
Role of Cardiovascular Imaging in the Follow-Up of Patients with Fontan Circulation
 , , ,
, , ,
Abstract
:1. Introduction
2. Echocardiography in Fontan Circulation
2.1. Segmental Analysis
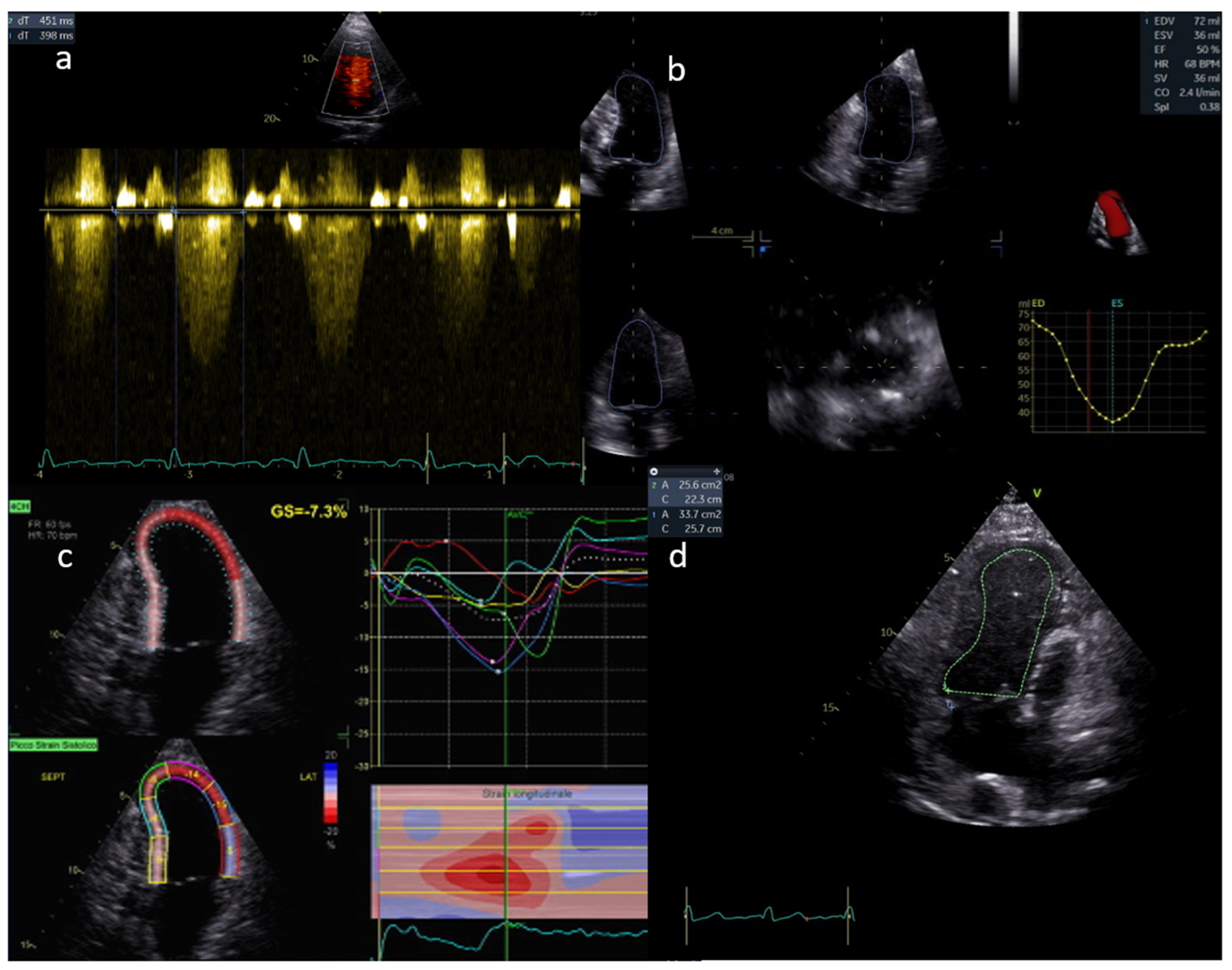
2.2. Single Ventricle Function
2.3. Atrio-Ventricular Valve Function
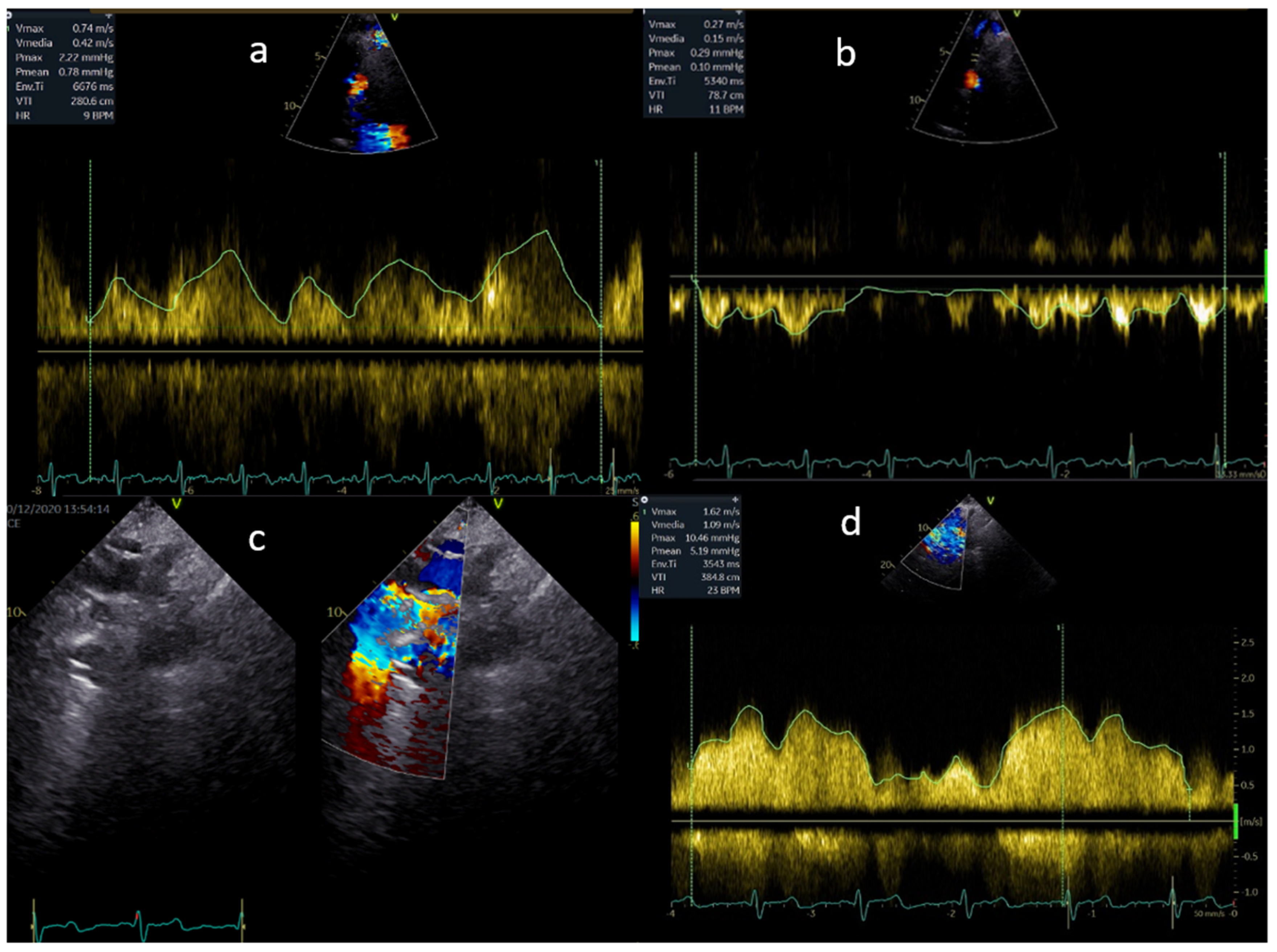
2.4. Venous and Arterial Pathway
2.5. Fenestration Flow
2.6. Collateral Flow
2.7. Transoesophageal Echocardiography
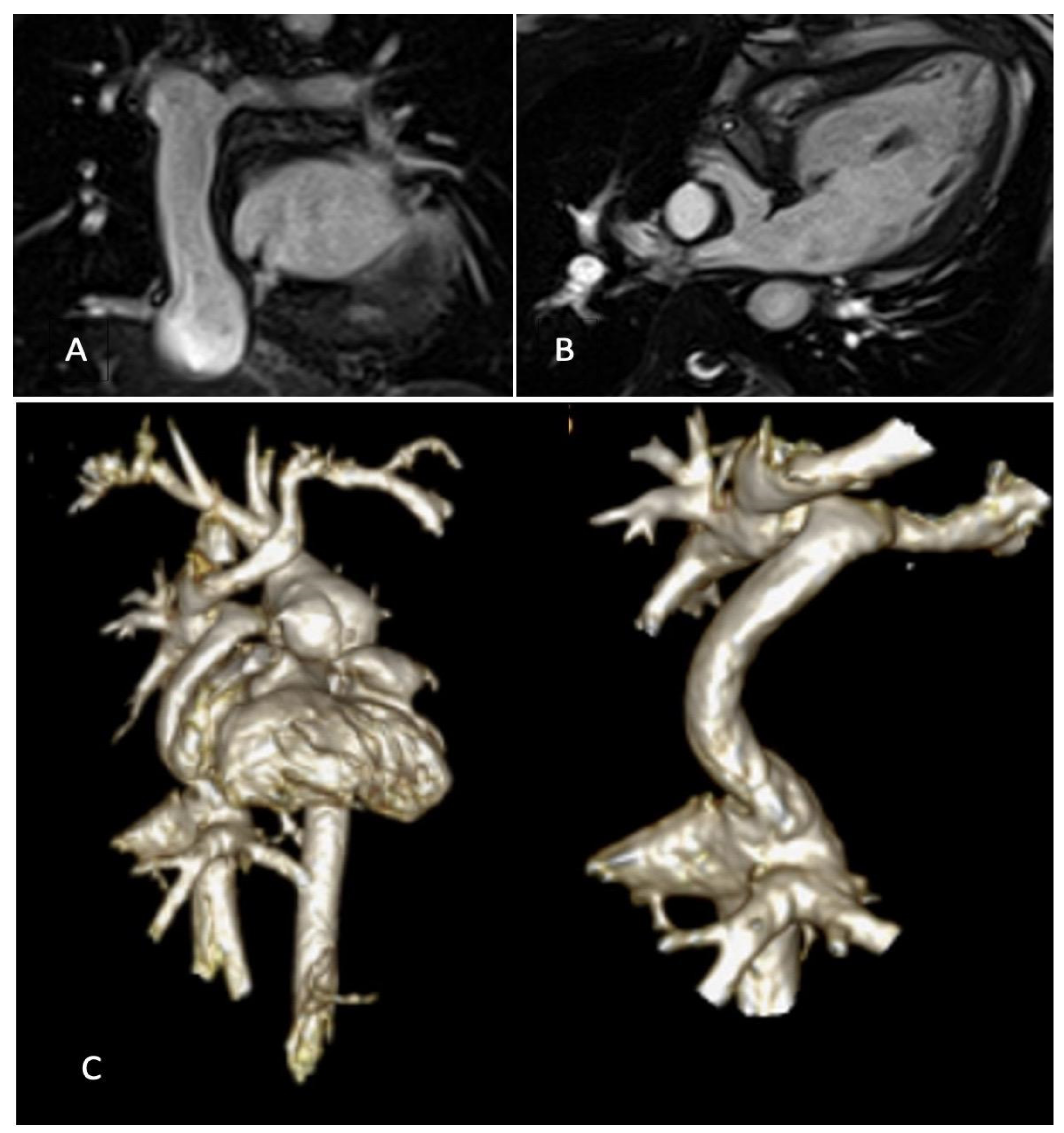
3. Cardiovascular Magnetic Resonance in Fontan Circulation
3.1. CMR Protocol
3.2. Use of CMR for Identification of Fontan Circuit Complications
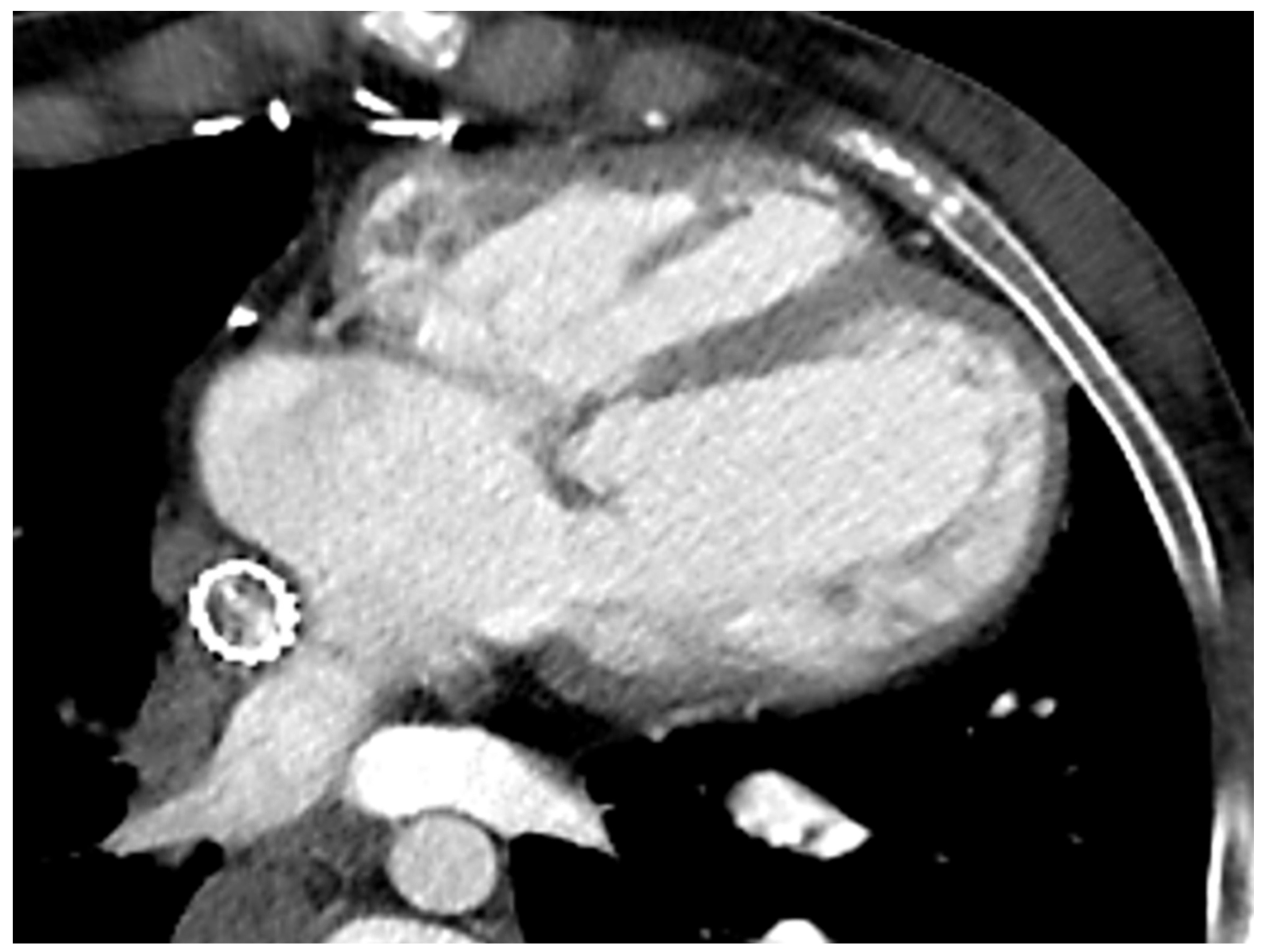
4. Cardiac Computed Tomography in Fontan Circulation
5. Cardiac Catheterisation in Fontan
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| 2D | Two-dimensional |
| 3D | Three-dimensional |
| 4D | Four-dimensional |
| ASD | Atrial septal defect |
| AV | Atrioventricular |
| AVM | Arterious venosus malformation |
| AZY | Azygous vein |
| bSSFP | Balanced steady-state free precession |
| CCT | Cardiac computed tomography |
| CT CHD | Computed tomography Congenital heart diseaseC |
| CHDs | Congenital heart diseases |
| CMR | Cardiovascular magnetic resonance |
| Dp/dt | Rates of ventricular pressure change |
| D-looping | Dextro-looping |
| EGE | Early gadolinium enhancement |
| ECG | Electrocardiogram |
| FNH-like | Focal nodular hyperplasia-like |
| GCS | Global circumferential strain |
| HLHS | Hypoplastic left heart syndrome |
| HV | Hepatic vein |
| IVC | Inferior vena cava |
| L-looping | Levo-looping |
| LGE | Late gadolinium enhancement |
| LPA | Left pulmonary artery |
| LS | Longitudinal strain |
| LV | Left ventricle |
| MAPCAs | Major aortopulmonary collateral arteries |
| PCI | Phase-contrast imaging |
| RV | Right ventricle |
| STE | Speckle-tracking echocardiography |
| SV | Single ventricle |
| SVC | Superior vena cava |
| RPA | Right pulmonary artery |
| TCPC | Total cavo pulmonary conduit |
| TTE | Transthoracic echocardiography |
| VSD | Ventricular septal defect |
| VV | Venovenous |
References
- Baker, D.W.; Dennis, M.R.; Zannino, D.; Schilling, C.; Moreno, P.D.; Bullock, A.; Disney, P.; Radford, D.J.; Hornung, T.; Grigg, L.; et al. Path ahead for ’low risk’ adolescents living with a Fontan circulation. Heart 2021, 107, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Fogel, M.A.; Weinberg, P.M.; Fellows, K.E.; Hoffman, E.A. A Study in ventricular-ventricular interaction: Single right ventricles compared with systemic right ventricles in a dual chambered circulation. Circulation 1995, 92, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Gewillig, M.; Brown, S.C.; van de Bruaene, A.; Rychik, J. Providing a framework of principles for conceptualising the Fontan circulation. Acta Paediatr. 2020, 109, 651–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rychik, J.; Atz, A.M.; Celermajer, D.S.; Deal, B.J.; Gatzoulis, M.A.; Gewillig, M.H.; Hsia, T.Y.; Hsu, D.T.; Kovacs, A.H.; McCrindle, B.W.; et al. American Heart Association Council on Cardiovascular Disease in the Young and Council on Cardiovascular and Stroke Nursing. Evaluation and Management of the Child and Adult With Fontan Circulation: A Scientific Statement From the American Heart Association. Circulation 2019, 140, e234–e284. [Google Scholar] [CrossRef] [PubMed]
- Brida, M.; Lovrić, D.; Griselli, M.; Riesgo Gil, F.; Gatzoulis, M.A. Heart failure in adults with congenital heart disease. Int. J. Cardiol. 2022, 357, 39–45. [Google Scholar] [CrossRef]
- Trusty, P.M.; Wei, Z.; Rychik, J.; Russo, P.A.; Surrey, L.F.; Goldberg, D.J.; Fogel, M.A.; Yoganathan, A.P. Impact of hemodynamics and fluid energetics on liver fibrosis after Fontan operation. J. Thorac. Cardiovasc. Surg. 2018, 156, 267–275. [Google Scholar] [CrossRef]
- Sutherland, G.R.; Di Salvo, G.; Claus, P.; D’hooge, J.; Bijnens, B. Strain and strain rate imaging: A new clinical approach to quantifying regional myocardial function. J. Am. Soc. Echocardiogr. 2004, 17, 788–802. [Google Scholar] [CrossRef]
- Borrelli, N.; Di Salvo, G.; Sabatino, J.; Ibrahim, A.; Avesani, M.; Sirico, D.; Josen, M.; Penco, M.; Fraisse, A.; Michielon, G.; et al. Serial changes in longitudinal strain are associated with outcome in children with hypoplastic left heart syndrome. Int. J. Cardiol. 2020, 317, 56–62. [Google Scholar] [CrossRef]
- Meyer, S.L.; St Clair, N.; Powell, A.J.; Geva, T.; Rathod, R.H. Integrated clinical and magnetic resonance imaging assessments late after Fontan operation. J. Am. Coll. Cardiol. 2021, 77, 2480. [Google Scholar] [CrossRef]
- Baumgartner, H.; De Backer, J.; Babu-Narayan, S.V.; Budts, W.; Chessa, M.; Diller, G.P.; Lung, B.; Kluin, J.; Lang, I.M.; Meijboom, F.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur. Heart J. 2021, 42, 563–645. [Google Scholar] [CrossRef]
- Kheiwa, A.; Harris, I.S.; Varadarajan, P. A practical guide to echocardiographic evaluation of adult Fontan patients. Echocardiography 2020, 37, 2222–2230. [Google Scholar] [CrossRef]
- Vitarelli, A.; Conde, Y.; Cimino, E.; D’Angeli, I.; D’Orazio, S.; Ventriglia, F.; Bosco, G.; Colloridi, V. Quantitative assessment of systolic and diastolic ventricular function with tissue Doppler imaging after Fontan type of operation. Int. J. Cardiol. 2005, 102, 61–69. [Google Scholar] [CrossRef]
- Bunting, K.V.; Formisano, F.; Green, J.; Steeds, R.P.; Hudsmith, L.; Clift, P. Assessing Univentricular Function in Adult Fontan Using 3D Echocardiography. Congenit. Heart Dis. 2020, 15, 89–100. [Google Scholar]
- Cheung, Y.F.; Penny, D.J.; Redington, A.N. Serial assessment of left ventricular diastolic function after Fontan procedure. Heart 2000, 83, 420–424. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.Q.; Conway, J.; Alvarez, S.; Goot, B.; Serrano-Lomelin, J.; Colen, T.; Tham, E.B.; Kutty, S.; Li, L. Reduced Right Ventricular Fractional Area Change, Strain, and Strain Rate before Bidirectional Cavopulmonary Anastomosis is Associated with Medium-Term Mortality for Children with Hypoplastic Left Heart Syndrome. J. Am. Soc. Echocardiogr. 2018, 31, 831–842. [Google Scholar] [CrossRef]
- Petko, C.; Hansen, J.H.; Scheewe, J.; Rickers, C.; Kramer, H.H. Comparison of longitudinal myocardial deformation and dyssynchrony in children with left and right ventricular morphology after the Fontan operation using two-dimensional speckle tracking. Congenit. Heart Dis. 2012, 7, 16–23. [Google Scholar] [CrossRef]
- Borrelli, N.; Sabatino, J.; Avesani, M.; Paredes, J.; Josen, M.; Fraisse, A.; Guccione, P.; Michielon, G.; Di Salvo, G. Longitudinal Evaluation of Right Ventricle Function after Right Ventricle-Pulmonary Artery Shunt vs. Blalock-Taussig Shunt. Congenit. Heart Dis. 2021, 16, 27–37. [Google Scholar] [CrossRef]
- Borrelli, N.; Avesani, M.; Sabatino, J.; Ibraim, A.; Josen, M.; Paredes, J.; Di Salvo, G. Blood speckle imaging: A new echocardiographic approach to study fluid dynamics in congenital heart disease. Int. J. Cardiol. Congenit. Heart Dis. 2021, 2, 100079. [Google Scholar] [CrossRef]
- Colquitt, J.L.; Loar, R.W.; Morris, S.A.; Feagin, D.K.; Sami, S.; Pignatelli, R.H. Serial strain analysis identifies Hypoplastic Left Heart Syndrome infants at risk for Cardiac morbidity and mortality: A pilot study. J. Am. Soc. Echocardiogr. 2019, 32, 643–650. [Google Scholar] [CrossRef]
- Rösner, A.; McElhinney, D.B.; Diab, S.G.; Friedberg, M.K.; Lui, G.K. Classic-Pattern Dyssynchrony Is Associated with Outcome in Patients with Fontan Circulation. J. Am. Soc. Echocardiogr. 2022, 35, 513–522. [Google Scholar] [CrossRef]
- Cordina, R.; von Klemperer, K.; Kempny, A.; West, C.; Senior, R.; Celermajer, D.S.; Gatzoulis, M.A.; Babu-Narayan, S.V.; Li, W. Echocardiographic Predictors of Mortality in Adults With a Fontan Circulation. JACC Cardiovasc. Imaging 2017, 10, 212–213. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, S.; Akazawa, Y.; Obinata, H.; Motoki, N.; Takei, K.; Yasukochi, S.; Takigiku, K. Ventricular myocardial response to exercise in patients with Fontan circulation. J. Echocardiogr. 2021, 19, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Jani, V.; Craft, M.; Olson, J.; Schuster, A.; Pedrizzetti, G.; Danford, D.; Kutty, S. Ventricular Flow Profile in Young Patients with Single Left Ventricle Fontan using Echocardiographic Contrast Particle Imaging Velocimetry. J. Am. Soc. Echocardiogr. 2022. [Google Scholar] [CrossRef] [PubMed]
- Kutty, S.; Rathod, R.H.; Danford, D.A.; Celermajer, D.S. Role of imaging in the evaluation of single ventricle with the Fontan palliation. Heart 2016, 102, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, M.; Breuer, J.; Steger, V.; Steil, E.; Sieverding, L.; Ziemer, G. Incidence and impact of systemic venous collateral development after Glenn and Fontan procedures. J. Thorac. Cardiovasc. Surg. 2001, 49, 172–178. [Google Scholar] [CrossRef]
- Puchalski, M.D.; Lui, G.K.; Miller-Hance, W.C.; Brook, M.M.; Young, L.T.; Bhat, A.; Roberson, D.A.; Mercer-Rosa, L.; Miller, O.I.; Parra, D.A.; et al. Guidelines for Performing a Comprehensive Transesophageal Echocardiographic: Examination in Children and All Patients with Congenital Heart Disease: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1373–1378. [Google Scholar] [CrossRef]
- Von Knobelsdorff-Brenkenhoff, F.; Schulz-Menger, J. Role of cardiovascular magnetic resonance in the guidelines of the European Society of Cardiology. J. Cardiovasc. Magn. Reson. 2016, 18, 6. [Google Scholar] [CrossRef] [Green Version]
- Kilner, P.J.; Geva, T.; Kaemmerer, H.; Trindade, P.T.; Schwitter, J.; Webb, G.D. Recommendations for cardiovascular magnetic resonance in adults with congenital heart disease from the respective working groups of the European Society of Cardiology. Eur. Heart J. 2010, 31, 794–805. [Google Scholar] [CrossRef] [Green Version]
- Ridgway, J.P. Cardiovascular magnetic resonance physics for clinicians: Part I. J. Cardiovasc. Magn. Reson. 2010, 12, 71. [Google Scholar] [CrossRef] [Green Version]
- Valsangiacomo Buechel, E.R.; Grosse-Wortmann, L.; Fratz, S.; Eichhorn, J.; Sarikouch, S.; Greil, G.F.; Beerbaum, P.; Bucciarelli-Ducci, C.; Bonello, B.; Sieverding, L.; et al. Indications for cardiovascular magnetic resonance in children with congenital and acquired heart disease: An expert consensus paper of the Imaging Working Group of the AEPC and the Cardiovascular Magnetic Resonance Section of the EACVI. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 281–297. [Google Scholar] [CrossRef]
- Do, C.; DeAguero, J.; Brearley, A.; Trejo, X.; Howard, T.; Escobar, G.P.; Wagner, B. Gadolinium-Based Contrast Agent Use, Their Safety, and Practice Evolution. Kidney360 2020, 1, 561–568. [Google Scholar] [CrossRef]
- Shellock, F.G.; Woods, T.O.; Crues, J.V., 3rd. MR labeling information for implants and devices: Explanation of terminology. Radiology 2009, 253, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Nazarian, S.; Hansford, R.; Roguin, A.; Goldsher, D.; Zviman, M.M.; Lardo, A.C.; Caffo, B.S.; Frick, K.D.; Kraut, M.A.; Kamel, I.R.; et al. A prospective evaluation of a protocol for magnetic resonance imaging of patients with implanted cardiac devices. Ann. Intern. Med. 2011, 155, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Nazarian, S.; Beinart, R.; Halperin, H.R. Magnetic resonance imaging and implantable devices. Circ. Arrhythmia Electrophysiol. 2013, 6, 419–428. [Google Scholar] [CrossRef] [Green Version]
- Ciliberti, P.; Ciancarella, P.; Bruno, P.; Curione, D.; Bordonaro, V.; Lisignoli, V.; Panebianco, M.; Chinali, M.; Secinaro, A.; Galletti, L.; et al. Cardiac Imaging in Patients After Fontan Palliation: Which Test and When? Front. Pediatr. 2022, 16, 876742. [Google Scholar] [CrossRef]
- Puricelli, F.; Voges, I.; Gatehouse, P.; Rigby, M.; Izgi, C.; Pennell, D.J.; Krupickova, S. Performance of Cardiac MRI in Pediatric and Adult Patients with Fontan Circulation. Radiol. Cardiothorac. Imaging 2022, 4, e210235. [Google Scholar] [CrossRef]
- Yeong, M.; Loughborough, W.; Hamilton, M.; Manghat, N. Role of cardiac MRI and CT in Fontan circulation. J. Congenit. Cardiol. 2017, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Fratz, S.; Chung, T.; Greil, G.F.; Samyn, M.M.; Taylor, A.M.; Valsangiacomo Buechel, E.R.; Yoo, S.J.; Powell, A.J. Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J. Cardiovasc. Magn. Reson. 2013, 15, 51. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, J.C.; Lyen, S.M.; Loughborough, W.; Amadu, A.M.; Baritussio, A.; Dastidar, A.G.; Manghat, N.E.; Bucciarelli-Ducci, C. Extra-cardiac findings in cardiovascular magnetic resonance: What the imaging cardiologist needs to know. J. Cardiovasc. Magn. Reson. 2016, 18, 26. [Google Scholar] [CrossRef] [Green Version]
- Rijnberg, F.M.; Westenberg, J.J.M.; van Assen, H.C.; Juffermans, J.F.; Kroft, L.J.M.; van den Boogaard, P.J.; Terol Espinosa de Los Monteros, C.; Warmerdam, E.G.; Leiner, T.; Grotenhuis, H.B.; et al. 4D flow cardiovascular magnetic resonance derived energetics in the Fontan circulation correlate with exercise capacity and CMR-derived liver fibrosis/congestion. J. Cardiovasc. Magn. Reson. 2022, 24, 21. [Google Scholar] [CrossRef]
- Triedman, J.K.; Bridges, N.D.; Mayer, J.E.J.; Lock, J.E. Prevalence and risk factors for aortopulmonary collateral vessels after Fontan and bidirectional Glenn procedures. J. Am. Coll. Cardiol. 1993, 22, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Prakash, A.; Rathod, R.H.; Powell, A.J.; McElhinney, D.B.; Banka, P.; Geva, T. Relation of systemic-to-pulmonary artery collateral flow in single ventricle physiology to palliative stage and clinical status. Am. J. Cardiol. 2012, 109, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Ghelani, S.J.; Harrild, D.M.; Gauvreau, K.; Geva, T.; Rathod, R.H. Comparison between echocardiography and cardiac magnetic resonance imaging in predicting transplant-free survival after the Fontan operation. Am. J. Cardiol. 2015, 116, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- d’Udekem, Y.; Iyengar, A.J.; Cochrane, A.D.; Grigg, L.E.; Ramsay, J.M.; Wheaton, G.R.; Penny, D.J.; Brizard, C.P. The Fontan procedure: Con-temporary techniques have improved long-term outcomes. Circulation 2007, 116 (Suppl. S11), 157–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haggerty, C.M.; Restrepo, M.; Tang, E.; de Zélicourt, D.A.; Sundareswaran, K.S.; Mirabella, L.; Bethel, J.; Whitehead, K.K.; Fogel, M.A.; Yoganathan, A.P. Fontan hemodynamics from 100 patient-specific cardiac magnetic resonance studies: A computational fluid dynamics analysis. J. Thorac. Cardiovasc. Surg. 2014, 148, 1481–1489. [Google Scholar] [CrossRef] [Green Version]
- Francone, M.; Gimelli, A.; Budde, R.P.J.; Caro-Dominguez, P.; Einstein, A.J.; Gutberlet, M.; Maurovich-Horvat, P.; Miller, O.; Nagy, E.; Natale, L.; et al. Radiation safety for cardiovascular computed tomography imaging in paediatric cardiology: A joint expert consensus document of the EACVI, ESCR, AEPC, and ESPR. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e279–e289. [Google Scholar] [CrossRef]
- Rappaport, B.; Mellon, R.D.; Simone, A.; Woodcock, J. Defining safe use of anesthesia in children. N. Engl. J. Med. 2011, 364, 1387–1390. [Google Scholar] [CrossRef]
- Nievelstein, R.A.J.; Van Dam, I.M.; Van Der Molen, A.J. Multidetector CT in children: Current concepts and dose reduction strategies. Pediatric. Radiol. 2010, 40, 1324–1344. [Google Scholar] [CrossRef] [Green Version]
- Dennis, M.; Zannino, D.; du Plessis, K.; Bullock, A.; Disney, P.J.S.; Radford, D.J.; Hornung, T.; Grigg, L.; Cordina, R.; d’Udekem, Y.; et al. Clinical Outcomes in Adolescents and Adults After the Fontan Procedure. J. Am. Coll. Cardiol. 2018, 71, 1009–1017. [Google Scholar] [CrossRef]
- Raman, S.V.; Shah, M.; McCarthy, B.; Garcia, A.; Ferketich, E.A.K. Multi-detector row cardiac computed tomography accurately quantifies right and left ventricular size and function compared with cardiac magnetic resonance. Am. Heart J. 2006, 151, 736–744. [Google Scholar] [CrossRef]
- Ghadimi Mahani, M.; Agarwal, P.P.; Rigsby, C.K.; Lu, J.C.; Fazeli Dehkordy, S.; Wright, R.A.; Dorfman, A.L.; Krishnamurthy, R. CT for Assessment of Thrombosis and Pulmonary Embolism in Multiple Stages of Single-Ventricle Palliation: Challenges and Suggested Protocols. Radiographics 2016, 36, 1273–1284. [Google Scholar] [CrossRef]
- Kumar, P.; Bhatia, E.M. Computed Tomography in the Evaluation of Fontan Circulation. J. Cardiovasc. Imaging 2021, 29, 108–122. [Google Scholar] [CrossRef]
- Boggs, R.; Dibert, T.; Co-Vu, J.; DeGroff, C.; Quinn, N.; Chandran, E.A. Optimized Computed Tomography Angiography Protocol for the Evaluation of Thrombus in Patients with Fontan Anatomy. Pediatr. Cardiol. 2020, 41, 1601–1607. [Google Scholar] [CrossRef]
- Hagler, D.J.; Miranda, W.R.; Haggerty, B.J.; Anderson, J.H.; Johnson, J.N.; Cetta, F.; Said, S.M.; Taggart, N.W. Fate of the Fontan connection: Mechanisms of stenosis and management. Congenit. Heart Dis. 2019, 14, 571–581. [Google Scholar] [CrossRef]
- Jalal, Z.; Gewillig, M.; Boudjemline, Y.; Guérin, P.; Pilati, M.; Butera, G.; Malekzadeh-Milani, S.; Avesani, M.; Thambo, J.B. Transcatheter interventions in patients with a Fontan circulation: Current practice and future developments. Front. Pediatr. 2022, 10, 965989. [Google Scholar] [CrossRef]
- Venturi, A.; Piscaglia, F.; Vidili, G.; Flori, S.; Righini, R.; Golfieri, R.; Bolondi, L. Diagnosis and management of hepatic focal nodular hyperplasia. J. Ultrasound 2007, 10, 116–127. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.K.; Jang, H.-J.; Khalili, K.; Wald, R.M.; Yoo, S.-J.; Kim, E.T.K. CT and MR imaging findings of the livers in adults with Fontan palliation: An observational stud, Abdom. Radiol. N.Y. 2020, 45, 188–202. [Google Scholar] [CrossRef]
- Patel, N.D.; Sullivan, P.M.; Sabati, A.; Hill, A.; Maedler-Kron, C.; Zhou, S.; Shillingford, N.; Williams, R.; Takao, C.; Badran, S. Routine Surveillance Catheterization is Useful in Guiding Management of StableFontan Patients. Pediatr. Cardiol. 2020, 41, 624–631. [Google Scholar] [CrossRef]
- Stumper, O.; Penford, G. Catheter hemodynamic assessment of the univentricular circulation. Ann. Pediatric Cardiol. 2017, 10, 167–174. [Google Scholar] [CrossRef]
- Wilkinson, J.L. Haemodynamic calculations in the catheter laboratory. Heart 2001, 85, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Fontan, F.; Baudet, E. Surgical repair of tricuspid atresia. Thorax 1971, 26, 240–248. [Google Scholar] [CrossRef] [PubMed]
- De Leval, M.R.; Kilner, P.; Gewillig, M.; Bull, C. Total cavopulmonary connection: A logical alternative to atriopulmonary connection for complex Fontan operations. Experimental studies and early clinical experience. J. Thorac. Cardiovasc. Surg. 1988, 96, 682695. [Google Scholar] [CrossRef]
- Fogel, M.A.; Anwar, S.; Broberg, C.; Chung, T.; Johnson, T.; Muthurangu, V.; Taylor, M.; Valsangiacomo-Buechel, E.; Wilhelm, C. Society for Cardiovascular Magnetic Resonance/European Society of Cardiovascular Imaging/American Society of Echocardiography/Society for Pediatric Radiology/North American Society for Cardiovascular Imaging Guidelines for the Use of Cardiac Magnetic Resonance in Pediatric Congenital and Acquired Heart Disease: Endorsed by The American Heart Association. Circ. Cardiovasc. Imaging 2022, 15, e014415. [Google Scholar] [PubMed]
- Venna, A.; Cetta, F., Jr.; d’Udekem, Y. Fontan candidacy, optimizing Fontan circulation, and beyond. JTCVS Open 2021, 9, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Park, P.W.; Atz, A.M.; Taylor, C.L.; Chowdhury, S.M. Speckle-Tracking Echocardiography Improves Pre-operative Risk Stratification Before the Total Cavopulmonary Connection. J. Am. Soc. Echocardiogr. 2017, 30, 478–484. [Google Scholar] [CrossRef] [Green Version]
- Fuchigami, T.; Nagashima, M.; Hiramatsu, T.; Matsumura, G.; Tateishi, M.; Masuda, N.; Yamazaki, K. Long-term follow-up of Fontan completion in adults and adolescents. J. Card. Surg. 2017, 32, 436–442. [Google Scholar] [CrossRef]
- Schwartz, I.; McCracken, C.E.; Petit, C.J.; Sachdeva, R. Late outcomes after the Fontan procedure in patients with single ventricle: A meta-analysis. Heart 2018, 104, 1508–1514. [Google Scholar] [CrossRef]
- Gewillig, M.; Goldberg, D.J. Failure of the fontan circulation. Heart Fail. Clin. 2014, 10, 105–116. [Google Scholar] [CrossRef]
- Edwards, R.M.; Reddy, G.P.; Kicska, G. The functional single ventricle: How imaging guides treatment. Clin. Imaging 2016, 40, 1146–1155. [Google Scholar] [CrossRef]
- Sato, T.; Calderon, R.J.; Klas, B.; Pedrizzetti, G.; Banerjee, A. Simultaneous Volumetric and Functional Assessment of the Right Ventricle in Hypoplastic Left Heart Syndrome After Fontan Palliation, Utilizing 3-Dimensional Speckle-Tracking Echocardiography. Circ. J. 2020, 84, 235–244. [Google Scholar] [CrossRef] [Green Version]
- Soriano, B.D.; Hoch, M.; Ithuralde, A.; Geva, T.; Powell, A.J.; Kussman, B.D.; Graham, D.A.; Tworetzky, W.; Marx, G.R. Matrix-array 3-dimensional echocardiographic assessment of volumes, mass, and ejection fraction in young pediatric patients with a functional single ventricle: A comparison study with cardiac magnetic resonance. Circulation 2008, 117, 1842–1848. [Google Scholar] [CrossRef]
- Mah, K.; Khoo, N.S.; Martin, B.J.; Maruyama, M.; Alvarez, S.; Rebeyka, I.M.; Smallhorn, J.; Colen, T. Insights from 3D Echocardiography in Hypoplastic Left Heart Syndrome Patients Undergoing TV Repair. Pediatr. Cardiol. 2022, 43, 735–743. [Google Scholar] [CrossRef]
- Avesani, M.; Kang, S.L.; Jalal, Z.; Thambo, J.B.; Iriart, X. Renaissance of Cardiac Imaging to Assist Percutaneous Interventions in Congenital Heart Diseases:The Role of Three-Dimensional Echocardiography and Multimodality Imaging. Front. Pediatr. 2022, 19, 894472. [Google Scholar] [CrossRef]
- Di Salvo, G.; Miller, O.; Babu Narayan, S.; Li, W.; Budts, W.; Valsangiacomo Buechel, E.R.; Frigiola, A.; van den Bosch, A.E.; Bonello, B.; Mertens, L.; et al. 2016–2018 EACVI Scientific Documents Committee. Imaging the adult with congenital heart disease: A multimodality imaging approach-position paper from the EACVI. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1077–1098. [Google Scholar] [CrossRef]
- Secinaro, A.; Ait-Ali, L.; Curione, D.; Clemente, A.; Gaeta, A.; Giovagnoni, A.; Alaimo, A.; Esposito, A.; Tchana, B.; Sandrini, C.; et al. Recommendations for cardiovascular magnetic resonance and computed tomography in congenital heart disease: A consensus paper from the CMR/CCT working group of the Italian Society of Pediatric Cardiology (SICP) and the Italian College of Cardiac Radiology endorsed by the Italian Society of Medical and Interventional Radiology (SIRM) Part I. Radiol. Med. 2022, 127, 788–802. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Views Acquisition | Image |
|---|---|
| Subcostal | Visceral situs Cardiac position and orientation Atrio–ventricular and ventricular–arterial connection ASD and VSD assessment IVC Fontan connection Fenestration flow |
| Apical | Single-ventricle systolic function: o LV: Biplane Simpson o RV: FAC o Both: 3D EF, dP/dT, AV S/D ratio, STE Single-ventricle diastolic function: o Pulmonary venous atrial reversal flow o E-wave deceleration time AV valve morphology and function: o Regurgitation: § Qualitative assessment § Semi-quantitative assessment: vena contracta width, density, and shape of continuous doppler signal of regurgitant jet o Stenosis: § Mean and peak transvalve gradient · Outflow tract assessment · Semilunar valve morphology and function: o Regurgitation: § Qualitative assessment § Semi-quantitative assessment: vena contracta width o Stenosis: § Mean and peak transvalve gradient |
| Parasternal | VSD assessment AV valve morphology and function (see apical view) Outflow tract assessment Semilunar valve morphology and function (see apical view) |
| Suprasternal | Aortic arch obstruction Fontan connection and pulmonary artery flow assessment Collaterals visualisation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moscatelli, S.; Borrelli, N.; Sabatino, J.; Leo, I.; Avesani, M.; Montanaro, C.; Di Salvo, G. Role of Cardiovascular Imaging in the Follow-Up of Patients with Fontan Circulation. Children 2022, 9, 1875. https://doi.org/10.3390/children9121875
Moscatelli S, Borrelli N, Sabatino J, Leo I, Avesani M, Montanaro C, Di Salvo G. Role of Cardiovascular Imaging in the Follow-Up of Patients with Fontan Circulation. Children. 2022; 9(12):1875. https://doi.org/10.3390/children9121875
Chicago/Turabian StyleMoscatelli, Sara, Nunzia Borrelli, Jolanda Sabatino, Isabella Leo, Martina Avesani, Claudia Montanaro, and Giovanni Di Salvo. 2022. "Role of Cardiovascular Imaging in the Follow-Up of Patients with Fontan Circulation" Children 9, no. 12: 1875. https://doi.org/10.3390/children9121875