
The Role of Urotensin-II in Obesity and Metabolic Syndrome in Pediatric Population

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Anthropometric and Clinical Assessments
2.2. Definitions
2.3. Laboratory Analysis
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of Childhood and Adult Obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Lobstein, T. Worldwide Trends in Childhood Overweight and Obesity. Int. J. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Simunovic, M.; Supe-Domic, D.; Karin, Z.; Degoricija, M.; Paradzik, M.; Bozic, J.; Unic, I.; Skrabic, V. Serum Catestatin Concentrations Are Decreased in Obese Children and Adolescents. Pediatr. Diabetes 2019, 20, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Amer, O.E.; Alfawaz, H.; Sabico, S.; Khattak, M.N.K.; Alnaami, A.M.; Aljohani, N.J.; AlHameidi, A.; Al-Daghri, N.M. Increasing Prevalence of Pediatric Metabolic Syndrome and Its Components among Arab Youth: A Time-Series Study from. Children 2021, 8, 1129. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.M.; van Raaij, J.M.; Spinelli, A.; Starc, G.; Hassapidou, M.; Spiroski, I.; Rutter, H.; Martos, É.; Rito, A.I.; Hovengen, R.; et al. WHO European Childhood Obesity Surveillance Initiative: Body Mass Index and Level of Overweight among 6–9-Year-Old Children from School Year 2007/2008 to School Year 2009/2010. BMC Public Health 2014, 14, 806. [Google Scholar] [CrossRef] [Green Version]
- Dietz, W.H.; Robinson, T.N. Clinical Practice. Overweight Children and Adolescents. N. Engl. J. Med. 2005, 352, 2100–2109. [Google Scholar] [CrossRef] [Green Version]
- Freedman, D.S.; Khan, L.K.; Serdula, M.K.; Dietz, W.H.; Srinivasan, S.R.; Berenson, G.S. Racial Differences in the Tracking of Childhood BMI to Adulthood. Obes. Res. 2005, 13, 928–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berenson, G.S.; Srinivasan, S.R.; Bao, W.; Newman, W.P.; Tracy, R.E.; Wattigney, W.A. Association between Multiple Cardiovascular Risk Factors and Atherosclerosis in Children and Young Adults. The Bogalusa Heart Study. N. Engl. J. Med. 1998, 338, 1650–1656. [Google Scholar] [CrossRef]
- Hannon, T.S.; Rao, G.; Arslanian, S.A. Childhood Obesity and Type 2 Diabetes Mellitus. Pediatrics 2005, 116, 473–480. [Google Scholar] [CrossRef] [Green Version]
- Weiss, R.; Kaufman, F.R. Metabolic Complications of Childhood Obesity: Identifying and Mitigating the Risk. Diabetes Care 2008, 31, S310–S316. [Google Scholar] [CrossRef] [Green Version]
- Zimmet, P.; Alberti, K.G.; Kaufman, F.; Tajima, N.; Silink, M.; Arslanian, S.; Wong, G.; Bennett, P.; Shaw, J.; Caprio, S. The Metabolic Syndrome in Children and Adolescents—an IDF Consensus Report. Pediatr. Diabetes 2007, 8, 299–306. [Google Scholar] [CrossRef]
- Weiss, R.; Bremer, A.A.; Lustig, R.H. What Is Metabolic Syndrome, and Why Are Children Getting It? Ann. N. Y. Acad. Sci. 2013, 1281, 123–140. [Google Scholar] [CrossRef] [Green Version]
- Cornier, M.-A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The Metabolic Syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar] [CrossRef]
- Šimunović, M.; Božić, J.; Milić, L.; Unić, I.; Škrabić, V. The Prevalence of Metabolic Syndrome and Cardiovascular Risk Factors in Obese Children and Adolescents in Dalmatia: A Hospital Based Study. Int. J. Endocrinol. 2016, 2016, 1823561. [Google Scholar] [CrossRef] [Green Version]
- Ko, D.H.; Kim, Y.K. The Prevalence of Metabolic Syndrome According to Grip Strength in Teenagers. Children 2021, 8, 108. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic Syndrome—A New World-Wide Definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Ames, R.S.; Sarau, H.M.; Chambers, J.K.; Willette, R.N.; Aiyar, N.V.; Romanic, A.M.; Louden, C.S.; Foley, J.J.; Sauermelch, C.F.; Coatney, R.W.; et al. Human Urotensin-II Is a Potent Vasoconstrictor and Agonist for the Orphan Receptor GPR14. Nature 1999, 401, 282–286. [Google Scholar] [CrossRef]
- Jiang, Z.; Michal, J.J.; Tobey, D.J.; Wang, Z.; MacNeil, M.D.; Magnuson, N.S. Comparative Understanding of UTS2 and UTS2R Genes for Their Involvement in Type 2 Diabetes Mellitus. Int. J. Biol. Sci. 2008, 4, 96–102. [Google Scholar] [CrossRef]
- Suzuki, S.; Wenyi, Z.; Hirai, M.; Hinokio, Y.; Suzuki, C.; Yamada, T.; Yoshizumi, S.; Suzuki, M.; Tanizawa, Y.; Matsutani, A.; et al. Genetic Variations at Urotensin II and Urotensin II Receptor Genes and Risk of Type 2 Diabetes Mellitus in Japanese. Peptides 2004, 25, 1803–1808. [Google Scholar] [CrossRef]
- Pearson, D.; Shively, J.E.; Clark, B.R.; Geschwind, I.I.; Barkley, M.; Nishioka, R.S.; Bern, H.A. Urotensin II: A Somatostatin-like Peptide in the Caudal Neurosecretory System of Fishes. Proc. Natl. Acad. Sci. USA 1980, 77, 5021–5024. [Google Scholar] [CrossRef] [Green Version]
- Ross, B.; McKendy, K.; Giaid, A. Role of Urotensin II in Health and Disease. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, R1156–R1172. [Google Scholar] [CrossRef] [PubMed]
- Charles, C.J.; Rademaker, M.T.; Richards, A.M.; Yandle, T.G. Urotensin II: Evidence for Cardiac, Hepatic and Renal Production. Peptides 2005, 26, 2211–2214. [Google Scholar] [CrossRef] [PubMed]
- Cheung, B.M.Y.; Leung, R.; Man, Y.B.; Wong, L.Y.F. Plasma Concentration of Urotensin II Is Raised in Hypertension. J. Hypertens. 2004, 22, 1341–1344. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Suguro, T.; Kanome, T.; Sakamoto, Y.-I.; Kodate, S.; Hagiwara, T.; Hongo, S.; Hirano, T.; Adachi, M.; Miyazaki, A. Human Urotensin II Accelerates Foam Cell Formation in Human Monocyte-Derived Macrophages. Hypertension 2005, 46, 738–744. [Google Scholar] [CrossRef] [Green Version]
- Totsune, K.; Takahashi, K.; Arihara, Z.; Sone, M.; Murakami, O.; Ito, S.; Kikuya, M.; Ohkubo, T.; Hashimoto, J.; Imai, Y. Elevated Plasma Levels of Immunoreactive Urotensin II and Its Increased Urinary Excretion in Patients with Type 2 Diabetes Mellitus: Association with Progress of Diabetic Nephropathy. Peptides 2004, 25, 1809–1814. [Google Scholar] [CrossRef]
- Giuliani, L.; Lenzini, L.; Antonello, M.; Aldighieri, E.; Belloni, A.S.; Fassina, A.; Gomez-Sanchez, C.; Rossi, G.P. Expression and Functional Role of Urotensin-II and Its Receptor in the Adrenal Cortex and Medulla: Novel Insights for the Pathophysiology of Primary Aldosteronism. J. Clin. Endocrinol. Metab. 2009, 94, 684–690. [Google Scholar] [CrossRef] [Green Version]
- Ong, K.L.; Wong, L.Y.F.; Cheung, B.M.Y. The Role of Urotensin II in the Metabolic Syndrome. Peptides 2008, 29, 859–867. [Google Scholar] [CrossRef]
- Simunovic, M.; Supe-Domic, D.; Karin, Z.; Degoricija, M.; Paradzik, M.; Skrabic, R.; Jukic, A.; Bozic, J.; Skrabic, V. The Relationship of Vitamin D Status, Adherence to the Mediterranean Diet, and Physical Activity in Obese Children and Adolescents. J. Med. Food 2020, 24, 385–393. [Google Scholar] [CrossRef]
- Marshall, W.A.; Tanner, J.M. Variations in the Pattern of Pubertal Changes in Boys. Arch. Dis. Child. 1970, 45, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Marshall, W.A.; Tanner, J.M. Variations in Pattern of Pubertal Changes in Girls. Arch. Dis. Child. 1969, 44, 291–303. [Google Scholar] [CrossRef] [Green Version]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. Update on the 1987 Task Force Report on High Blood Pressure in Children and Adolescents: A Working Group Report from the National High Blood Pressure Education Program. Pediatrics 1996, 98, 649–658. [Google Scholar] [CrossRef]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar] [CrossRef]
- WHO. AnthroPlus for Personal Computers Manual: Software for Assessing Growth of the World’s Children and Adolescents. 2009. Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/application-tools (accessed on 3 February 2022).
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J.; et al. Obesity and the Metabolic Syndrome in Children and Adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar] [CrossRef] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, D.T.; Kailasam, M.T.; Kennedy, B.P.; Ziegler, M.G.; Yanaihara, N.; Parmer, R.J. Early Decline in the Catecholamine Release-Inhibitory Peptide Catestatin in Humans at Genetic Risk of Hypertension. J. Hypertens. 2002, 20, 1335–1345. [Google Scholar] [CrossRef]
- You, Z.; Al Kindi, H.; Abdul-Karim, A.; Barrette, P.O.; Schwertani, A. Blocking the Urotensin II Receptor Pathway Ameliorates the Metabolic Syndrome and Improves Cardiac Function in Obese Mice. FASEB J. 2014, 28, 1210–1220. [Google Scholar] [CrossRef]
- Gartlon, J.; Parker, F.; Harrison, D.C.; Douglas, S.A.; Ashmeade, T.E.; Riley, G.J.; Hughes, Z.A.; Taylor, S.G.; Munton, R.P.; Hagan, J.J.; et al. Central Effects of Urotensin-II Following ICV Administration in Rats. Psychopharmacology 2001, 155, 426–433. [Google Scholar] [CrossRef]
- Guler, E.M.; Gokce, M.; Bacaksiz, A.; Kocyigit, A. Urotensin-II, Oxidative Stress, and Inflammation Increase in Hypertensive and Resistant Hypertensive Patients. Clin. Exp. Hypertens. 2021, 43, 211–216. [Google Scholar] [CrossRef]
- Barrette, P.O.; Schwertani, A.G. A Closer Look at the Role of Urotensin II in the Metabolic Syndrome. Front. Endocrinol. 2012, 3, 165. [Google Scholar] [CrossRef] [Green Version]
- Alicic, D.; Martinovic, D.; Rusic, D.; Zivkovic, P.M.; Hadjina, I.T.; Vilovic, M.; Kumric, M.; Tokic, D.; Supe-Domic, D.; Lupi-Ferandin, S.; et al. Urotensin II Levels in Patients with Inflammatory Bowel Disease. World J. Gastroenterol. 2021, 27, 6142–6153. [Google Scholar] [CrossRef]
- Ong, K.L.; Wong, L.Y.F.; Man, Y.B.; Leung, R.Y.H.; Song, Y.Q.; Lam, K.S.L.; Cheung, B.M.Y. Haplotypes in the Urotensin II Gene and Urotensin II Receptor Gene Are Associated with Insulin Resistance and Impaired Glucose Tolerance. Peptides 2006, 27, 1659–1667. [Google Scholar] [CrossRef] [Green Version]
- Demirpence, M.; Guler, A.; Yilmaz, H.; Sayin, A.; Pekcevik, Y.; Turkon, H.; Colak, A.; Ari, E.M.; Aslanipour, B.; Kocabas, G.U.; et al. Is Elevated Urotensin II Level a Predictor for Increased Cardiovascular Risk in Subjects with Acromegaly? J. Endocrinol. Investig. 2019, 42, 207–215. [Google Scholar] [CrossRef]
- Chen, X.; Yin, L.; Jia, W.; Wang, N.; Xu, C.; Hou, B.; Li, N.; Zhang, L.; Qiang, G.; Yang, X.; et al. Chronic Urotensin-II Administration Improves Whole-Body Glucose Tolerance in High-Fat Diet-Fed Mice. Front. Endocrinol. 2019, 10, 453. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.; Singh, J.; Bala, K.; Singh, J. Association of Resistin (Rs3745367) and Urotensin II (Rs228648 and Rs2890565) Gene Polymorphisms with Risk of Type 2 Diabetes Mellitus in Indian Population. Mol. Biol. Rep. 2020, 47, 9489–9497. [Google Scholar] [CrossRef]
- Sondermeijer, B.; Kompa, A.; Komesaroff, P.; Krum, H. Effect of Exogenous Urotensin-II on Vascular Tone in Skin Microcirculation of Patients with Essential Hypertension. Am. J. Hypertens. 2005, 18, 1195–1199. [Google Scholar] [CrossRef] [Green Version]
- Yi, L.; Gu, Y.H.; Wang, X.L.; An, L.Z.; Xie, X.D.; Shao, W.; Ma, L.Y.; Fang, J.R.; An, Y.D.; Wang, F.; et al. Association of ACE, ACE2 and UTS2 Polymorphisms Wih Essential Hypertension in Han and Dongxiang Populations from North-Western China. J. Int. Med. Res. 2006, 34, 272–283. [Google Scholar] [CrossRef]
- Pawar, R.; Kemp, W.; Roberts, S.; Krum, H.; Yandle, T.; Hardikar, W. Urotensin II Levels Are an Important Marker for the Severity of Portal Hypertension in Children. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 88–92. [Google Scholar] [CrossRef]




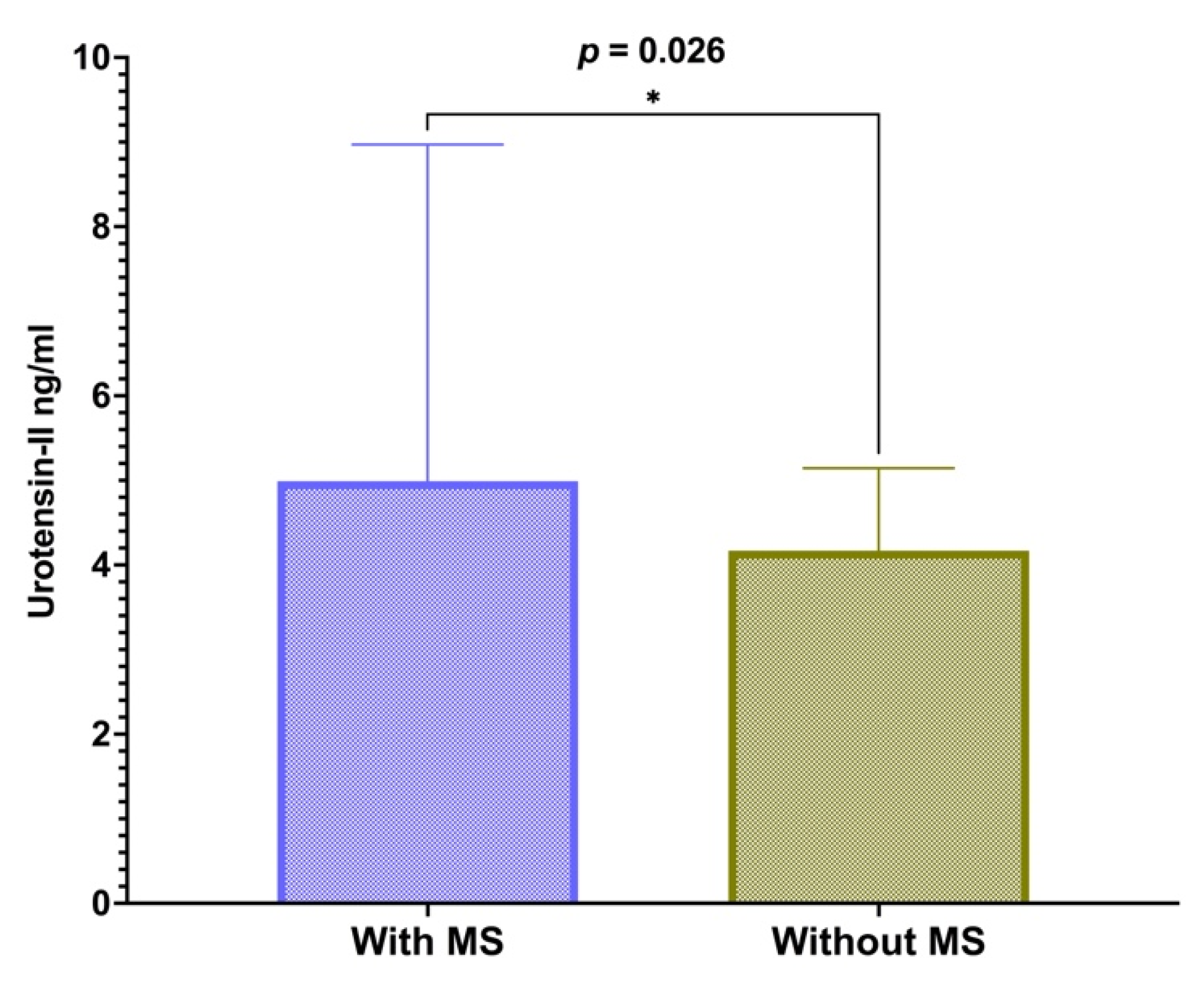{kind=link}
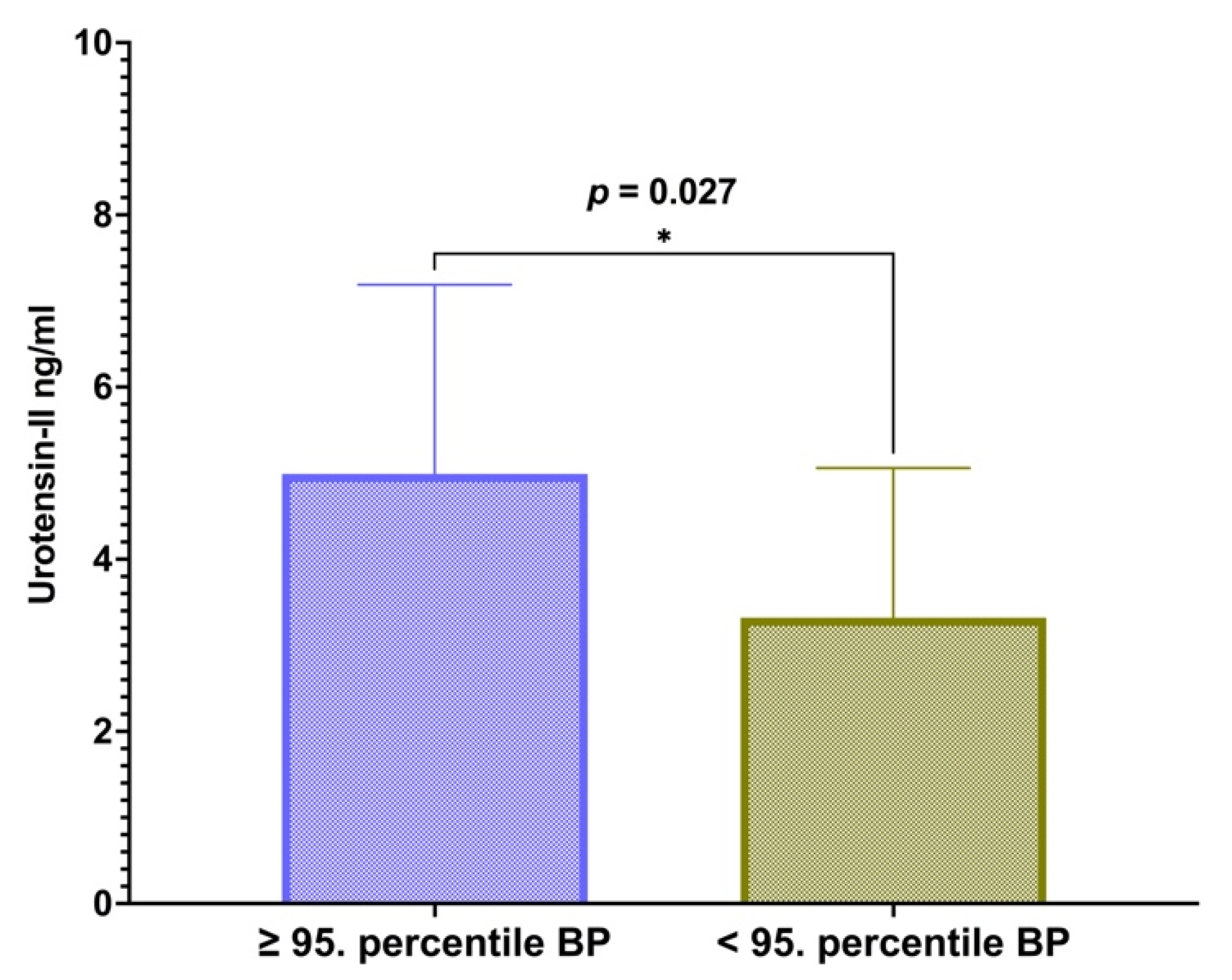{kind=link}
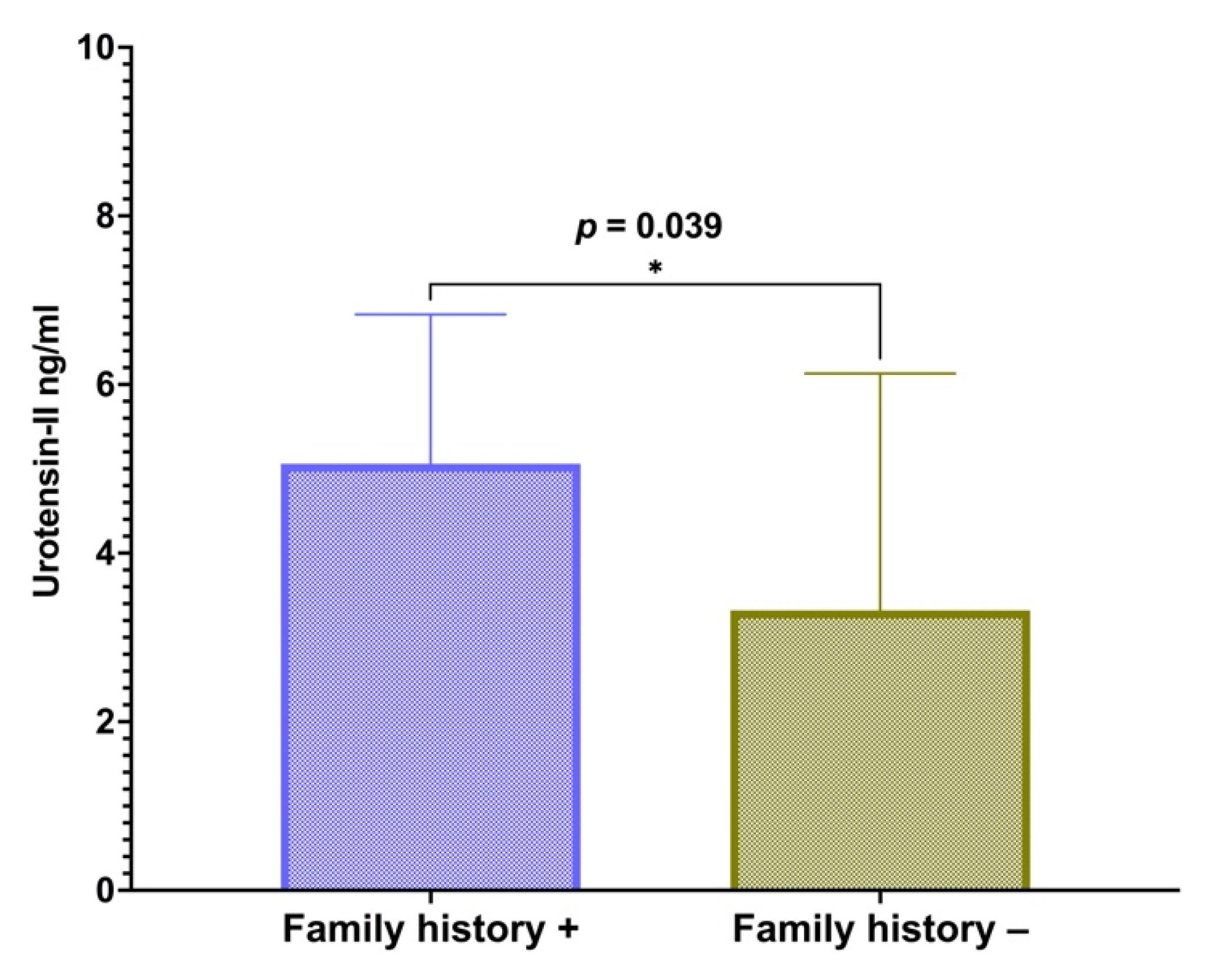{kind=link}
| Factor | With Metabolic Syndrome (n = 26) | Without Metabolic Syndrome (n = 26) | p * |
|---|---|---|---|
| Gender–N (%) | |||
| Male | 13 (50) | 18 (69.2) | 0.158 |
| Female | 13 (50) | 8 (30.8) | |
| Age (years) | 16.42 ± 8.34 | 14.12 ± 2.27 | 0.172 |
| Height (cm) | 170.0 ± 11.72 | 167.6 ± 12.98 | 0.476 |
| Weight (kg) | 91.34 ± 17.74 | 87.54 ± 18.84 | 0.458 |
| BMI (kg/m2) | 31.44 ± 3.92 | 30.7 ± 3.62 | 0.456 |
| BMI z score | 2.82 ± 0.56 | 2.76 ± 0.43 | 0.661 |
| Waist circumference | 103.6 ± 9.25 | 102.3 ± 9.19 | 0.617 |
| Pubertal status—N (%) | |||
| Tanner 1 | 2 (7.7) | 4 (15.4) | 0.793 |
| Tanner 2 | 3 (11.5) | 2 (7.7) | |
| Tanner 3 | 4 (15.4) | 4 (15.4) | |
| Tanner 4 | 8 (30.8) | 10 (38.4) | |
| Tanner 5 | 9 (34.6) | 6 (23.1) |
| Factor | With Metabolic Syndrome (n = 26) | Without Metabolic Syndorme (n = 26) | p * |
|---|---|---|---|
| Total cholesterol (mmol/L) | 4.4 (4.80–3.65) | 4 (4.9–3.78) | 0.487 |
| Triglycerides (mmol/L) | 1.51 ± 0.69 | 1.02 ± 0.38 | 0.003 |
| HDL cholesterol (mmol/L) | 1.00 (1.00–0.90) | 1.20 (1.30–1.10) | <0.001 |
| LDL cholesterol (mmol/L) | 2.70 (3.13–2.20) | 2.50 (3.03–2.00) | 0.190 |
| Fasting glucose (mmol/L) | 5.09 (5.45–4.81) | 4.98 (5.3–4.79) | 0.370 |
| Fasting insulin (mIU/L) | 25.7 (42.23–19.75) | 23.6 (37.23–15.98) | 0.315 |
| HOMA-IR | 5.97 (10.02–4.30) | 5.56 (7.99–3.55) | 0.351 |
| HemoglobinA1c (%) | 5.49 ± 0.36 | 5.43 ± 0.31 | 0.512 |
| SBP (mmHg) | 135.5 ± 15.56 | 124.0 ± 10.01 | 0.003 |
| DBP (mmHg) | 79.50 (85.00–75.00) | 75.00 (80.50–70.00) | 0.120 |
| Factor | Odds Ratio | 95% CI | p * |
|---|---|---|---|
| Age (years) | 0.73 | 0.48–1.09 | 0.142 |
| Sex | 3.59 | 0.77–16.74 | 0.104 |
| BMI (kg/m2) | 1.20 | 0.96–1.50 | 0.102 |
| Urotensin-II (ng/mL) | 1.38 | 1.01–1.92 | 0.046 |
| Positive family history | 3.92 | 0.79–19.43 | 0.095 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simunovic, M.; Jukic, A.; Paradzik, M.; Supe-Domic, D.; Stanisic, L.; Degoricija, M.; Hillestad, A.H.; Skrabic, V.; Bozic, J. The Role of Urotensin-II in Obesity and Metabolic Syndrome in Pediatric Population. Children 2022, 9, 204. https://doi.org/10.3390/children9020204
Simunovic M, Jukic A, Paradzik M, Supe-Domic D, Stanisic L, Degoricija M, Hillestad AH, Skrabic V, Bozic J. The Role of Urotensin-II in Obesity and Metabolic Syndrome in Pediatric Population. Children. 2022; 9(2):204. https://doi.org/10.3390/children9020204
Chicago/Turabian StyleSimunovic, Marko, Andrija Jukic, Martina Paradzik, Daniela Supe-Domic, Lada Stanisic, Marina Degoricija, Anna Hummelvoll Hillestad, Veselin Skrabic, and Josko Bozic. 2022. "The Role of Urotensin-II in Obesity and Metabolic Syndrome in Pediatric Population" Children 9, no. 2: 204. https://doi.org/10.3390/children9020204