

Infodemiology of RSV in Italy (2017–2022): An Alternative Option for the Surveillance of Incident Cases in Pediatric Age?

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Epidemiological Data
2.2. Internet Search Volumes
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
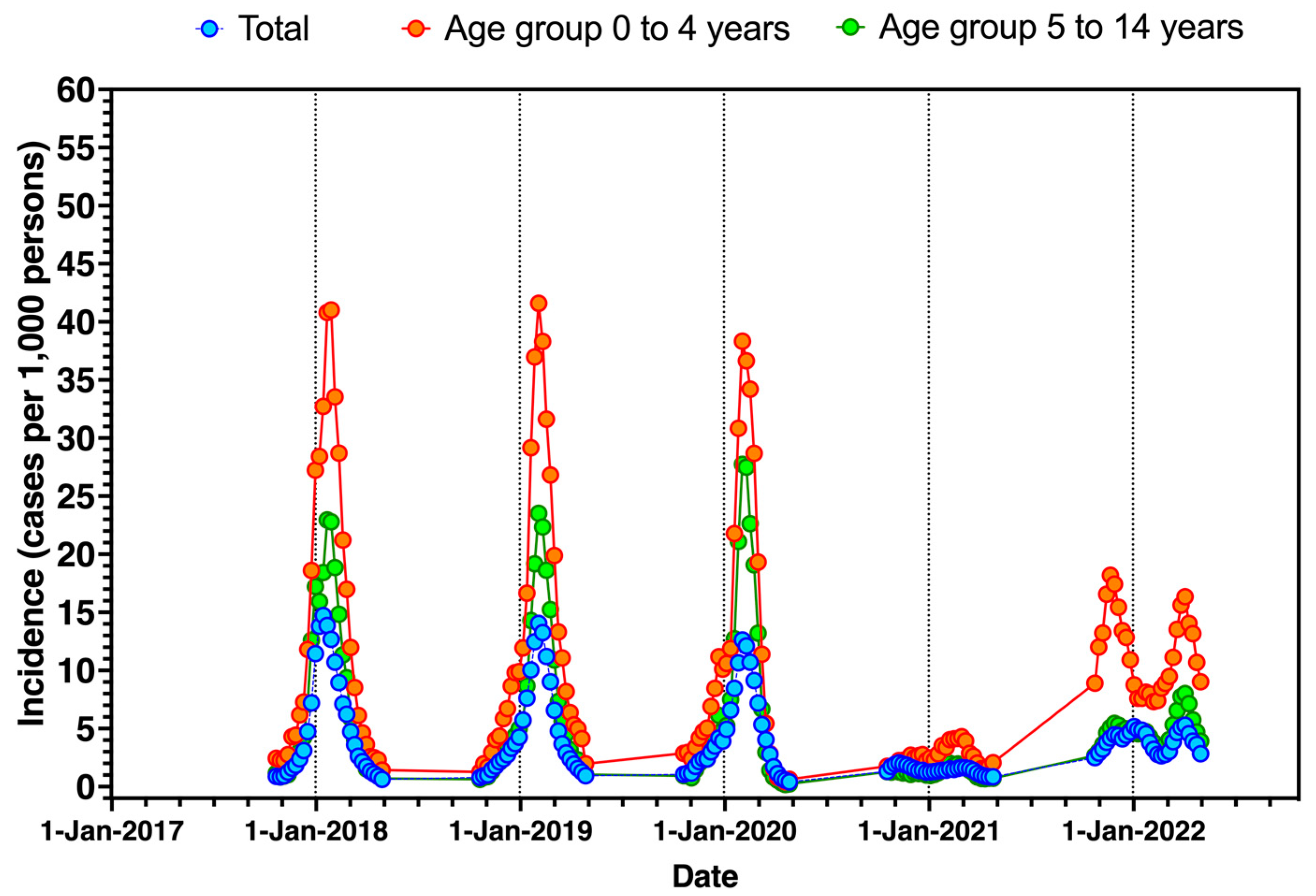
3.1. Incidence of ILI in Italy
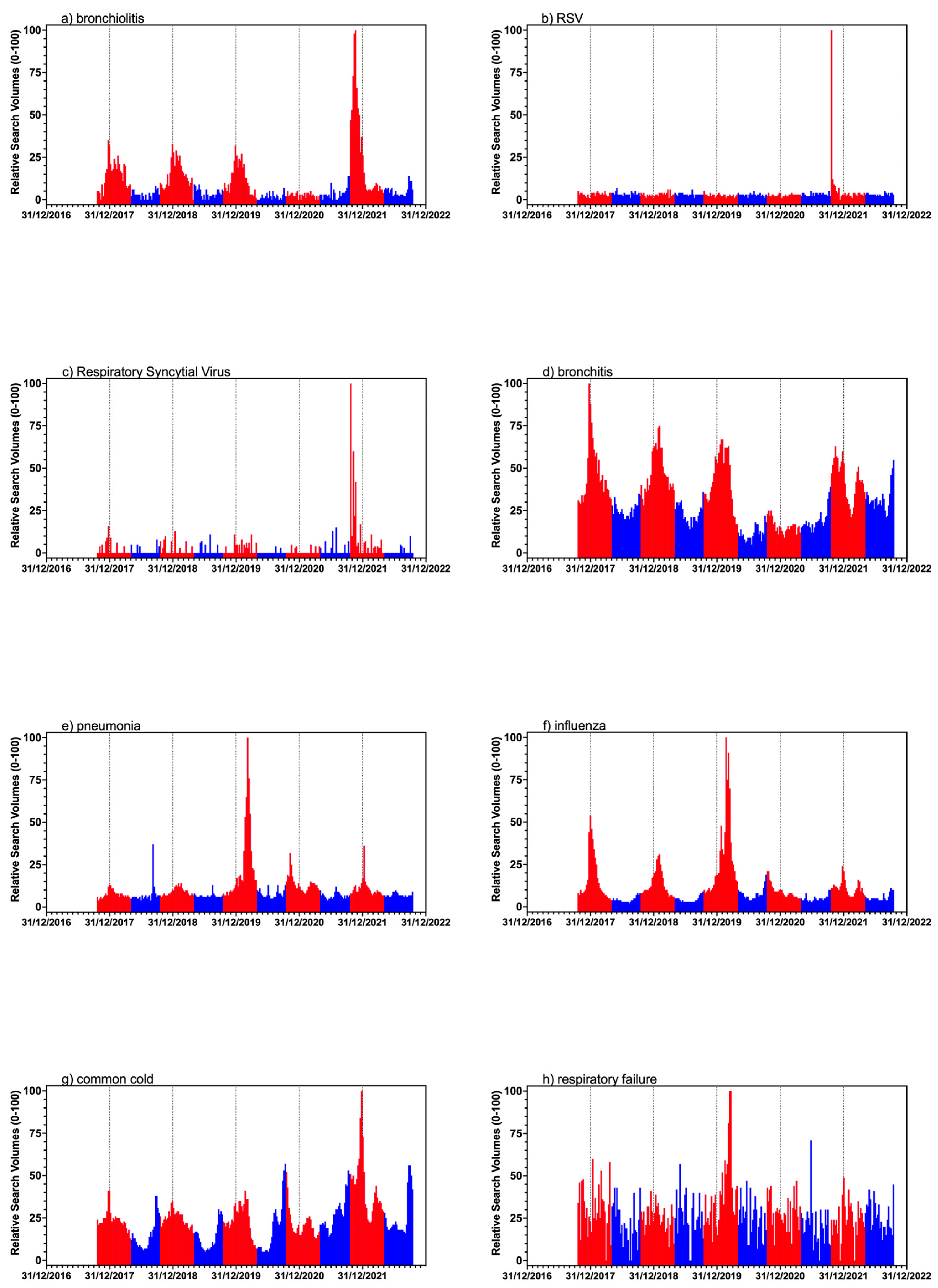
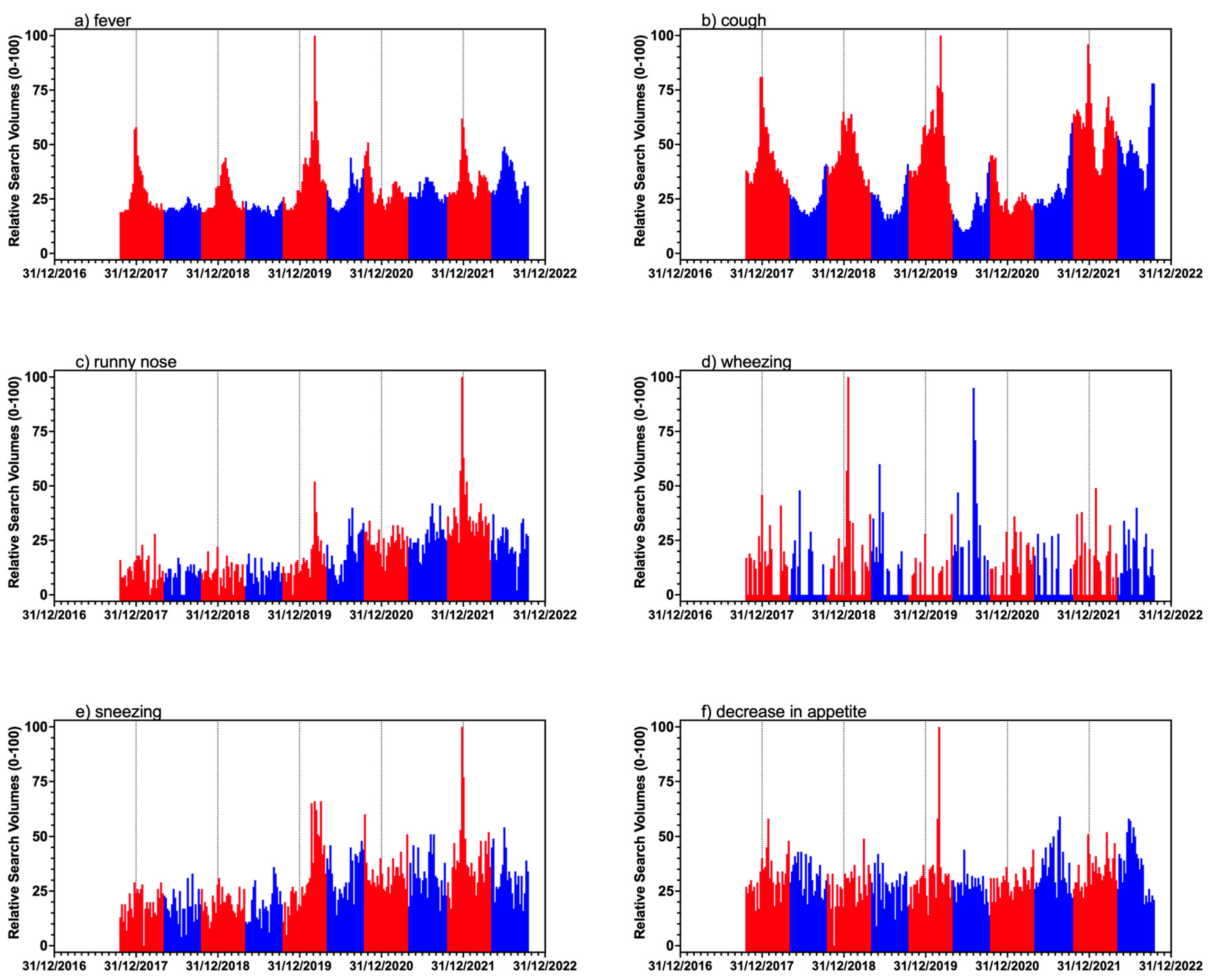
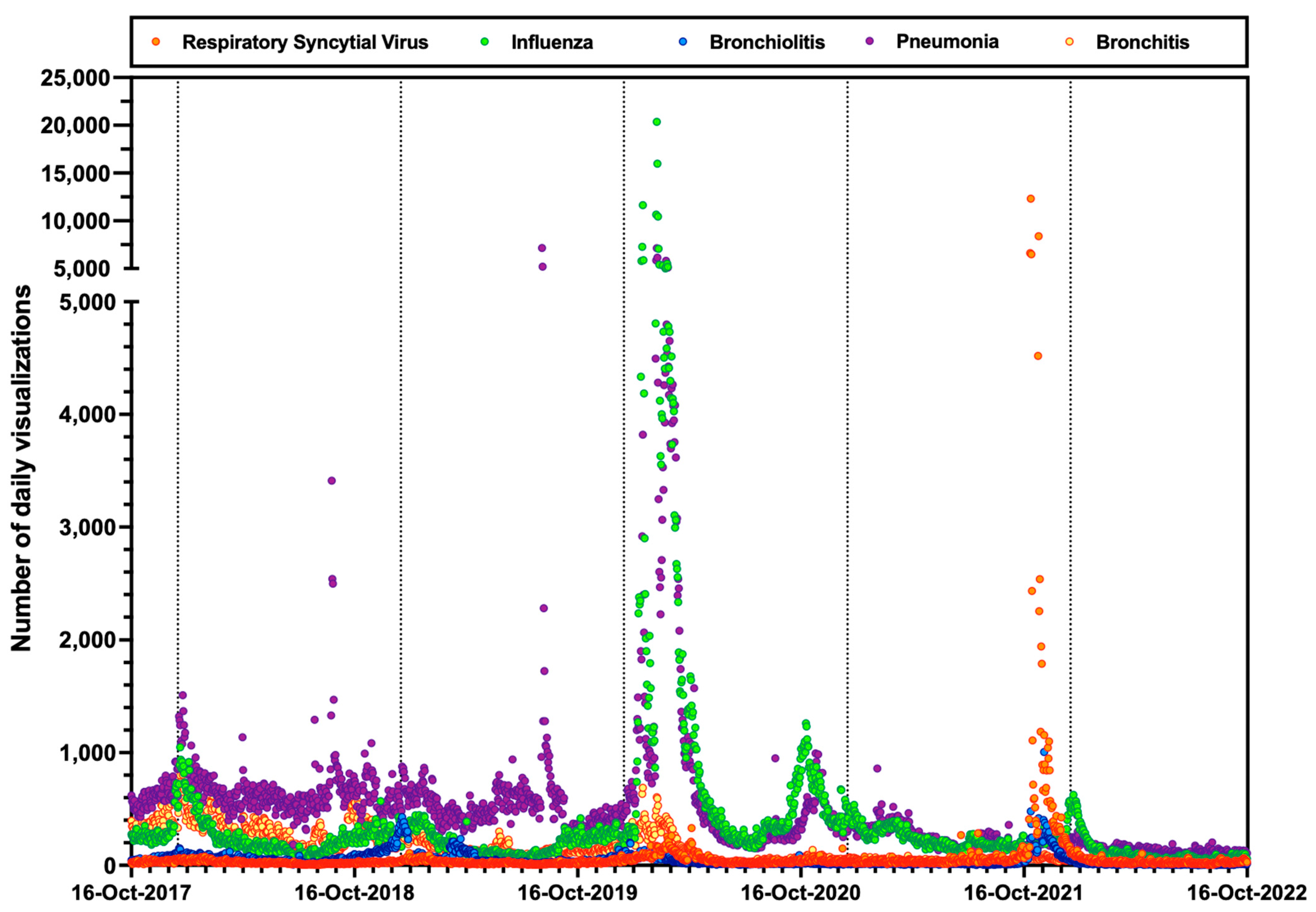
3.2. RSV-Related Queries
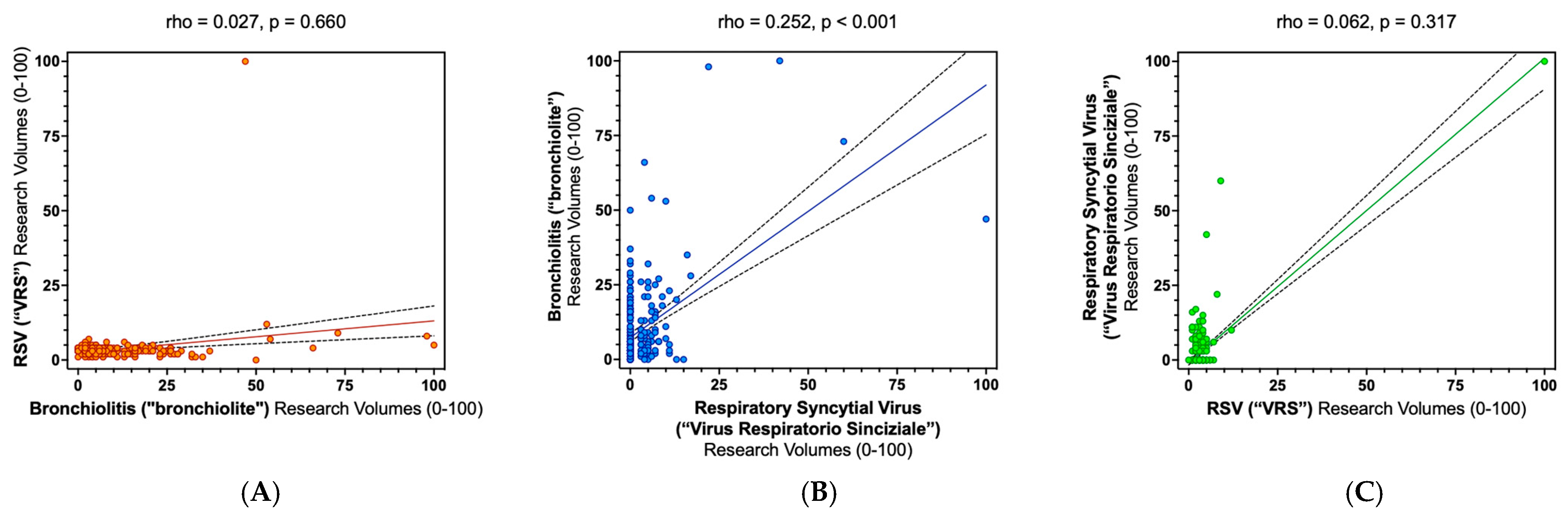
3.3. Correlation between Research Terms and Estimates for ILI
3.4. Regression Analysis
- Model 1 (Total population) included the ILI rates as outcome variables, and assessed the search volumes for brochiolitis, Respiratory Syncytial virus, Bronchitis, Pneumonia, fever, decrease in appetite, cough, influenza, and all of the assessed web searches from Wikipedia as explanatory variables.
- Model 2 (age 0–4 years) included all of the aforementioned explanatory variables, with the exception of the search volumes Pneumonia; similarly, the estimates for the Wikipedia visualizations for influenza and Pneumonia were excluded.
- Model 3 (age 5–14 years) included all of the explanatory variables included in model 1 with the exception of the daily visualization rates for Pneumonia.
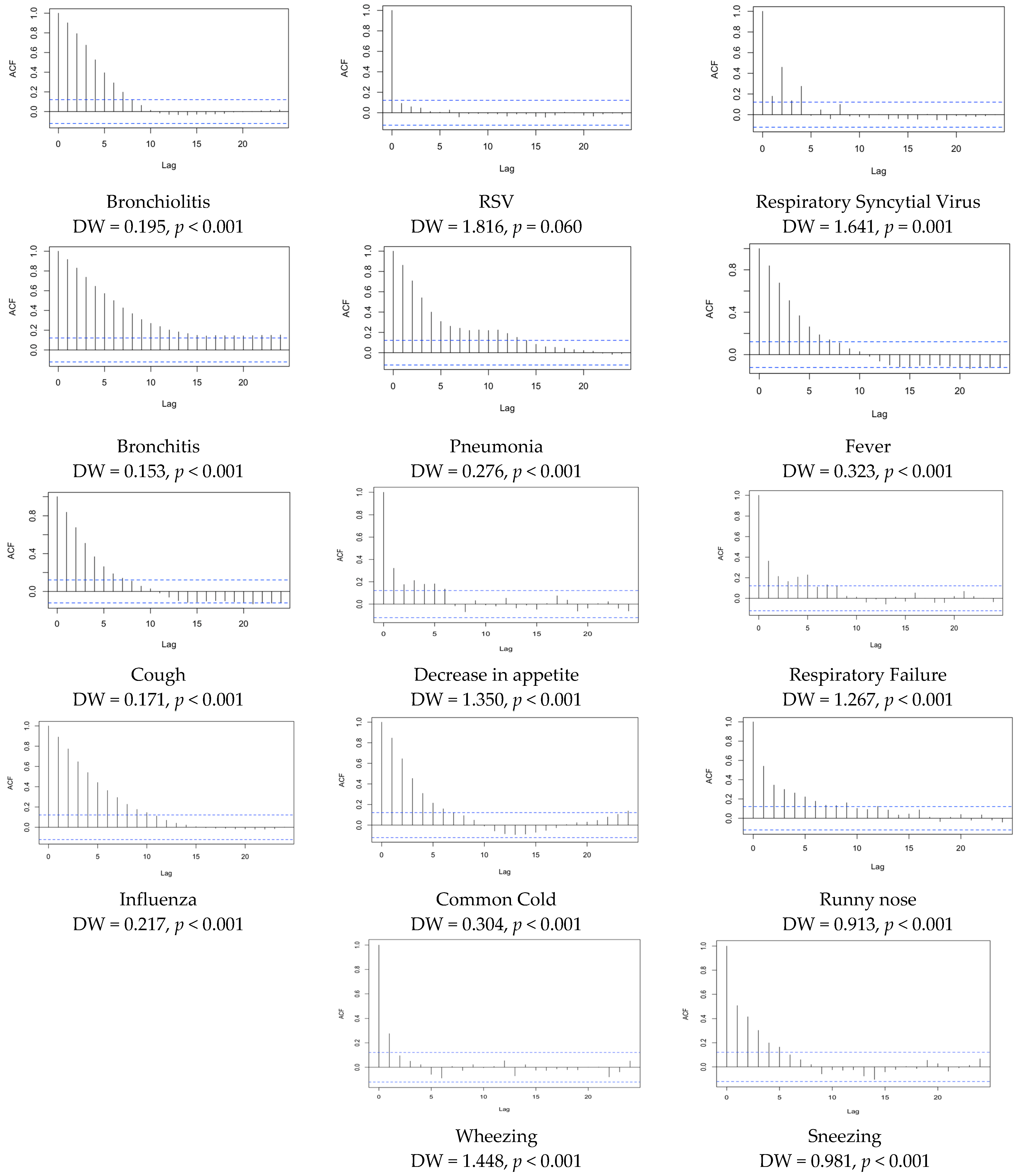
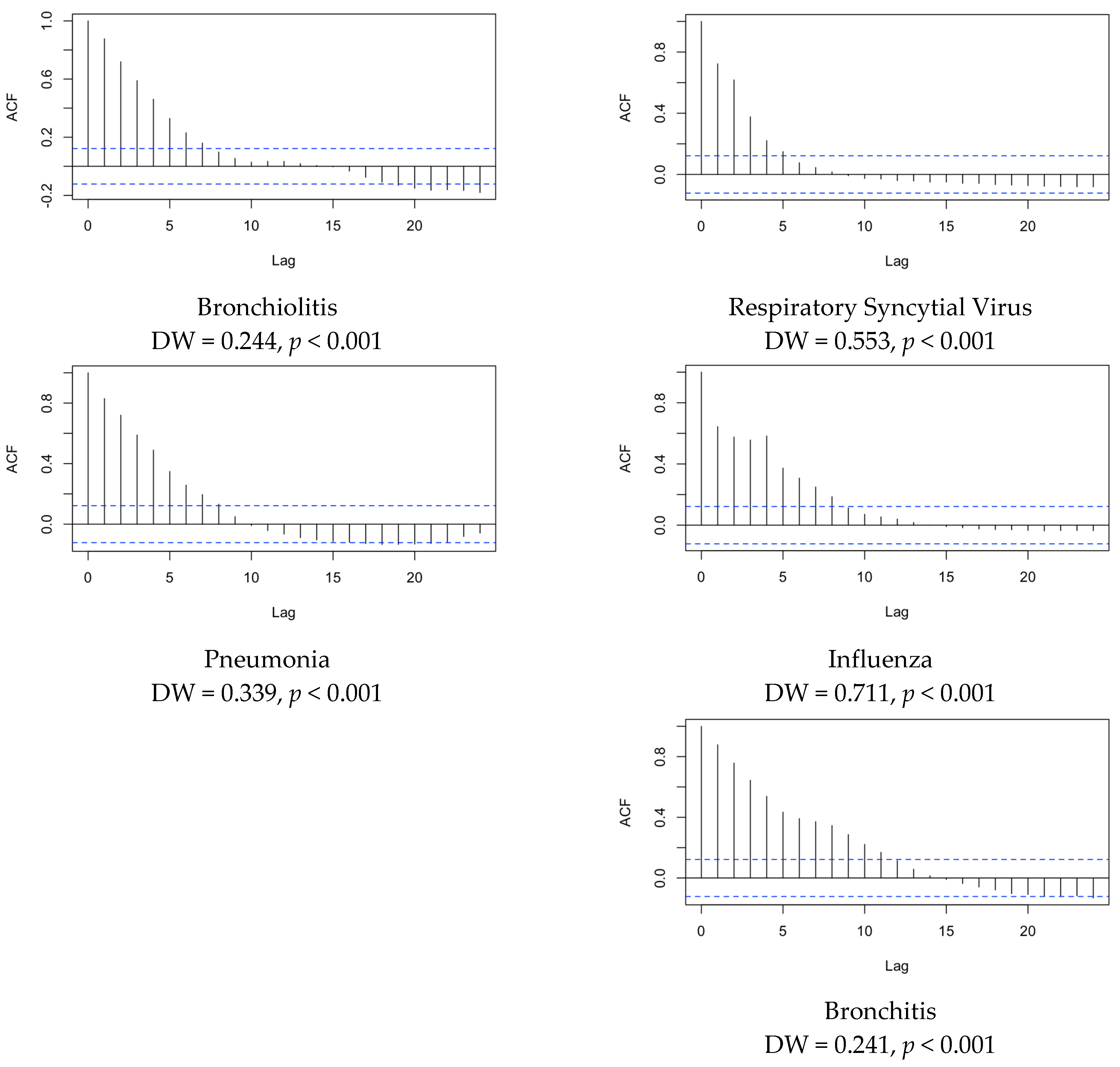
3.5. Time Series
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Term (Italian) | Daily Visualizations Spearman’s ρ, (p Value) | ||
|---|---|---|---|
| Bronchiolitis | Respiratory Syncytial Virus | RSV | |
| Bronchitis | 0.829 (p < 0.001) | 0.276 (p < 0.001) | 0.065 (p = 0.294) |
| Pneumonia | 0.249 (p < 0.001) | 0.148 (p = 0.017) | −0.148 (p = 0.017) |
| Fever | 0.221 (p < 0.001) | 0.168 (p = 0.007) | −0.099 (p = 0.111) |
| Cough | 0.750 (p < 0.001) | 0.283 (p < 0.001) | 0.006 (p = 0.923) |
| Sneezing | −0.129 (p = 0.037) | 0.039 (p = 0.525) | −0.117 (p = 0.058) |
| Wheezing | −0.040 (p = 0.521) | −0.009 (p = 0.888) | 0.061 (p = 0.329) |
| Decrease in appetite | −0.013 (p = 0.833) | 0.021 (p = 0.734) | −0.049 (p = 0.435) |
| Respiratory Failure | 0.117 (p = 0.058) | −0.012 (p = 0.852) | −0.038 (p = 0.540) |
| Running Nose | 0.010 (p = 0.877) | 0.010 (p = 0.877) | −0.051 (p = 0.410) |
| Common Cold | 0.588 (p < 0.001) | 0.266 (p < 0.001) | 0.004 (p = 0.947) |
| Influenza | 0.598 (p < 0.001) | 0.250 (p < 0.001) | −0.120 (p = 0.052) |
| Research Term (Italian) | Daily Visualizations—Spearman’s ρ, (p Value) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bronchitis | Pneumonia | Fever | Cough | Sneezing | Wheezing | Decrease in Appetite | Respiratory Failure | Runny Nose | Common Cold | Influenza | |
| Bronchitis | - | 0.259 (p < 0.001) | 0.291 (p < 0.001) | 0.870 (p < 0.001) | −0.133 (p = 0.031) | −0.007 (p = 0.914) | 0.090 (p = 0.146) | 0.127 (p = 0.040) | −0.055 (p = 0.374) | 0.569 (p < 0.001) | 0.606 (p < 0.001) |
| Pneumonia | 0.259 (p < 0.001) | - | 0.588 (p < 0.001) | 0.399 (p < 0.001) | 0.385 (p < 0.001) | −0.012 (p = 0.850) | 0.045 (p = 0.465) | 0.214 (p = 0.001) | 0.320 (p < 0.001) | 0.321 (p < 0.001) | 0.637 (p < 0.001) |
| Fever | 0.291 (p < 0.001) | 0.588 (p < 0.001) | - | 0.583 (p < 0.001) | 0.598 (p < 0.001) | 0.074 (p = 0.231) | 0.294 (p < 0.001) | 0.126 (p = 0.042) | 0.587 (p < 0.001) | 0.530 (p < 0.001) | 0.491 (p < 0.001) |
| Cough | 0.870 (p < 0.001) | 0.399 (p < 0.001) | 0.583 (p < 0.001) | - | 0.176 (p = 0.004) | −0.001 (p = 0.993) | 0.130 (p = 0.037) | 0.138 (p =0.026) | 0.306 (p < 0.001) | 0.782 (p < 0.001) | 0.694 (p < 0.001) |
| Sneezing | −0.133 (p = 0.031) | 0.385 (p < 0.001) | 0.598 (p < 0.001) | 0.176 (p = 0.004) | - | 0.020 (p = 0.746) | 0.215 (p < 0.001) | 0.103 (p = 0.097) | 0.646 (p < 0.001) | 0.267 (p 0.001) | 0.197 (p = 0.001) |
| Wheezing | −0.007 (p = 0.914) | −0.012 (p = 0.850) | 0.074 (p = 0.231) | −0.001 (p = 0.993) | 0.020 (p = 0.746) | - | 0.047 (p = 0.449) | 0.006 (p = 0.926) | 0.046 (pp = 0.462) | −0.030 (p = 0.626) | −0.022 (p = 0.725) |
| Decrease in appetite | −0.049 (p = 0.435) | 0.045 (p = 0.465) | 0.294 (p < 0.001) | 0.130 (p = 0.037) | 0.215 (p < 0.001) | 0.047 (p = 0.449) | - | 0.092 (p = 0.139) | 0.159 (p = 0.010) | −0.050 (p = 0.420) | −0.097 (p = 0.119) |
| Respiratory Failure | 0.127 (p = 0.040) | 0.214 (p = 0.001) | 0.126 (p = 0.042) | 0.138 (p = 0.026) | 0.103 (p = 0.097) | 0.006 (p = 0926) | 0.092 (p = 0.139) | - | −0.014 (p = 0.821) | −0.017 (p = 0.784) | 0.204 (p = 0.001) |
| Runny Nose | −0.055 (p = 0.374) | 0.320 (p < 0.001) | 0.587 (p < 0.001) | 0.306 (p < 0.001) | 0.646 (p < 0.001) | 0.046 (p = 0.462) | 0.159 (p = 0.010) | −0.014 (p = 0.821) | - | 0.479 (p < 0.001) | 0.163 (p = 0.008) |
| Common Cold | 0.569 (p < 0.001) | 0.321 (p < 0.001) | 0.530 (p < 0.001) | 0.782 (p < 0.001) | 0.267 (p < 0.001) | −0.030 (p = 0.626) | −0.050 (p = 0.420) | −0.017 (p = 0.784) | 0.479 (p < 0.001) | - | 0.627 (p < 0.001) |
| Influenza | 0.606 (p < 0.001) | 0.637 (p < 0.001) | 0.491 (p < 0.001) | 0.694 (p < 0.001) | 0.197 (p = 0.001) | −0.022 (p = 0.725) | −0.097 (p = 0.119) | 0.204 (p = 0.001) | 0.163 (p = 0.008) | 0.627 (p < 0.001) | - |
| Research Term (Italian) | Daily Visualizations Spearman’s ρ, (p Value) | ||||
|---|---|---|---|---|---|
| Bronchiolitis | Human Respiratory Syncytial Virus | Bronchitis | Pneumonia | Influenza | |
| Bronchiolitis | 0.603 (p < 0.001) | 0.396 (p < 0.001) | 0.433 (p < 0.001) | 0.212 (p = 0.001) | 0.204 (p = 0.001) |
| RSV | 0.056 (p = 0.372) | −0.063 (p = 0.371) | 0.051 (p = 0.416) | −0.026 (p = 0.681) | −0.162 (p = 0.009) |
| Respiratory Syncytial Virus | 0.225 (p < 0.001) | 0.248 (p < 0.001) | 0.135 (p = 0.031) | 0.057 (p = 0.361) | 0.090 (p = 0.151) |
| Bronchitis | 0.646 (p < 0.001) | 0.317 (p < 0.001) | 0.544 (p < 0.001) | 0.318 (p < 0.001) | 0.122 (p = 0.051) |
| Pneumonia | 0.170 (p = 0.006) | 0.249 (p < 0.001) | 0.057 (p = 0.359) | 0.200 (p = 0.001) | 0.562 (p < 0.001) |
| Fever | −0.154 (p = 0.013) | 0.221 (p < 0.001) | −0.239 (p < 0.001) | −0.161 (p = 0.010) | 0.283 (p < 0.001) |
| Cough | 0.380 (p < 0.001) | 0.750 (p < 0.001) | 0.221 (p < 0.001) | 0.032 (p = 0.604) | 0.181 (p = 0.004) |
| Sneezing | −0.372 (p < 0.001) | 0.360 (p < 0.001) | −0.463 (p < 0.001) | −0.361 (p < 0.001) | −0.198 (p = 0.001) |
| Wheezing | −0.020 (p = 0.754) | −0.052 (p = 0.407) | −0.069 (p = 0.269) | −0.085 (p = 0.173) | −0.027 (p = 0.664) |
| Decrease in appetite | −0.176 (p = 0.005) | 0.035 (p = 0.574) | −0.158 (p = 0.011) | −0.158 (p = 0.011) | −0.176 (p = 0.005) |
| Respiratory Failure | 0.097 (p = 0.121) | 0.117 (p = 0.058) | 0.168 (p = 0.007) | 0.219 (p < 0.001) | 0.231 (p < 0.001) |
| Runny Nose | −0.383 (p < 0.001) | 0.010 (p = 0.877) | −0.520 (p < 0.001) | −0.504 (< 0.001) | 0.042 (p = 0.503) |
| Common Cold | 0.258 (p < 0.001) | 0.526 (p < 0.001) | 0.088 (p = 0.159) | −0.088 (p = 0.160) | 0.295 (p < 0.001) |
| Influenza | 0.494 (p < 0.001) | 0.652 (p < 0.001) | 0.383 (p < 0.001) | 0.320 (p < 0.001) | 0.740 (p < 0.001) |
| Daily Visualizations Spearman’s ρ, (p Value) | |||||
|---|---|---|---|---|---|
| Bronchiolitis | Human Respiratory Syncytial Virus | Bronchitis | Pneumonia | Influenza | |
| Bronchiolitis | - | 0.273 (p < 0.001) | 0.805 (p < 0.001) | 0.643 (p < 0.001) | 0.412 (p < 0.001) |
| Human Respiratory Syncytial Virus | 0.273 (p < 0.001) | - | 0.037 (p = 0.550) | 0.020 (p = 0.752) | 0.568 (p < 0.001) |
| Bronchitis | 0.805 (p < 0.001) | 0.037 (p = 0.550) | - | 0.877 (p < 0.001) | 0.393 (p < 0.001) |
| Pneumonia | 0.643 (p < 0.001) | 0.020 (p = 0.752) | 0.877 (p < 0.001) | - | 0.473 (p < 0.001) |
| Influenza | 0.412 (p < 0.001) | 0.568 (p < 0.001) | 0.393 (p < 0.001) | 0.473 (p < 0.001) | - |
References
- Baraldi, E.; Checcucci Lisi, G.; Costantino, C.; Heinrichs, J.H.; Manzoni, P.; Riccò, M.; Roberts, M.; Vassilouthis, N. RSV Disease in Infants and Young Children: Can We See a Brighter Future? Hum. Vaccines Immunother. 2022, 18, 2079322. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Ranzieri, S. Respiratory Syncytial Virus: Knowledge, Attitudes and Beliefs of General Practitioners from North-Eastern Italy (2021). Pediatr. Rep. 2022, 14, 147–165. [Google Scholar] [CrossRef] [PubMed]
- Bozzola, E. Respiratory Syncytial Virus Resurgence in Italy: The Need to Protect All Neonates and Young Infants. Int. J. Environ. Res. Public Health 2022, 19, 380. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Checcucci Lisi, G.; et al. Epidemiology and Prevention of Respiratory Syncytial Virus Infections in Children in Italy. Ital. J. Pediatr. 2021, 47, 198. [Google Scholar] [CrossRef] [PubMed]
- Blanken, M.O.; Rovers, M.M.; Molenaar, J.M.; Winkler-Seinstra, P.L.; Meijer, A.; Kimpen, J.L.L.; Bont, L. Respiratory Syncytial Virus and Recurrent Wheeze in Healthy Preterm Infants. N. Engl. J. Med. 2013, 368, 1791–1799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, C.B. Respiratory Syncytial Virus and Parainfluenza Virus. N. Engl. J. Med. 2001, 344, 1917–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, C.B.; Weinberg, G.A.; Iwane, M.K.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Auinger, P.; Griffin, M.R.; Poehling, K.A.; Erdman, D.; et al. The Burden of Respiratory Syncytial Virus Infection in Young Children. N. Engl. J. Med. 2009, 360, 588–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weigl, J.A.I.; Puppe, W.; Schmitt, H.J. Incidence of Respiratory Syncytial Virus-Positive Hospitalizations in Germany. Eur. J. Clin. Microbiol. Infect. Dis. 2001, 20, 452–459. [Google Scholar] [CrossRef]
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children in 2015: A Systematic Review and Modelling Study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [Green Version]
- Leader, S.; Kohlhase, K. Respiratory Syncytial Virus-Coded Pediatric Hospitalizations, 1997 to 1999. Pediatr. Infect. Dis. J. 2002, 21, 629–661. [Google Scholar] [CrossRef]
- Leader, S.; Kohlhase, K.; Pearlman, M.H.; Williams, J.V.; Engle, W.A. Recent Trends in Severe Respiratory Syncytial Virus (RSV) among US Infants, 1997 to 2000. J. Pediatr. 2003, 143, S127–S132. [Google Scholar] [CrossRef] [PubMed]
- Palmer, L.; Hall, C.B.; Katkin, J.P.; Shi, N.; Masaquel, A.S.; McLaurin, K.K.; Mahadevia, P.J. Healthcare Costs within a Year of Respiratory Syncytial Virus among Medicaid Infants. Pediatr. Pulmonol. 2010, 45, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Campbell, I.; Moran, E.; Li, X.; Campbell, H.; Demont, C.; Nyawanda, B.O.; Chu, H.Y.; et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2021, 222, S577–S583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staadegaard, L.; Caini, S.; Wangchuk, S.; Thapa, B.; de Almeida, W.A.F.; de Carvalho, F.C.; Njouom, R.; Fasce, R.A.; Bustos, P.; Kyncl, J.; et al. The Global Epidemiology of RSV in Community and Hospitalized Care: Findings from 15 Countries. Open Forum Infect. Dis 2021, 8, ofab159. [Google Scholar] [CrossRef]
- Nair, H.; Theodoratou, E.; Rudan, I.; Nokes, D.J.; Ngama HND, M.; Munywoki, P.K.; Dherani, M.; Nair, H.; James Nokes, D.; Gessner, B.D.; et al. Global Burden of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children: A Systematic Review and Meta-Analysis. Lancet 2010, 375, 1545–1555. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Children Younger than 5 Years in 2019: A Systematic Analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Pitzer, V.E.; Viboud, C.; Alonso, W.J.; Wilcox, T.; Metcalf, C.J.; Steiner, C.A.; Haynes, A.K.; Grenfell, B.T. Environmental Drivers of the Spatiotemporal Dynamics of Respiratory Syncytial Virus in the United States. PLoS Pathog. 2015, 11, e1004591. [Google Scholar] [CrossRef]
- Baker, R.E.; Mahmud, A.S.; Wagner, C.E.; Yang, W.; Pitzer, V.E.; Viboud, C.; Vecchi, G.A.; Metcalf, C.J.E.; Grenfell, B.T. Epidemic Dynamics of Respiratory Syncytial Virus in Current and Future Climates. Nat. Commun. 2019, 10, 5512. [Google Scholar] [CrossRef] [Green Version]
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Cereda, D.; Anselmi, G.; Binda, S.; Gramegna, M.; Pariani, E. Respiratory Syncytial Virus in Influenza-like Illness Cases: Epidemiology and Molecular Analyses of Four Consecutive Winter Seasons (2014-2015/2017-2018) in Lombardy (Northern Italy). J. Med. Virol. 2020, 92, 2999–3006. [Google Scholar] [CrossRef]
- Teirlinck, A.C.; Broberg, E.K.; Berg, A.S.; Campbell, H.; Reeves, R.M.; Carnahan, A.S.; Lina, B.; Pakarna, G.; Bøås, H.; Nohynek, H.; et al. Recommendations for Respiratory Syncytial Virus Surveillance at the National Level. Eur. Respir. J. 2021, 58, 2003766. [Google Scholar] [CrossRef]
- Tramuto, F.; Maida, C.M.; di Naro, D.; Randazzo, G.; Vitale, F.; Restivo, V.; Costantino, C.; Amodio, E.; Casuccio, A.; Graziano, G.; et al. Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI. Vaccines 2021, 9, 1334. [Google Scholar] [CrossRef] [PubMed]
- Pariani, E.; Amendola, A.; Piatti, A.; Anselmi, G.; Ranghiero, A.; Bubba, L.; Rosa, A.M.; Pellegrinelli, L.; Binda, S.; Coppola, L.; et al. Ten Years (2004–2014) of Influenza Surveillance in Northern Italy. Hum. Vaccines Immunother. 2015, 11, 198–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasparini, R.; Bonanni, P.; Amicizia, D.; Bella, A.; Donatelli, I.; Cristina, M.L.; Panatto, D.; Luigi Lai, P. Influenza Epidemiology in Italy Two Years after the 2009–2010 Pandemic Need to Improve Vaccination Coverage. Hum. Vaccines Immunother. 2013, 9, 561–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Seiti, A.; Anselmi, G.; Primache, V.; Signorini, L.; Delbue, S.; Binda, S.; Pariani, E. Respiratory Syncytial Virus in Pediatric Influenza-like Illness Cases in Lombardy, Northern Italy, during Seven Consecutive Winter Seasons (from 2014–2015 to 2020–2021). Influenza Other Respir. Viruses 2022, 16, 481–491. [Google Scholar] [CrossRef]
- de Francesco, M.A.; Pollara, C.; Gargiulo, F.; Giacomelli, M.; Caruso, A. Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 9525. [Google Scholar] [CrossRef] [PubMed]
- Indolfi, G.; Resti, M.; Zanobini, A.; Pediatrici, A.O. Outbreak of Respiratory Syncytial Virus Bronchiolitis in Italy. Clin. Infect. Dis. 2022, 75, 549–550. [Google Scholar] [CrossRef]
- Calderaro, A.; de Conto, F.; Buttrini, M.; Piccolo, G.; Montecchini, S.; Maccari, C.; Martinelli, M.; di Maio, A.; Ferraglia, F.; Pinardi, F.; et al. Human Respiratory Viruses, Including SARS-CoV-2, Circulating in the Winter Season 2019–2020 in Parma, Northern Italy. Int. J. Infect. Dis. 2021, 102, 79–84. [Google Scholar] [CrossRef]
- Ippolito, G.; la Vecchia, A.; Umbrello, G.; di Pietro, G.; Bono, P.; Scalia, S.; Pinzani, R.; Tagliabue, C.; Bosis, S.; Agostoni, C.; et al. Disappearance of Seasonal Respiratory Viruses in Children Under Two Years Old During COVID-19 Pandemic: A Monocentric Retrospective Study in Milan, Italy. Front. Pediatr. 2021, 9, 721005. [Google Scholar] [CrossRef]
- de Conto, F.; Conversano, F.; Medici, M.C.; Ferraglia, F.; Pinardi, F.; Arcangeletti, M.C.; Chezzi, C.; Calderaro, A. Epidemiology of Human Respiratory Viruses in Children with Acute Respiratory Tract Infection in a 3-Year Hospital-Based Survey in Northern Italy. Diagn. Microbiol. Infect. Dis. 2019, 94, 260–267. [Google Scholar] [CrossRef]
- Nuti, S.V.; Wayda, B.; Ranasinghe, I.; Wang, S.; Dreyer, R.P.; Chen, S.I.; Murugiah, K. The Use of Google Trends in Health Care Research: A Systematic Review. PLoS ONE 2014, 9, e109583. [Google Scholar] [CrossRef]
- Rovetta, A. Reliability of Google Trends: Analysis of the Limits and Potential of Web Infoveillance During COVID-19 Pandemic and for Future Research. Front. Res. Metr. Anal. 2021, 6, 670226. [Google Scholar] [CrossRef] [PubMed]
- Bragazzi, N.L. Infodemiology and Infoveillance of Multiple Sclerosis in Italy. Mult. Scler. Int. 2013, 2013, 924029. [Google Scholar] [CrossRef] [PubMed]
- Kow, R.Y.; Mohamad Rafiai, N.; Ahmad Alwi, A.A.; Low, C.L.; Ahmad, M.W.; Zakaria, Z.; Zulkifly, A.H. COVID-19 Infodemiology: Association Between Google Search and Vaccination in Malaysian Population. Cureus 2022, 14, e29515. [Google Scholar] [CrossRef]
- Ciaffi, J.; Meliconi, R.; Landini, M.P.; Mancarella, L.; Brusi, V.; Faldini, C.; Ursini, F. Seasonality of Back Pain in Italy: An Infodemiology Study. Int. J. Environ. Res. Public Health 2021, 18, 1325. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.T.; Besser, G.; Leonhard, M.; Bartosik, T.J.; Parzefall, T.; Brkic, F.F.; Mueller, C.A.; Riss, D. Seasonal Variations in Public Inquiries into Laryngitis: An Infodemiology Study. J. Voice 2022, 36, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Pinto, B.; Halonen, J.I.; Antó, A.; Jormanainen, V.; Czarlewski, W.; Bedbrook, A.; Papadopoulos, N.G.; Freitas, A.; Haahtela, T.; Antó, J.M.; et al. Prediction of Asthma Hospitalizations for the Common Cold Using Google Trends: Infodemiology Study. J. Med. Internet Res. 2021, 23, e27044. [Google Scholar] [CrossRef] [PubMed]
- Huynh Dagher, S.; Lamé, G.; Hubiche, T.; Ezzedine, K.; Doung, T.A. The Influence of Media Coverage and Governmental Policies on Google Queries Related to COVID-19 Cutaneous Symptoms: Infodemiology Study. JMIR Public Health Surveill. 2022, 8, e32364. [Google Scholar] [CrossRef]
- Cai, O.; Sousa-Pinto, B. United States Influenza Search Patterns Since the Emergence of COVID-19: Infodemiology Study. JMIR Public Health Surveill. 2022, 8, e32364. [Google Scholar] [CrossRef]
- Bhagavathula, A.S.; Massey, P.M. Google Trends on Human Papillomavirus Vaccine Searches in the United States From 2010 to 2021: Infodemiology Study. JMIR Public Health Surveill. 2022, 8, e37656. [Google Scholar] [CrossRef]
- Santangelo, O.E.; Provenzano, S.; Gianfredi, V. Infodemiology of Flu: Google Trands-Based Analysis of Italians’ Digital Behavior and a Focus on SARS-CoV-2, Italy. J. Prev. Med. Hyg. 2021, 62, E586–E591. [Google Scholar]
- Nucci, D.; Santangelo, O.E.; Nardi, M.; Provenzano, S.; Gianfredi, V. Wikipedia, Google Trends and Diet: Assessment of Temporal Trends in the Internet Users’ Searches in Italy before and during Covid-19 Pandemic. Nutrients 2021, 13, 3683. [Google Scholar] [CrossRef] [PubMed]
- Provenzano, S.; Gianfredi, V.; Santangelo, O.E. Insight the Data: Wikipedia’s Researches and Real Cases of Arboviruses in Italy. Public Health 2021, 192, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Infodemiology and Infoveillance: Framework for an Emerging Set of Public Health Informatics Methods to Analyze Search, Communication and Publication Behavior on the Internet. J. Med. Internet Res. 2009, 11, e1157. [Google Scholar] [CrossRef] [PubMed]
- Rovetta, A. Google Trends as a Predictive Tool for COVID-19 Vaccinations in Italy: Retrospective Infodemiological Analysis. JMIRx Med. 2022, 3, e35356. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Bragazzi, N.L.; Mahamid, M.; Bisharat, B.; Mahroum, N.; Amital, H.; Adawi, M. Monitoring Public Interest toward Pertussis Outbreaks: An Extensive Google Trends–Based Analysis. Public Health 2018, 165, 9–15. [Google Scholar] [CrossRef]
- Cervellin, G.; Comelli, I.; Lippi, G. Is Google Trends a Reliable Tool for Digital Epidemiology? Insights from Different Clinical Settings. J. Epidemiol. Glob. Health 2017, 7, 185–189. [Google Scholar] [CrossRef]
- Riccò, M.; Valente, M.; Marchesi, F. Are Symptoms Associated with SARS-CoV-2 Infections Evolving over Time? Infect. Dis. Now 2022, 52, 110–112. [Google Scholar] [CrossRef]
- Barbati, F.; Moriondo, M.; Pisano, L.; Calistri, E.; Lodi, L.; Ricci, S.; Giovannini, M.; Canessa, C.; Indolfi, G.; Azzari, C. Epidemiology of Respiratory Syncytial Virus-Related Hospitalization over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution before Vaccine Introduction. Vaccines 2020, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control (ECDC) EU Case Definitions of Infectious Diseases as Published in the Official Journal of the European Union (Commission Implementing Decision (EU) 2018/945). Available online: https://www.ecdc.europa.eu/en/all-topics/eu-case-definitions (accessed on 5 November 2022).
- Rizzo, C.; Rota, M.C.; Bella, A.; Giannitelli, S.; Santis, D.; Nacca, S.; Pompa, G.G.; Vellucci, M.G.; Salmaso, L.; Declich, S. Response to the 2009 Influenza A (H1N1) Pandemic in Italy. Eurosurveillance 2010, 15, 19744. [Google Scholar] [CrossRef] [Green Version]
- Gasparini, R.; Amicizia, D.; Lai, P.L.; Panatto, D. Clinical and Socioeconomic Impact of Seasonal and Pandemic Influenza in Adults and the Elderly. Hum. Vaccines Immunother. 2012, 8, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention Respiratory Syncytial Virus Infection (RSV)—Symptoms and Care. Available online: https://www.cdc.gov/rsv/about/symptoms.html (accessed on 20 October 2022).
- Britton, P.N.; Hu, N.; Saravanos, G.; Shrapnel, J.; Davis, J.; Snelling, T.; Dalby-Payne, J.; Kesson, A.M.; Wood, N.; Macartney, K.; et al. COVID-19 Public Health Measures and Respiratory Syncytial Virus. Lancet Child Adolesc. Health 2020, 4, e42–e43. [Google Scholar] [CrossRef] [PubMed]
- Gastaldi, A.; Donà, D.; Barbieri, E.; Giaquinto, C.; Bont, L.J.; Baraldi, E. COVID-19 Lesson for Respiratory Syncytial Virus (RSV): Hygiene Works. Children 2021, 8, 1144. [Google Scholar] [CrossRef] [PubMed]
- di Mattia, G.; Nenna, R.; Mancino, E.; Rizzo, V.; Pierangeli, A.; Villani, A.; Midulla, F. During the COVID-19 Pandemic Where Has Respiratory Syncytial Virus Gone? Pediatr. Pulmonol. 2021, 56, 3106–3109. [Google Scholar] [CrossRef]
- White, K.J. The Durbin-Watson Test for Autocorrelation in Nonlinear Models 370 The Review of Economics and Statistics the Durbin-Watson Test for Autocorrelation in Nonlinear Models. Rev. Econ. Stat. 1992, 74, 370–373. [Google Scholar] [CrossRef]
- R Development Core Team. R a Language and Environment for Statistical Computing: Reference Index; R Foundation for Statistical Computing: Vienna, Austria, 2010; ISBN 3900051070. [Google Scholar]
- Perez, A.; Lively, J.Y.; Curns, A.; Weinberg, G.A.; Halasa, N.B.; Staat, M.A.; Szilagyi, P.G.; Stewart, L.S.; Mcneal, M.M.; Clopper, B. Respiratory Virus Surveillance Among Children with Acute Respiratory Illnesses-New Vaccine Surveillance Network, United States, 2016–2021. Morb. Mortal. Wkly. Rep. 2022, 71, 1253–1259. [Google Scholar] [CrossRef]
- Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh, E.E. Respiratory Syncytial Virus Infection in Elderly and High-Risk Adults. N. Engl. J. Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Lopardo, G.; Scarpellini, B.; Stein, R.T.; Ribeiro, D. Systematic Review on Respiratory Syncytial Virus Epidemiology in Adults and the Elderly in Latin America. Int. J. Infect. Dis. 2020, 90, 170–180. [Google Scholar] [CrossRef] [Green Version]
- Billard, M.; van de Ven, P.M.; Baraldi, B.; Kragten-Tabatabaie, L.; Bont, L.J.; Wildenbeest, J.G. International Changes in Respiratory Syncytial Virus (RSV) Epidemiology during the COVID-19 Pandemic: Association with School Closures. Influenza Other Respir. Viruses 2022, 16, 926–936. [Google Scholar] [CrossRef]
- van Brusselen, D.; de Troeyer, K.; ter Haar, E.; vander Auwera, A.; Poschet, K.; van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S.; van Herendael, B.; et al. Bronchiolitis in COVID-19 Times: A Nearly Absent Disease? Eur. J. Pediatr. 2021, 180, 1969–1973. [Google Scholar] [CrossRef]
- Taylor, A.; Whittaker, E. The Changing Epidemiology of Respiratory Viruses in Children During the COVID-19 Pandemic: A Canary in a COVID Time. Pediatr. Infect. Dis. J. 2022, 41, E46–E48. [Google Scholar] [CrossRef]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N.; Ujiie, M. Resurgence of Respiratory Syncytial Virus Infections during Covid-19 Pandemic, Tokyo, Japan. Emerg. Infect. Dis. 2021, 27, 2969–2970. [Google Scholar] [CrossRef] [PubMed]
- Mameli, C.; Picca, M.; Buzzetti, R.; Pace, M.E.; Badolato, R.; Cravidi, C.; Zuccotti, G.V.; Marchisio, P.; Sala, M.; di Cosimo, M.E. Incidence of Acute Respiratory Infections in Preschool Children in an Outpatient Setting before and during Covid-19 Pandemic in Lombardy Region, Italy. Ital. J. Pediatr. 2022, 48, 18. [Google Scholar] [CrossRef]
- Castagno, E.; Raffaldi, I.; del Monte, F.; Garazzino, S.; Bondone, C. New Epidemiological Trends of Respiratory Syncytial Virus Bronchiolitis during COVID-19 Pandemic. World J. Pediatr. 2022. [Google Scholar] [CrossRef] [PubMed]
- Rabbone, I.; Monzani, A.; Scaramuzza, A.E.; Cavalli, C. See-Sawing COVID-19 and RSV Bronchiolitis in Children under 2 Years of Age in Northern Italy. Acta Paediatr. Int. J. Paediatr. 2022, 111, 2174–2175. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Abu Raya, B.; Baraldi, E.; Flanagan, K.; Martinon Torres, F.; Tsolia, M.; Zielen, S. RSV Prevention in All Infants: Which Is the Most Preferable Strategy? Front. Immunol. 2022, 13, 880368. [Google Scholar] [CrossRef]
- di Carlo, P.; Romano, A.; Plano, M.R.A.; Gueli, A.; Scarlata, F.; Mammina, C. Children, Parents and Respiratory Syncytial Virus in Palermo, Italy: Prevention Is Primary. J. Child Health Care 2010, 14, 396–407. [Google Scholar] [CrossRef]
- Reyes Domínguez, A.I.; Pavlovic Nesic, S.; Urquía Martí, L.; Pérez González, M.D.C.; Reyes Suárez, D.; García-Muñoz Rodrigo, F. Effects of Public Health Measures during the SARS-CoV-2 Pandemic on the Winter Respiratory Syncytial Virus Epidemic: An Interrupted Time Series Analysis. Paediatr. Perinat. Epidemiol. 2022, 36, 329–336. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Balzarini, F.; Capozzi, V.A.; Volpi, L. Knowledge, Attitudes, Beliefs and Practices of Obstetrics-Gynecologists on Seasonal Influenza and Pertussis Immunizations in Pregnant Women: Preliminary Results from North-Western Italy. Minerva Ginecol. 2019, 71, 288–297. [Google Scholar] [CrossRef]
- Gabutti, G.; Azzari, C.; Bonanni, P.; Prato, R.; Tozzi, A.E.; Zanetti, A.; Zuccotti, G. Pertussis. Hum. Vaccines Immunother. 2015, 11, 108–117. [Google Scholar] [CrossRef] [Green Version]
- Esposito, S.; Principi, N. Prevention of Pertussis: An Unresolved Problem. Hum. Vaccines Immunother. 2018, 14, 2452–2459. [Google Scholar] [CrossRef] [Green Version]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Bragazzi, N.L.; Balzarini, F. Pertussis Immunization in Healthcare Workers Working in Pediatric Settings: Knowledge, Attitudes and Practices (KAP) of Occupational Physicians. Preliminary Results from a Web-Based Survey (2017). J. Prev. Med. Hyg. 2020, 61, E66–E75. [Google Scholar]
- Haynes, A.K.; Prill, M.M.; Iwane, M.K.; Gerber, S.I. Morbidity and Mortality Weekly Report. Morb. Mortal. Wkly. Rep. MMWR 2014, 63, 1133–1136. [Google Scholar]
- Janet, S.; Broad, J.; Snape, M.D. Respiratory Syncytial Virus Seasonality and Its Implications on Prevention Strategies. Hum. Vaccines Immunother. 2018, 14, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Rose, E.B.; Wheatley, A.; Langley, G.; Gerber, S.; Haynes, A. Amber Morbidity and Mortality Weekly Report Respiratory Syncytial Virus Seasonality-United States, 2014–2017. Morb. Mortal. Wkly. Rep. 2018, 67, 71. [Google Scholar] [CrossRef]
- Griffiths, C.; Drews, S.J.; Marchant, D.J. Respiratory Syncytial Virus: Infection, Detection, and New Options for Prevention and Treatment. Clin. Microbiol. Rev. 2017, 30, 277–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenmoe, S.; Bigna, J.J.; Well, E.A.; Simo, F.B.N.; Penlap, V.B.; Vabret, A.; Njouom, R. Prevalence of Human Respiratory Syncytial Virus Infection in People with Acute Respiratory Tract Infections in Africa: A Systematic Review and Meta-Analysis. Influenza Other Respir. Viruses 2018, 12, 793–803. [Google Scholar] [CrossRef]
- Suleiman-Martos, N.; Caballero-Vázquez, A.; Gómez-Urquiza, J.L.; Albendín-García, L.; Romero-Béjar, J.L.; Cañadas-De la Fuente, G.A. Prevalence and Risk Factors of Respiratory Syncytial Virus in Children under 5 Years of Age in the Who European Region: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 416. [Google Scholar] [CrossRef]
- Mphil, N.; Stadler, J.A.M.; Gray, D.; Mph, B.; Lesosky, M.; Zar, H.J.; Cross War, R.; Nduru, P.; Stadler, J.A.M.; Gray, D.; et al. Early-Life Respiratory Syncytial Virus Lower Respiratory Tract Infection in a South African Birth Cohort: Epidemiology and Effect on Lung Health. Lancet Glob. Health 2020, 8, e1316–e1325. [Google Scholar]
- Andeweg, S.P.; Schepp, R.M.; van de Kassteele, J.; Mollema, L.; Berbers, G.A.M.; van Boven, M. Population-Based Serology Reveals Risk Factors for RSV Infection in Children Younger than 5 Years. Sci. Rep. 2021, 11, 8953. [Google Scholar] [CrossRef]
- Fan Leung, T.; Atkins, K.; Salimi, V.; Bozzola, E.; Olivier, W.C.; Alonso, N.J. The Assessment of Future RSV Immunizations: How to Protect All Infants? Front. Pediatr. 2022, 10, 981741. [Google Scholar] [CrossRef]
- Amicizia, D.; Lai, P.L.; Gasparini, R.; Panatto, D. Influenza Vaccination of Elderly: Relaunch Time. Ann. Ig. 2018, 30, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Cerviere, M.P.; Corrado, S.; Ranzieri, S.; Marchesi, F. Respiratory Syncytial Virus: An Uncommon Cause of Febrile Seizures—Results from a Systematic Review and Meta-Analysis. Pediatr. Rep. 2022, 14, 464–478. [Google Scholar] [CrossRef] [PubMed]
- Mazur, N.I.; Martinón-Torres, F.; Baraldi, E.; Fauroux, B.; Greenough, A.; Heikkinen, T.; Manzoni, P.; Mejias, A.; Nair, H.; Papadopoulos, N.G.; et al. Lower Respiratory Tract Infection Caused by Respiratory Syncytial Virus: Current Management and New Therapeutics. Lancet Respir. Med. 2015, 3, 888–900. [Google Scholar] [CrossRef]
- Torchin, H.; Charkaluk, M.L.; Rousseau, J.; Marchand-Martin, L.; Treluyer, L.; Nuytten, A.; Truffert, P.; Jarreau, P.H.; Ancel, P.Y. Full Compliance with Respiratory Syncytial Virus Prophylaxis Was Associated with Fewer Respiratory-Related Hospital Admissions in Preterm Children: A Cohort Study. Acta Paediatr. Int. J. Paediatr. 2021, 110, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Kombe, I.K.; Agoti, C.N.; Munywoki, P.K.; Baguelin, M.; Nokes, D.J.; Medley, G.F. Integrating Epidemiological and Genetic Data with Different Sampling Intensities into a Dynamic Model of Respiratory Syncytial Virus Transmission. Sci. Rep. 2021, 11, 1463. [Google Scholar] [CrossRef]
- Sullender, W.M. Respiratory Syncytial Virus Genetic and Antigenic Diversity. Clin. Microbiol. Rev. 2000, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Piedimonte, G.; Perez, M.K. Respiratory Syncytial Virus Infection and Bronchiolitis Practice Gaps. Pediatr. Rev. 2014, 35, 519–530. [Google Scholar] [CrossRef]
- Weber, A.; Weber, M.; Milligan, P. Modeling Epidemics Caused by Respiratory Syncytial Virus (RSV). Math. Biosci. 2001, 172, 95–113. [Google Scholar] [CrossRef]
- Biggerstaff, M.; Cauchemez, S.; Reed, C.; Gambhir, M.; Finelli, L. Estimates of the Reproduction Number for Seasonal, Pandemic, and Zoonotic Influenza: A Systematic Review of the Literature. BMC Infect. Dis. 2014, 14, 480. [Google Scholar] [CrossRef] [Green Version]
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and Influenza Pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef]
- Dota, F.; Panaccione, D. Use of Italian Language, Dialects and Foreign Languages; ISTAT: Rome, Italy, 2017. [Google Scholar]
- Candela, M.; Prado, A. Italian Operators’ Response to the COVID-19 Pandemic; Italian Operators’ Response to the COVID-19 Pandemic. ACM SIGCOMM Comput. Commun. Rev. 2021, 51, 26–31. [Google Scholar] [CrossRef]
- Perrone, A. Italy’s Bad Internet Connection: Italians Have One of the Lowest Levels of Digital Skills in Europe and Are Struggling to Understand Implications of the New Pandemic World. Index Censorsh. 2020, 49, 43–45. [Google Scholar] [CrossRef]
- Matteo Riccò Excess Mortality in Mountain Areas of Emilia Romagna Region during the First Months of SARS-CoV-2 Pandemic: A “Canary in the Coal Mine”? Acta Biomed. 2022, 93, e20222247. [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Satta, E.; Ranzieri, S. Excess Mortality on Italian Small Islands during the SARS-CoV-2 Pandemic: An Ecological Study. Infect. Dis. Rep. 2022, 14, 391–412. [Google Scholar] [CrossRef]
- Gatto, M.; Bertuzzo, E.; Mari, L.; Miccoli, S.; Carraro, L.; Casagrandi, R.; Rinaldo, A. Spread and Dynamics of the COVID-19 Epidemic in Italy: Effects of Emergency Containment Measures. Proc. Natl. Acad. Sci. USA 2020, 117, 10484–10491. [Google Scholar] [CrossRef] [Green Version]
- Scortichini, M.; Schneider Dos Santos, R.; De’ Donato, F.; de Sario, M.; Michelozzi, P.; Davoli, M.; Masselot, P.; Sera, F.; Gasparrini, A. Excess Mortality during the COVID-19 Outbreak in Italy: A Two-Stage Interrupted Time-Series Analysis. Int. J. Epidemiol. 2020, 49, 1909–1917. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Regional Office for Europe: An Unprecedented Challenge: Italy’s First Response to COVID-19; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Odone, A.; Delmonte, D.; Scognamiglio, T.; Signorelli, C. COVID-19 Deaths in Lombardy, Italy: Data in Context. Lancet Public Health 2020, 5, e310. [Google Scholar] [CrossRef]
- Caranci, N.; di Girolamo, C.; Bartolini, L.; Fortuna, D.; Berti, E.; Sforza, S.; Rossi, P.G.; Moro, M.L. General and COVID-19-Related Mortality by Pre-Existing Chronic Conditions and Care Setting during 2020 in Emilia-Romagna Region, Italy. Int. J. Environ. Res. Public Health 2021, 18, 13224. [Google Scholar] [CrossRef]
- la Rosa, G.; Mancini, P.; Bonanno Ferraro, G.; Veneri, C.; Iaconelli, M.; Bonadonna, L.; Lucentini, L.; Suffredini, E. SARS-CoV-2 Has Been Circulating in Northern Italy since December 2019: Evidence from Environmental Monitoring. Sci. Total Environ. 2021, 750, 141711. [Google Scholar] [CrossRef]
- Trombetta, C.M.; Marchi, S.; Viviani, S.; Manenti, A.; Casa, E.; Dapporto, F.; Remarque, E.J.; Bollati, V.; Manini, I.; Lazzeri, G.; et al. A Serological Investigation in Southern Italy: Was SARS-CoV-2 Circulating in Late 2019? Hum. Vaccines Immunother. 2022, 18, 2047582. [Google Scholar] [CrossRef]
- Capalbo, C.; Bertamino, E.; Zerbetto, A.; Santino, I.; Petrucca, A.; Mancini, R.; Bonfini, R.; Alfonsi, V.; Ferracuti, S.; Marchetti, P.; et al. No Evidence of Sars-Cov-2 Circulation in Rome (Italy) during the Pre-Pandemic Period: Results of a Retrospective Surveillance. Int. J. Environ. Res. Public Health 2020, 17, 8461. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.; Tambuzzi, S.; Bergna, A.; Battistini, A.; della Ventura, C.; Galli, M.; Zoja, R.; Zehender, G.; Cattaneo, C. Evidence of SARS-CoV-2 Antibodies and RNA on Autopsy Cases in the Pre-Pandemic Period in Milan (Italy). Front. Microbiol. 2022, 13, 886317. [Google Scholar] [CrossRef] [PubMed]

| Section/Topic | Google Research Volume | Wikipedia |
|---|---|---|
| Access Date | 20 October 2022 | 20 October 2022 |
| Time period | 16 October 2017–16 October 2022 | 16 October 2017–16 October 2022 |
| Search Tool | Google TrendsTM (https://trends.google.it/) | Pageviews Analysis (https://pageviews.wmcloud.org/) |
| Limits | Searches from Italy | Only pages in Italian |
| Search Input (Italian) | Bronchiolitis (“bronchiolite”) Respiratory Syncytial Virus (“Virus Respiratorio Sinciziale”) RSV (“VRS”) Bronchitis (“bronchite”) Pneumonia (“polmonite”) common cold (“raffreddore”) influenza (“influenza”) respiratory failure (“insufficienza respiratoria”) fever (“febbre”) Cough (“tosse”) wheezing (“respire sibilante”) sneezing (“starnuti”) runny nose (“naso che cola”) decrease in appetite (“inappetenza”) | Bronchiolitis (“bronchiolite”) Human Respiratory Syncytial Virus (“Virus Respiratorio Sinciziale Umano”) Bronchitis (“bronchite”) Pneumonia (“polmonite”) influenza/flu (“influenza”) |
| Combination | Only one search term | Only one search term |
| Retrieved data | Relative Search Volumes | Number of Daily Visualizations |
| Seasonal Incidence Rate (Cases per 1000 Persons; 95%CI) | Excess Incidence Rates (%, 95%CI) | ||||||
|---|---|---|---|---|---|---|---|
| 2017–2018 | 2018–2019 | 2019–2020 | 2020–2021 | 2021–2022 | 2017–2020 vs. 2020–2021 | 2017–2020 vs. 2021–2022 | |
| 0–4 years | 13.46 (8.65; 18.26) [REFERENCE] | 13.06 (8.52; 17.60) [p = 1.000] | 11.37 (6.94; 15.80) [p = 0.839] | 2.67 (2.35; 2.98) [p < 0.001] | 11.58 (10.32; 12.84) [p = 0.882] | −78.89% (−91.06.; −66.72) | −8.31% (−88.71; +72.10) |
| 5–14 years | 7.41 (4.64; 10.18) [REFERENCE] | 6.91 (4.32; 9.49) [p = 0.994] | 7.11 (3.90; 10.31) [p = 0.999] | 1.26 (1.12; 1.40) [p = 0.001] | 4.81 (4.32; 5.30) [p = 0.307] | −82.38% (−99.40; −65.36) | −32.66% (−99.68; +34.36) |
| TOTAL | 5.11 (3.29; 6.94) [REFERENCE] | 4.79 (3.19; 6.38) [p = 0.988] | 4.49 (3.04; 5.95) [p = 0.888] | 1.44 (1.32; 1.56) [p < 0.001] | 3.94 (3.61; 4.27) [p = 0.475] | −69.94% (−89.26; −50.62) | −17.85% (−64.10; +28.39) |
| Relative Search Volumes | Average, 95% Confidence Interval |
|---|---|
| Bronchiolitis | 14.56 (11.80; 17.31) |
| RSV | 3.76 (2.37; 5.15) |
| Respiratory Syncytial Virus | 3.84 (2.03; 5.65) |
| Bronchitis | 39.91 (36.91; 42.91) |
| Pneumonia | 13.26 (11.15; 15.36) |
| Fever | 31.11 (29.14; 33.08) |
| Cough | 45.04 (42.18; 47.90) |
| Sneezing | 28.99 (26.57; 31.40) |
| Wheezing | 12.11 (9.66; 14.56) |
| Decrease in appetite | 30.83 (29.13; 32.54) |
| Respiratory Failure | 30.22 (27.70; 32.74) |
| Runny Nose | 19.96 (17.66; 22.27) |
| Common Cold | 27.74 (25.55; 29.92) |
| Influenza | 16.14 (13.57; 18.71) |
| Wikipedia Daily Visualizations | Average, 95% Confidence Interval. |
| Bronchiolitis | 67.57 (56.42; 78.73) |
| Influenza | 602.17 (402.33; 801.70) |
| Respiratory Syncytial Virus | 88.67 (47.69; 129.65) |
| Bronchitis | 192.44 (165.68; 219.20) |
| Pneumonia | 638.82 (516.16; 761.49) |
| Relative Search Volumes (Average, 95%CI.) | |||||
|---|---|---|---|---|---|
| 2017–2018 | 2018–2019 | 2019–2020 | 2020–2021 | 2021–2022 | |
| Bronchiolitis | 9.52 (7.05; 11.99) [REF.] | 10.19 (7.82; 12.56) [p = 0.996] | 7.77 (5.39; 10.15) [p = 0.043] | 3.28 (2.48; 4.08) [p = 0.012] | 16.92 (10.22; 23.62) [p = 0.999] |
| RSV | 3.33 (3.00; 3.66) [REF.] | 3.10 (3.00; 3.66) [p = 0.999] | 2.69 (2.44; 2.95) [p = 0.957] | 2.91 (2.66; 3.15) [p = 0.990] | 5.35 (1.58; 9.11) [p = 0.269] |
| Respiratory Syncytial Virus | 1.65 (0.73; 2.58) [REF.] | 1.85 (0.90; 2.80) [p = 1.000] | 1.63 (0.82; 2.45) [p = 1.000] | 1.47 (0.59; 2.34) [p = 1.000] | 6.44 (1.73; 11.16) [p = 0.010] |
| Bronchitis | 37.31 (32.47; 42.14) [REF.] | 36.79 (32.29; 41.29) [p = 0.999] | 29.37 (23.65; 35.08) [p = 0.028] | 17.72 (16.13; 19.30) [p < 0.001] | 38.25 (35.07; 41.43) [p = 0.993] |
| Pneumonia | 7.58 (6.27; 8.88) [REF.] | 8.08 (7.43; 8.72) [p = 0.996] | 16.92 (11.57; 22.28) [p < 0.001] | 10.51 (9.06; 11.95) [p = 0.316] | 9.31 (8.05; 10.57) [p = 0.754] |
| Fever | 24.88 (22.47; 27.29) [REF.] | 23.96 (22.11; 25.82) [p = 0.964] | 32.33 (28.29; 36.36) [p < 0.001] | 29.09 (27.41; 30.78) [p = 0.073] | 34.48 (32.12; 36.84) [p < 0.001] |
| Cough | 34.77 (30.59; 38.95) [REF.] | 35.06 (30.95; 39.17) [p = 1.000] | 35.85 (29.90; 41.79) [p = 0.990] | 27.72 (25.19; 30.24) [p = 0.065] | 54.02 (50.06; 57.98) [p < 0.001] |
| Sneezing | 18.69 (16.76; 20.63) [REF.] | 19.33 (17.46; 21.20) [p = 0.995] | 32.33 (28.35; 36.31) [p < 0.001] | 33.00 (30.58; 35.42) [p < 0.001] | 36.33 (32.31; 40.34) [p < 0.001] |
| Wheezing | 10.94 (7.36; 14.53) [REF.] | 14.08 (8.75; 14.53) [p = 0.681] | 12.44 (7.16; 17.73) [p = 0.965] | 9.64 (6.60; 12.69) [p = 0.979] | 13.94 (10.40; 17.49) [p = 0.712] |
| Decrease in appetite | 31.67 (29.29; 34.06) [REF.] | 26.92 (24.53; 39.32) [p = 0.045] | 30.00 (26.59; 33.41) [p = 0.792] | 31.87 (29.50; 34.23) [p = 1.000] | 32.25 (32.44; 38.05) [p = 0.681] |
| Respiratory Failure | 27.33 (23.35; 31.30) [REF.] | 26.00 (23.07; 28.93) [p = 0.967] | 33.37 (27.87; 38.86) [p = 0.087] | 25.49 (22.15; 28.83) [p = 0.901] | 25.42 (22.60; 28.25) [p = 0.891] |
| Runny Nose | 10.46 (8.85; 12.08) [REF.] | 9.96 (8.53; 11.39) [p = 0.996] | 17.65 (14.88; 20.42) [p < 0.001] | 25.30 (23.57; 27.03) [p < 0.001] | 31.19 (27.20; 35.18) [p < 0.001] |
| Common Cold | 19.90 (17.41; 22.40) [REF.] | 19.77 (17.42; 22.12) [p = 1.000] | 22.06 (18.49; 25.63) [p = 0.781] | 24.64 (21.85; 27.43) [p = 0.152] | 35.42 (30.34; 40.51) [p < 0.001] |
| Influenza | 10.94 (7.57; 14.31) [REF.] | 9.50 (7.44; 11.56) [p = 0.928] | 19.56 (13.50; 25.61) [p = 0.001] | 7.30 (6.21; 8.39) [p = 0.331] | 8.65 (7.42; 9.89) [p = 0.724] |
| Wikipedia Daily visualizations (Average, 95%CI) | |||||
| Bronchiolitis | 53.16 (46.90; 59.41) [REF.] | 79.96 (59.42; 100.50) [p = 0.037] | 41.30 (32.69; 49.91) [p = 0.614] | 22.15 (13.43; 30.86) [p = 0.011] | 42.39 (19.28; 65.50) [p = 0.700] |
| Influenza | 254.89 (206.23; 301.95) [REF.] | 209.78 (182.92; 236.63) [p = 0.996] | 1147.31 (636.49; 1568.13) [p < 0.001] | 301.19 (250.26; 352.13) [p = 0.995] | 138.08 (103.87; 172.29) [p = 0.894] |
| Respiratory Syncytial Virus | 26.81 (23.22; 30.40) [REF.] | 26.04 (22.51; 29.57) [p = 1.000] | 57.29 (44.89; 69.68) [p = 0.943] | 126.66 (3.19; 250.12) [p = 0.181] | 158.90 (42.51; 275.28) [p = 0.050] |
| Bronchitis | 335.18 (297.66; 382.69) [REF.] | 182.05 (155.75; 208.34) [p < 0.001] | 137.36 (103.43; 171.28) [p < 0.001] | 45.10 (41.27; 48.92) [p < 0.001] | 34.97 (30.04; 39.91) [p < 0.001] |
| Pneumonia | 668.89 (609.23; 728.55) [REF.] | 597.85 (518.76; 676.94) [p = 0.906] | 872.26 (556.07; 1188.45) [p = 0.170] | 298.54 (259.96; 337.12) [p = 0.002] | 148.09 (135.76; 160.42) [p < 0.001] |
| Research Field | Excess Volume Search Rates (%, 95%CI) | |
|---|---|---|
| 2017–2020 vs. 2020–2021 | 2017–2020 vs. 2021–2022 | |
| Google TrendsTM | ||
| Bronchiolitis | −74.50% (−82.83; −66.16) | +255.62% (+35.02; +478.21) |
| RSV | −4.45% (−15.89; +24.78) | +118.18% (−26.16; +262.52) |
| Respiratory Syncytial Virus | −51.73% (−94.73; −8.73) | +356.16% (+4.48; +708.85) |
| Bronchitis | −61.17% (−68.11; −54.23) | +3.89 (−13.32; +21.11) |
| Pneumonia | +37.37% (−2.00; +76.75) | +1.78% (−19.50; +23.06) |
| Fever | +8.67% (−11.99; +29.33) | +17.36% (+6.89; +27.84) |
| Cough | −38.38% (−49.20; −27.56) | +35.43% (+18.41; +52.44) |
| Sneezing | +52.93% (+30.11; +75.75) | +82.97% (+48.34; +117.60) |
| Wheezing | +40.50% (−35.59; +116.59) | +55.53% (−25.95; +138.02) |
| Decrease in appetite | +0.21% (−10.77; +11.20) | +16.33% (+5.75; +26.90) |
| Respiratory Failure | −1.35% (−19.23; +16.52) | −16.68% (−34.66; +1.30) |
| Running Nose | +102.94% (+72.35; +133.54) | +212.27% (+158.80; +265.73) |
| Common Cold | −8.44% (−23.42; +6.54) | +81.08% (+57.36; +104.80) |
| Influenza | −30.16% (−55.25; −5.07) | −24.67% (−40.39; −8.96) |
| Wikipedia | ||
| Bronchiolitis | −80.77% (−84.34;−77.20) | −20.68% (−92.26; +50.90) |
| Influenza | −48.63% (−88.19; −9.08) | −75.86% (−97.21; −54.51) |
| Respiratory Syncytial Virus | −31.40% (−52.13; −10.74) | +418.81% (−425.28 +1263.91) |
| Bronchitis | −81.87% (−83.85; −79.75) | −83.82% (−85.84; −81.79) |
| Pneumonia | −54.92% (−67.43; −43.42) | −80.05% (−84.69; −75.40) |
| Research Field | In Season (Average, 95%CI) | Out of Season (Average, 95%CI) | M-W U (p Value) |
|---|---|---|---|
| Google TrendsTM | Relative Search Volumes | ||
| Bronchiolitis | 14.56 (11.80; 17.31) | 3.68 (3.14; 4.22) | 13,474.5, p < 0.001 |
| RSV | 3.76 (2.37; 5.15) | 3.14 (2.96; 3.32) | 7758.0, p = 0.220 |
| Respiratory Syncytial Virus | 3.84 (2.03; 5.65) | 1.17 (0.67; 1.68) | 10,184.0, p < 0.001 |
| Bronchitis | 39.91 (36.91; 42.91) | 22.49 (20.86; 24.12) | 13,432.0, p < 0.001 |
| Pneumonia | 13.26 (11.15; 15.36) | 7.26 (6.67; 7.86) | 13,852.0, p < 0.001 |
| Fever | 31.11 (29.14; 33.08) | 26.45 (25.18; 27.73) | 10,552.5, p = 0.001 |
| Cough | 45.04 (42.18; 47.90) | 28.65 (26.19; 31.12) | 13,260.5, p < 0.001 |
| Sneezing | 28.99 (26.57; 31.40) | 26.76 (24.76; 28.76) | 8942.5, p = 0.437 |
| Wheezing | 12.11 (9.66; 14.56) | 12.30 (9.40; 15.19) | 8612.5, p = 0.806 |
| Decrease in appetite | 30.83 (29.93; 32.37) | 31.50 (29.74; 33.27) | 8279.5, p = 0.754 |
| Respiratory Failure | 30.22 (27.70; 32.74) | 24.38 (22.21; 26.55) | 10,500.0, p = 0.001 |
| Running Nose | 19.96 (17.66; 22.27) | 17.75 (13.57; 18.71) | 8946.0, p = 0.434 |
| Common Cold | 27.74 (25.55; 29.92) | 20.45 (18.13; 22.78) | 11,756.0, p < 0.001 |
| Influenza | 16.14 (13.57; 18.71) | 5.43 (4.97; 5.89) | 15,342, p < 0.001 |
| Wikipedia | Daily Visualizations | ||
| Bronchiolitis | 67.57 (56.42; 78.73) | 24.24 (19.81; 28.67) | 12,709.5, p < 0.001 |
| Influenza | 88.67 (47.70; 129.65) | 66.21 (10.85; 121.56) | 12,527.0, p < 0.001 |
| Respiratory Syncytial Virus | 192.44 (165.68; 219.20) | 94.92 (77.54; 112.31) | 12,009.0, p < 0.001 |
| Bronchitis | 638.82 (516.16; 761.49) | 380.28 (323.21; 437.35) | 11,044.5, p < 0.001 |
| Pneumonia | 602.02 (402.34; 801.70) | 188.37 (161.37; 215.37) | 14,068.0, p < 0.001 |
| Influenza-like Illnesses (2017–2022) | |||
|---|---|---|---|
| Research Field | 0–4 Years | 5–14 Years | TOTAL |
| Google TrendsTM | |||
| Bronchiolitis | ρ = 0.776 p < 0.001 | ρ = 0.735 p < 0.001 | ρ = 0.726 p < 0.001 |
| RSV | ρ = 0.111 p = 0.193 | ρ = 0.042 p = 0.620 | ρ = 0.035 p = 0.679 |
| Respiratory Syncytial Virus | ρ = 0.206 p = 0.015 | ρ = 0.172 p = 0.042 | ρ = 0.185 p = 0.029 |
| Bronchitis | ρ = 0.839 p < 0.001 | ρ = 0.827 p < 0.001 | ρ = 0.826 p < 0.001 |
| Pneumonia | ρ = 0.103 p = 0.224 | ρ = 0.169 p = 0.046 | ρ = 0.290 p = 0.001 |
| Fever | ρ = 0.456 p < 0.001 | ρ = 0.524 p < 0.001 | ρ = 0.605 p < 0.001 |
| Cough | ρ = 0.769 p < 0.001 | ρ = 0.777 p < 0.001 | ρ = 0.812 p < 0.001 |
| Sneezing | ρ = −0.043 p = 0.614 | ρ = 0.020 p = 0.811 | ρ = −0.075 p = 0.380 |
| Wheezing | ρ = 0.016 p = 0.847 | ρ = −0.007 p = 0.932 | ρ = 0.037 p = 0.668 |
| Decrease in appetite | ρ = 0.247 p = 0.003 | ρ = 0.239 p = 0.005 | ρ = 0.228 p = 0.007 |
| Respiratory Failure | ρ = −0.024 p = 0.777 | ρ = 0.021 p = 0.810 | ρ = 0.051 p = 0.547 |
| Running Nose | ρ = 0.034 p = 0.692 | ρ = 0.038 p = 0.652 | ρ = 0.088 p = 0.300 |
| Common Cold | ρ = 0.680 p < 0.001 | ρ = 0.689 p < 0.001 | ρ = 0.686 p < 0.001 |
| Influenza | ρ = 0.553 p < 0.001 | ρ = 0.569 p < 0.001 | ρ = 0.688 p < 0.001 |
| Wikipedia | |||
| Bronchiolitis | ρ = 0.429 p < 0.001 | ρ = 0.395 p < 0.001 | ρ = 0.365 p < 0.001 |
| Influenza | ρ = 0.416 p < 0.001 | ρ = 0.413 p < 0.001 | ρ = 0.500 p < 0.001 |
| Respiratory Syncytial Virus | ρ = 0.275 p = 0.001 | ρ = 0.395 p < 0.001 | ρ = 0.283 p = 0.001 |
| Bronchitis | ρ = 0.132 p = 0.120 | ρ = 0.204 p = 0.016 | ρ = 0.241 p = 0.004 |
| Pneumonia | ρ = 0.072 p = 0.400 | ρ = 0.112 p = 0.186 | ρ = 0.214 p = 0.011 |
| Variable | ILI Age Group | B | 95%CI | β | t | p Value | |
|---|---|---|---|---|---|---|---|
| Bronchiolitis | TOTAL | 0.030 | −0.006 | 0.066 | 0.141 | 1.654 | 0.101 |
| 0–4 yrs | 0.133 | 0.015 | 0.251 | 0.210 | 2.223 | 0.028 | |
| 5–14 yrs | 0.057 | −0.139 | 0.057 | 0.147 | 1.688 | 0.094 | |
| Respiratory Syncytial Virus | TOTAL | −0.028 | −0.080 | 0.023 | −0.088 | −1.095 | 0.276 |
| 0–4 yrs | −0.094 | −0.273 | 0.085 | −0.098 | −1.043 | 0.299 | |
| 5–14 yrs | −0.041 | −0.139 | 0.057 | −0.070 | −0.831 | 0.407 | |
| Bronchitis | TOTAL | 0.115 | 0.051 | 0.178 | 0.588 | 3.586 | <0.001 |
| 0–4 yrs | 0.568 | 0.404 | 0.732 | 0.983 | 6.857 | <0.001 | |
| 5–14 yrs | 0.200 | 0.080 | 0.320 | 0.563 | 3.294 | 0.001 | |
| Pneumonia | TOTAL | −0.155 | −0.250 | −0.060 | −0.560 | −3.241 | 0.002 |
| 0–4 yrs | - | - | - | - | - | - | |
| 5–14 yrs | −0.374 | −0.493 | −0.255 | −0.740 | −6.226 | <0.001 | |
| Fever | TOTAL | 0.122 | 0.047 | 0.196 | 0.410 | 3.235 | 0.002 |
| 0–4 yrs | 0.056 | −0.160 | 0.272 | 0.063 | 0.511 | 0.610 | |
| 5–14 yrs | 0.174 | 0.066 | 0.304 | 0.322 | 2.638 | 0.009 | |
| Cough | TOTAL | −0.004 | −0.076 | 0.068 | −0.020 | −0.110 | 0.913 |
| 0–4 yrs | −0.208 | −0.440 | 0.024 | −0.342 | −1.771 | 0.079 | |
| 5–14 yrs | −0.016 | −0.155 | 0.122 | −0.044 | −0.236 | 0.814 | |
| Influenza | TOTAL | 0.096 | 0.035 | 0.158 | 0.424 | 3.104 | 0.002 |
| 0–4 yrs | 0.038 | −0.142 | 0.218 | 0.056 | 0.419 | 0.676 | |
| 5–14 yrs | 0.219 | 0.104 | 0.335 | 0.529 | 3.753 | <0.001 | |
| Common Cold | TOTAL | −0.081 | −0.134 | −0.029 | −0.305 | −3.061 | 0.003 |
| 0–4 yrs | −0.056 | −0.224 | 0.112 | −0.071 | −0.664 | 0.508 | |
| 5–14 yrs | −0.151 | −0.251 | −0.050 | −0.310 | −2.966 | 0.005 | |
| Decrease in appetite | TOTAL | 0.017 | −0.019 | 0.053 | 0.050 | 0.941 | 0.348 |
| 0–4 yrs | 0.109 | −0.010 | 0.228 | 0.107 | 1.813 | 0.072 | |
| 5–14 yrs | 0.040 | −0.026 | 0.106 | 0.063 | 1.190 | 0.236 | |
| WIKI–Human Respiratory Syncytial Virus | TOTAL | 0.001 | −0.001 | 0.003 | 0.062 | 0.753 | 0.453 |
| 0–4 yrs | 0.005 | −0.004 | 0.013 | 0.108 | 1.106 | 0.271 | |
| 5–14 yrs | 0.002 | −0.003 | 0.006 | 0.062 | 0.715 | 0.476 | |
| WIKI–Bronchiolitis | TOTAL | −0.008 | −0.015 | −0.001 | −0.152 | −2.173 | 0.032 |
| 0–4 yrs | −0.041 | −0.066 | −0.016 | −0.264 | −3.262 | 0.001 | |
| 5–14 yrs | −0.019 | −0.033 | −0.006 | −0.202 | −2.782 | 0.006 | |
| WIKI–Influenza | TOTAL | 0.001 | 0.000 | 0.001 | 0.198 | 1.494 | 0.138 |
| 0–4 yrs | 0.001 | −0.001 | 0.002 | 0.066 | 0.885 | 0.378 | |
| 5–14 yrs | 0.001 | 0.001 | 0.002 | 0.245 | 3.531 | 0.001 | |
| WIKI–Pneumonia | TOTAL | −0.001 | −0.003 | 0.001 | −0.164 | −0.692 | 0.490 |
| 0–4 yrs | - | - | - | - | - | - | |
| 5–14 yrs | - | - | - | - | - | - | |
| WIKI–Bronchitis | TOTAL | 0.000 | −0.004 | 0.004 | −0.005 | −0.054 | 0.957 |
| 0–4 yrs | - | - | - | - | - | - | |
| 5–14 yrs | −0.004 | −0.010 | 0.002 | −0.100 | −1.368 | 0.174 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Baldassarre, A.; Provenzano, S.; Corrado, S.; Cerviere, M.P.; Parisi, S.; Marchesi, F.; Bottazzoli, M. Infodemiology of RSV in Italy (2017–2022): An Alternative Option for the Surveillance of Incident Cases in Pediatric Age? Children 2022, 9, 1984. https://doi.org/10.3390/children9121984
Riccò M, Baldassarre A, Provenzano S, Corrado S, Cerviere MP, Parisi S, Marchesi F, Bottazzoli M. Infodemiology of RSV in Italy (2017–2022): An Alternative Option for the Surveillance of Incident Cases in Pediatric Age? Children. 2022; 9(12):1984. https://doi.org/10.3390/children9121984
Chicago/Turabian StyleRiccò, Matteo, Antonio Baldassarre, Sandro Provenzano, Silvia Corrado, Milena Pia Cerviere, Salvatore Parisi, Federico Marchesi, and Marco Bottazzoli. 2022. "Infodemiology of RSV in Italy (2017–2022): An Alternative Option for the Surveillance of Incident Cases in Pediatric Age?" Children 9, no. 12: 1984. https://doi.org/10.3390/children9121984