
Quantitative Assessment of Sensory Integration and Balance in Children with Autism Spectrum Disorders: Cross-Sectional Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
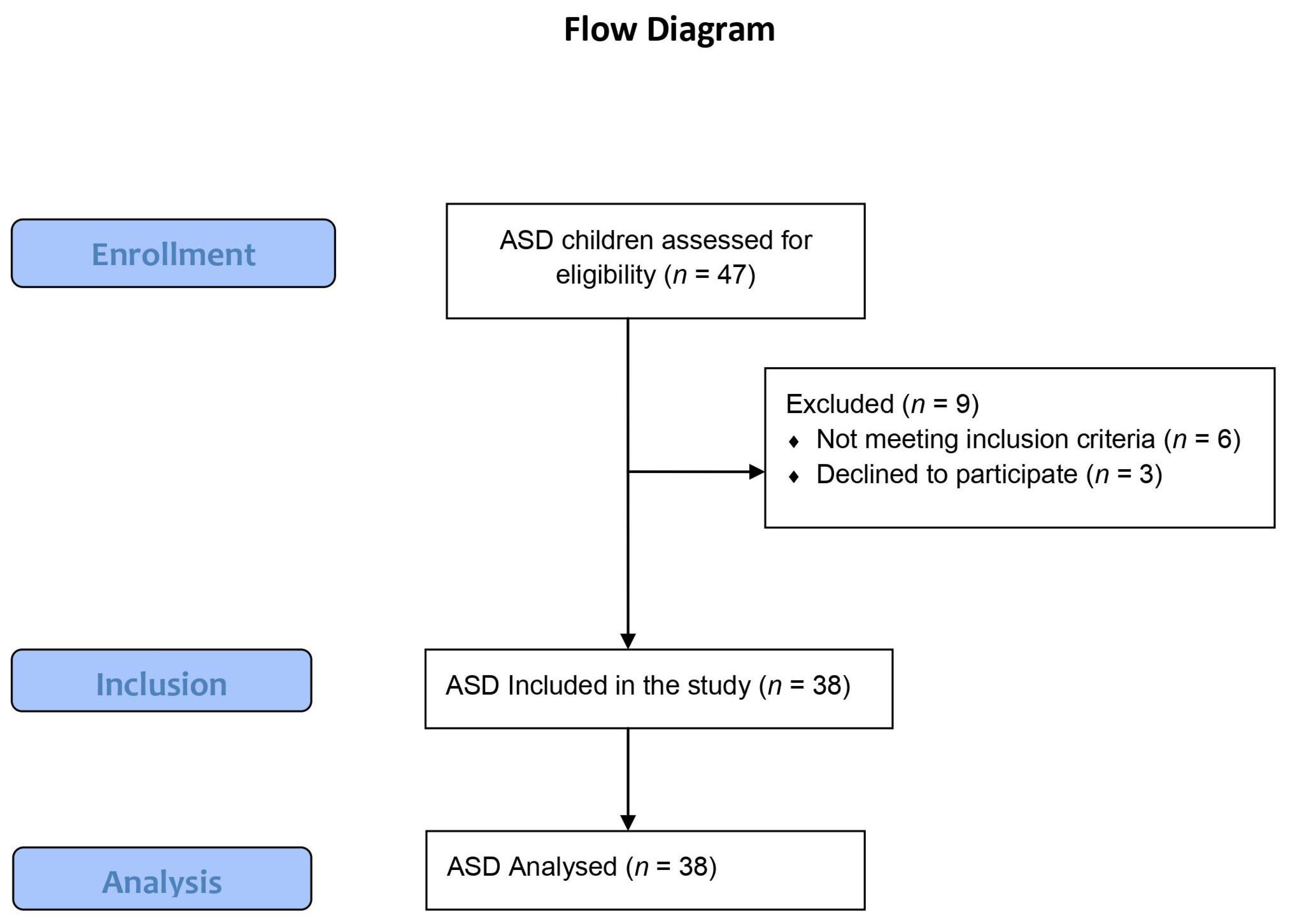
2.2. Participants
2.3. Procedures
2.3.1. Evaluation Procedures
Assessment of IQ
Balance Assessment
2.3.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fournier, K.A.; Kimberg, C.I.; Radonovich, K.J.; Tillman, M.D.; Chow, J.W.; Lewis, M.H.; Bodfish, J.W.; Chriss, J.H. Decreased Static and Dynamic Postural Control in Children with Autism Spectrum Disorders. Gait Posture 2010, 32, 6–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013; ISBN 9780890425541. [Google Scholar]
- Provost, B.; Lopez, B.R.; Heimerl, S. A Comparison of Motor Delays in Young Children: Autism Spectrum Disorder, Developmental Delay, and Developmental Concerns. J. Autism Dev. Disord. 2007, 37, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Minshew, N.J.; Sung, K.; Jones, B.L.; Furman, J.M. Underdevelopment of the postural control system in autism. Neurology 2004, 63, 2056–2061. [Google Scholar] [CrossRef]
- Inui, T.; Kumagaya, S.; Myowa-Yamakoshi, M. Neurodevelopmental Hypothesis about the Etiology of Autism Spectrum Disorders. Front. Hum. Neurosci. 2017, 11, 354. [Google Scholar] [CrossRef] [Green Version]
- Nayate, A.; Bradshaw, J.L.; Rinehart, N.J. Autism and Asperger’s disorder: Are they movement disorders involving the cerebellum and/or basal ganglia ? Brain Res. Bull. 2005, 67, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.H.; Tanimura, Y.; Lee, L.W.; Bodfish, J.W. Animal models of restricted repetitive behavior in autism. Behav. Brain Res. 2007, 176, 66–74. [Google Scholar] [CrossRef] [Green Version]
- Hallett, M.; Lebiedowska, M.K.; Denckla, M.B.; Rumsey, J.; Stanhope, S.J. Locomotion of Autistic Adults. Arch. Neurol. 1993, 50, 1304–1308. [Google Scholar] [CrossRef] [PubMed]
- Molloy, C.A.; Dietrich, K.N.; Bhattacharya, A. Postural Stability in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2003, 33, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Almeida, G.P.L.; Monteiro, I.O.; Marizeiro, D.F.; Maia, L.B.; de Paula Lima, P.O. Y balance test has no correlation with the Stability Index of the Biodex Balance System. Musculoskelet. Sci. Pract. 2017, 27, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Maurer, C.; Mergner, T.; Peterka, R.J. Multisensory control of human upright stance. Exp. Brain Res. 2006, 171, 231–250. [Google Scholar] [CrossRef] [PubMed]
- Gouleme, N.; Scheid, I.; Peyre, H.; Seassau, M.; Maruani, A.; Clarke, J.; Delorme, R.; Bucci, M.P. Postural control and emotion in children with autism spectrum disorders. Transl. Neurosci. 2017, 8, 158–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doumas, M.; Mckenna, R.; Murphy, B. Postural Control Deficits in Autism Spectrum Disorder: The Role of Sensory Integration. J. Autism Dev. Disord. 2016, 46, 853–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casartelli, L.; Molteni, M.; Ronconi, L. So close yet so far: Motor anomalies impacting on social functioning in autism spectrum disorder. Neurosci. Biobehav. Rev. 2016, 63, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Reed, P.; McCarthy, J. Cross-Modal Attention-Switching is Impaired in Autism Spectrum Disorders. J. Autism Dev. Disord. 2012, 42, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Noterdaeme, M.; Mildenberger, K.; Minow, F.; Hedwig, A. Evaluation of neuromotor deficits in children with autism and children with a specific speech and language disorder. Eur. Child Adolesc. Psychiatry 2002, 11, 219–225. [Google Scholar] [CrossRef]
- Memari, A.H.; Ghanouni, P.; Shayestehfar, M.; Ghaheri, B. Postural Control Impairments in Individuals with Autism Spectrum Disorder: A Critical Review of Current Literature. Asian J. Sport. Med. 2014, 5, e22963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawson, N.; Dzurino, D.; Karleskint, M.; Tucker, J. Examining the reliability, correlation, and validity of commonly used assessment tools to measure balance. Health Sci. Rep. 2018, 1, e98. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.H.; Lee, H.C.; Falkmer, T.; Allison, G.T.; Tan, T.; Lee, W.L.; Morris, S.L. Effect of Visual Information on Postural Control in Children with Autism Spectrum. J. Autism Dev. Disord. 2020, 50, 3320–3325. [Google Scholar] [CrossRef] [PubMed]
- Janzen, H.L.; Obrzut, J.E.; Marusiak, C.W. Test Review: Roid, G.H. Stanford-Binet Intelligence Scales, Fifth Edition (SB:V). Itasca, IL: Riverside Publishing. Can. J. Sch. Psychol. 2004, 19, 235–244. [Google Scholar] [CrossRef]
- Bain, S.K.; Allin, J.D. Book Review: Stanford-Binet Intelligence Scales, Fifth Edition. J. Psychoeduc. Assess. 2005, 23, 87–95. [Google Scholar] [CrossRef]
- Arifin, N.; Osman, N.A.A.; Abas, W.A.B.W. Intrarater Test-Retest Reliability of Static and Dynamic Stability Indexes Measurement Using the Biodex Stability System During Unilateral Stance. J. Appl. Biomech. 2014, 30, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Matos, M.R.; Matos, C.P.G.; Santos Oliveira, C. Static balance of low vision children using stabilometric parameters. Fisioter. Mov. 2010, 23, 361–369. [Google Scholar] [CrossRef]
- Stins, J.F.; Emck, C. Balance Performance in Autism: A Brief Overview. Front. Psychol. 2018, 9, 901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, S.A.; Abbott, A.E.; Nair, A.; Lincoln, A.J.; Müller, R.-A.; Goble, D.J. The Influence of Task Difficulty and Participant Age on Balance Control in ASD. J. Autism Dev. Disord. 2014, 45, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Adamovic, M.; Nikic, R.; Eminovic, F.; Stosljevic, M.; Pacic, S. The Ability to Maintain Balance in Children with Autism and the Ability to Maintain Balance in Children with Autism. Acta Kinesiol. 2015, 9, 54–60. [Google Scholar]
- Moseley, R.L.; Pulvermüller, F. What can autism teach us about the role of sensorimotor systems in higher cognition? New clues from studies on language, action semantics, and abstract emotional concept processing. Cortex 2018, 100, 149–190. [Google Scholar] [CrossRef]
- Stins, J.F.; Emck, C.; De Vries, E.M.; Doop, S.; Beek, P.J. Attentional and sensory contributions to postural sway in children with autism spectrum disorder. Gait Posture 2015, 42, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.H.; Partridge, K.; Girdler, S.; Morris, S.L. Standing Postural Control in Individuals with Autism Spectrum Disorder: Systematic Review and Meta-analysis. J. Autism Dev. Disord. 2017, 47, 2238–2253. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, E.S.G.; Aprígio, L.C.S.; Azoni, C.A.S.; Gazzola, J.M. Postural balance in children with Autism Spectrum Disorders. Rev. CEFAC 2021, 23, 5–11. [Google Scholar] [CrossRef]
- Kaur, M.; Srinivasan, S.; Bhat, A.; Program, M.S.; Program, T. Comparing motor performance, praxis, coordination, and interpersonal synchrony between children with and without Autism Spectrum Disorder (ASD). Res. Dev. Disabil. 2018, 72, 79–95. [Google Scholar] [CrossRef]
- Ramos-Sánchez, C.P.; Kortekaas, D.; Van Biesen, D.; Vancampfort, D.; Tine, V.D. The Relationship between Motor Skills and Intelligence in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2021, 52, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- Yumeng, L.; Ting, L.; Venuti, C.E. Development of postural stability in children with autism spectrum disorder: A cross-sectional study. Int. Biomech. 2021, 8, 54–62. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Groups | ASD Children, (n = 38) | TD Children, (n = 36) | p-Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 9.57 ± 2.08 | 10.84 ± 2.91 | 0.911 |
| Height (m) | 1.39 ± 9.72 | 1.31 ± 5.104 | 0.648 |
| Weight (kg) | 41.68 ± 9.13 | 37.45 ± 5.68 | 0.895 |
| BMI | 20.56 ± 6.41 | 19.89 ± 3.05 | 0.917 |
| IQ | 95 ± 11 | 115 ± 9 | 0.001 |
| Sex (girls/boys) | 13/25 | 15/21 | 0.827 |
| Variables | Age | p-Value | ||
|---|---|---|---|---|
| 6–9 Year | 10–14 Year | |||
| Mean ± SD | Mean ± SD | |||
| Eyes open/firm surface | ASD children | 5.73 ± 1.34 | 3.26 ± 1.15 | 0.017 * |
| TD children | 0.71 ±0.07 | 0.59 ± 0.03 | 0.022 * | |
| p-value | 0.001 * | 0.002 * | ||
| Eyes closed/firm surface | ASD children | 5.24 ± 1.71 | 4.47 ± 1.72 | 0.526 |
| TD children | 1.69 ± 0.09 | 1.07 ± 0.08 | 0.020 * | |
| p-value | 0.001 * | 0.007 * | ||
| Eyes open/foam surface | ASD children | 5.06 ± 2.21 | 3.16 ± 0.87 | 0.015 * |
| TD children | 1.34 ± 0.02 | 0.97 ± 0.3 | 0.024 * | |
| p-value | 0.001 * | 0.005 * | ||
| Eyes closed/foam surface | ASD children | 7.21 ± 1.68 | 6.78 ± 2.11 | 0.670 |
| TD children | 2.02 ± 0.26 | 1.45 ± 0.13 | 0.018 * | |
| p-value | 0.001 * | 0.001 * | ||
| Overall sway index score | ASD children | 6.58 ± 0.62 | 4.25 ± 1.15 | 0.021 * |
| TD children | 1.50 ± 0.04 | 1.03 ± 0.07 | 0.017 * | |
| p-value | 0.001 * | 0.007 * | ||
| Variables | IQ Score | p-Value | ||
|---|---|---|---|---|
| 70–89 | ≥90 | |||
| Mean ± SD | Mean ± SD | |||
| Eyes open/firm surface | ASD children | 6.02 ± 1.05 | 3.89 ± 1.78 | 0.020 * |
| TD children | 0.64 ±0.14 | 0.62 ± 0.06 | 0.802 | |
| p-value | 0.001 * | 0.003 * | ||
| Eyes closed/firm surface | ASD children | 5.87 ± 1.08 | 3.1 ± 0.99 | 0.019 * |
| TD children | 1.49 ± 0.28 | 1.42 ± 0.43 | 0.801 | |
| p-value | 0.001 * | 0.006 * | ||
| Eyes open/foam surface | ASD children | 5.21 ± 2.06 | 3.27 ± 0.98 | 0.021 * |
| TD children | 1.25 ± 0.11 | 1.29 ± 0.07 | 0.789 | |
| p-value | 0.002 * | 0.018 * | ||
| Eyes closed/foam surface | ASD children | 6.92 ± 1.97 | 4.62 ± 0.73 | 0.021 * |
| TD children | 1.83 ± 0.51 | 2.00 ± 0.28 | 0.425 | |
| p-value | 0.001 * | 0.019 * | ||
| Overall sway index score | ASD children | 6.82 ± 0.38 | 3.45 ± 0.35 | 0.020 * |
| TD children | 1.45 ± 0.09 | 1.06 ± 0.1 | 0.022 * | |
| p-value | 0.001 * | 0.006 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdel Ghafar, M.A.; Abdelraouf, O.R.; Abdelgalil, A.A.; Seyam, M.K.; Radwan, R.E.; El-Bagalaty, A.E. Quantitative Assessment of Sensory Integration and Balance in Children with Autism Spectrum Disorders: Cross-Sectional Study. Children 2022, 9, 353. https://doi.org/10.3390/children9030353
Abdel Ghafar MA, Abdelraouf OR, Abdelgalil AA, Seyam MK, Radwan RE, El-Bagalaty AE. Quantitative Assessment of Sensory Integration and Balance in Children with Autism Spectrum Disorders: Cross-Sectional Study. Children. 2022; 9(3):353. https://doi.org/10.3390/children9030353
Chicago/Turabian StyleAbdel Ghafar, Mohamed A., Osama R. Abdelraouf, Abdelgalil A. Abdelgalil, Mohamed K. Seyam, Rafik E. Radwan, and Amira E. El-Bagalaty. 2022. "Quantitative Assessment of Sensory Integration and Balance in Children with Autism Spectrum Disorders: Cross-Sectional Study" Children 9, no. 3: 353. https://doi.org/10.3390/children9030353