
Intra-Abdominal Hypertension and Compartment Syndrome after Pediatric Liver Transplantation: Incidence, Risk Factors and Outcome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Cohort
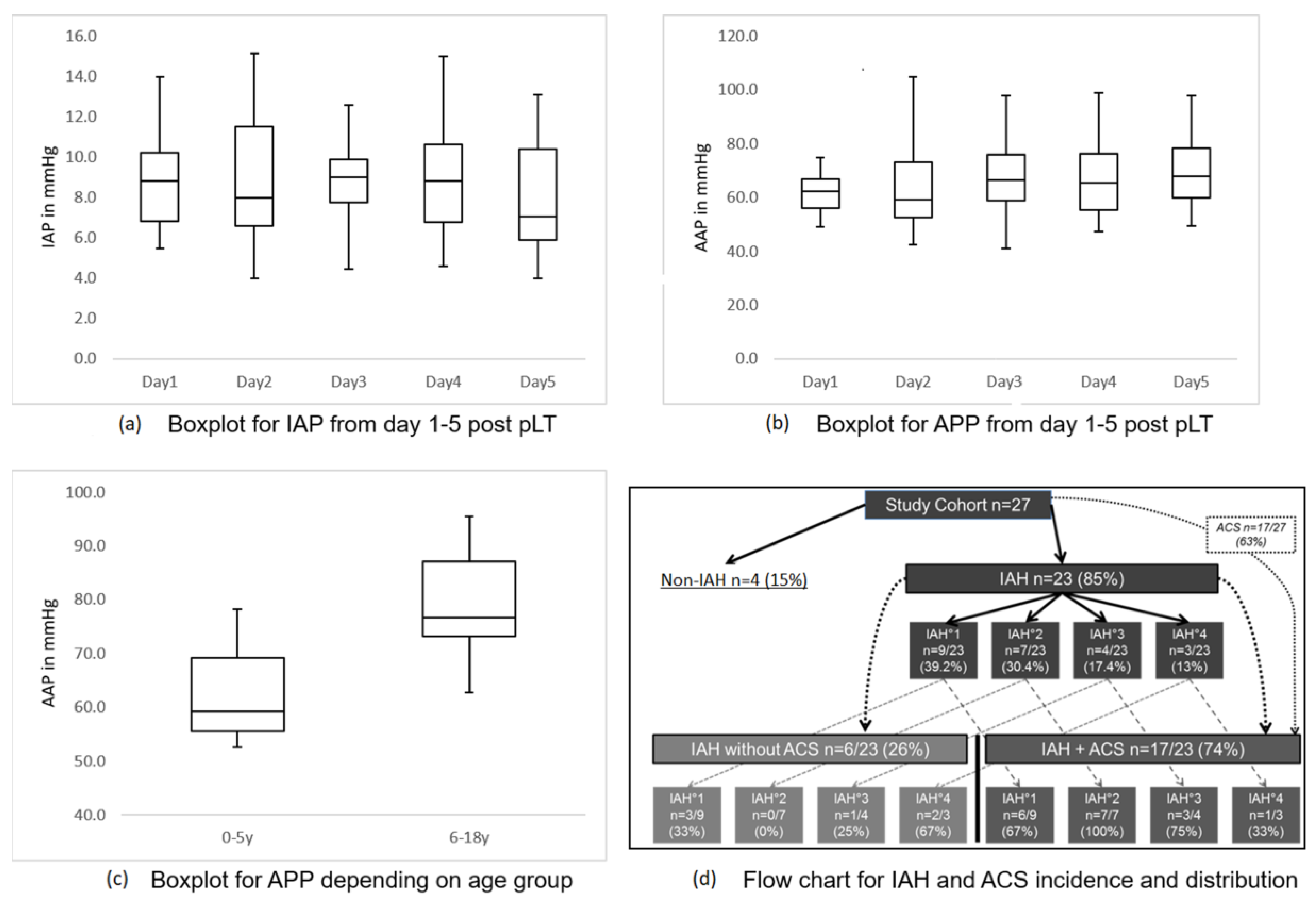
3.2. Intra-abdominal Pressure and Abdominal Perfusion Pressure
3.3. Incidence of Intra-abdominal Hypertension and Acute Compartment Syndrome
3.4. Risk Factors for IAH and ACS
3.5. Analysis of Clinical, Laboratory and Vital Parameters, Depending on the Occurrence of IAH or ACS
3.6. Ultrasound Analysis of Liver Perfusion
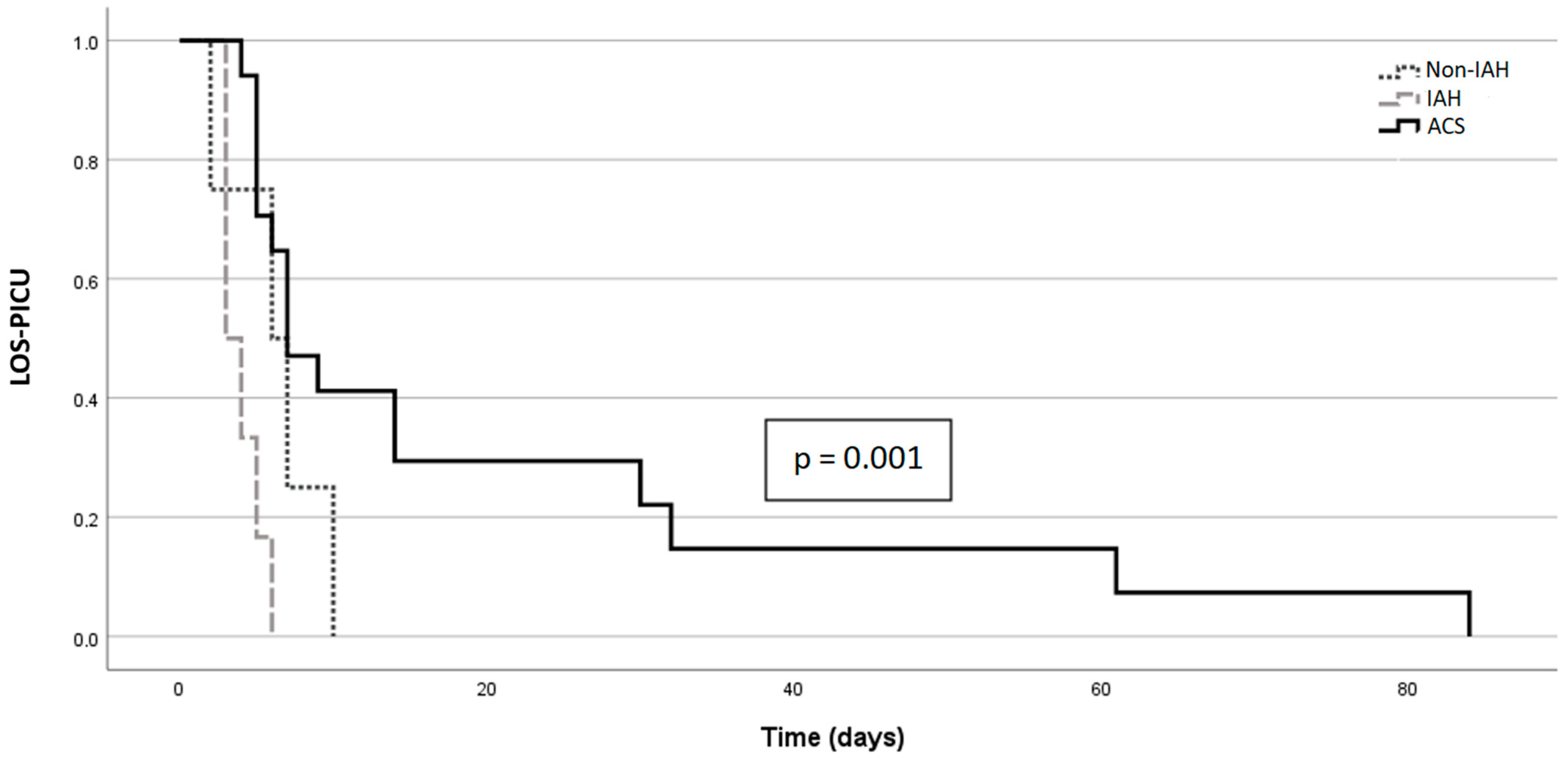
3.7. IAH/ACS and Outcome
3.8. Analysis of Microcirculation Parameters, Depending on the Occurrence of IAH or ACS
4. Discussion
4.1. IAP, APP, IAH, ACS and Their Risk Factors in Our Cohort
4.2. ACS and PAWC/SAWC
4.3. IAH/ACS and Outcome
4.4. Microcirculation
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leiskau, C.; Junge, N.; Pfister, E.-D.; Goldschmidt, I.; Mutschler, F.; Laue, T.; Ohlendorf, J.; Nasser, H.; Beneke, J.; Richter, N.; et al. Recipient-Specific Risk Factors Impairing Patient and Graft Outcome after Pediatric Liver Transplantation—Analysis of 858 Transplantations in 38 Years. Children 2021, 8, 641. [Google Scholar] [CrossRef] [PubMed]
- Pfister, E.-D.; Karch, A.; Adam, R.; Polak, W.G.; Karam, V.; Mirza, D.; O’Grady, J.; Klempnauer, J.; Reding, R.; Kalicinski, P.; et al. Predictive Factors for Survival in Children Receiving Liver Transplants for Wilson’s Disease: A Cohort Study Using European Liver Transplant Registry Data. Liver Transplant. 2018, 24, 1186–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biancofiore, G.; Bindi, M.L.; Romanelli, A.; Boldrini, A.; Consani, G.; Bisà, M.; Filipponi, F.; Vagelli, A.; Mosca, F. Intra-abdominal pressure monitoring in liver transplant recipients: A prospective study. Intensiv. Care Med. 2003, 29, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Bressan, A.K.; Ball, C.G. Intra-abdominal hypertension and abdominal compartment syndrome in acute pancreatitis, hepato-pancreato-biliary operations and liver transplantation. Anaesthesiol. Intensiv. Ther. 2017, 49, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Deindl, P.; Wagner, J.; Herden, U.; Schulz-Jürgensen, S.; Schild, R.; Vettorazzi, E.; Bergers, M.; Keck, M.; Singer, D.; Fischer, L.; et al. Monitoring intra-abdominal pressure after liver transplantation in children. Pediatr. Transplant. 2019, 23, e13565. [Google Scholar] [CrossRef] [Green Version]
- Kathemann, S.; Dohna-Schwake, C.; Paul, A.; Hoyer, P.F.; Gerner, P. Intraabdominal Pressure Monitoring in Pediatric Liver Transplant Recipients: A Useful Tool for the Detection of Abdominal Compartment Syndrome. Transplantation 2012, 94, 665. [Google Scholar] [CrossRef]
- Kirkpatrick, A.W.; The Pediatric Guidelines Sub-Committee for the World Society of the Abdominal Compartment Syndrome; Roberts, D.J.; De Waele, J.; Jaeschke, R.; Malbrain, M.L.N.G.; De Keulenaer, B.; Duchesne, J.; Bjorck, M.; Leppaniemi, A.; et al. Intra-abdominal hypertension and the abdominal compartment syndrome: Updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensiv. Care Med. 2013, 39, 1190–1206. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Tao, S.; Gu, B.; Huang, H.; Zhong, Z.; Shi, J.; Guan, X.; Tang, W. Intra-abdominal Pressure Has a Good Predictive Power for 28-Day Mortality: A Prospective Observational Study Conducted in Critically Ill Children. Front. Pediatr. 2020, 8, 567876. [Google Scholar] [CrossRef]
- Santa-Teresa, P.; Muñoz, J.; Montero, I.; Zurita, M.; Tomey, M.; Álvarez-Sala, L.; García, P. Incidence and prognosis of intra-abdominal hypertension in critically ill medical patients: A prospective epidemiological study. Ann. Intensiv. Care 2012, 2 (Suppl. 1), S3. [Google Scholar] [CrossRef] [Green Version]
- Steinau, G.; Kaussen, T.; Bolten, B.; Schachtrupp, A.; Neumann, U.P.; Conze, J.; Boehm, G. Abdominal compartment syndrome in childhood: Diagnostics, therapy and survival rate. Pediatr. Surg. Int. 2010, 27, 399–405. [Google Scholar] [CrossRef]
- Divarci, E.; Karapinar, B.; Yalaz, M.; Ergun, O.; Celik, A. Incidence and prognosis of intraabdominal hypertension and abdominal compartment syndrome in children. J. Pediatr. Surg. 2016, 51, 503–507. [Google Scholar] [CrossRef] [PubMed]
- di Natale, A.; Moehrlen, U.; Neeser, H.R.; Zweifel, N.; Meuli, M.; Mauracher, A.A.; Brotschi, B.; Tharakan, S.J. Abdominal compartment syndrome and decompressive laparotomy in children: A 9-year single-center experience. Pediatr. Surg. Int. 2020, 36, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Carlotti, A.P.C.P.; Carvalho, W.B. Abdominal compartment syndrome: A review. Pediatr. Crit. Care Med. 2009, 10, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Chadi, S.A.; Abdo, H.; Bihari, A.; Parry, N.; Lawendy, A.-R. Hepatic microvascular changes in rat abdominal compartment syndrome. J. Surg. Res. 2015, 197, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriadis, E.; Kotzampassi, K. Hepatic microcirculation after continuous 7-day elevated intra-abdominal pressure in cirrhotic rats. Hepatol. Res. 2005, 32, 96–100. [Google Scholar] [CrossRef]
- Singh, Y.; Villaescusa, J.U.; da Cruz, E.M.; Tibby, S.M.; Bottari, G.; Saxena, R.; Guillén, M.; Herce, J.L.; Di Nardo, M.; Cecchetti, C.; et al. Recommendations for hemodynamic monitoring for critically ill children—Expert consensus statement issued by the cardiovascular dynamics section of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC). Crit. Care 2020, 24, 620. [Google Scholar] [CrossRef] [PubMed]
- Scholbach, T.; Dimos, I.; Scholbach, J. A New Method of Color Doppler Perfusion Measurement via Dynamic Sonographic Signal Quantification in Renal Parenchyma. Nephron Physiol. 2004, 96, 99. [Google Scholar] [CrossRef]
- Scholbach, T.; Girelli, E.; Scholbach, J. Dynamic Tissue Perfusion Measurement: A Novel Tool in Follow-Up of Renal Transplants. Transplantation 2005, 79, 1711–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neto, J.S.; Pugliese, R.; Fonseca, E.A.; Vincenzi, R.; Pugliese, V.; Candido, H.; Stein, A.B.; Benavides, M.; Ketzer, B.; Teng, H.; et al. Four hundred thirty consecutive pediatric living donor liver transplants: Variables associated with posttransplant patient and graft survival. Liver Transplant. 2012, 18, 577–584. [Google Scholar] [CrossRef]
- Gaies, M.G.; Gurney, J.G.; Yen, A.H.; Napoli, M.L.; Gajarski, R.J.; Ohye, R.G.; Charpie, J.R.; Hirsch, J.C. Vasoactive–inotropic score as a predictor of morbidity and mortality in infants after cardiopulmonary bypass. Pediatr. Crit. Care Med. 2010, 11, 234–238. [Google Scholar] [CrossRef]
- Pollack, M.M.; Patel, K.M.; Ruttimann, U.E. PRISM III: An updated pediatric risk of mortality score. Crit. Care Med. 1996, 24, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Kron, I.L.; Harman, P.K.; Nolan, S.P. The Measurement of Intra-abdominal Pressure as a Criterion for Abdominal Re-exploration. Ann. Surg. 1984, 199, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Kaussen, T.; Gutting, M.; Lasch, F.; Boethig, D.; von Gise, A.; Dingemann, J.; Koeditz, H.; Jack, T.; Sasse, M.; Beerbaum, P.; et al. Continuous intra-gastral monitoring of intra-abdominal pressure in critically ill children: A validation study. Intensiv. Care Med. Exp. 2021, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.L.N.G. Different techniques to measure intra-abdominal pressure (IAP): Time for a critical re-appraisal. Intensiv. Care Med. 2004, 30, 357–371. [Google Scholar] [CrossRef] [PubMed]
- Balogh, Z.; Jones, F.; D’Amours, S.; Parr, M.; Sugrue, M. Continuous intra-abdominal pressure measurement technique. Am. J. Surg. 2004, 188, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Kaussen, T.; Steinau, G.; Srinivasan, P.K.; Otto, J.; Sasse, M.; Staudt, F.; Schachtrupp, A. Recognition and management of abdominal compartment syndrome among German pediatric intensivists: Results of a national survey. Ann. Intensiv. Care 2012, 2 (Suppl. 1), S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, B.; Giroir, B.; Randolph, A. International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr. Crit. Care Med. 2005, 6, 2–8. [Google Scholar] [CrossRef] [Green Version]
- Deeg, K.-H.; Rupprecht, T.; Hofbeck, M. Doppler Sonography in Infancy and Childhood; Springer: Heidelberg, Germany, 2015; ISBN 978-3-319-03505-5. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New Equations to Estimate GFR in Children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, M.S.; Nacul, F.E.; Malbrain, M.L.; Silva, R.C.; Lobo, F.R.; Oliveira, N.E.; da Silva, R.F.; Lobo, S.M. Intra-abdominal hypertension, fluid balance, and adverse outcomes after orthotopic liver transplantation. J. Crit. Care 2021, 62, 271–275. [Google Scholar] [CrossRef]
- Cresswell, A.B.; Jassem, W.; Srinivasan, P.; A Prachalias, A.; Sizer, E.; Burnal, W.; Auzinger, G.; Muiesan, P.; Rela, M.; Heaton, N.D.; et al. The effect of body position on compartmental intra-abdominal pressure following liver transplantation. Ann. Intensiv. Care 2012, 2 (Suppl. 1), S12. [Google Scholar] [CrossRef] [Green Version]
- Biancofiore, G.; Bindi, M.L.; Romanelli, A.M.; Bisà, M.; Boldrini, A.; Consani, G.; Filipponi, F.; Mosca, F. Postoperative Intra-abdominal Pressure and Renal Function After Liver Transplantation. Arch. Surg. 2003, 138, 703–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biancofiore, G.; Bindi, L.; Romanelli, A.M.; Bisà, M.; Boldrini, A.; Consani, G.; Danella, A.; Urbani, L.; Filipponi, F.; Mosca, F. Renal failure and abdominal hypertension after liver transplantation: Determination of critical intra-abdominal pressure. Liver Transplant. 2002, 8, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Horoz, O.O.; Yildizdas, D.; Sari, Y.; Unal, I.; Ekinci, F.; Petmezci, E. The relationship of abdominal perfusion pressure with mortality in critically ill pediatric patients. J. Pediatr. Surg. 2019, 54, 1731–1735. [Google Scholar] [CrossRef] [PubMed]
- Cheatham, M.L.; White, M.W.; Sagraves, S.G.; Johnson, J.L.; Block, E.F.J. Abdominal Perfusion Pressure: A Superior Parameter in the Assessment of Intra-abdominal Hypertension. J. Trauma 2000, 49, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Gül, F.; Sayan, I.; Kasapoglu, U.S.; Erol, D.; Arslantaş, M.K.; Cinel, I.; Aykaç, Z. Abdominal perfusion pressure is superior from intra-abdominal pressure to detect deterioration of renal perfusion in critically Ill patients. Turk. J. Trauma Emerg. Surg. 2019, 25, 561–566. [Google Scholar] [CrossRef]
- Malbrain, M.L.N.G.; Cheatham, M.L.; Kirkpatrick, A.; Sugrue, M.; Parr, M.; De Waele, J.; Balogh, Z.; Leppäniemi, A.; Olvera, C.; Ivatury, R.; et al. Results from the International Conference of Experts on Intra-abdominal Hypertension and Abdominal Compartment Syndrome. I. Definitions. Intensiv. Care Med. 2006, 32, 1722–1732. [Google Scholar] [CrossRef] [PubMed]
- Vidal, M.G.; Weisser, J.R.; Gonzalez, F.; Toro, M.A.; Loudet, C.; Balasini, C.; Canales, H.; Reina, R.; Estenssoro, E. Incidence and clinical effects of intra-abdominal hypertension in critically ill patients. Crit. Care Med. 2008, 36, 1823–1831. [Google Scholar] [CrossRef]
- Perova-Sharonova, V.; Albokrinov, A.; Fesenko, U.; Gutor, T. Effect of intraabdominal hypertension on splanchnic blood flow in children with appendicular peritonitis. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Malbrain, M.L.; De Waele, J.J.; De Keulenaer, B.L. What every ICU clinician needs to know about the cardiovascular effects caused by abdominal hypertension. Anaesthesiol. Intensiv. Ther. 2015, 47, 388–399. [Google Scholar] [CrossRef]
- Zhao, Z.; Guo, Z.; Yin, Z.; Qiu, Y.; Zhou, B. Gut Microbiota Was Involved in the Process of Liver Injury During Intra-Abdominal Hypertension. Front. Physiol. 2021, 12, 790182. [Google Scholar] [CrossRef]
- Horoz, Ö.Ö.; Aslan, N.; Yildizdaş, D.; Çoban, Y.; Sertdemir, Y.; Al-Subu, A. Somatic regional oxygen saturation as an early marker of intra-abdominal hypertension in critically ill children: A pilot study. Turk. J. Med. Sci. 2020, 50, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Ghidini, F.; Benetti, E.; Zucchetta, P.; Amigoni, A.; Gamba, P.; Castagnetti, M. Transcutaneous near-infrared spectroscopy (NIRS) for monitoring kidney and liver allograft perfusion. Int. J. Clin. Pract. 2021, 75, e14034. [Google Scholar] [CrossRef] [PubMed]
- Colle, I.; Van Vlierberghe, H.; Troisi, R.; De Hemptinne, B. Transplanted liver: Consequences of denervation for liver functions. Anat. Rec. 2004, 280, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Civantos, D.P.; Cantero, A.M.; Marcos, M.R.; Morillas, F.F.; Arias, M.C.; Seijas, H.F. Utility of Basal Regional Oximetry as an Early Predictor of Graft Failure After Liver Transplant. Transplant. Proc. 2019, 51, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Shiba, J.; Satoh, M.; Taira, K.; Niwa, Y.; Inoue, S.; Mizuta, K.; Takeuchi, M. Near-infrared spectroscopy might be a useful tool for predicting the risk of vascular complications after pediatric liver transplants: Two case reports. Pediatr. Transplant. 2018, 22, e13089. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Non-IAH | IAH | ACS | Total | Kruskal–Wallis Test p-Value | |
|---|---|---|---|---|---|
| Patients (n =) | 4 | 6 | 17 | 27 | |
| Age (years) * | 4.00 [±6.68] | 8.67 [±7.20] | 4.76 [±6.17] | 5.52 [±6.45] | 0.68 |
| Sex distribution (% girls) | 75% | 66% | 53% | 59% | 0.67 |
| Weight (kg) * | 14.94 [±13.38] | 45.02 [±36.41] | 21.62 [±21.11] | 25.83 [±23.87] | 0.62 |
| PRISM III Score * On admission | 14.25 [±4.11] | 14.83 [±5.19] | 18.00 [±25.78] | 16.74 [±6.23] | 0.45 |
| Previously transplanted | 0 | 0 | 2 | 2 | 0.54 |
| Total Number in the Study Cohort | Study Cohort in Percentages (n = 27) | All IAH Patients in Percentages (n = 23) | All ACS Patients in Percentages (n = 17) | |
|---|---|---|---|---|
| Renal dysfunction * | 15 | 56% | 65% | 88% |
| Cardiovascular dysfunction * | 11 | 41% | 48% | 65% |
| Pulmonary dysfunction * | 8 | 30% | 35% | 47% |
| Analyzed Parameter/Independent Variable | Coefficient B (Unstandardized) | 95% CI | p-Value |
|---|---|---|---|
| Cold ischemia time (per hour) | 0.26 | 0.01–0.50 | 0.044 |
| Abdominal wall closure (primary vs. staged) | −0.65 | −2.52–1.22 | 0.479 |
| Type of arteria hepatic anastomosis (non-aortal vs. aortal) | 2.51 | 0.74–4.28 | 0.008 |
| Patients’ liver to graft liver weight ratio | 1.32 | −0.13–2.77 | 0.073 |
| Analyzed Parameter/Independent Variable | Coefficient B (Unstandardized) | 95% CI | p-Value |
|---|---|---|---|
| Cold ischemia time (per hour) | 0.89 | −0.246–2.01 | 0.116 |
| Abdominal wall closure (primary vs. staged) | −17.40 | −25.83–−8.97 | <0.001 |
| Type of arteria hepatic anastomosis (nonaortal vs. aortal) | −5.68 | −13.70–2.33 | 0.156 |
| Patients’ liver–to–graft liver weight ratio | 2.63 | −3.95–9.21 | 0.416 |
| Analyzed Parameter/Independent Variable | Odds Ratio | 95% CI for Odds Ratio | p-Value |
|---|---|---|---|
| Abdominal wall closure (primary vs. staged) | 35.82 | 1.64–784.94 | 0.023 |
| Type of arteria hepatic anastomosis (aortal vs. nonaortal) | 1.21 | 0.10–14.32 | 0.879 |
| Patients’ liver–to–graft liver weight ratio | 1.00 | 1.00–1.00 | 0.819 |
| Cold ischemia time per hour | 1.57 | 1.06–2.33 | 0.023 |
| No IAH | IAH | ACS | Kruskal–Wallis Test p-Value | Mann–Whitney U Test for IAH vs. ACS p-Value | |
|---|---|---|---|---|---|
| Patients (n=) | 4 | 6 | 17 | ||
| PRISM III-Score at discharge (mean [±standard deviation]) | 7.75 [±3.00] | 7.50 [±3.21] | 8.06 [±7.81] | 0.84 | |
| Length of stay in PICU in days (mean [±standard deviation]) | 6.25 [±3.30] | 4.00 [±1.27] | 18.94 [±22.5] | 0.01 | IAH vs. ACS p = 0.003 |
| Length of stay in hospital in days (mean [±standard deviation]) | 35.75 [±14.80] | 29.17 [±6.08] | 43.53 [+23.87] | 0.24 | |
| Length of postoperative invasive ventilation in hours (mean [±standard deviation]) | 73.75 [±55.14] | 17.00 [±11.76] | 201 [±307.73] | 0.02 | IAH vs. ACS p = 0.004 |
| Necessity for early retransplantation | 0 | 0 | 3 (18%) | 0.38 | |
| Deceased | 0 | 0 | 1 (9%) | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Junge, N.; Artmann, A.; Richter, N.; Vondran, F.W.R.; Böthig, D.; Sasse, M.; Köditz, H.; Baumann, U.; Beerbaum, P.; Kaussen, T. Intra-Abdominal Hypertension and Compartment Syndrome after Pediatric Liver Transplantation: Incidence, Risk Factors and Outcome. Children 2022, 9, 1993. https://doi.org/10.3390/children9121993
Junge N, Artmann A, Richter N, Vondran FWR, Böthig D, Sasse M, Köditz H, Baumann U, Beerbaum P, Kaussen T. Intra-Abdominal Hypertension and Compartment Syndrome after Pediatric Liver Transplantation: Incidence, Risk Factors and Outcome. Children. 2022; 9(12):1993. https://doi.org/10.3390/children9121993
Chicago/Turabian StyleJunge, Norman, Annika Artmann, Nicolas Richter, Florian W. R. Vondran, Dietmar Böthig, Michael Sasse, Harald Köditz, Ulrich Baumann, Philipp Beerbaum, and Torsten Kaussen. 2022. "Intra-Abdominal Hypertension and Compartment Syndrome after Pediatric Liver Transplantation: Incidence, Risk Factors and Outcome" Children 9, no. 12: 1993. https://doi.org/10.3390/children9121993