
Effects of Adherence to Once-Daily Treatment on Lung Function, Bronchial Hyperreactivity and Health Outcomes in Adolescents with Mild-to-Moderate Asthmoka: A Twelve-Month Survey

Abstract
:1. Introduction
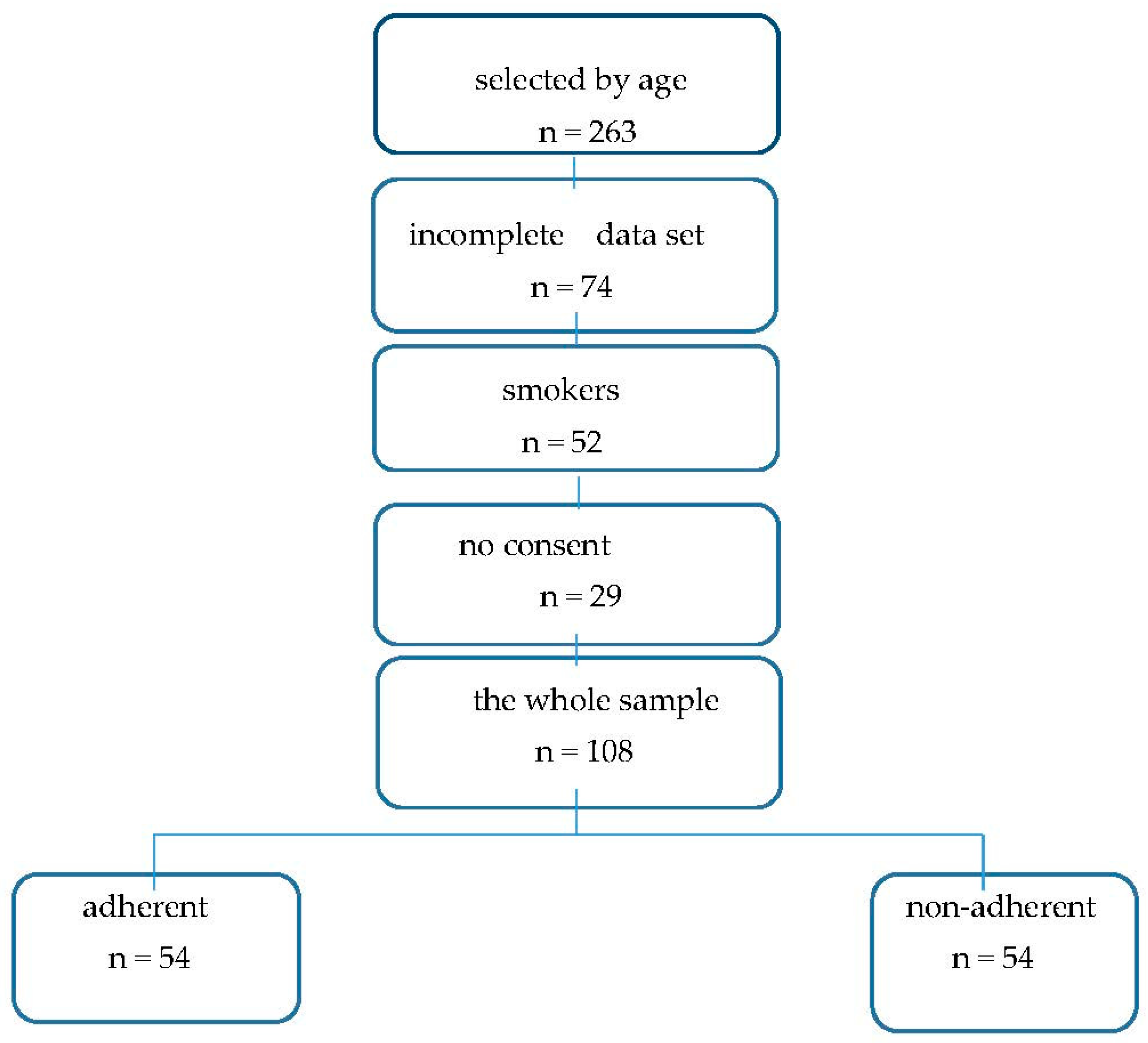
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Naimi, D.R.; Freedman, T.G.; Ginsburg, K.R.; Bogen, D.; Rand, C.S.; Apter, A.J. Adolescents and asthma: Why bother with our meds? J. Allergy Clin. Immunol. 2009, 123, 1335–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fidler, A.; Sweenie, R.; Ortega, A.; Cushing, C.C.; Ramsey, R.; Fedele, D. Meta-analysis of adherence promotion interventions in pediatric asthma. J. Ped. Psychol. 2021, 46, 119–212. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Physicians (RCP). The National Review of Asthma Deaths. Why Asthma Still Kills. 2015. Available online: https://www.rcplondon.ac.uk/projects/outputs/why-asthma-still-kills (accessed on 11 January 2018).
- Lenney, W.; Bush, A.; Fitzgerald, D.A.; Fletcher, M.; Ostrem, A.; Pedersen, S.; Szeflr, S.J.; Zar, H.J. Improving the global diagnosis and management of asthma in children. Thorax 2018, 73, 662–669. [Google Scholar] [CrossRef] [Green Version]
- Goeman, D.P.; Hogan, C.D.; Aroni, R.A.; Abramson, M.J.; Sawyer, S.M.; Stewart, K.; Sanci, L.A.; Douglass, J.A. Barriers to delivering asthma care: A qualitative study of general practitioners. Med. J. Aust. 2005, 183, 457–460. [Google Scholar] [CrossRef]
- Chipps, B.E.; Spahn, J.D. What are the determinants of asthma control? J. Asthma 2006, 43, 567–572. [Google Scholar] [CrossRef]
- Jebrak, G.; Houdouin, V.; Terrioux, P.; Maitre, B.; Ruppert, A.-M. Therapeutic adherence among asthma patients: Variations according to age groups. How can it be improved? The potential contributions of new technologies. Rev. Mal. Respir. 2022, 39, 442–454. [Google Scholar]
- Dut, R.; Soyer, O.; Sahiner, U.M.; Esemboga, S.; Gur Cetinkaya, P.G.; Akgul, S.; Derman, O.; Sekerel, B.E.; Kanbur, N. Psychological burden of asthma in adolescents and their parents. J. Asthma 2022, 59, 1116–1121. [Google Scholar] [CrossRef]
- Dinakar, C.; Brimer, A.G.; Adams, C.D.; Mahli, K. Social perceptions and adherence of youth in asthma. Mo. Med. 2006, 103, 553–556. [Google Scholar]
- Cheng, R.; Tan, Y.H.; Teoh, O.H.; Lee, J.H. Keeping pace with adolescent asthma: A practical approach to optimizing care. Pulm. Ther. 2022, 8, 123–137. [Google Scholar] [CrossRef]
- Ayala, G.X.; Miller, D.L.; Zagami, E.; Riddle, C.; Willis, S.; King, D. Asthma in middle school: What students have to say about their asthma. J. Sch. Health 2006, 76, 208–214. [Google Scholar] [CrossRef]
- Miller, B.D.; Wood, B.L. Childhood asthma in interaction with family, school, and peer systems: A developed model for primary care. J. Asthma 1991, 28, 405–414. [Google Scholar] [CrossRef]
- Sweenie, R.; Cushing, C.C.; Fleming, K.K.; Prabhakaran, S.; Fedele, D.A. daily adherence variability and psychosocial differences in adolescents with asthma: A pilot study. J. Behav. Med. 2022, 45, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Dozier, A.; Aligne, C.A.; Schlabach, M.B. What is asthma control? Discrepancies between patients’ perceptions and official definitions. J. Sch. Health 2006, 76, 215–218. [Google Scholar] [CrossRef]
- Crocker, D.; Brown, C.; Moolenaar, R.; Moorman, J.; Bailey, C.; Mannino, D.; Holguin, F. Racial and ethnic disparities in asthma medication usage and health-care utilization: Data from the National Asthma Survey. Chest 2009, 136, 1063–1071. [Google Scholar] [CrossRef]
- Bollinger, M.E.; Mudd, K.E.; Boldt, A.; Tsoukleris, M.G.; Butz, A.M. Prescription fill patterns in undeserved children with asthma receiving subspecialty care. Ann. Allergy Asthma Immunol. 2013, 111, 185–189. [Google Scholar] [CrossRef] [Green Version]
- Dal Negro, R.W.; Micheletto, C.; Bisato, R.; Trevisan, F.; Pomari, C.; Tognella, S. Associazione estemporanea o precostituita di beta2-adrenergico long-acting e steroide inalatorio nell’asma persistente lieve-moderato: Indagine telefonica in cieco per la valutazione della adesione alla terapia. It. J. Chest Dis. 2002, 56, 442–447. [Google Scholar]
- Voshaar, T.; Spinola, M.; Linnane, P.; Campanini, A.; Lock, D.; Lafratta, A.; Scuri, M.; Ronca, B.; Melani, A.S. Comparing usability of NEXThaler® with other inhaled corticosteroid/longacting β2-agonist fixed combination dry powder inhalers in asthma patients. J. Aerosol Med. Pulm. Drug Deliv. 2014, 27, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Gray, E.L.; Chang, V.; Thomas, P.S. Fluticasone furoate and vilanterol trifenatate combination therapy for the treatment of asthma. Expert Rev. Respir. Med. 2016, 10, 839–847. [Google Scholar] [CrossRef]
- Global Initiative on Asthma (GINA). Global Strategy for Asthma Management and Prevention. 2020. Available online: http://ginasthma.org/ (accessed on 22 November 2022).
- B.T.S. BTS/SIGN British Guideline on the Management of Asthma. 2016. Available online: https://www.brit.thoracic.org.UK/standardsofcare/guidelines/btssign-britishguideline-on-the-management-of-asthma/ (accessed on 1 January 2020).
- Rajesh, V.; Augustine, J.; Divya, R.; Cleetus, M. Inhaled formoterol-Fluticasone single inhaler therapy in asthma: Real-word efficacy, budget impact, and potential to improve adherence. Can. Resp. J. 2020, 2020, 8631316. [Google Scholar] [CrossRef]
- Tan, L.D.; Chan, A.L.; Albertson, T.E. New combination treatments in the management of asthma: Focus on fluticasone/vilanterol. J. Asthma Allergy 2014, 7, 77–83. [Google Scholar]
- Boole, G. Mathematical Analysis of Logic, Being an Essay towards a Calculus of Deductive Reasoning; MacMillan, Barclays & MacMillan, Cambridge and George Bell: London, UK, 1847; also reprinted by Basil Blackwell: London, UK, 1948. [Google Scholar]
- Crompton, G.K. Problems patients have using pressurized aerosol inhalers. Eur. J. Resp. Dis. 1982, 63 (Suppl. S119), 101–104. [Google Scholar]
- Milgrom, H.; Bender, B.; Ackerson, L.; Bowry, P.; Smith, B.; Rand, C. Noncompliance and treatment failure in children with asthma. J. Allergy Clin. Immunol. 1996, 98, 1051–1057. [Google Scholar] [CrossRef]
- Birkhead, G.; Attaway, N.J.; Strunk, R.C.; Towsend, M.C.; Teutsch, S. Investigation of a cluster of death of adolescents with asthma: Evidence implicating inadequate treatment and poor patient adherence with medications. J. Allery Clin. Immunol. 1989, 84, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Bruzzese, J.M.; Bonner, S.; Vincent, E.J.; Sheares, B.J.; Mellins, R.B.; Levison, M.J.; Wiesemann, S.; Du, Y.; Zimmerman, B.J.; Evans, D. Asthma education: The adolescent experience. Patient Educ. Couns. 2004, 55, 396–406. [Google Scholar] [CrossRef]
- Bender, B.; Zhang, L. Negative affect, medication adherence, and asthma control in children. J. Allergy Clin. Immunol. 2008, 122, 490–495. [Google Scholar] [CrossRef]
- Fleming, L.; Wilson, N.; Bush, A. Difficult to control asthma in children. Curr. Opin. Allergy Clin. Immunol. 2007, 7, 190–195. [Google Scholar] [CrossRef]
- Rabe, K.F.; Adachi, M.; Lai, C.K.V. Worldwide severity and asthma control in children and adults: The global asthma insight and reality surveys. J. Allergy Clin. Immunol. 2004, 114, 40–47. [Google Scholar] [CrossRef]
- Partridge, M.R. The asthma consultation: What is important? Curr. Med. Res. Opin. 2005, 21 (Suppl. S4), S11–S17. [Google Scholar] [CrossRef]
- Averell, C.M.; Laliberté, F.; German, G.; Shade, J.; Duh, M.S.; Spahn, J. Disease burden and treatment adherence among children and adolescent patients with asthma. J. Asthma 2022, 59, 1687–1696. [Google Scholar] [CrossRef]
- Bernstein, D.I.; Bateman, E.D.; Woodcock, A.; Toler, W.T.; Forth, R.; Jacques, L.; Nunn, C.; O’Byrne, P.M. Flu ticasone furoate (FF)/vilanterol (100/25 mcg or 200/25 mcg) or FF (100 mcg) in persistent asthma. J. Asthma 2015, 52, 1073–1083. [Google Scholar] [CrossRef]
- Slack, R.J.; Barrett, V.J.; Morrison, V.S.; Sturton, R.G.; Emmons, A.J.; Ford, A.J.; Knowles, R.G. In vitro pharmacological characterization of vilanterol, a novel long-acting β2-ad-renoceptor agonist with 24-hour duration of action. J. Pharmacol. Exp. Ther. 2013, 344, 218–230. [Google Scholar] [CrossRef] [Green Version]
- Dal Negro, R.W.; Bonadiman, L.; Turco, P. Fluticasone furoate/Vilanterol 92/22 μg once-a-day vs. Beclomethasone dipropionate/Formoterol 100/6 μg b.I.d.: A 12-month comparison of outcomes in mild-to-moderate asthma. Multidiscip. Respir. Med. 2018, 13, 18. [Google Scholar] [CrossRef] [Green Version]
- Rhee, H.; Belyea, M.J.; Clurzynski, S.; Brasch, J. Barriers to asthma self-management in adolescents: Relationships to psychological factors. Pediatr. Pulmonol. 2009, 44, 183–191. [Google Scholar] [CrossRef] [Green Version]
- Stridsman, C.; Backman, H.; Eklund, B.M.; Rönmark, E.; Hedman, L. Adolescent girls with asthma have worse asthma control and health related quality of life than boys. A population based study. Pediatr. Pulmonol. 2017, 52, 866–872. [Google Scholar] [CrossRef]
- Mancuso, C.A.; Peterson, M.G.E.; Charlson, M.E. Effects of depressive symptoms on health related quality of life in asthma patients. J. Gen. Intern. Med. 2000, 15, 300–310. [Google Scholar] [CrossRef]
- De Simoni, A.; Horne, R.; Fleming, L.; Bush, A.; Griffiths, C. What do adolescents with asthma really think about adherence to inhalers? Insight from a qualitative analysis of a UK online forum. BMJ Open 2017, 7, e015245. [Google Scholar] [CrossRef]
- Ulrik, C.S.; Backer, V.; Soes-Petersen, U.; Lange, P.; Harving, H.; Plaschke, P.P. The patient’s perspective: Adherence or non-adherence to asthma controller therapy. J. Asthma 2006, 43, 701–704. [Google Scholar] [CrossRef]
- Carpenter, D.M.; Geryk, L.L.; Sage, A.; Arrindell, C.; Sleath, B.L. Exploring the theoretical pathways through which asthma app features can promote adolescent self-management. TBM 2016, 6, 509–518. [Google Scholar] [CrossRef] [Green Version]
- Morton, R.W.; Everard, M.L.; Elphick, H.E. Adherence in childhood asthma: The elephant in the room. Arch. Dis. Chest 2014, 99, 949–953. [Google Scholar] [CrossRef]
- Murphy, J.; McSharry, J.; Hynes, L.; Molloy, G.J. A smartphone app to support adherence to inhaled corticosteroids in young adults with athma: Multi-Methods feasibility study. JMIR Form. Res. 2012, 5, e28784. [Google Scholar] [CrossRef]
- Timm, L.H.; Farrag, G.; Wolf, D.; Baxmann, M.; Schwendicke, F. Effect of electronic reminders on patients compliance during clear aligner treatment: An interrupetd time series study. Sci. Rep. 2022, 12, 16652. [Google Scholar] [CrossRef]
- Pai, A.L.; Mc Grady, M. Systematic review and meta-analysis of psychological interventions to promote treatment adherence in children, adolescents, and young adults with chronic illness. J. Pediatr. Psychol. 2014, 39, 918–931. [Google Scholar] [CrossRef] [Green Version]
- Dean, A.J.; Walters, J.; Hall, A. A systematic review of interventions to enhance medication adherence in children and adolescents with chronic illness. Arch. Dis. Child. 2010, 95, 717–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosnaim, G.S.; Pappalardo, A.A.; Resnick, S.E.; Codispoti, C.D.; Bandi, S.; Nackers, L.; Malik, R.N.; Vijayaraghavan, V.; Lynch, E.B.; Powell, L.H. Behavioural interventions to improve asthma outcomes for adolescents: A systematic review. J. Allergy Clin. Immunol. Pract. 2016, 4, 130–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos-Valente, E. Biologicals in childhood severe asthma: The EuropeanPERMEABLE survey on the status quo. Eur. Respir. J. 2021, 7, 00143–02021. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Subjects (n) | 108 |
| males/females (n) | 52/56 |
| mean age | 15.5 ± 1.8 |
| BMI | 21.8 ± 0.6 |
| Allegens (n) | |
| only seasonal | 22 |
| seasonal & perennial | 61 |
| only perennial | 25 |
| Lung function at recruitment | |
| FEV1 (% pred.) | 85.8 ± 14.7 |
| MMEF (% pred.) | 52.8 ± 18.7 |
| V25 (% pred.) | 45.2 ± 19.1 |
| PD20 FEV1 (mcg) | 877.4 ± 526.9 |
| Outcomes over the 6 months before recruitment | |
| Exacerbations (n) | 0.9 ± 0.9 |
| School days off (n) | 2.6 ± 2.3 |
| GP visits (n) | 1.4 ± 1.4 |
| Specialist visits (n) | 1.6 ± 1.2 |
| Steroid courses (n) | 0.9 ± 0.3 |
| Antibiotic courses (n) | 0.9 ± 1.0 |
| Compliant | Non-Compliant | |||||||
|---|---|---|---|---|---|---|---|---|
| At Recruitment | +6 Months | +12 Months | p | At Recruitment | 6 Months | 12 Months | p | |
| FEV1 (% pred.) | 85.2 ± 15.5 | 91.8 ± 17.1 | 93.7 ± 18.6 | 0.002 | 87.4 ± 14.1 | 88.1 ± 17.2 | 87.6 ± 204.4 | ns |
| MMEF (% pred.) | 51.4 ± 17.3 | 55.8 ± 16.1 | 57.3 ± 17.4 | 0.001 | 52.9 ± 19.4 | 50.1 ± 20.6 | 48.7 ± 23.7 | ns |
| V25 (% pred.) | 44.8 ± 18.1 | 48.9 ± 18.2 | 50.7 ± 17.3 | 0.001 | 45.1 ± 19.5 | 39.9 ± 17.9 | 40.8 ± 20.7 | ns |
| PD20 FEV1 (mcg) | 807.1 ± 411.4 | 1289.7 ± 521.2 | 1408.6 ± 618.2 | 0.001 | 908.7 ± 544.1 | 894.2 ± 621.3 | 801.6 ± 704.2 | ns |
| Compliant | Non-Compliant | |||||||
|---|---|---|---|---|---|---|---|---|
| Over 6 Months before Recruitment | +6 Months | +12 Months | p | Over 6 Months before Recruitment | +6 Months | +12 Months | p | |
| Exacerbations (n) | 0.9 ± 0.8 | 0.5 ± 0.7 | 0.3 ± 0.6 | <0.002 | 0.8 ± 0.9 | 0.8 ± 0.9 | 0.9 ± 1.0 | ns |
| School days off (n) | 2.5 ± 2.5 | 0.4 ± 0.8 | 0.2 ± 0.8 | <0.001 | 2.7 ± 2.2 | 2.9 ± 2.3 | 2.7 ± 2.3 | ns |
| GP visits (n) | 1.6 ± 1.8 | 0.5 ± 0.8 | 0.2 ± 0.4 | <0.001 | 1.5 ± 1.1 | 1.7 ± 1.6 | 1.6 ± 1.6 | ns |
| Specialist visits (n) | 1.5 ± 1.3 | 0.9 ± 0.9 | 0.8 ± 0.7 | <0.002 | 1.7 ± 1.1 | 1.7 ± 1.2 | 1.7 ± 1.4 | ns |
| Steroid courses (n) | 0.9 ± 0.8 | 0.2 ± 0.4 | 0.1 ± 0.3 | <0.001 | 0.8 ± 0.9 | 0.7 ± 0.87 | 0.7 ± 1.0 | ns |
| Antibiotic courses (n) | 0.9 ± 1.1 | 0.4 ± 0.7 | 0.1 ± 0.3 | <0.001 | 0.9 ± 0.9 | 0.9 ± 0.9 | 0.8 ± 0.8 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dal Negro, R.W.; Turco, P. Effects of Adherence to Once-Daily Treatment on Lung Function, Bronchial Hyperreactivity and Health Outcomes in Adolescents with Mild-to-Moderate Asthmoka: A Twelve-Month Survey. Children 2022, 9, 1854. https://doi.org/10.3390/children9121854
Dal Negro RW, Turco P. Effects of Adherence to Once-Daily Treatment on Lung Function, Bronchial Hyperreactivity and Health Outcomes in Adolescents with Mild-to-Moderate Asthmoka: A Twelve-Month Survey. Children. 2022; 9(12):1854. https://doi.org/10.3390/children9121854
Chicago/Turabian StyleDal Negro, Roberto W., and Paola Turco. 2022. "Effects of Adherence to Once-Daily Treatment on Lung Function, Bronchial Hyperreactivity and Health Outcomes in Adolescents with Mild-to-Moderate Asthmoka: A Twelve-Month Survey" Children 9, no. 12: 1854. https://doi.org/10.3390/children9121854