
Identification of a Novel FAM83H Mutation and Management of Hypocalcified Amelogenesis Imperfecta in Early Childhood

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Family Recruitment
2.2. DNA Isolation and Whole Exome Sequencing
2.3. Bioinformatics
2.4. Sanger Sequencing
3. Results
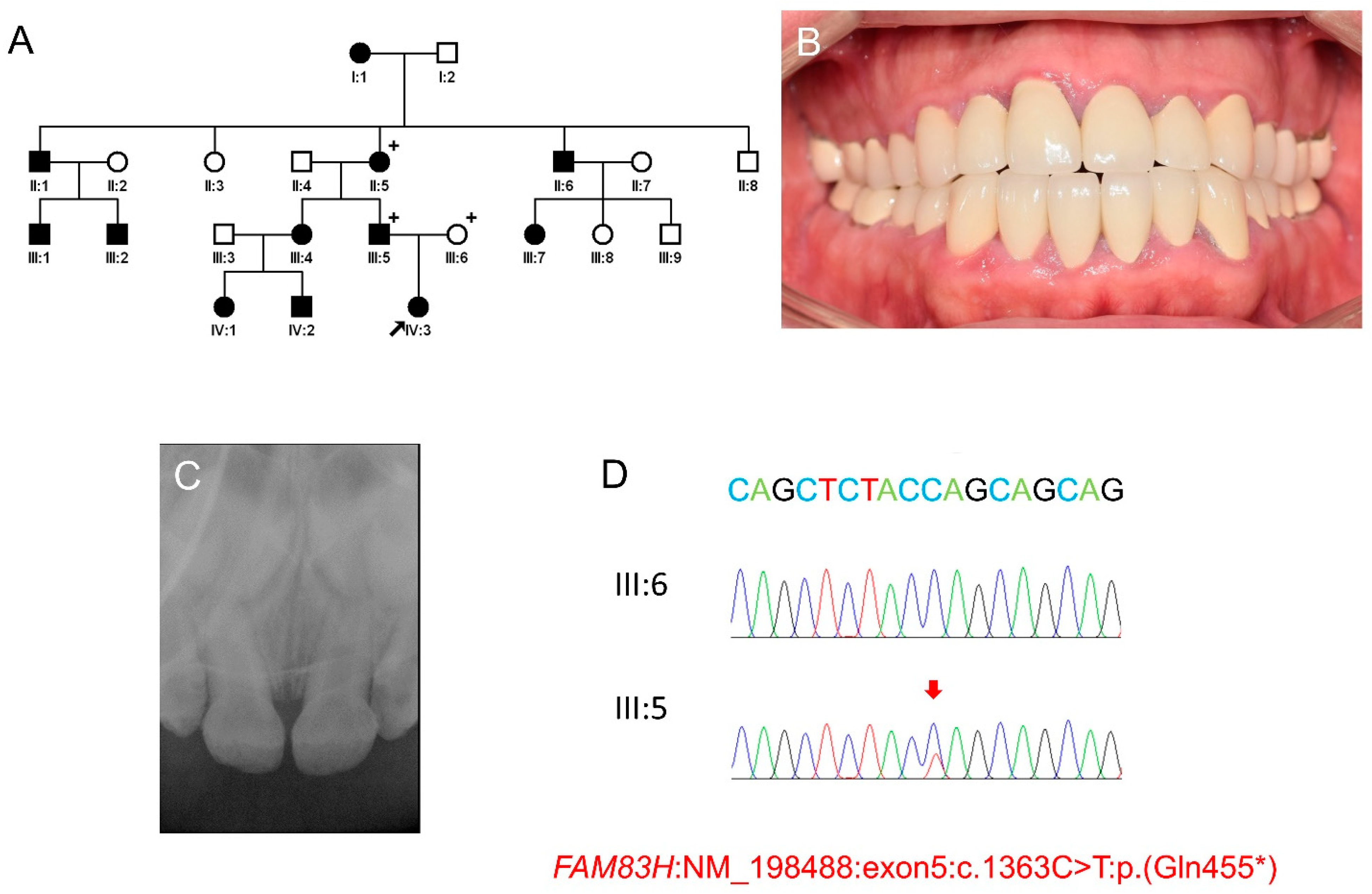
3.1. Mutational Analysis
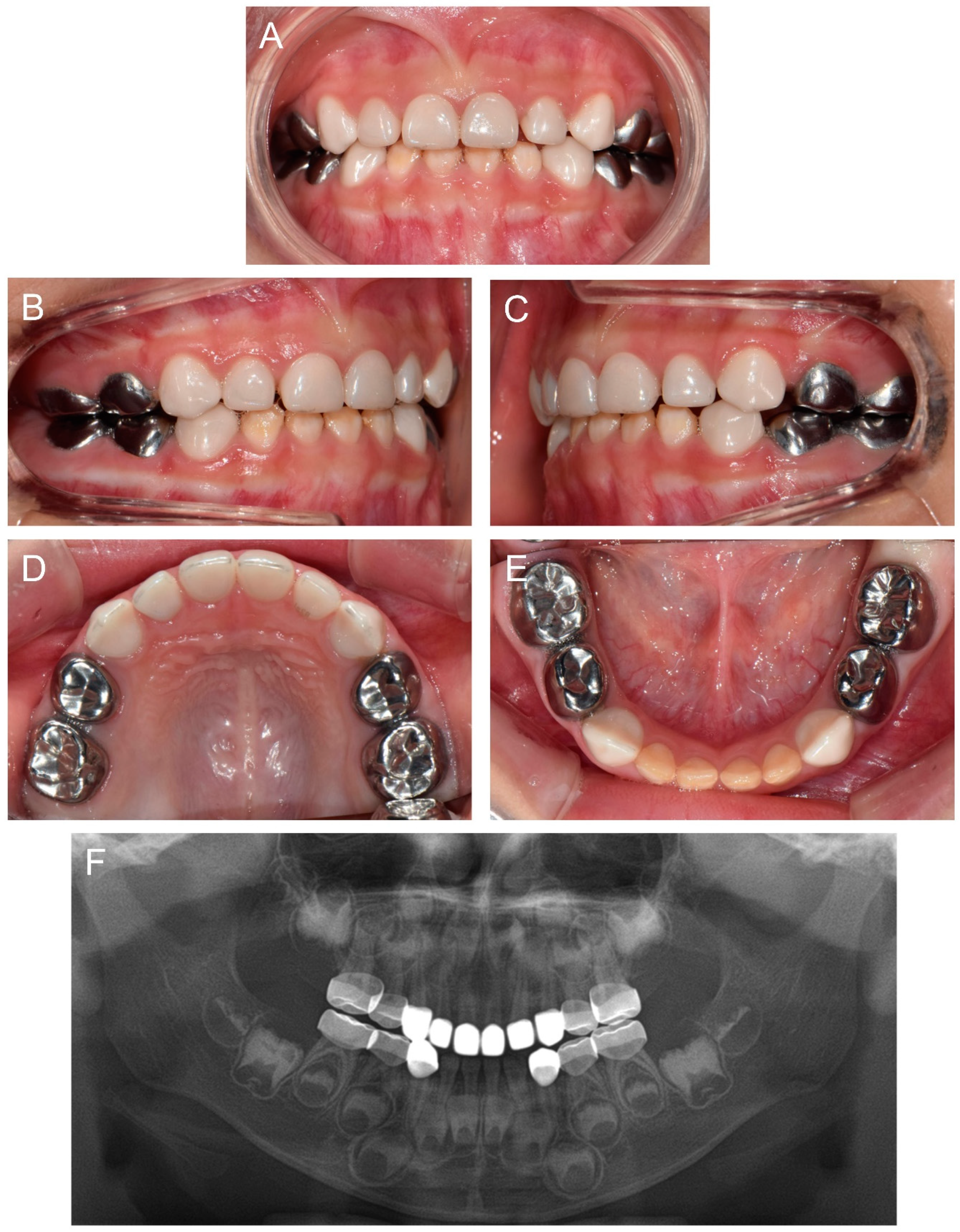
3.2. Clinical Phenotype and Treatment of the Proband
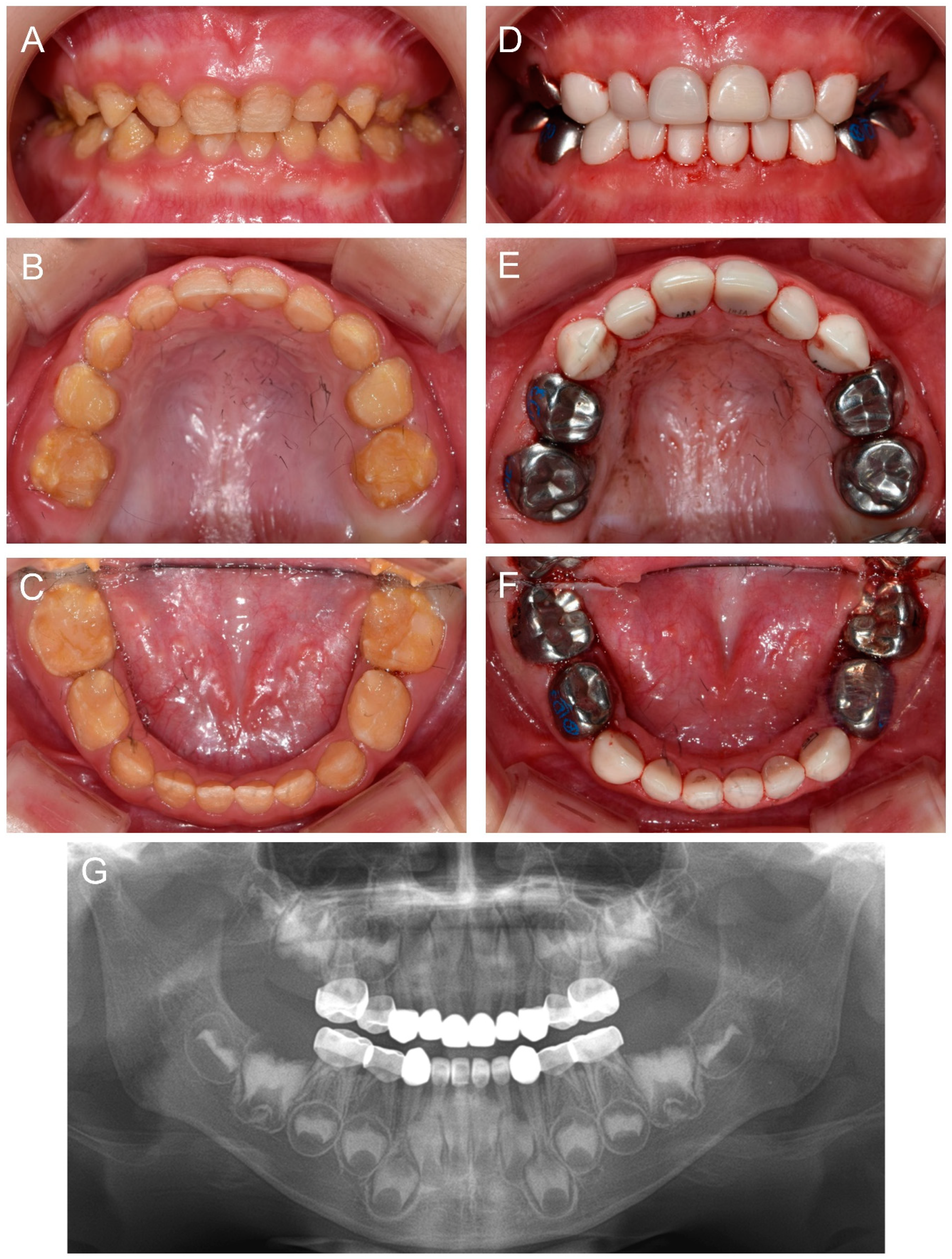
3.3. Treatment of the Affected Individual (IV:1)
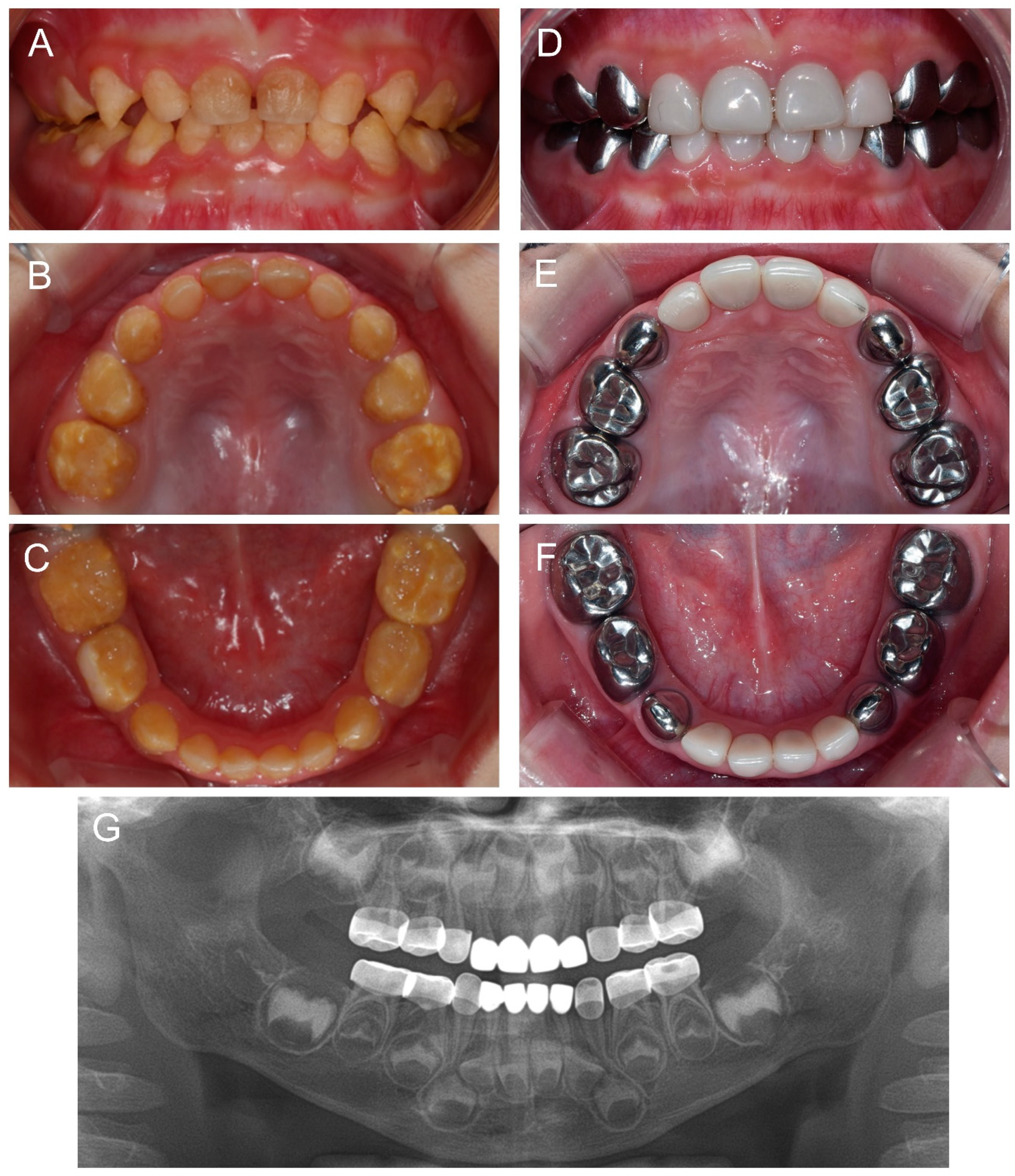
3.4. Treatment of the Affected Individual (IV:2)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Witkop, C.J., Jr. Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: Problems in classification. J. Oral Pathol. Med. 1988, 17, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.C.-C.; Chun, Y.-H.P.; Al Hazzazzi, T.; Simmer, J.P. Enamel Formation and Amelogenesis Imperfecta. Cells Tissues Organs 2007, 186, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Rajpar, M.H.; Harley, K.; Laing, C.; Davies, R.M.; Dixon, M.J. Mutation of the gene encoding the enamel-specific protein, enamelin, causes autosomal-dominant amelogenesis imperfecta. Hum. Mol. Genet. 2001, 10, 1673–1677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, J.T. The molecular etiologies and associated phenotypes of amelogenesis imperfecta. Am. J. Med. Genet. Part A 2006, 140, 2547–2555. [Google Scholar] [CrossRef] [Green Version]
- Prasad, M.K.; Laouina, S.; El Alloussi, M.; Dollfus, H.; Bloch-Zupan, A. Amelogenesis Imperfecta: 1 Family, 2 Phenotypes, and 2 Mutated Genes. J. Dent. Res. 2016, 95, 1457–1463. [Google Scholar] [CrossRef]
- Hart, P.S.; Hart, T.C.; Michalec, M.D.; Ryu, O.H.; Simmons, D.; Hong, S.; Wright, J.T. Mutation in kallikrein 4 causes autosomal recessive hypomaturation amelogenesis imperfecta. J. Med. Genet. 2004, 41, 545–549. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-W.; Simmer, J.P.; Hart, T.C.; Hart, P.S.; Ramaswami, M.D.; Bartlett, J.D.; Hu, J.C.-C. MMP-20 mutation in autosomal recessive pigmented hypomaturation amelogenesis imperfecta. J. Med. Genet. 2005, 42, 271–275. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-W.; Lee, S.-K.; Lee, Z.H.; Park, J.-C.; Lee, K.-E.; Lee, M.-H.; Park, J.-T.; Seo, B.-M.; Hu, J.C.-C.; Simmer, J.P. FAM83H Mutations in Families with Autosomal-Dominant Hypocalcified Amelogenesis Imperfecta. Am. J. Hum. Genet. 2008, 82, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Cho, E.S.; Kim, K.-J.; Lee, K.-E.; Lee, E.-J.; Yun, C.Y.; Lee, M.-J.; Shin, T.J.; Hyun, H.K.; Kim, Y.-J.; Lee, S.-H.; et al. Alteration of Conserved Alternative Splicing in AMELX Causes Enamel Defects. J. Dent. Res. 2014, 93, 980–987. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.-C.; Estrella, N.M.R.P.; Milkovich, R.N.; Kim, J.-W.; Simmer, J.P.; Hu, J.C.-C. Target gene analyses of 39 amelogenesis imperfecta kindreds. Eur. J. Oral Sci. 2011, 119, 311–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Zhang, H.; Hu, C.; Liu, J.; Chadha, S.; Kim, J.; Simmer, J.; Hu, J. FAM83H and Autosomal Dominant Hypocalcified Amelogenesis Imperfecta. J. Dent. Res. 2021, 100, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.; Frazier-Bowers, S.; Simmons, D.; Alexander, K.; Crawford, P.; Han, S.; Hart, P.; Hart, T. Phenotypic Variation in FAM83H-associated Amelogenesis Imperfecta. J. Dent. Res. 2009, 88, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Hu, Y.; Smith, C.E.; Yang, J.; Zeng, C.; Kim, J.; Hu, J.C.; Simmer, J.P. The Enamel Phenotype in Homozygous Fam83h Truncation Mice. Mol. Genet. Genom. Med. 2019, 7, e724. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Hu, Y.; Yang, J.; Smith, C.E.; Richardson, A.S.; Yamakoshi, Y.; Lee, Y.; Seymen, F.; Koruyucu, M.; Gencay, K.; et al. Fam83h null mice support a neomorphic mechanism for human ADHCAI. Mol. Genet. Genom. Med. 2016, 4, 46–67. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-K.; Lee, K.-E.; Jeong, T.-S.; Hwang, Y.-H.; Kim, S.; Hu, J.-C.; Simmer, J.; Kim, J.-W. FAM83H Mutations Cause ADHCAI and Alter Intracellular Protein Localization. J. Dent. Res. 2011, 90, 377–381. [Google Scholar] [CrossRef]
- Coffield, K.D.; Phillips, C.; Brady, M.; Roberts, M.W.; Strauss, R.P.; Wright, J.T. The psychosocial impact of developmental dental defects in people with hereditary amelogenesis imperfecta. J. Am. Dent. Assoc. 2005, 136, 620–630. [Google Scholar] [CrossRef]
- Kim, J.W.; Zhang, H.; Seymen, F.; Koruyucu, M.; Hu, Y.; Kang, J.; Kim, Y.J.; Ikeda, A.; Kasimoglu, Y.; Bayram, M.; et al. Mutations in RELT cause autosomal recessive amelogenesis imperfecta. Clin. Genet. 2019, 95, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Martin, M. Cutadapt removes adapter sequences from high-throughput sequencing reads. EMBnet. J. 2011, 17, 10–12. [Google Scholar] [CrossRef]
- Li, H.; Durbin, R. Fast and accurate long-read alignment with Burrows–Wheeler transform. Bioinformatics 2010, 26, 589–595. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Handsaker, B.; Wysoker, A.; Fennell, T.; Ruan, J.; Homer, N.; Marth, G.; Abecasis, G.; Durbin, R. 1000 Genome Project Data Processing Subgroup. The Sequence Alignment/Map format and SAMtools. Bioinformatics 2009, 25, 2078–2079. [Google Scholar] [CrossRef] [Green Version]
- McKenna, A.; Hanna, M.; Banks, E.; Sivachenko, A.; Cibulskis, K.; Kernytsky, A.; Garimella, K.; Altshuler, D.; Gabriel, S.; Daly, M.; et al. The Genome Analysis Toolkit: A MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010, 20, 1297–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Li, M.; Hakonarson, H. ANNOVAR: Functional annotation of genetic variants from high-throughput sequencing data. Nucleic Acids Res. 2010, 38, e164. [Google Scholar] [CrossRef] [PubMed]
- Sim, N.-L.; Kumar, P.; Hu, J.; Henikoff, S.; Schneider, G.; Ng, P.C. SIFT web server: Predicting effects of amino acid substitutions on proteins. Nucleic Acids Res. 2012, 40, W452–W457. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, J.M.; Cooper, D.N.; Schuelke, M.; Seelow, D. MutationTaster2: Mutation prediction for the deep-sequencing age. Nat. Methods 2014, 11, 361. [Google Scholar] [CrossRef] [PubMed]
- Adzhubei, I.A.; Schmidt, S.; Peshkin, L.; Ramensky, V.E.; Gerasimova, A.; Bork, P.; Kondrashov, A.S.; Sunyaev, S.R. A method and server for predicting damaging missense mutations. Nat. Methods 2010, 7, 248–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitkov, L.; Hannig, M.; Krautgartner, W.-D. Restorative therapy of primary teeth severely affected by amelogenesis imperfecta. Quintessence Int. 2006, 37, 219–224. [Google Scholar] [PubMed]
- Şaroğlu, I.; Aras, S.; Öztaş, D. Effect of deproteinization on composite bond strength in hypocalcified amelogenesis imperfecta. Oral Dis. 2006, 12, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Hyun, H.K.; Lee, S.-K.; Lee, K.-E.; Kang, H.-Y.; Kim, E.-J.; Choung, P.-H.; Kim, J.-W. Identification of a novelFAM83Hmutation and microhardness of an affected molar in autosomal dominant hypocalcified amelogenesis imperfecta. Int. Endod. J. 2009, 42, 1039–1043. [Google Scholar] [CrossRef]
- Sardana, D.; Manchanda, S.; Ekambaram, M.; Yang, Y.; McGrath, C.P.; Yiu, C.K.Y. Prevention of demineralization during multi-bracketed fixed orthodontic treatment: An overview of systematic reviews. Int. J. Paediatr. Dent. 2021. [Google Scholar] [CrossRef]
- Reynolds, E. Casein Phosphopeptide-Amorphous Calcium Phosphate: The Scientific Evidence. Adv. Dent. Res. 2009, 21, 25–29. [Google Scholar] [CrossRef]
- Lundgren, G.P.; Dahllöf, G. Outcome of restorative treatment in young patients with amelogenesis imperfecta. A cross-sectional, retrospective study. J. Dent. 2014, 42, 1382–1389. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, J.-S.; Lee, Y.; Shin, T.J.; Hyun, H.-K.; Kim, Y.-J.; Kim, J.-W. Identification of a Novel FAM83H Mutation and Management of Hypocalcified Amelogenesis Imperfecta in Early Childhood. Children 2022, 9, 429. https://doi.org/10.3390/children9030429
Song J-S, Lee Y, Shin TJ, Hyun H-K, Kim Y-J, Kim J-W. Identification of a Novel FAM83H Mutation and Management of Hypocalcified Amelogenesis Imperfecta in Early Childhood. Children. 2022; 9(3):429. https://doi.org/10.3390/children9030429
Chicago/Turabian StyleSong, Ji-Soo, Yejin Lee, Teo Jeon Shin, Hong-Keun Hyun, Young-Jae Kim, and Jung-Wook Kim. 2022. "Identification of a Novel FAM83H Mutation and Management of Hypocalcified Amelogenesis Imperfecta in Early Childhood" Children 9, no. 3: 429. https://doi.org/10.3390/children9030429