
Comparison between Digital Casts and Cone Beam Computed Tomography for Measuring Maxillary Transverse Dimensions in Patients with Impacted Canines



Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects and Study Design
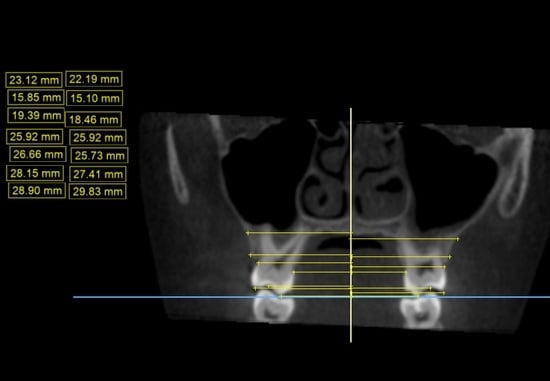
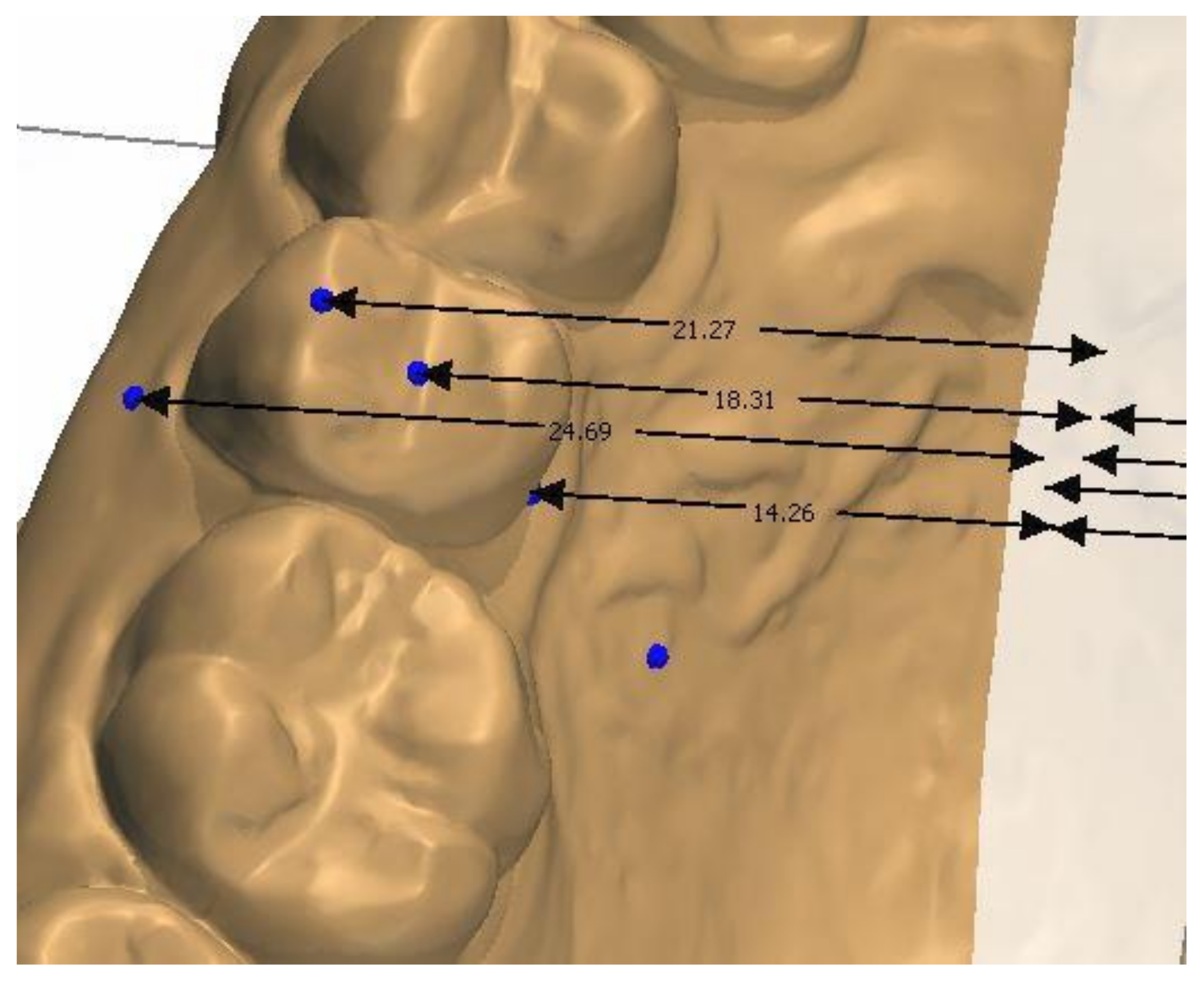
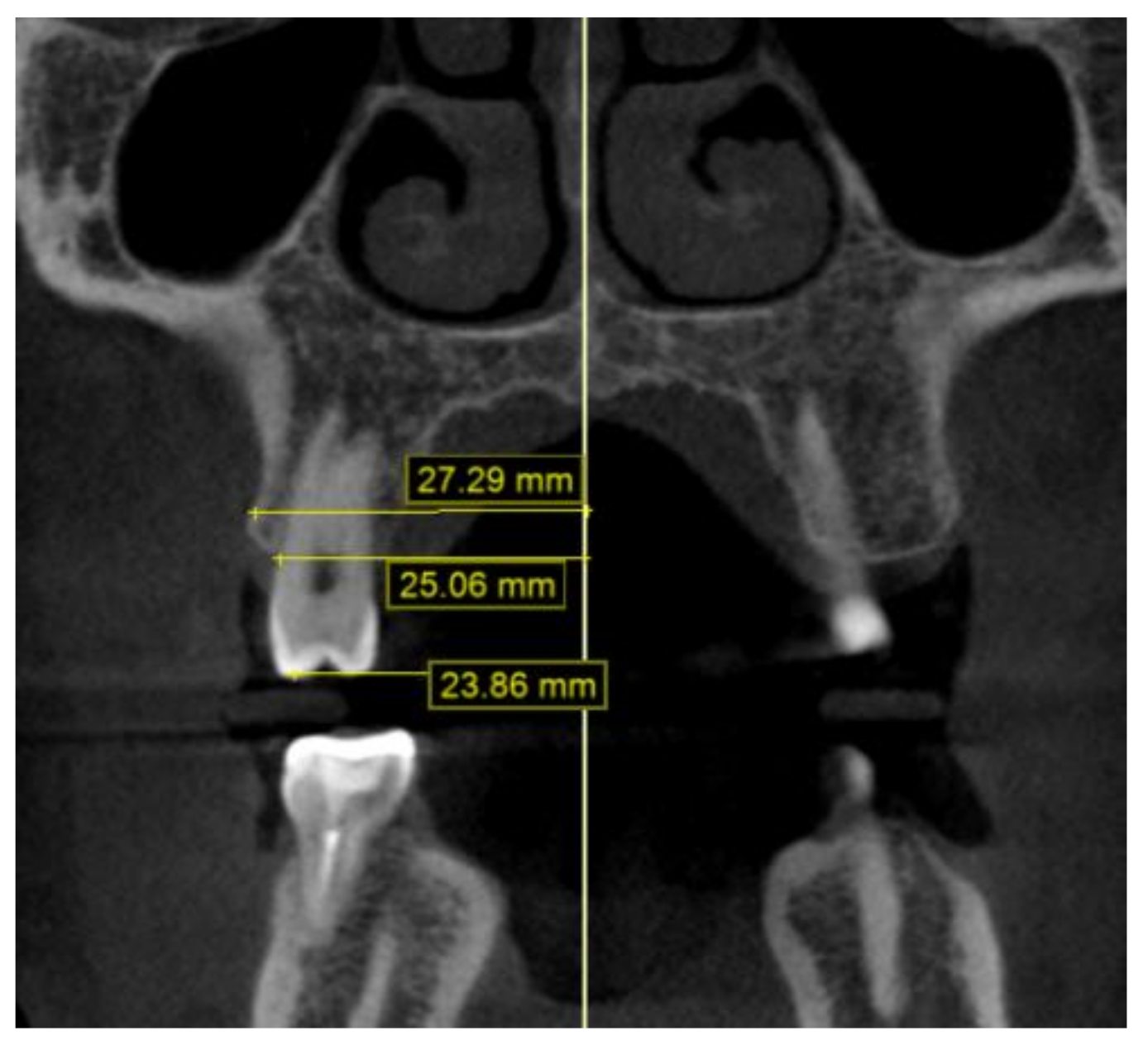
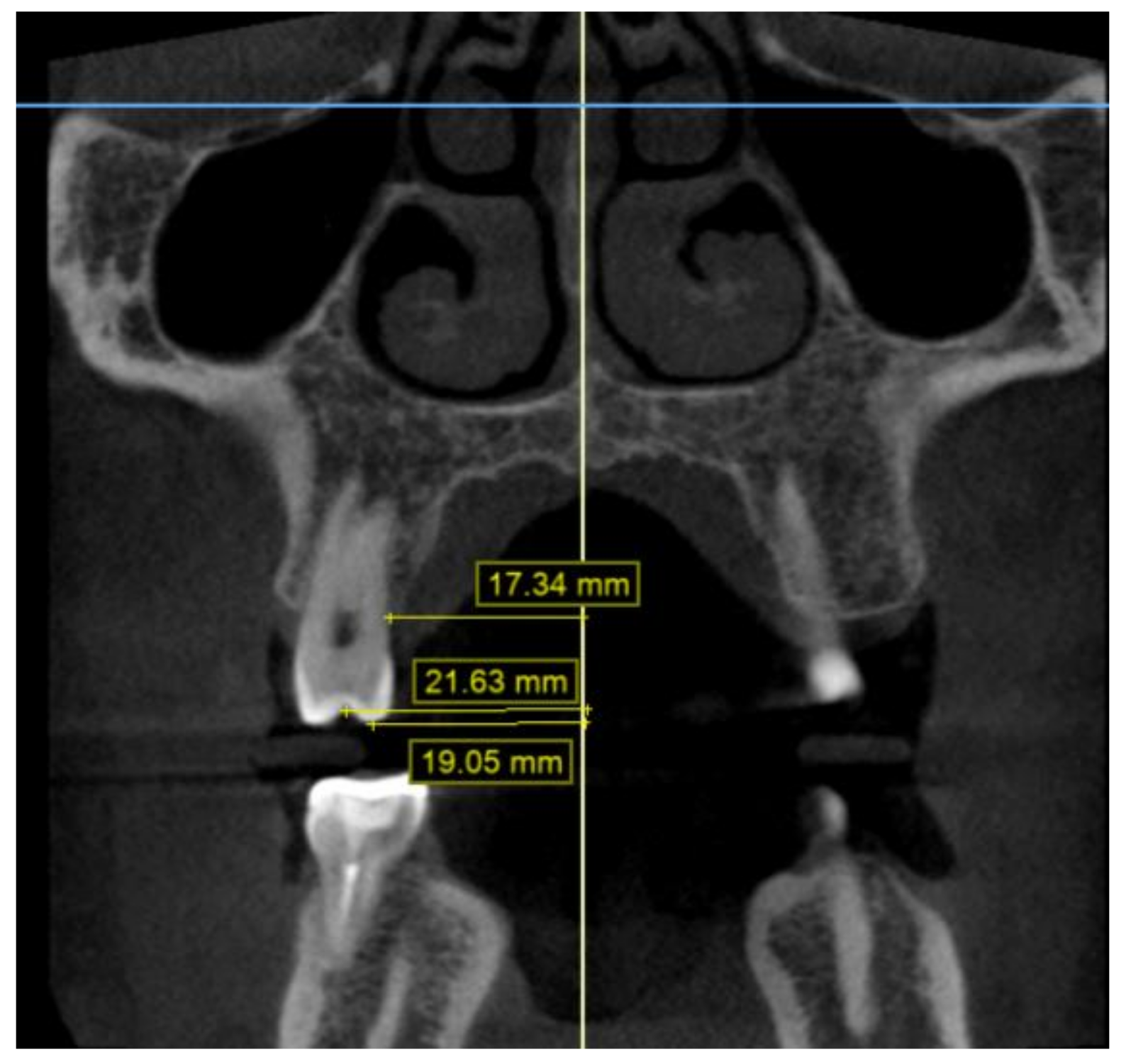
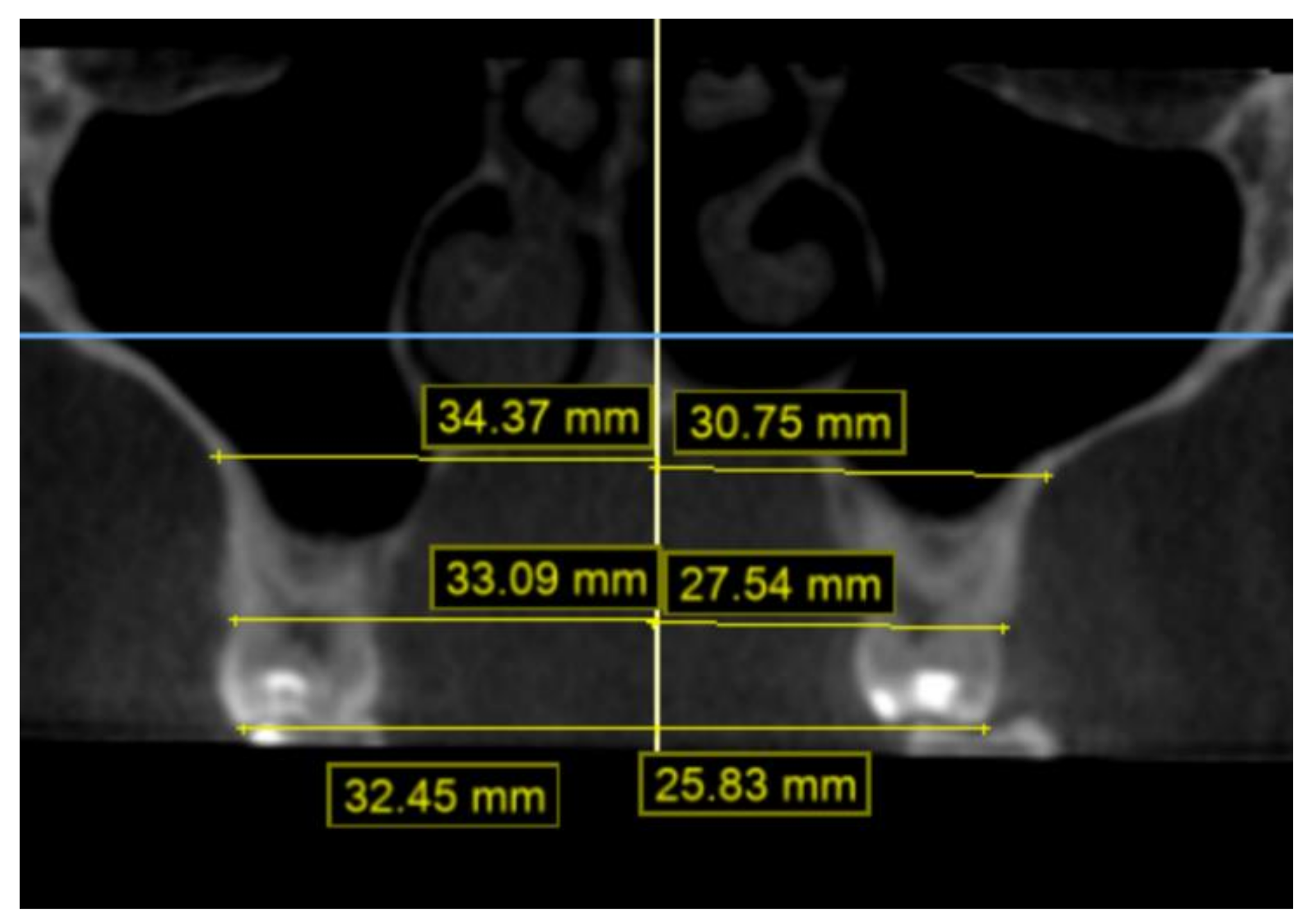
2.2. Methodology of Measurements
2.3. Statistical Analysis
3. Results
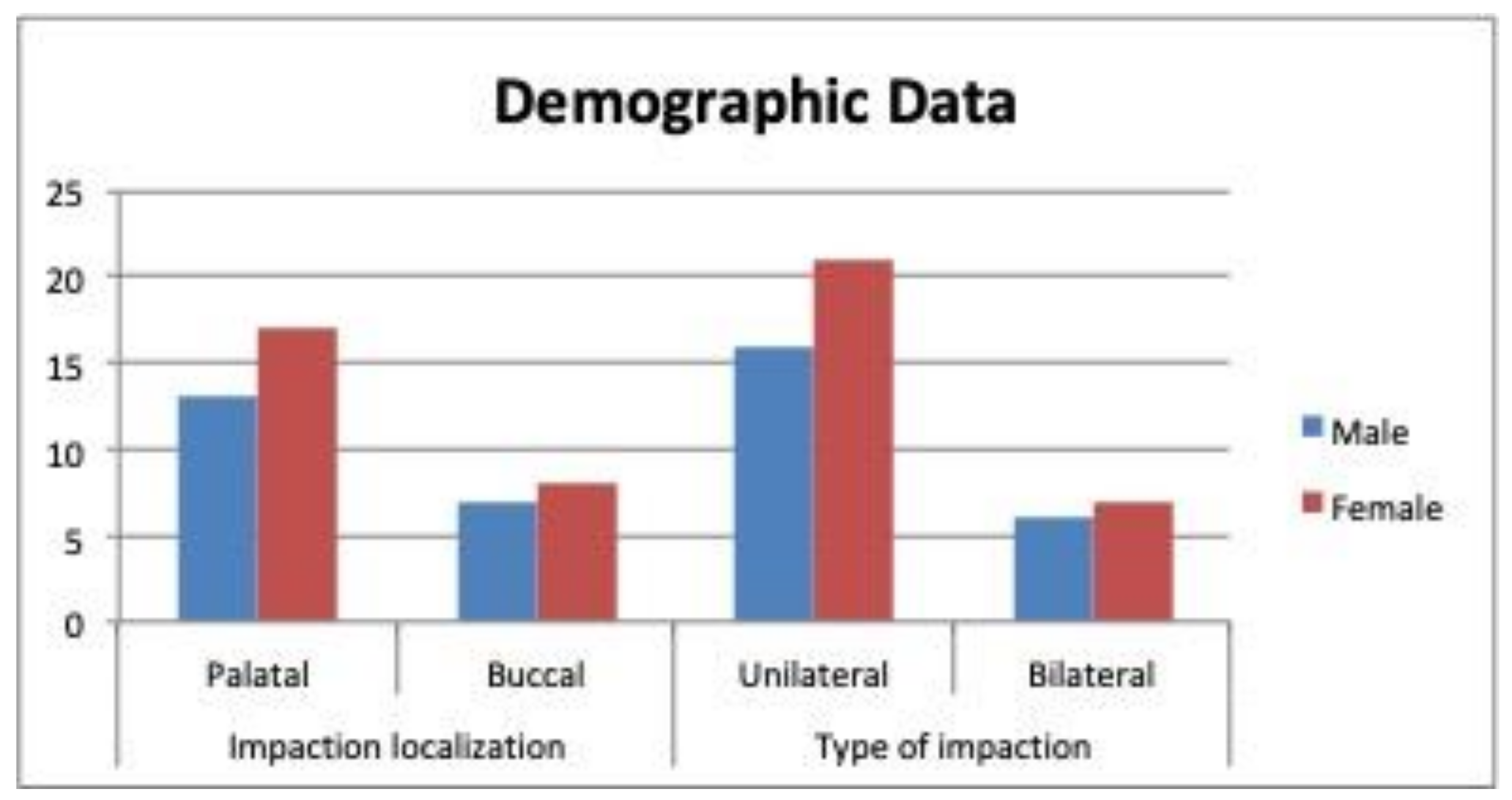
3.1. Demographic Data
3.2. Transverse Width
4. Discussion
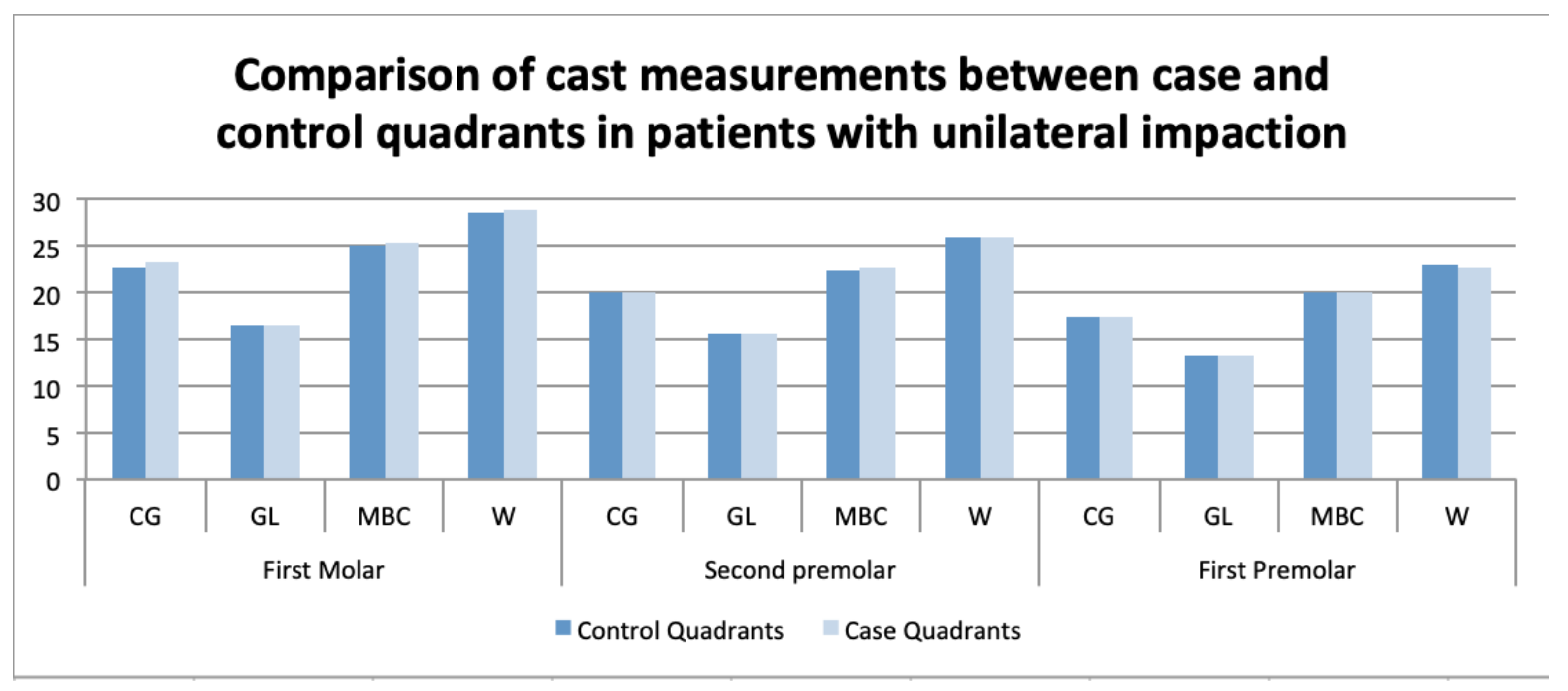
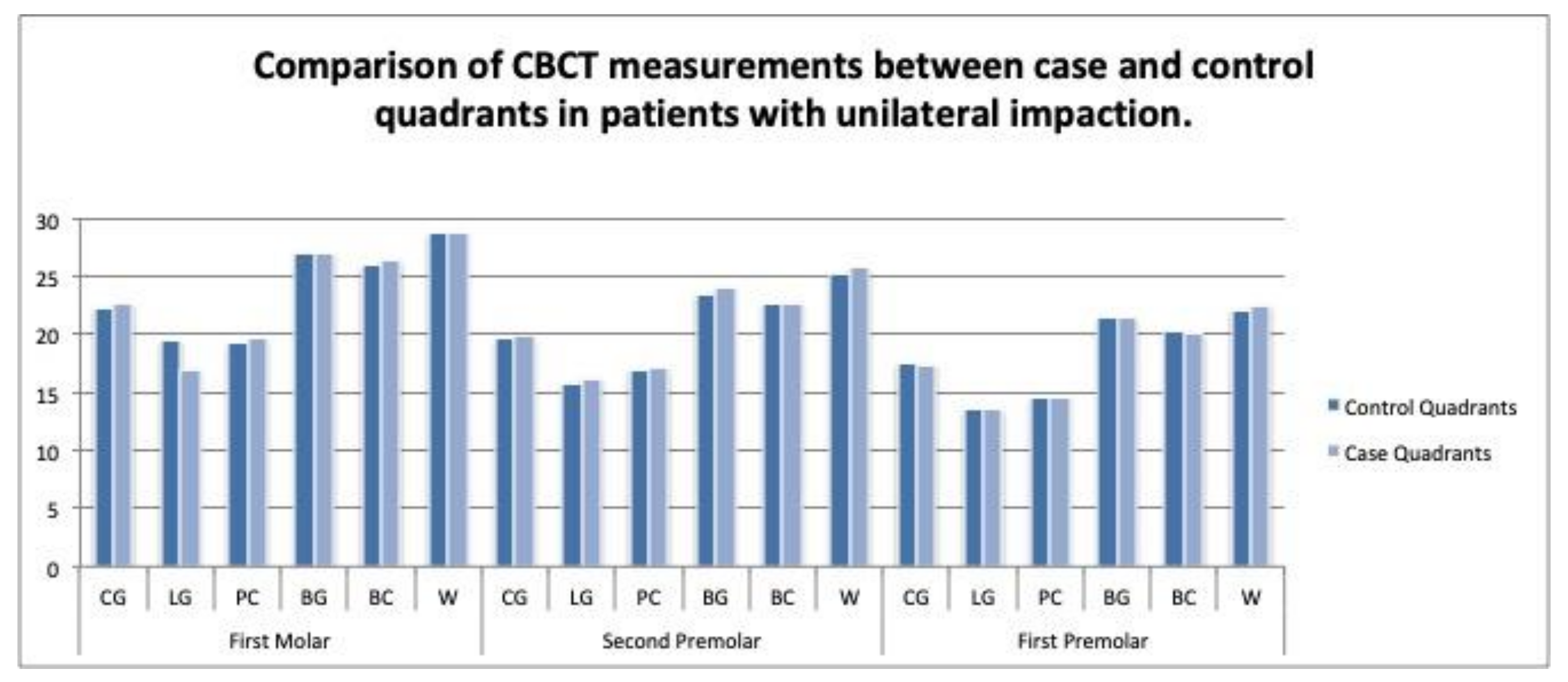
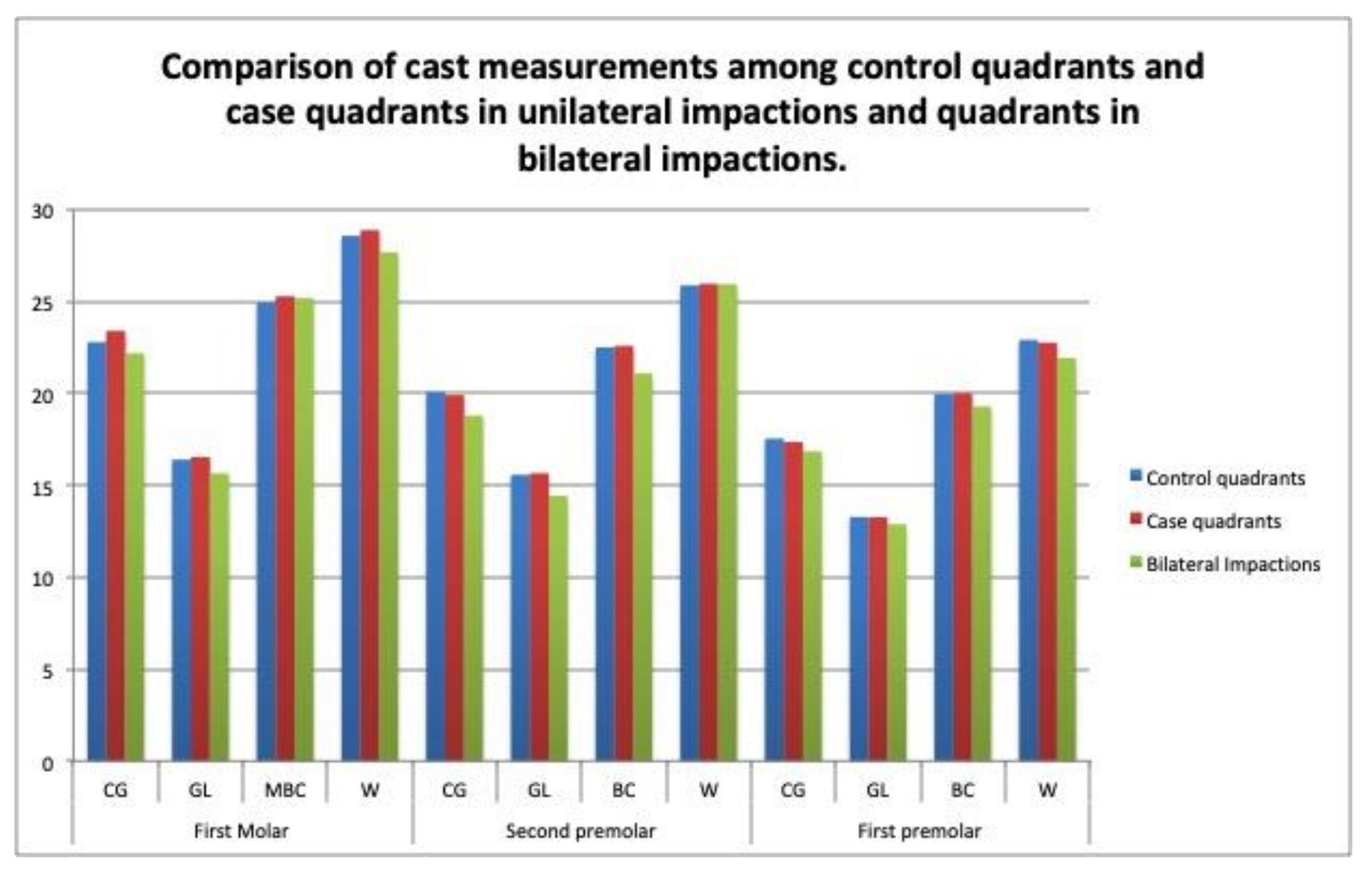
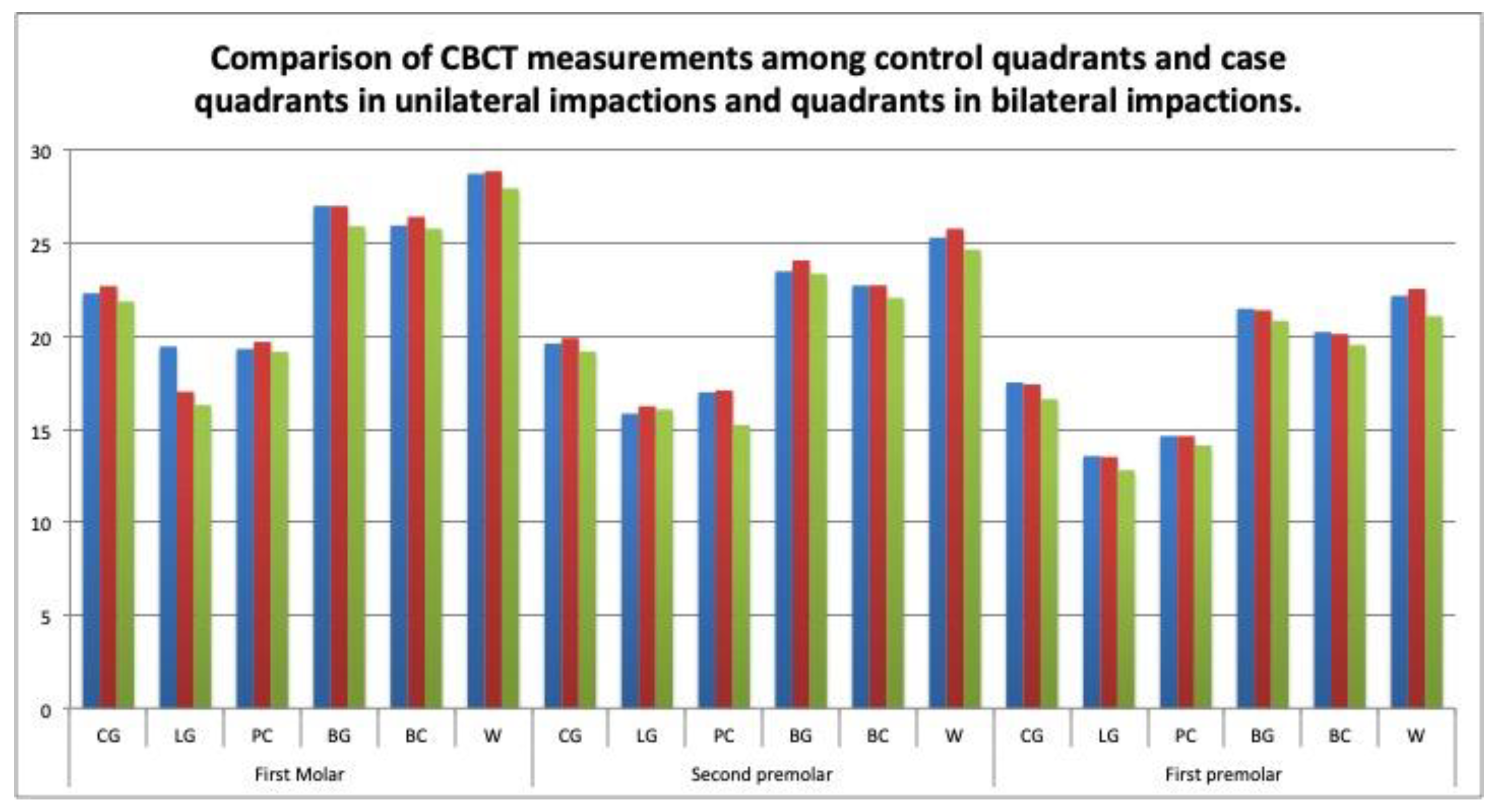
4.1. Transverse Dimensions in Case versus Control Quadrants in Unilateral Impactions
4.2. Transverse Dimensions in Unilateral versus Bilateral Impactions by Quadrant
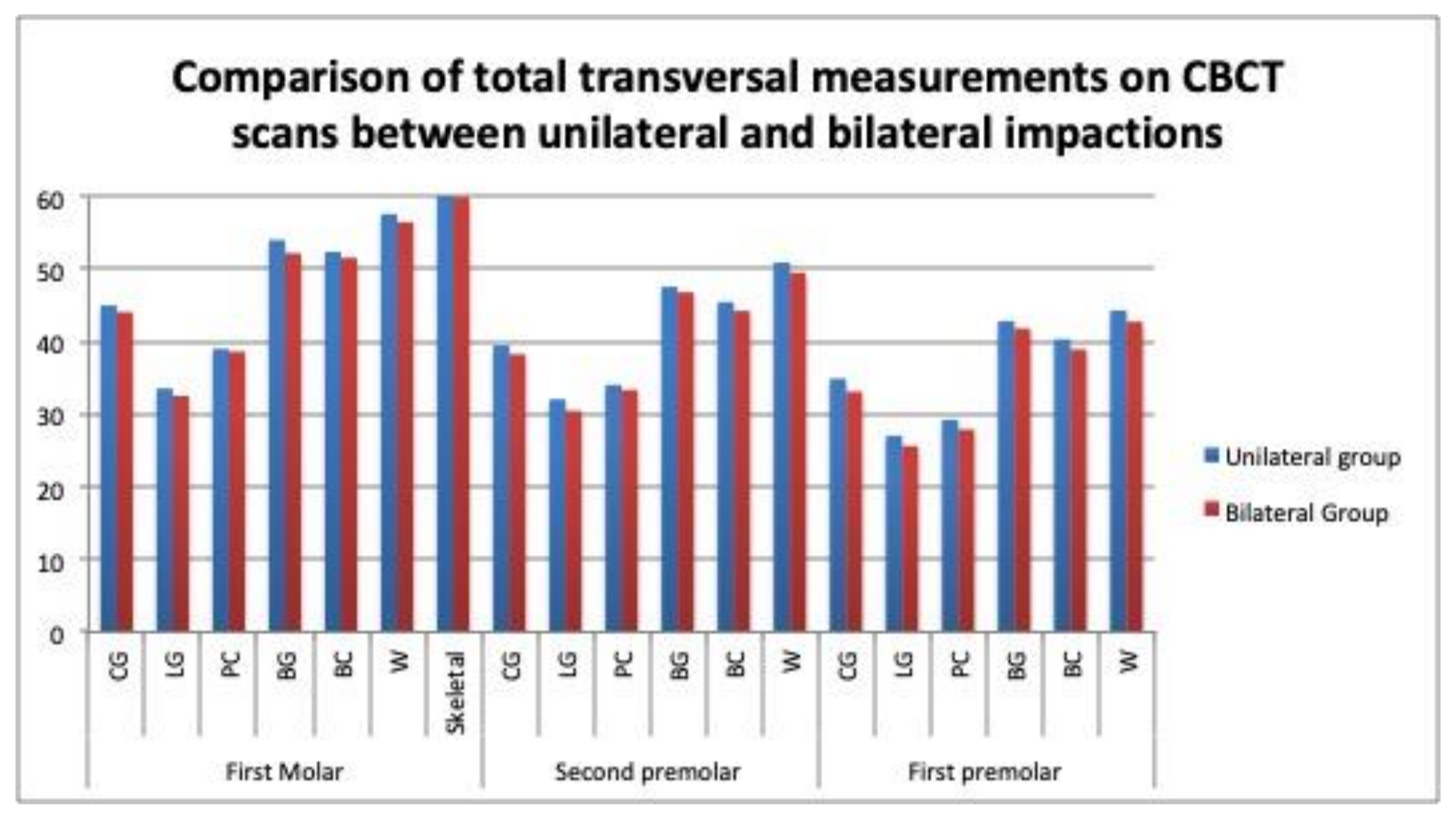
4.3. Transverse Dimensions in Unilateral versus Bilateral Impactions by Arch
4.4. Transverse Dimensions in Buccal versus Palatal Impactions
4.5. Transverse Measurements on CBCT Scans versus Casts
4.6. Clinical Relevance
- -
- Taking impressions with alginate and the subsequent casting in plaster may lead to certain accuracy errors in the digital models. The use of the latest-generation intraoral scanner could possibly produce a more accurate result because of the lack of cumulative errors, as the results from the systematic review by Jedliński et al. suggest [24].
- -
- It would be worthwhile to compare the results obtained with the results obtained from intraoral scans;
- -
- The infrabony position of the impacted canine, especially the distance to the occlusal plane, has not been considered (only its palatal or buccal position). The transversal maxillary development may be affected by this factor.
5. Conclusions
- The demographic data confirm that impacted canines were more frequent in females versus males, and when the impaction was palatal versus buccal, and unilateral versus bilateral. These impaction characteristics were not related to the maxillary arch width;
- There is no relationship between the maxillary arch width and the buccal or palatal displacement of the impacted canine;
- In the bilateral impactions, the maxillary arch had a smaller transverse width at the dental level. This difference was statistically significant on the digital casts but not on the CBCT scans;
- In the unilateral impactions, statistically significant differences in the measurements were observed between the case and control quadrants on both the digital casts and the CBCT scans.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bishara, S. Clinical Management of Impacted Maxillary Canines. Semin. Orthod. 1988, 4, 87–98. [Google Scholar] [CrossRef]
- Becker, A. Guidance theory of palatal canine displacement. Angle Orthod. 1995, 65, 95–102. [Google Scholar] [PubMed]
- Peck, S.; Peck, L.; Kataja, M. Concomitant occurrence of canine malposition and tooth agenesis: Evidence of orofacial genetic fields. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S. Impacted Maxilary canines: A review. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 159–171. [Google Scholar] [CrossRef]
- Jacoby, H. The etiology of maxillary canine impactions. Am. J. Orthod. Dentofac. Orthop. 1983, 84, 125–132. [Google Scholar] [CrossRef]
- McConnell, T.; Hoffman, D.L.; Forbes, D.P.; Janzen, E.K.; Weintrub, N.H. Maxillary canine impaction in patients with transverse maxillary deficiency. J. Dent. Child. 1996, 7, 190–195. [Google Scholar]
- Kim, Y.; Hyun, H.-K.; Jang, K.-T. Interrelationship between the position of impacted maxillary canines and the morphology of the maxilla. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 556–562. [Google Scholar] [CrossRef]
- Langberg, B.J.; Peck, S. Adequacy of maxillary dental arch width in patients with palatally displaced canines. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 220–223. [Google Scholar] [CrossRef]
- Saiar, M.; Rebellato, J.; Sheats, R.D. Palatal displacement of canines and maxillary skeletal width. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 511–519. [Google Scholar] [CrossRef]
- Yan, B.; Sun, Z.; Fields, H.; Wang, L.; Luo, L. Etiologic factors for buccal and palatal maxillary canine impaction: A perspective based on cone-beam computed tomography analyses. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 527–534. [Google Scholar] [CrossRef]
- Tai, B.; Goonewardene, M.S.; Murray, K.; Koong, B.; Islam, S.M.S. The reliability of using postero-anterior cephalometry and cone-beam CT to determine transverse dimensions in clinical practice. Aust. Orthod. 2014, 30, 132–142. [Google Scholar]
- Bizzarro, M.; Generali, C.; Maietta, S.; Martorelli, M.; Ferrillo, M.; Flores-Mir, C.; Perillo, L. Association between 3D palatal morphology and upper arch dimensions in buccally displaced maxillary canines early in mixed dentition. Eur. J. Orthod. 2018, 40, 592–596. [Google Scholar] [CrossRef]
- Ghaffar, F.; Sukhia, R.H.; Fida, M. Association between maxillary transverse discrepancy and occurrence of potentially impacted maxillary canines in mixed dentition patients. Int. Orthod. 2019, 17, 554–561. [Google Scholar] [CrossRef]
- Mucedero, M.; Rozzi, M.; Di Fusco, G.; Danessi, C.; Cozza, P. Morphometric analysis of the palatal shape and arch dimension in subjects with buccally displaced canine. Eur. J. Orthod. 2020, 42, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Hong, W.H.; Radfar, R.; Chung, C.-H. Relationship between the maxillary transverse dimension and palatally displaced canines: A cone-beam computed tomographic study. Angle Orthod. 2015, 85, 440–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arboleda-Ariza, N.; Schilling, J.; Arriola-Guillén, L.E.; Ruíz-Mora, G.A.; Rodríguez-Cárdenas, Y.A.; Castillo, A.A.-D. Maxillary transverse dimensions in subjects with and without impacted canines: A comparative cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Miresmaeili, A.; Shokri, A.; Salemi, F.; Dehghani, F.; Shahidi-Zandi, V.; Rad, R.; Shahdoost, M. Morphology of maxilla in patients with palatally displaced canines. Int. Orthod. 2019, 17, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Guo, J. Efficiency of upper arch expansion with the Invisalign system. Angle Orthodontist 2020, 90, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Cacciatore, G.; Poletti, L.; Sforza, C. Early diagnosed impacted maxillary canines and the morphology of the maxilla: A three-dimensional study. Prog. Orthod. 2018, 19, 20. [Google Scholar] [CrossRef]
- Ferrillo, M.; Curci, C.; Roccuzzo, A.; Migliario, M.; Invernizzi, M.; de Sire, A. Reliability of cervical vertebral maturation compared to hand-wrist for skeletal maturation assessment in growing subjects: A systematic review. J. Back Musculoskelet Rehabil. 2021, 34, 925–936. [Google Scholar] [CrossRef]
- Anic-Milosevic, S.; Varga, S.; Lapter-Varga, M.; Slaj, M. Dental and occlusal features in patients with palatally displaced maxillary canines. Eur. J. Orthod. 2009, 31, 367–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schindel, R.H.; Duffy, S.L. Maxillary Transverse Discrepancies and Potentially Impacted Maxillary Canines in Mixed-dentition Patients. Angle Orthod. 2006, 77, 430–435. [Google Scholar] [CrossRef]
- Naoumova, J.; Alfaro, G.E.; Peck, S. Space conditions, palatal vault height, and tooth size in patients with and without palatally displaced canines: A prospective cohort study. Angle Orthod. 2018, 2, 726–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jedliński, M.; Mazur, M.; Grocholewicz, K.; Janiszewska-Olszowska, J. 3D Scanners in Orthodontics—Current Knowledge and Future Perspectives—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1121. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Impaction Localization | Type of Impaction | Age (Years) | ||
|---|---|---|---|---|---|
| Palatal | Buccal | Unilateral | Bilateral | μ ± SD | |
| Male | 13 | 7 | 16 | 6 | 15.61 ± 3.42 |
| Female | 17 | 8 | 21 | 7 | 14.66 ± 4.20 |
| TOTAL | 30 | 15 | 34 | 11 | |
| p value | 0.504 | 0.554 | 0.806 | ||
| Interclass Coefficients for Interexaminer Agreement | Median | Max | Min |
|---|---|---|---|
| Casts | 0.919 | 0.997 | 0.54 |
| CBCT scans | 0.887 | 0.988 | 0.32 |
| Tooth | Parameter | Control Quadrants | Case Quadrants | p Value * |
|---|---|---|---|---|
| First Molar | CG | 22.78 | 23.4 | 0.103 |
| GL | 16.4 | 16.54 | 0.671 | |
| MBC | 24.94 | 25.28 | 0.343 | |
| W | 28.56 | 28.87 | 0.286 | |
| Second Premolar | CG | 20.07 | 19.9 | 0.56 |
| GL | 15.56 | 15.65 | 0.758 | |
| MBC | 22.5 | 22.57 | 0.798 | |
| W | 25.86 | 25.95 | 0.65 | |
| First Premolar | CG | 17.53 | 17.35 | 0.506 |
| GL | 13.27 | 13.26 | 0.935 | |
| MBC | 19.97 | 20 | 0.919 | |
| W | 22.9 | 22.75 | 0.56 |
| Tooth | Parameter | Control Quadrants | Case Quadrants | p Value * |
|---|---|---|---|---|
| First Molar | CG | 22.3 | 22.69 | 0.265 |
| LG | 19.44 | 17.01 | 0.001 * | |
| PC | 19.31 | 19.69 | 0.281 | |
| BG | 27 | 26.99 | 0.956 | |
| BC | 25.94 | 26.41 | 0.162 | |
| W | 28.72 | 28.86 | 0.642 | |
| Second Premolar | CG | 19.6 | 19.89 | 0.303 |
| LG | 15.83 | 16.23 | 0.175 | |
| PC | 16.98 | 17.08 | 0.771 | |
| BG | 23.48 | 24.07 | 0.158 | |
| BC | 22.72 | 22.73 | 0.984 | |
| W | 25.29 | 25.77 | 0.048 * | |
| First Premolar | CG | 17.51 | 17.4 | 0.724 |
| LG | 13.55 | 13.51 | 0.882 | |
| PC | 14.63 | 14.63 | 0.99 | |
| BG | 21.47 | 21.39 | 0.852 | |
| BC | 20.22 | 20.11 | 0.746 | |
| W | 22.16 | 22.54 | 0.163 |
| Tooth | Parameter | Control Quadrants | Case Quadrants | Bilateral Impactions | p Value * |
|---|---|---|---|---|---|
| First Molar | CG | 22.78 | 23.39 | 22.17 | 0. 145 |
| GL | 16.39 | 16.53 | 15.64 | 0. 267 | |
| MBC | 24.94 | 25.27 | 25.17 | 0.456 | |
| W | 28.56 | 28.87 | 27.66 | 0.456 | |
| Second Premolar | CG | 20.07 | 19.9 | 18.78 | 0.069 |
| GL | 15.56 | 15.65 | 14.42 | 0.76 | |
| BC | 22.5 | 22.57 | 21.07 | 0.025 * | |
| W | 25.86 | 25.95 | 25.93 | 0.145 | |
| First Premolar | CG | 17.53 | 17.35 | 16.84 | 0.487 |
| GL | 13.27 | 13.26 | 12.87 | 0.716 | |
| BC | 19.97 | 20 | 19.28 | 0.373 | |
| W | 22.9 | 22.75 | 21.92 | 0.277 |
| Tooth | Parameter | Control Quadrants | Case Quadrants | Bilateral Group | p Value * |
|---|---|---|---|---|---|
| First Molar | CG | 22.3 | 22.69 | 21.86 | 0.231 |
| LG | 19.44 | 17.01 | 16.29 | 0.001 * | |
| PC | 19.31 | 19.69 | 19.16 | 0.556 | |
| BG | 27 | 26.99 | 25.9 | 0.093 | |
| BC | 25.94 | 26.41 | 25.77 | 0.413 | |
| W | 28.72 | 28.86 | 27.94 | 0.375 | |
| Second Premolar | CG | 19.6 | 19.89 | 19.17 | 0.427 |
| LG | 15.83 | 16.23 | 32.05 | 0.208 | |
| PC | 16.98 | 17.08 | 15.22 | 0.914 | |
| BG | 23.48 | 24.07 | 23.35 | 0.587 | |
| BC | 22.72 | 22.73 | 22.05 | 0.399 | |
| W | 25.29 | 25.77 | 24.65 | 0.208 | |
| First Premolar | CG | 17.51 | 17.4 | 16.61 | 0.204 |
| LG | 13.55 | 13.51 | 12.79 | 0.384 | |
| PC | 14.63 | 14.63 | 14.12 | 0.691 | |
| BG | 21.47 | 21.39 | 20.82 | 0.539 | |
| BC | 20.22 | 20.11 | 19.52 | 0.558 | |
| W | 22.16 | 22.54 | 21.07 | 0.051 * |
| Tooth | Parameter | Unilateral Group | Bilateral Group | n | p Value * |
|---|---|---|---|---|---|
| First Molar | CG | 46.18 | 44.1 | 2.08 | 0. 071 |
| GL | 32.94 | 31.29 | 1.65 | 0. 120 | |
| MBC | 50.22 | 48.45 | 1.77 | 0.209 | |
| W | 57.44 | 54.99 | 2.45 | 0.054 * | |
| Second Premolar | CG | 39.98 | 37.27 | 2.71 | 0.028 * |
| GL | 31.21 | 28.65 | 2.59 | 0.041 * | |
| BC | 45.07 | 41.85 | 3.23 | 0.018 * | |
| W | 51.81 | 48.8 | 2.95 | 0.060 * | |
| First Premolar | CG | 34.88 | 33 | 1.88 | 0.08 |
| GL | 26.53 | 25.2 | 1.34 | 0.323 | |
| BC | 39.97 | 37.88 | 2.09 | 0.094 | |
| W | 45.65 | 43.02 | 2.63 | 0.128 |
| Tooth | Parameter | Unilateral Group | Bilateral Group | n | p Value * |
|---|---|---|---|---|---|
| First Molar | CG | 44.99 | 44.07 | 0.92 | 0.365 |
| LG | 33.55 | 32.54 | 1 | 0.385 | |
| PC | 39 | 38.62 | 0.38 | 0.792 | |
| BG | 53.99 | 52.17 | 1.82 | 0.141 | |
| BC | 52.35 | 51.53 | 0.82 | 0.543 | |
| W | 57.58 | 56.44 | 1.14 | 0.497 | |
| Skeletal | 61.12 | 59.94 | 1.19 | 0.385 | |
| Second Premolar | CG | 39.48 | 38.25 | 1.23 | 0.391 |
| LG | 32.06 | 30.47 | 1.59 | 0.214 | |
| PC | 34.05 | 33.35 | 0.7 | 0.596 | |
| BG | 47.55 | 46.79 | 0.76 | 0.465 | |
| BC | 45.45 | 44.23 | 1.22 | 0.298 | |
| W | 50.9 | 49.49 | 1.41 | 0.307 | |
| First Premolar | CG | 34.91 | 33.1 | 1.81 | 0.093 |
| LG | 27.06 | 25.64 | 1.42 | 0.306 | |
| PC | 29.26 | 27.91 | 1.35 | 0.315 | |
| BG | 42.84 | 41.82 | 1.04 | 0.622 | |
| BC | 40.33 | 38.93 | 1.4 | 0.139 | |
| W | 44.31 | 42.74 | 1.57 | 0.315 |
| Tooth | Parameter | Control Quadrants | Case Quadrants | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Buccal | Palatal | p Value * | Buccal | Palatal | p Value * | Buccal | Palatal | p Value * | ||
| First Molar | CG | 23.42 | 22.1 | 0.133 | 23.39 | 23.49 | 0. 953 | 46.82 | 45.53 | 0.35 |
| GL | 16.75 | 16.03 | 0.235 | 16.86 | 16.47 | 0.644 | 33.62 | 32.56 | 0.389 | |
| MBC | 25.65 | 24.25 | 0.188 | 25.43 | 25.03 | 0. 616 | 51.09 | 49.29 | 0.229 | |
| W | 29.24 | 28.09 | 0.193 | 29.3 | 28.75 | 0.441 | 57.07 | 57.6 | 0.249 | |
| Second Premolar | CG | 20.36 | 19.8 | 0.494 | 19.95 | 19.79 | 0.828 | 39.6 | 40.32 | 0.615 |
| GL | 16 | 15.37 | 0.443 | 15.51 | 31.28 | 0.485 | 31.28 | 31.51 | 0.866 | |
| BC | 23.01 | 22.23 | 0.343 | 22.48 | 22.47 | 0.987 | 44.7 | 45.5 | 0.583 | |
| W | 26.54 | 25.48 | 0.2 | 26.58 | 25.73 | 0.3 | 51.21 | 53.12 | 0.23 | |
| First Premolar | CG | 17.55 | 17.56 | 0.997 | 17.61 | 17.22 | 0.555 | 35.16 | 34.78 | 0.779 |
| GL | 13.21 | 13.33 | 0.803 | 13.25 | 13.33 | 0.906 | 26.46 | 27.24 | 0.6 | |
| BC | 19.99 | 19.97 | 0.986 | 19.97 | 19.97 | 0.995 | 39.96 | 39.98 | 0.989 | |
| W | 23.37 | 22.5 | 0.414 | 23.34 | 22.5 | 0.307 | 46.7 | 45.2 | 0.32 | |
| Tooth | Parameter | Control Quadrants | Case Quadrants | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Buccal | Palatal | p Value * | Buccal | Palate | p Value * | Buccal | Palatal | p Value * | ||
| First Molar | CG | 23.02 | 22.04 | 0.135 | 22.5 | 22.75 | 0.761 | 45.53 | 44.79 | 0.556 |
| LG | 20.23 | 19.15 | 0.063 | 17.52 | 16.81 | 0.422 | 34.83 | 33.07 | 0.166 | |
| PC | 20.09 | 19.02 | 0.102 | 19.42 | 19.78 | 0.646 | 39.51 | 38.81 | 0.566 | |
| BG | 27.74 | 26.72 | 0.134 | 27.05 | 26.95 | 0.912 | 54.8 | 53.68 | 0.422 | |
| BC | 26.82 | 25.61 | 0.08 | 26.72 | 26.29 | 0.631 | 53.55 | 51.991 | 0.244 | |
| W | 29.45 | 28.45 | 0.223 | 29.28 | 28.7 | 0.558 | 58.73 | 57.15 | 0.347 | |
| Second Premolar | CG | 19.84 | 19.5 | 0.612 | 20.01 | 19.84 | 0.834 | 39.86 | 39.35 | 0.701 |
| LG | 16.11 | 15.73 | 0.567 | 16.36 | 16.18 | 0.833 | 32.47 | 31.91 | 0.684 | |
| PC | 16.92 | 16.99 | 0.924 | 16.8 | 17.16 | 0.66 | 33.73 | 24.16 | 0.754 | |
| BG | 23.95 | 23.3 | 0.602 | 24.52 | 23.9 | 0.483 | 48.48 | 47.21 | 0.51 | |
| BC | 22.93 | 22.64 | 0.682 | 22.82 | 22.69 | 0.868 | 45.76 | 45.33 | 0.75 | |
| W | 26.06 | 25.01 | 0.15 | 26.57 | 25.49 | 0.091 | 52.63 | 50.51 | 0.176 | |
| First Premolar | CG | 17.45 | 17.52 | 0.93 | 17.55 | 17.34 | 0.783 | 35.01 | 34.87 | 0.921 |
| LG | 13.41 | 13.59 | 0.841 | 13.67 | 13.44 | 0.723 | 27.09 | 27.04 | 0.972 | |
| PC | 14.61 | 14.64 | 0.977 | 14.6 | 14.63 | 0.968 | 29.21 | 29.27 | 0.968 | |
| BG | 21.9 | 21.31 | 0.507 | 21.62 | 21.31 | 0.713 | 43.53 | 42.62 | 0.544 | |
| BC | 20.59 | 20.09 | 0.415 | 20.37 | 20.01 | 0.692 | 40.96 | 40.1 | 0.619 | |
| W | 22.5 | 22.04 | 0.368 | 22.77 | 22.46 | 0.757 | 43.76 | 44.5 | 0.673 | |
| Tooth | Parameter | Control Quadrants | Case Quadrants | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Cast | CBCT | p Value * | Cast | CBCT | p Value * | Cast | CBCT | p Value * | ||
| First Molar | CG | 22.55 | 22.37 | 0.548 | 23.28 | 22.7 | 0.041 * | 45.83 | 45.07 | 0.012 * |
| GL | 16.28 | 19.5 | 0.0001 * | 16.42 | 16.97 | 0.049 * | 32.7 | 33.56 | 0.001 * | |
| W | 28.37 | 28.74 | 0.018 * | 28.71 | 28.86 | 0.526 | 57.07 | 57.6 | 0.018 * | |
| Second Premolar | CG | 19.93 | 19.64 | 0.336 | 19.63 | 19.91 | 0.232 | 39.56 | 39.54 | 0.96 |
| GL | 15.53 | 15.86 | 0.251 | 15.61 | 16.27 | 0.018 * | 31.14 | 32.12 | 0.001 * | |
| W | 25.66 | 25.36 | 0.001 * | 25.8 | 25.81 | 0.937 | 51.45 | 51.18 | 0.306 | |
| First Premolar | CG | 17.46 | 17.49 | 0.883 | 17.13 | 17.22 | 0.606 | 34.59 | 34.71 | 0.406 |
| GL | 13.28 | 13.82 | 0.055 | 13.14 | 13.55 | 0.063 | 26.67 | 27.89 | 0.001 * | |
| W | 22.78 | 22.31 | 0.026 * | 22.42 | 22.54 | 0.699 | 45.3 | 44.38 | 0.164 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez Madero, E.; García Montarelo, J.; Aguayo, G.S.; Martin, C. Comparison between Digital Casts and Cone Beam Computed Tomography for Measuring Maxillary Transverse Dimensions in Patients with Impacted Canines. Children 2022, 9, 278. https://doi.org/10.3390/children9020278
Martinez Madero E, García Montarelo J, Aguayo GS, Martin C. Comparison between Digital Casts and Cone Beam Computed Tomography for Measuring Maxillary Transverse Dimensions in Patients with Impacted Canines. Children. 2022; 9(2):278. https://doi.org/10.3390/children9020278
Chicago/Turabian StyleMartinez Madero, Elena, Jaime García Montarelo, Grace Stefany Aguayo, and Conchita Martin. 2022. "Comparison between Digital Casts and Cone Beam Computed Tomography for Measuring Maxillary Transverse Dimensions in Patients with Impacted Canines" Children 9, no. 2: 278. https://doi.org/10.3390/children9020278