

Under-Recognized Macrophage Activation Syndrome in Refractory Kawasaki Disease: A Wolf in Sheep’s Clothing

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Definitions
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Incidence of MAS in KD and Refractory KD
3.2. Comparison of Characteristics between the Two Groups
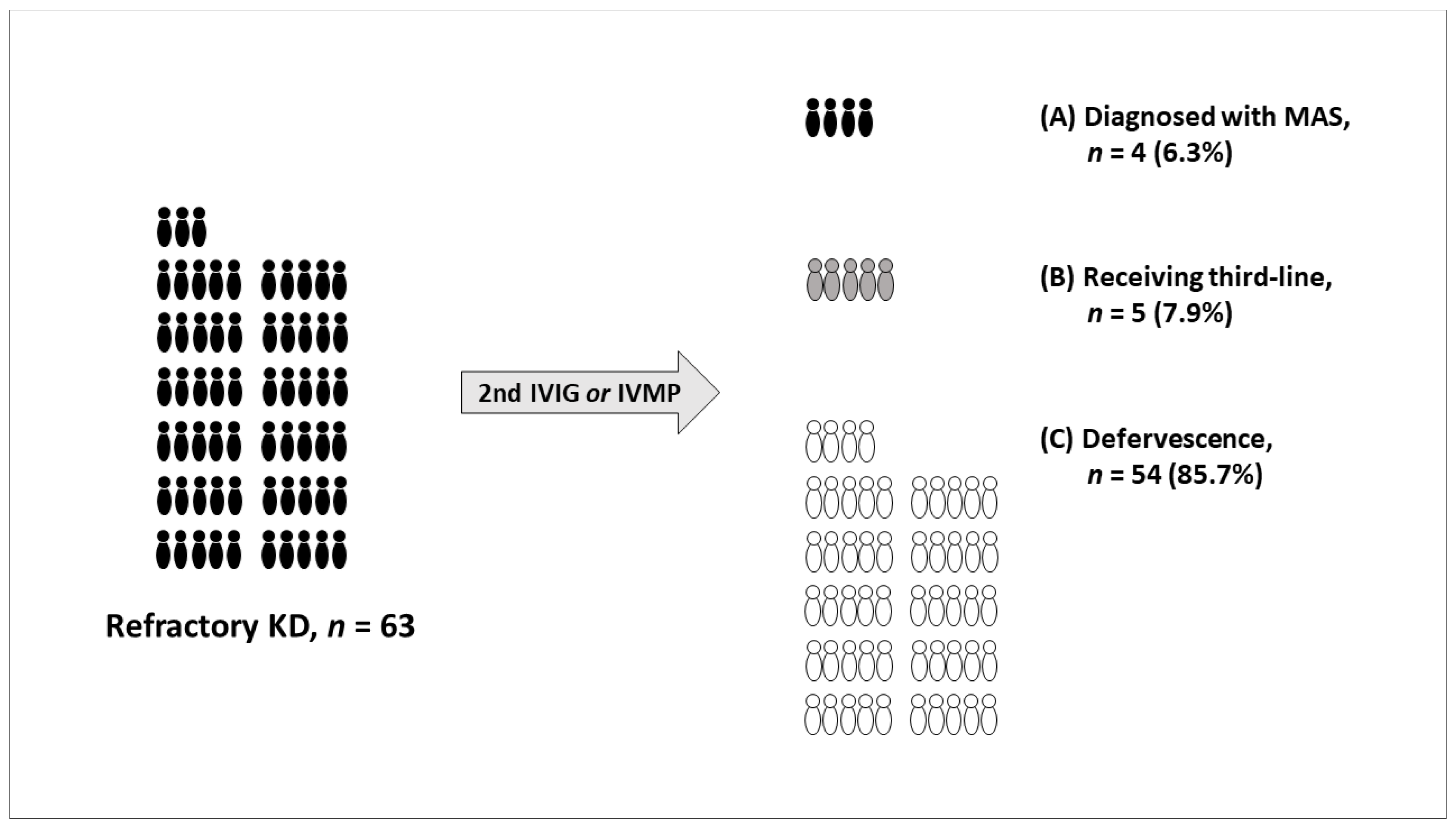
3.3. Patients Who Received Third-Line Treatment
3.4. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef] [PubMed]
- Han, S.B.; Lee, S.Y. Differentiating Kawasaki disease from urinary tract infection in febrile children with pyuria and C-reactive protein elevation. Ital. J. Pediatr. 2018, 44, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newburger, J.W.; Takahashi, M.; Burns, J.C.; Beiser, A.S.; Chung, K.J.; Duffy, C.E.; Glode, M.P.; Mason, W.H.; Reddy, V.; Sanders, S.P.; et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N. Engl. J. Med. 1986, 315, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.B.; Park, S.; Eun, L.Y.; Han, J.W.; Lee, S.Y.; Yoon, K.L.; Yu, J.J.; Choi, J.W.; Lee, K.Y. Epidemiology and clinical features of Kawasaki disease in South Korea, 2012–2014. Pediatr. Infect. Dis. J. 2017, 36, 482–485. [Google Scholar] [CrossRef]
- Egami, K.; Muta, H.; Ishii, M.; Suda, K.; Sugahara, Y.; Iemura, M.; Matsuishi, T. Prediction of resistance to intravenous immunoglobulin treatment in patients with Kawasaki disease. J. Pediatr. 2006, 149, 237–240. [Google Scholar] [CrossRef]
- Kobayashi, T.; Inoue, Y.; Takeuchi, K.; Okada, Y.; Tamura, K.; Tomomasa, T.; Kobayashi, T.; Morikawa, A. Prediction of intravenous immunoglobulin unresponsiveness in patients with Kawasaki disease. Circulation 2006, 113, 2606–2612. [Google Scholar] [CrossRef]
- Liu, G.; Wang, S.; Du, Z. Risk factors of intravenous immunoglobulin resistance in children with Kawasaki disease: A meta-analysis of case-control studies. Front. Pediatr. 2020, 8, 187. [Google Scholar] [CrossRef] [Green Version]
- Henter, J.I.; Horne, A.; Aricó, M.; Egeler, R.M.; Filipovich, A.H.; Imashuku, S.; Ladisch, S.; McClain, K.; Webb, D.; Winiarski, J.; et al. HLH-2004: Diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr. Blood Cancer 2007, 48, 124–131. [Google Scholar] [CrossRef]
- Ravelli, A.; Davi, S.; Minoia, F.; Martini, A.; Cron, R.Q. Macrophage activation syndrome. Hematol. Oncol. Clin. N. Am. 2015, 29, 927–941. [Google Scholar] [CrossRef]
- Bagri, N.K.; Gupta, L.; Sen, E.S.; Ramanan, A.V. Macrophage activation syndrome in children: Diagnosis and management. Indian Pediatr. 2021, 58, 1155–1161. [Google Scholar] [CrossRef]
- Cron, R.Q.; Davi, S.; Minoia, F.; Ravelli, A. Clinical features and correct diagnosis of macrophage activation syndrome. Expert Rev. Clin. Immunol. 2015, 11, 1043–1053. [Google Scholar] [CrossRef] [PubMed]
- Natoli, V.; Rosina, S.; Ravelli, A. Is macrophage activation syndrome in Kawasaki disease underrecognized? J. Rheumatol. 2021, 48, 162–164. [Google Scholar] [CrossRef] [PubMed]
- Han, S.B.; Lee, S.Y. Macrophage activation syndrome in children with Kawasaki disease: Diagnostic and therapeutic approaches. World J. Pediatr. 2020, 16, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.E.; Kwak, Y.; Huh, J.W.; Yoo, E.S.; Ryu, K.H.; Sohn, S.; Hong, Y.M. Differentiation between incomplete Kawasaki disease and secondary hemophagocytic lymphohistiocytosis following Kawasaki disease using N-terminal pro-brain natriuretic peptide. Korean J. Pediatr. 2018, 61, 167–173. [Google Scholar] [CrossRef]
- Han, S.B.; Lee, S.Y. Systemic-onset juvenile idiopathic arthritis and incomplete Kawasaki disease may belong to a single clinical syndrome within a spectrum of severity. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 122), 3. [Google Scholar]
- Latino, G.A.; Manlhiot, C.; Yeung, R.S.; Chahal, N.; McCrindle, B.W. Macrophage activation syndrome in the acute phase of Kawasaki disease. J. Pediatr. Hematol. Oncol. 2010, 32, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Gong, F.; Zhu, W.; Fu, S.; Zhang, Q. Macrophage activation syndrome in Kawasaki disease: More common than we thought? Semin. Arthritis Rheum. 2015, 44, 405–410. [Google Scholar] [CrossRef]
- Mousavi, M.S.; Assari, R.; Tahghighi, F.; Eshaghi, H.; Ziaee, V. Prolonged fever and intravenous immunoglobulin resistance in Kawasaki disease: Should macrophage activation syndrome be considered? Iran. J. Pediatr. 2019, 29, e69170. [Google Scholar] [CrossRef] [Green Version]
- Pilania, R.K.; Jindal, A.K.; Johnson, N.; Prithvi, A.; Vignesh, P.; Suri, D.; Rawat, A.; Gupta, A.; Singh, S. Macrophage activation syndrome in children with Kawasaki disease: An experience from a tertiary care hospital in northwest India. Rheumatology 2021, 60, 3413–3419. [Google Scholar] [CrossRef]
- Roh, D.E.; Kwon, J.E.; Choi, H.J.; Kim, Y.H. Importance of serum ferritin level for early diagnosis and differentiation in patients with Kawasaki disease with macrophage activation syndrome. Children 2021, 8, 269. [Google Scholar]
- Qiu, Z.; Liu, H.H.; Fan, G.Z.; Chen, W.X.; Hu, P. The clinical implications of serum ferritin in Kawasaki disease: A helpful biomarker for evaluating therapeutic responsiveness, coronary artery involvement and the tendency of macrophage activation syndrome. Arch. Med. Sci. 2022, 18, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Ohga, S.; Ooshima, A.; Fukushige, J.; Ueda, K. Histiocytic haemophagocytosis in a patient with Kawasaki disease: Changes in the hypercytokinaemic state. Eur. J. Pediatr. 1995, 154, 539–541. [Google Scholar] [CrossRef] [PubMed]
- García-Pavón, S.; Yamazaki-Nakashimada, M.A.; Báez, M.; Borjas-Aguilar, K.L.; Murata, C. Kawasaki disease complicated with macrophage activation syndrome: A systematic review. J. Pediatr. Hematol. Oncol. 2017, 39, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Gamez-Gonzalez, L.B.; Moribe-Quintero, I.; Cisneros-Castolo, M.; Varela-Ortiz, J.; Muñoz-Ramírez, M.; Garrido-García, M.; Yamazaki-Nakashimada, M. Kawasaki disease shock syndrome: Unique and severe subtype of Kawasaki disease. Pediatr. Int. 2018, 60, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Vilaiyuk, S.; Sirachainan, N.; Wanitkun, S.; Pirojsakul, K.; Vaewpanich, J. Recurrent macrophage activation syndrome as the primary manifestation in systemic lupus erythematosus and the benefit of serial ferritin measurements: A case-based review. Clin. Rheumatol. 2013, 32, 899–904. [Google Scholar] [CrossRef]
- Behrens, E.M.; Beukelman, T.; Paessler, M.; Cron, R.Q. Occult macrophage activation syndrome in patients with systemic juvenile idiopathic arthritis. J. Rheumatol. 2007, 34, 1133–1138. [Google Scholar]
- Zeng, P.; Li, F.; Zeng, H. Occult macrophage activation syndrome in systemic-onset juvenile idiopathic arthritic syndrome—A case report. Acta Reumatol. Port. 2013, 38, 196–200. [Google Scholar]
- Choi, U.Y.; Han, S.B.; Lee, S.Y. Should refractory Kawasaki disease be considered occult macrophage activation syndrome? Semin. Arthritis Rheum. 2017, 46, e17. [Google Scholar] [CrossRef]
- Kang, D.W.; Kim, S.H. Clinical aspects of splenomegaly as a possible predictive factor of coronary artery changes in Kawasaki disease. Cardiol. Young 2019, 29, 297–302. [Google Scholar] [CrossRef]
- Shao, S.; Zhou, K.; Liu, X.; Liu, L.; Wu, M.; Deng, Y.; Duan, H.; Li, Y.; Hua, Y.; Wang, C. Predictive value of serum lipid for intravenous immunoglobulin resistance and coronary artery lesion in Kawasaki d isease. J. Clin. Endocrinol. Metab. 2021, 106, e4210–e4220. [Google Scholar] [CrossRef]
- Ravelli, A.; Minoia, F.; Davì, S.; Horne, A.; Bovis, F.; Pistorio, A.; Arico, M.; Avcin, T.; Behrens, E.; Benedetti, F.; et al. 2016 Classification criteria for macrophage activation syndrome complicating systemic juvenile idiopathic arthritis: A European league against rheumatism/American College of Rheumatology/Paediatric Rheumatology International Trials Organisation Collaborative Initiative. Ann. Rheum. Dis. 2016, 75, 481–489. [Google Scholar] [PubMed]
- Han, S.B.; Lee, S.Y.; Jeong, D.C.; Kang, J.H. Should 2016 criteria for macrophage activation syndrome be applied in children with Kawasaki disease, as well as with systemic-onset juvenile idiopathic arthritis? Ann. Rheum. Dis. 2016, 75, e44. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Refractory KD (n = 59) | MAS (n = 4) | p-Value | |
|---|---|---|---|
| Clinical | |||
| Age (years) | 2.6 (0.3–11.1) | 4.4 (1.6–13.1) | 0.481 |
| Sex (male) | 38 (64.4) | 3 (75.0) | 1.000 |
| Duration of fever (days) | 4.0 (2.0–10.0) | 5.0 (4.0–7.0) | 0.087 |
| Length of hospital stay (days) | 9.0 (3.0–24.0) | 12.0 (10.0–41.0) | 0.064 |
| Principal features (e.g., conjunctivitis) a | 57 (96.6) | 3 (75.0) | 0.181 |
| Incomplete KD | 8 (13.6) | 3 (75.0) | 0.015 |
| Hepatosplenomegaly | 2 (3.4) | 4 (100.0) | <0.001 |
| Third-line treatment b | 5 (8.5) | 4 (100.0) | <0.001 |
| Coronary artery complications | 10 (16.9) | 0 (0.0) | 1.000 |
| Laboratory | |||
| Hemoglobin (g/dL) | 11.4 (8.8–13.7) | 10.0 (5.7–11.6) | 0.108 |
| WBC count (×109/L) | 16.3 (2.7–49.3) | 8.0 (2.1–32.8) | 0.210 |
| Platelet count (×109/L) | 310.0 (26.0–545.0) | 68.5 (59.0–414.0) | 0.071 |
| ESR (mm/h) | 58.0 (3.0–120.0) | 39.0 (12.0–62.0) | 0.143 |
| CRP (mg/dL) | 9.9 (0.8–25.9) | 18.5 (7.8–21.5) | 0.055 |
| Sodium (mmol/L) | 136.0 (127.0–141.0) | 135.0 (134.0–135.0) | 0.243 |
| Albumin (g/dL) | 3.6 (2.1–4.8) | 2.7 (2.5–2.9) | 0.004 |
| AST (U/L) | 76.0 (18.0–754.0) | 234.0 (75.0–964.0) | 0.065 |
| ALT (U/L) | 85.0 (9.0–498.0) | 233.0 (26.0–1099.0) | 0.190 |
| MAS screening c | 9 (15.3) | 4 (100.0) | 0.001 |
| MAS (n = 4) | Refractory KD (n = 5) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 a | 3 | 4 | 1 | 2 | 3 | 4 | 5 | |
| Sex/age (years) | M/1.8 | F/1.6 | M/7.0 | M/13.1 | F/2.3 | F/0.5 | M/6.1 | M/2.5 | M/3.0 |
| Fever despite 2nd IVIG or IVMP | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Hepatosplenomegaly | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No |
| Cytopenia (≥2 cell lines) | No | Bicyto- | Pancyto- | Bicyto- | No | Anemia | Thrombo- | Anemia | Thrombo- |
| AST/ALT (U/L) b | 190/236 | 964/1099 | 278/230 | 75/26 | 189/374 | 146/86 | 299/181 | 137/338 | 48/19 |
| Abnormal TG or fibrinogen | Yes | Yes | Yes | Yes | – | – | – | – | No |
| Ferritin (>500 ng/mL) | 5130 | 57100 | 1420 | 790 | – | – | – | – | 570 |
| Hemophagocytosis | Yes | Yes | No | – | – | – | – | – | – |
| Management and outcomes | |||||||||
| Admission to ICU | Yes | No | No | Yes | No | No | Yes | Yes | No |
| Third-line treatment | IVMP | CS + DX | HLH-2004 | IVIG + DX | IVMP | IVMP | IVIG + IVMP | IVMP | Infliximab |
| Coronary artery complications | No | No | No | No | No | Yes | No | No | No |
| Other complications | Shock | Arthritis | No | DIC, seizure | GB hydrops | Meningitis | ARDS, shock | AKI, seizure | No |
| Successful recovery | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Subjects | MAS in KD | IVIG Resistance in MAS | MAS in Refractory KD | |
|---|---|---|---|---|
| Latino et al. [16], Canada | n = 638 | 12/638 (1.9%) | 12/12 (100.0%) | 12/96 (12.5%) b |
| Wang et al. [17], China | n = 719 | 8/719 (1.1%) | 7/8 (87.5%) | 7/108 (6.5%) b |
| Mousavi et al. [18], Iran | n = 218 | 4/218 (1.8%) | 4/4 (100.0%) | 4/33 (12.1%) b |
| Pilania et al. [19], India | n = 950 | 12/950 (1.3%) | 12/12 (100.0%) | 12/143 (8.4%) b |
| Roh et al. [20], Korea | n = 158 | 5/158 (3.2%) a | 5/5 (100.0%) | 5/71 (7.0%) |
| Qiu et al. [21], China | n = 244 | 1/244 (0.4%) | 1/1 (100.0%) | 1/15 (6.7%) |
| This study, Korea | n = 468 | 4/468 (0.8%) | 4/4 (100.0%) | 4/63 (6.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rhee, S.; Kim, D.; Cho, K.; Rhim, J.W.; Lee, S.-Y.; Jeong, D.C. Under-Recognized Macrophage Activation Syndrome in Refractory Kawasaki Disease: A Wolf in Sheep’s Clothing. Children 2022, 9, 1588. https://doi.org/10.3390/children9101588
Rhee S, Kim D, Cho K, Rhim JW, Lee S-Y, Jeong DC. Under-Recognized Macrophage Activation Syndrome in Refractory Kawasaki Disease: A Wolf in Sheep’s Clothing. Children. 2022; 9(10):1588. https://doi.org/10.3390/children9101588
Chicago/Turabian StyleRhee, Sangwon, Danbi Kim, Kyoungsoon Cho, Jung Woo Rhim, Soo-Young Lee, and Dae Chul Jeong. 2022. "Under-Recognized Macrophage Activation Syndrome in Refractory Kawasaki Disease: A Wolf in Sheep’s Clothing" Children 9, no. 10: 1588. https://doi.org/10.3390/children9101588