
The Importance of Monitoring and Factors That May Influence Leg Length Difference in Developmental Dysplasia of the Hip
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
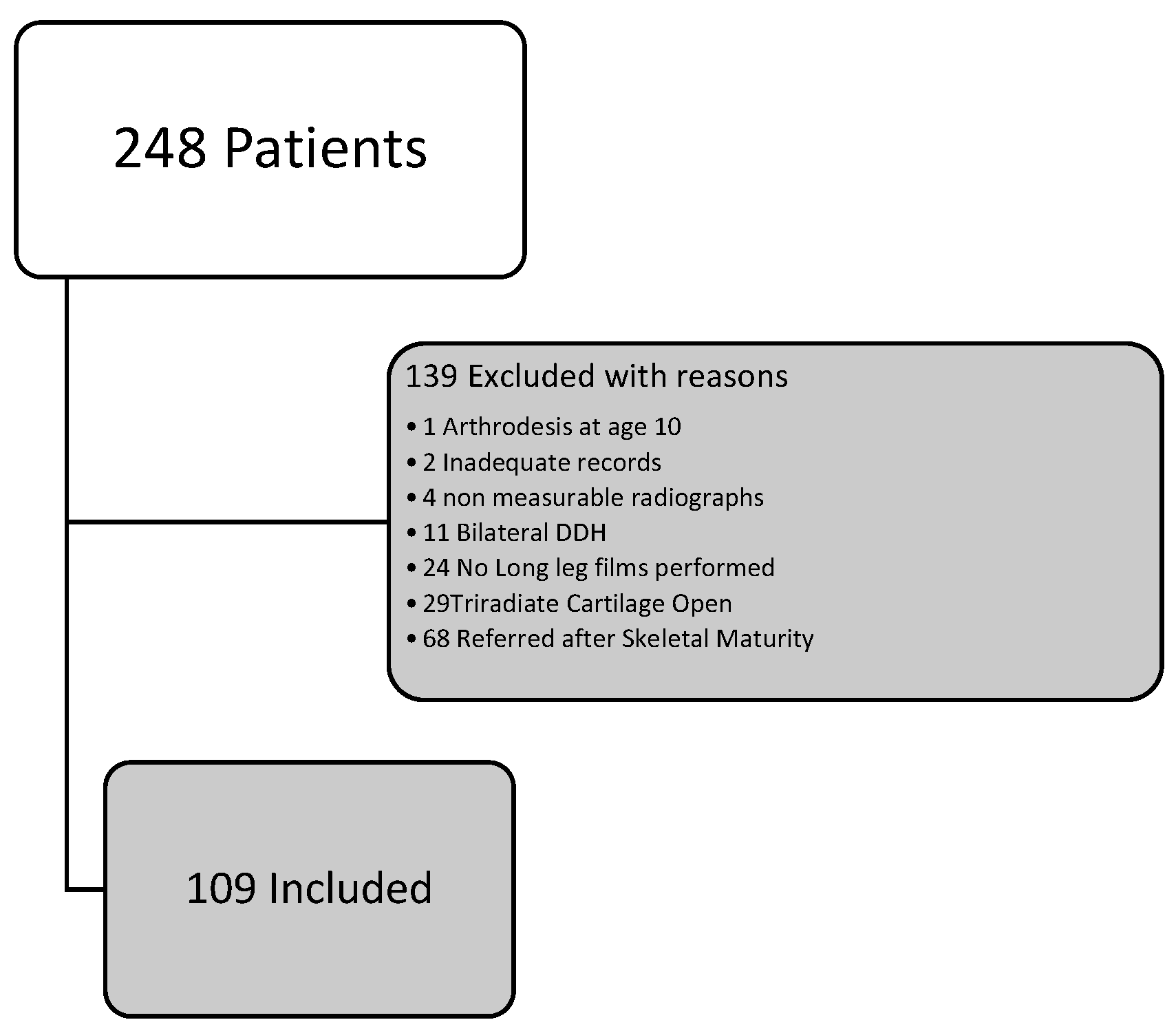
2.1. Data Collection
- (1)
- Successful closed reduction;
- (2)
- Failed (or successful) closed reduction proceeding to an open reduction without bone surgery;
- (3)
- Reduction proceeding to a femoral osteotomy;
- (4)
- Reduction proceeding to a pelvic osteotomy;
- (5)
- Reduction proceeding to a femoral and pelvic osteotomy.
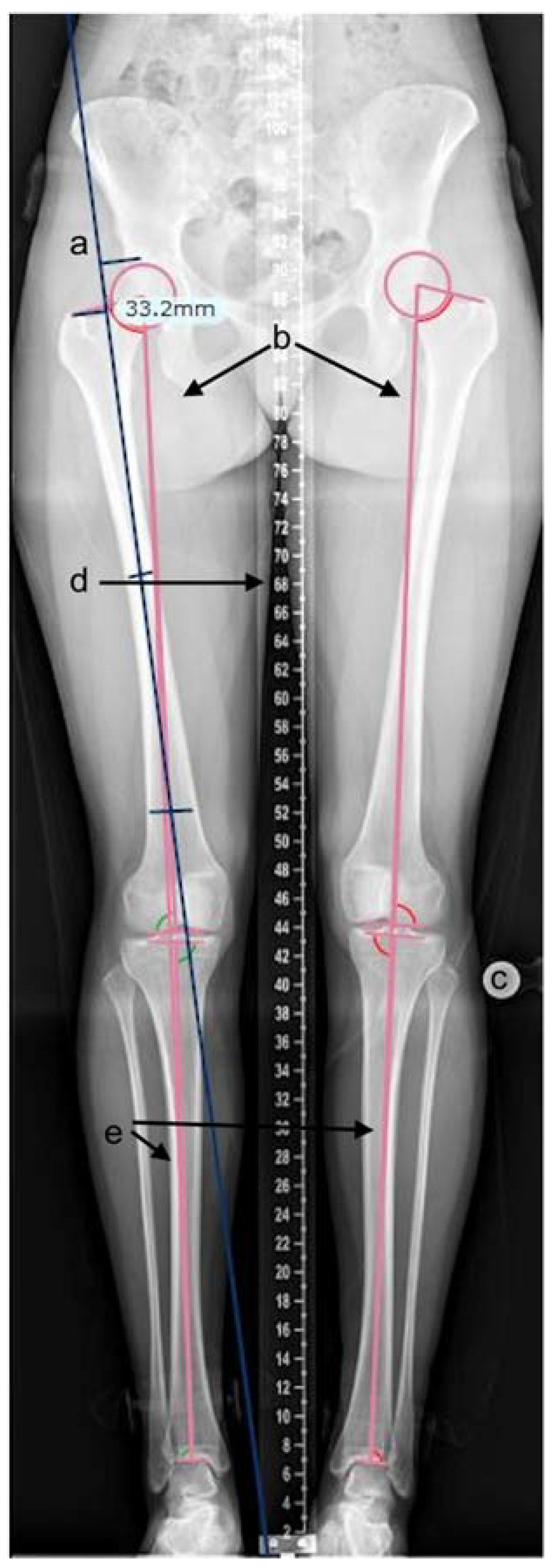
2.2. Radiographic Measurements
2.3. Statistical Analysis
3. Results
3.1. Avascular Necrosis
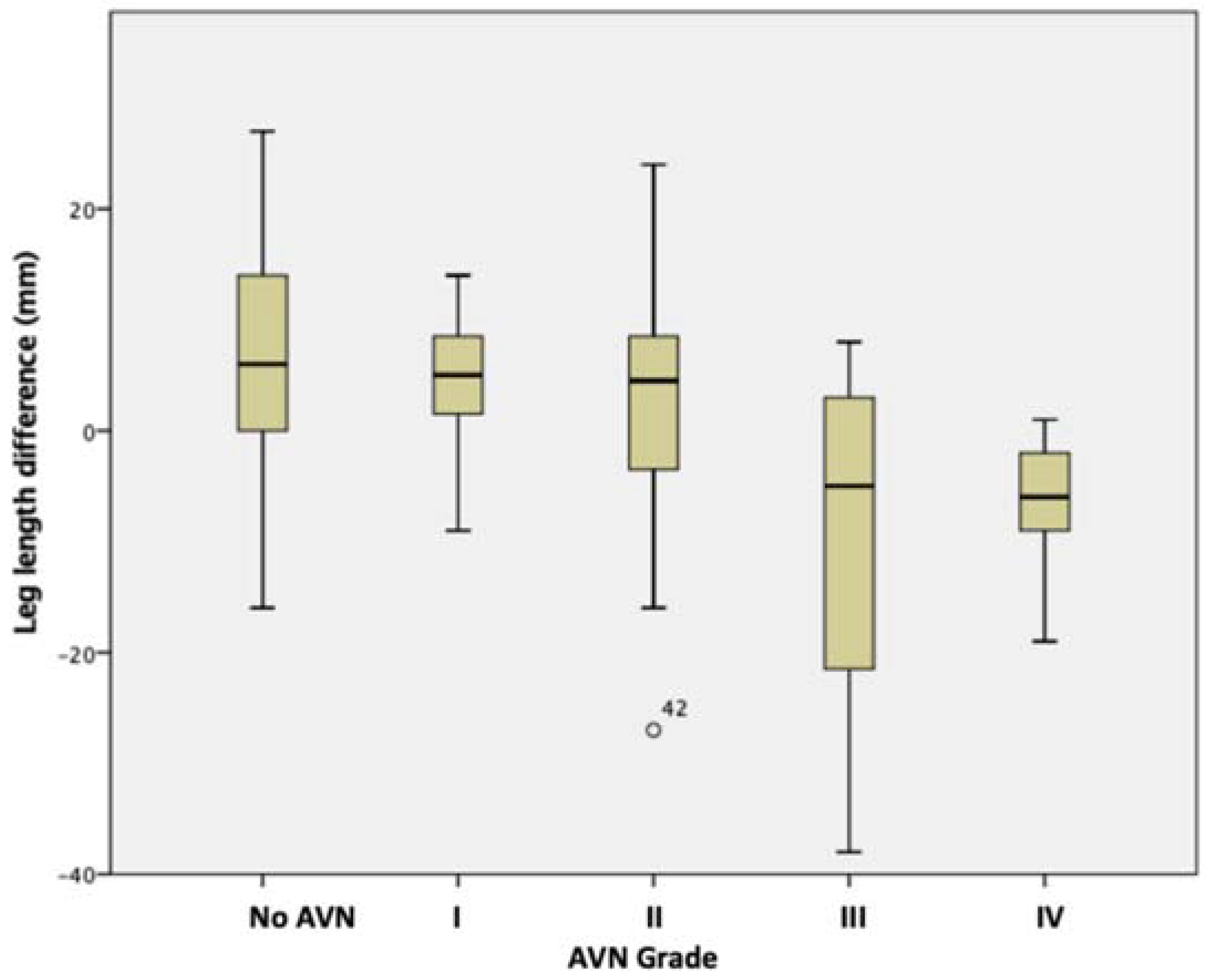
3.2. Leg Length and Segmental Differences
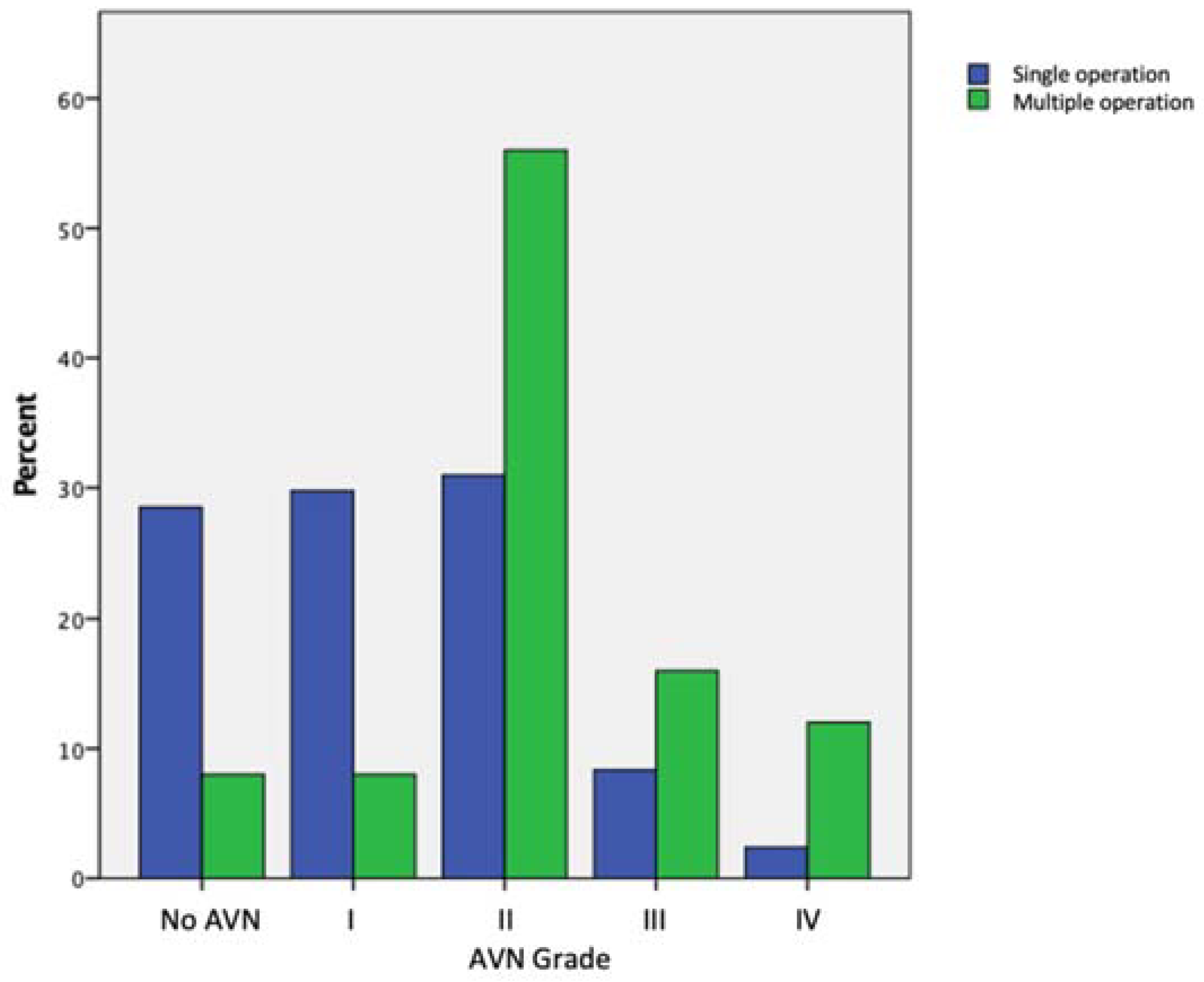
3.3. Interventions for Leg Length Difference
4. Discussion
4.1. Leg Length Discrepancy in DDH
4.2. Consequences of LLD in DDH
4.3. Appropriate Monitoring of LLD in DDH
4.4. Treatment of LLD in DDH
4.5. Influence of AVN on LLD in DDH
4.6. Consequences of Untreated Leg Length Discrepancy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ponseti, I.V. Growth and development of the acetabulum in the normal child. Anatomical, histological, and roentgenographic studies. J. Bone Jt. Surg.-Ser. A. 1978, 60, 575–585. [Google Scholar] [CrossRef]
- Weinstein, S.L. Natural history of congenital hip dislocation (CDH) and hip dysplasia. Clin. Orthop. Relat. Res. 1987, 225, 62–76. [Google Scholar] [CrossRef]
- Gillingham, B.L.; Sanchez, A.A.; Wenger, D.R. Pelvic osteotomies for the treatment of hip dysplasia in children and young adults. J. Am. Acad. Orthop. Surg. 1999, 7, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Bøhm, P.; Weber, G. Salter’s innominate osteotomy for hip dysplasia in adolescents and young adults: Results in 58 patients (69 osteotomies) at 4–12 years. Acta Orthop. Scand. 2003, 74, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.P.; Doddabasappa, S.N.; Mulpuri, K. Evidence-based management of developmental dysplasia of the hip. Orthop. Clin. N. Am. 2014, 45, 341–354. [Google Scholar] [CrossRef]
- Nishiyama, T.; Saegusa, Y.; Fujishiro, T.; Hayashi, S.; Kanzaki, N.; Hashimoto, S.; Kurosaka, M. Long-term results of intertrochanteric varus osteotomy for the dysplastic hip. Hip. Int. 2012, 22, 628–632. [Google Scholar] [CrossRef]
- Yoon, C.; Shin, C.H.; Kim, D.O.; Park, M.S.; Yoo, W.J.; Chung, C.Y.; Choi, I.H.; Cho, T.J. Overgrowth of the lower limb after treatment of developmental dysplasia of the hip: Incidence and risk factors in 101 children with a mean follow-up of 15 years. Acta Orthop. 2020, 91, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Metcalfe, J.E.; Banaszkiewicz, P.; Kapoor, B.; Richardson, J.; Jones, C.W.; Kuiper, J. Unexpected long femur in adults with acetabular dysplasia. Acta Orthop. Belg. 2005, 71, 424–428. [Google Scholar]
- Tamura, K.; Takao, M.; Hamada, H.; Ando, W.; Sakai, T.; Sugano, N. Femoral morphology asymmetry in hip dysplasia makes radiological leg length measurement inaccurate. Bone Jt. J. 2019, 101, 297–302. [Google Scholar] [CrossRef]
- Inan, M.; Chan, G.; Bowen, J.R. The correction of leg-length discrepancy after treatment in developmental dysplasia of the hip by using a percutaneous epiphysiodesis. J. Pediatr. Orthop. Part B. 2008, 17, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Zadeh, H.G.; Catterall, A.; Hashemi-Nejad, A.; Perry, R.E. Test of stability as an aid to decide the need for osteotomy in association with open reduction in developmental dysplasia of the hip. A long term review. J. Bone Jt. Surg.-Ser. B. 2000, 82, 17–27. [Google Scholar] [CrossRef]
- Khamis, S.; Carmeli, E. Relationship and significance of gait deviations associated with limb length discrepancy: A systematic review. Gait Posture 2017, 57, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.E.; Davis, L.E. Leg Length Discrepancy: The Natural History (And What Do We Really Know). J. Pediatr. Orthop. 2019, 39, S10–S13. [Google Scholar] [CrossRef] [PubMed]
- Harvey, W.F.; Yang, M.; Cooke, T.D.; Segal, N.A.; Lane, N.; Lewis, C.E.; Felson, D.T. Association of leg-length inequality with knee osteoarthritis a cohort study. Ann. Intern. Med. 2010, 152, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Murray, K.J.; Azari, M.F. Leg length discrepancy and osteoarthritis in the knee, hip and lumbar spine. J. Can. Chiropr. Assoc. 2015, 59, 226–237. [Google Scholar] [PubMed]
- ten Brinke, A.; Van Der Aa, H.E.; van der Palen, J.; Oosterveld, F. Is leg length discrepancy associated with the side of radiating pain in patients with a lumbar herniated disc? Spine 1999, 24, 684–686. [Google Scholar] [CrossRef]
- Campbell, T.M.; Ghaedi, B.B.; Tanjong Ghogomu, E.; Welch, V. Shoe Lifts for Leg Length Discrepancy in Adults With Common Painful Musculoskeletal Conditions: A Systematic Review of the Literature. Arch. Phys. Med. Rehabil. 2018, 99, 981–993.e2. [Google Scholar] [CrossRef]
- Renkawitz, T.; Weber, T.; Dullien, S.; Woerner, M.; Dendorfer, S.; Grifka, J.; Weber, M. Leg length and offset differences above 5 mm after total hip arthroplasty are associated with altered gait kinematics. Gait Posture 2016, 49, 196–201. [Google Scholar] [CrossRef]
- Guo, S.J.; Zhou, Y.X.; Yang, D.J.; Yang, X.C. Lower-limb valgus deformity associated with developmental hip dysplasia. Chin. Med. J. 2012, 125, 3956–3960. [Google Scholar] [CrossRef]
- Zhang, Z.; Luo, D.; Cheng, H.; Xiao, K.; Zhang, H. Unexpected long lower limb in patients with unilateral hip dislocation. J. Bone Jt. Surg.-Am. Vol. 2018, 100, 388–395. [Google Scholar] [CrossRef]
- Makarov, M.R.; Jackson, T.J.; Smith, C.M.; Jo, C.H.; Birch, J.G. Timing of epiphysiodesis to correct leg-length discrepancy: A comparison of prediction methods. J. Bone Jt. Surg.-Am. Vol. 2018, 100, 1217–1222. [Google Scholar] [CrossRef]
- Tolk, J.J.; Merchant, R.; Eastwood, D.M.; Buddhdev, P.; Hashemi-Nejad, A. The Development of Leg Length Difference and Influence on Persistent Dysplasia in Patients with Developmental Dysplasia of the Hip. Indian J. Orthop. 2021, 55, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Tallroth, K.; Ristolainen, L.; Manninen, M. Is a long leg a risk for hip or knee osteoarthritis? Acta Orthop. 2017, 88, 512–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, J.; Tudor, F.; Luff, T.; Hashemi-Nejad, A. Surveillance after treatment of children with developmental dysplasia of the hip: Current UK practice and the proposed Stanmore protocol. J. Pediatr. Orthop. Part B. 2013, 22, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Segev, E.; Hemo, Y.; Wientroub, S.; Ovadia, D.; Fishkin, M.; Steinberg, D.M.; Hayek, S. Intra- and interobserver reliability analysis of digital radiographic measurements for pediatric orthopedic parameters using a novel PACS integrated computer software program. J. Child. Orthop. 2010, 4, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Kalamchi, A.; MacEwen; G.D. Avascular Necrosis Following Treatment of Hip Dislocation. Citeseer. 1980, 62, 876–888. [Google Scholar] [CrossRef]
- Weinstein, S.L.; Dolan, L.A. Proximal femoral growth disturbance in developmental dysplasia of the hip: What do we know? J. Child. Orthop. 2018, 12, 331–341. [Google Scholar] [CrossRef]
- Knutson, G.A. Anatomic and functional leg-length inequality: A review and recommendation for clinical decision-making. Part I, anatomic leg-length inequality: Prevalence, magnitude, effects and clinical significance. Chiropr. Osteopat. 2005, 13, 11. [Google Scholar] [CrossRef] [Green Version]
- Tolk, J.; Eastwood, D.; Hashemi-Nejad, A. Femoral Morphological Changes and The Role of Contralateral Epiphysiodesis in Patients with Legg-Calvé-Perthes Disease. Orthop. Proc. 2021, 103, 8. [Google Scholar] [CrossRef]
- Song, K.M.; Halliday, S.E.; Little, D.G. The effect of limb-length discrepancy on gait. J. Bone Jt. Surg. Am. 1997, 79, 1690–1698. [Google Scholar] [CrossRef]
- Gurney, B.; Mermier, C.; Robergs, R.; Gibson, A.; Rivero, D. Effects of limb-length discrepancy on gait economy and lower-extremity muscle activity in older adults. J. Bone Jt. Surg. Am. 2001, 83, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Sabharwal, S.; Kumar, A. Methods for assessing leg length discrepancy. Clin. Orthop. Relat. Res. 2008, 466, 2910–2922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolk, J.J.; Merchant, R.; Calder, P.R.; Hashemi-Nejad, A.; Eastwood, D.M. Tension-band Plating for Leg-length Discrepancy Correction. Strateg. Trauma Limb Reconstr. 2022, 17, 19–25. [Google Scholar] [CrossRef]
- Applebaum, A.; Nessim, A.; Cho, W. Overview and Spinal Implications of Leg Length Discrepancy: Narrative Review. Clin. Orthop. Surg. 2021, 13, 127–134. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | n = 109 |
|---|---|
| Mean age at referral with range in years | 2.7 (0–13) |
| Mean age at diagnosis with range in years | 1.5 (0–10.5) |
| Mean age at follow-up with range in years | 15.2 (10.6 to 49.9) |
| Side affected | Right 51/Left 58 |
| Sex | Female 95/male 14 |
| Surgical procedure Groups (Last surgical Procedure) | n = 109 |
| Closed reduction | 17 (15.8%) |
| Open reduction only | 17(15.8%) |
| Reduction + Femoral osteotomy | 30 (27.5%) |
| Reduction + Pelvic osteotomy | 15 (13.6%) |
| Reduction + Pelvic and femoral | 30 (27.3%) |
| Total | 109(100%) |
| Multiple Surgeries (bone and/or soft tissue) | 25/109 (23%) |
| Values presented as mean with standard deviation between brackets for continuous variables and count with percentages between brackets for dichotomous variables. | |
| Age of First Surgery | Total | ||
|---|---|---|---|
| ≤3 years | >3 years | ||
| No AVN | 26/95 (27.4%) | 0 | 26 (23.9%) |
| AVN Type I | 24/95 (25.3%) | 3/14 (21.4%) | 27 (24.8%) |
| AVN Type II | 32/95 (33.7%) | 8/14 (57.1%) | 40 (36.7%) |
| AVN Type III | 9/95 (9.5%) | 2/14 (14.3%) | 11 (10.1%) |
| AVN Type IV | 4/95 (4.2%) | 1/14 (7.1%) | 5 (4.6%) |
| Total | 95 (100.0%) | 14 (100.0%) | 109 (100.0%) |
| Segmental Leg Length Difference | DDH Leg Longer (Mean Length Difference in mm, CI) (n = 72) | DDH Leg Shorter (Mean Length Difference in mm, CI) (n = 34) | ||
|---|---|---|---|---|
| Total leg length discrepancy | 8.25 (6.8, 9.6) | p < 0.001 | −9.5 (−12, −6.4) | p < 0.001 |
| Femoral length difference | 7.5 (6.04, 8.8) | p < 0.001 | −6.5 (−9.6, −3.2) | p < 0.001 |
| Tibial difference in | 0.5 (−0.5, 1.4) | p = 0.3 | −1.9 (−4.2, 0.3) | p = 0.09 |
| Articulo-trochanteric distance difference | 0.28 (−0.9, 1.4)) | p = 0.63 | −5.2 (−9.2, −1.01) | p = 0.016 |
| Diaphyseal length difference | 7.1 (5.4, 8.9) | p < 0.001 | −1.32 (−5.9, 3.3) | p = 0.565 |
| Frequency (n [%]) | OR | 95% CI | |
|---|---|---|---|
| Closed reduction (n = 17) | 4/17 (23.5%) | 0.78 | (0.23–2.62) |
| Open reduction (n = 18) | 2/18 (11.1%) | 0.31 | (0.07–1.42) |
| Femoral osteotomy (n = 30) | 11/30 (36.7%) | 1.83 | (0.74–4.52) |
| Pelvic osteotomy (n = 15) | 4/15 (26.7%) | 0.95 | (0.28–3.26) |
| Pelvic and femoral (n = 29) | 9/29 (31.0%) | 1.18 | (0.47–2.99) |
| Multiple operations (n = 25) | 9/25 (36.0%) | 1.69 | (0.65–4.38) |
| Frequency (f/n [%]) | OR | 95% CI | |
|---|---|---|---|
| No AVN/Type I (n = 53) | 15/53 (28.3%) | 1.08 | (0.47–2.50) |
| Type II (n = 40) | 8/40 (20.0 %) | 0.53 | (0.21–1.35) |
| Type III (n = 11) | 3/11 (27.3%) | 0.99 | (0.24–4.00) |
| Type IV (n = 5) | 4/5 (80%) | 12.00 | (1.28–112.25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merchant, R.M.; Tolk, J.J.; Ayub, A.A.; Eastwood, D.M.; Hashemi-Nejad, A. The Importance of Monitoring and Factors That May Influence Leg Length Difference in Developmental Dysplasia of the Hip. Children 2022, 9, 1945. https://doi.org/10.3390/children9121945
Merchant RM, Tolk JJ, Ayub AA, Eastwood DM, Hashemi-Nejad A. The Importance of Monitoring and Factors That May Influence Leg Length Difference in Developmental Dysplasia of the Hip. Children. 2022; 9(12):1945. https://doi.org/10.3390/children9121945
Chicago/Turabian StyleMerchant, Rajiv M., Jaap J. Tolk, Anouska A. Ayub, Deborah M. Eastwood, and Aresh Hashemi-Nejad. 2022. "The Importance of Monitoring and Factors That May Influence Leg Length Difference in Developmental Dysplasia of the Hip" Children 9, no. 12: 1945. https://doi.org/10.3390/children9121945