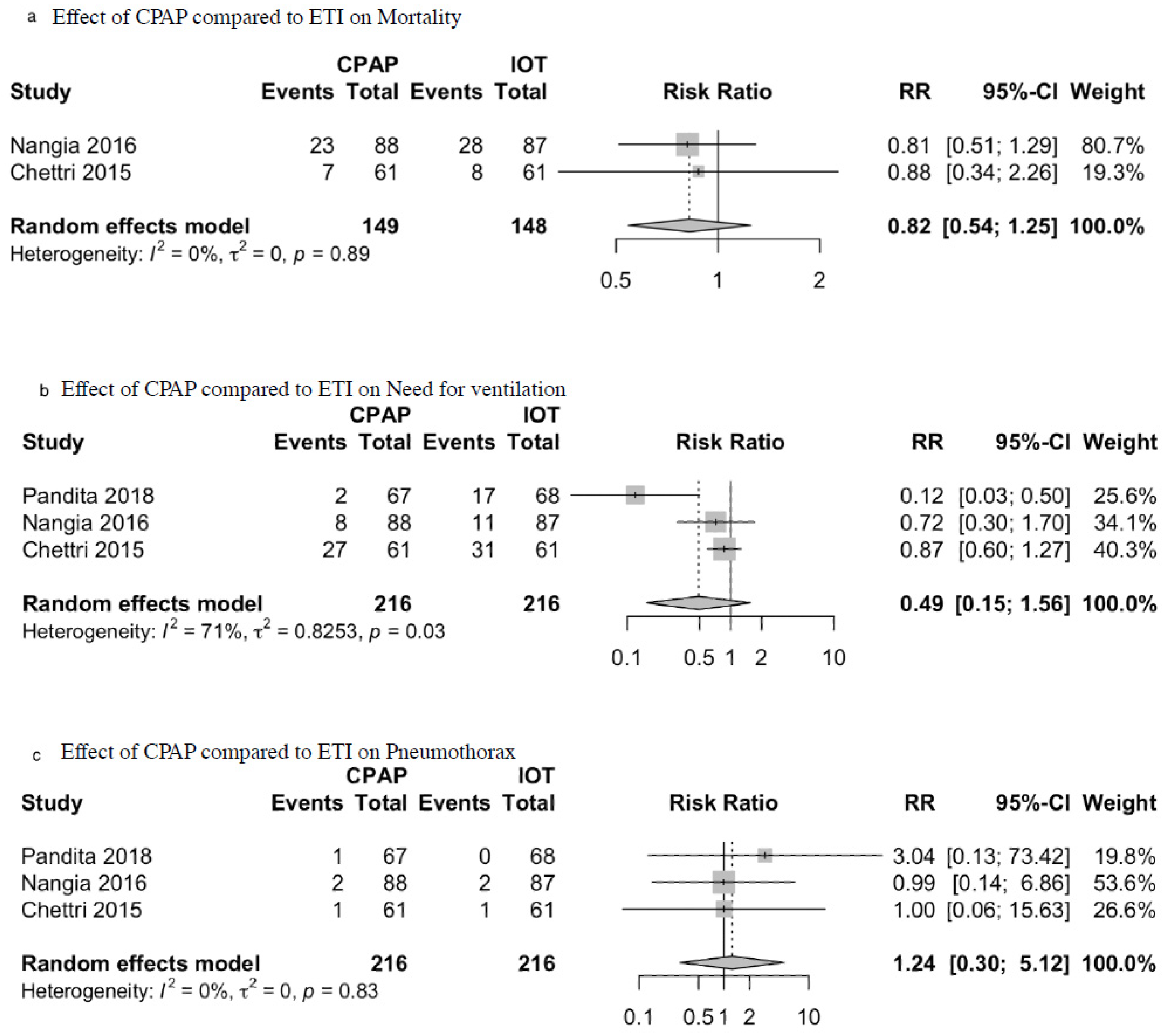
3.4. Effect of CPAP on Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vijayalakshmi, P.; Venugopal, S.; Chandrashekar, B.; Veeresh, S.M. A Prospective Study of Meconium Aspiration Syndrome in Newborns in a District Hospital in Southern India. J. Evol. Med. Dent. Sci. 2015, 4, 8489–8494. [Google Scholar] [CrossRef]
- Santhalingam, T.; Ali, K.; Greenough, A. Outcomes of infants born through meconium stained amniotic fluid (MSAF) according to grade of meconium. Br. Assoc. Perinat. Med. 2017, 102, A186–A187. [Google Scholar] [CrossRef]
- Vidyasagar, D. The management of a neonate born with meconium stained amniotic fluid. J. Perinat. Med. 2013, 41, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Mathew, J.L. Endotracheal Suctioning for Nonvigorous Neonates Born Through Meconium Stained Amniotic Fluid. Indian Pediatr. 2015, 52, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Pohunek, P.; Cerny, M. The difficulty to extubate newborns in the neonatal intensive care unit. Pediatr. Pulmonol. 2017, 52, S79–S81. [Google Scholar]
- Upadhyay, A.; Deorari, A.K. Continuous positive airway pressure—A gentler approach to ventilation. Indian Pediatr. 2004, 41, 459–469. [Google Scholar] [PubMed]
- Flannery, D.; O’Donnell, E.; Kornhauser, M.; Dysart, K.; Greenspan, J.; Aghai, Z.H. Continuous Positive Airway Pressure versus Mechanical Ventilation on the First Day of Life in Very Low-Birth-Weight Infants. Am. J. Perinatol. 2016, 33, 939–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chettri, S.; Adhisivam, B.; Bhat, B.V. Endotracheal Suction for Nonvigorous Neonates Born through Meconium Stained Am-niotic Fluid: A Randomized Controlled Trial. J. Pediatr. 2015, 166, 1208–1213.e1. [Google Scholar] [CrossRef] [PubMed]
- Nangia, S.; Sunder, S.; Biswas, R.; Saili, A. Endotracheal suction in term non vigorous meconium stained neonates—A pilot study. Resuscitation 2016, 105, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Pandita, A.; Murki, S.; Oleti, T.P.; Tandur, B.; Kiran, S.; Narkhede, S.; Prajapati, A. Effect of Nasal Continuous Positive Airway Pressure on Infants with Meconium Aspiration Syndrome: A Randomized Clinical Trial. JAMA Pediatr. 2018, 172, 161–165. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, C.K. Management of Meconium-Stained Newborns in the Delivery Room. Neonatal Netw. 2018, 37, 141–148. [Google Scholar] [CrossRef]
- Bouziri, A.; Hamdi, A.; Khaldi, A.; Hadj, S.B.; Menif, K.; Ben Jaballah, N. Management of meconium aspiration syndrome with highfrequency oscillatory ventilation. Tunis. Med. 2011, 89, 632–637. [Google Scholar] [PubMed]
- Halliday, H.L.; Sweet, D.G. Endotracheal intubation at birth for preventing morbidity and mortality in vigorous, meconium-stained infants born at term. Cochrane Database Syst. Rev. 2001, 2001, CD000500. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, K.A.; Rose, R.S. Can nasal continuous positive airway pressure be used as primary respiratory support for infants with meconium aspiration syndrome? J. Perinatol. 2019, 39, 339–341. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed, S.A.; Shehab, M.M.; Ahmady, M.M.; Baraka, A. Early management of newborn with meconium aspiration syndrome using continuous positive airway pressure as a special modality. Int. J. Pharm. Phytopharm. Res. 2018, 8, 16–20. [Google Scholar]
- Anderson, J. Delivery Through Meconium-stained Amniotic Fluid. NeoReviews 2012, 13, e384–e386. [Google Scholar] [CrossRef]
- Dargaville, P.A.; Copnell, B.; Australian and New Zealand Neonatal Network. The Epidemiology of Meconium Aspiration Syndrome: Incidence, Risk Factors, Therapies, and Outcome. Pediatrics 2006, 117, 1712–1721. [Google Scholar] [CrossRef] [PubMed]
- Karlson, K.H.; Du Rant, R.H. High Frequency Positive Pressure Ventilation in Experimental Meconium Aspiration Syndrome. Am. J. Med. Sci. 1986, 292, 92–96. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Type of Study | Country | Number of Participants | Interventión | Controls (n) | Birth Weight, gm (Mean and sd) (Cpap/Intubatión) | Gestational Age, Weeks (Mean and sd) (Cpap/Intubatión) | Apgar 1 min (Mean and sd) (Cpap/Intubatión) | Apgar 5 min (Mean and sd) (Cpap/Intubatión) | Ph Cord (Mean and sd) (Cpap/Intubatión) | Length of Hospitalization, Days (Mean and sd) (Cpap/Intubatión) | Mortality (ee/te; ec/tc) | Pneumothorax (ee/te; ec/tc) | Ventilation Requeriment (ee/te; ec/tc) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NANGIA [11] | 2016 | RCT | India | 175 | No intubation, PPV | Endotracheal intubation | 2763 (533)/2649 (437) | 39 (0.77)/39 (0.77) | 6 (0.77)/8 (0.77) | 6 (0.77)/8 (0.77) | 7.14 (0.13)/7.13 (0.14) | 2.95 (0.86)/2.99 (1.26) | 23/88; 28/87 | 2/88; 2/87 | 8/88; 11/87 |
| PANDITA [12] | 2018 | RCT | India | 135 | CPAP | Endotracheal intubation | 2926 (389)/2963 (426) | 38.1 (1.3)/38.2 (1.3) | 7 (1.79)/7 (1.28) | 8 (0.77)/8 (0.77) | 7.2 (0.08)/7.2 (0.07) | 4 (0.51)/5 (1.22) | 1/67; 0/68 | 2/67; 17/68 | |
| CHETTRI [10] | 2015 | RCT | India | 122 | No intubation | Endotracheal intubation | 2900 (350)/2870 (490) | 27/61; 31/61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toro-Huamanchumo, C.J.; Hilario-Gomez, M.M.; Diaz-Reyes, N.; Caballero-Alvarado, J.A.; Barboza, J.J. The Efficacy of CPAP in Neonates with Meconium Aspiration Syndrome: A Systematic Review and Meta-Analysis. Children 2022, 9, 589. https://doi.org/10.3390/children9050589
Toro-Huamanchumo CJ, Hilario-Gomez MM, Diaz-Reyes N, Caballero-Alvarado JA, Barboza JJ. The Efficacy of CPAP in Neonates with Meconium Aspiration Syndrome: A Systematic Review and Meta-Analysis. Children. 2022; 9(5):589. https://doi.org/10.3390/children9050589
Chicago/Turabian StyleToro-Huamanchumo, Carlos J., Maryori M. Hilario-Gomez, Nelson Diaz-Reyes, José A. Caballero-Alvarado, and Joshuan J. Barboza. 2022. "The Efficacy of CPAP in Neonates with Meconium Aspiration Syndrome: A Systematic Review and Meta-Analysis" Children 9, no. 5: 589. https://doi.org/10.3390/children9050589