
A Music Therapy Intervention for Refugee Children and Adolescents in Schools: A Process Evaluation Using a Mixed Method Design
 , ,
, ,
Abstract
:
1. Introduction
2. Methods
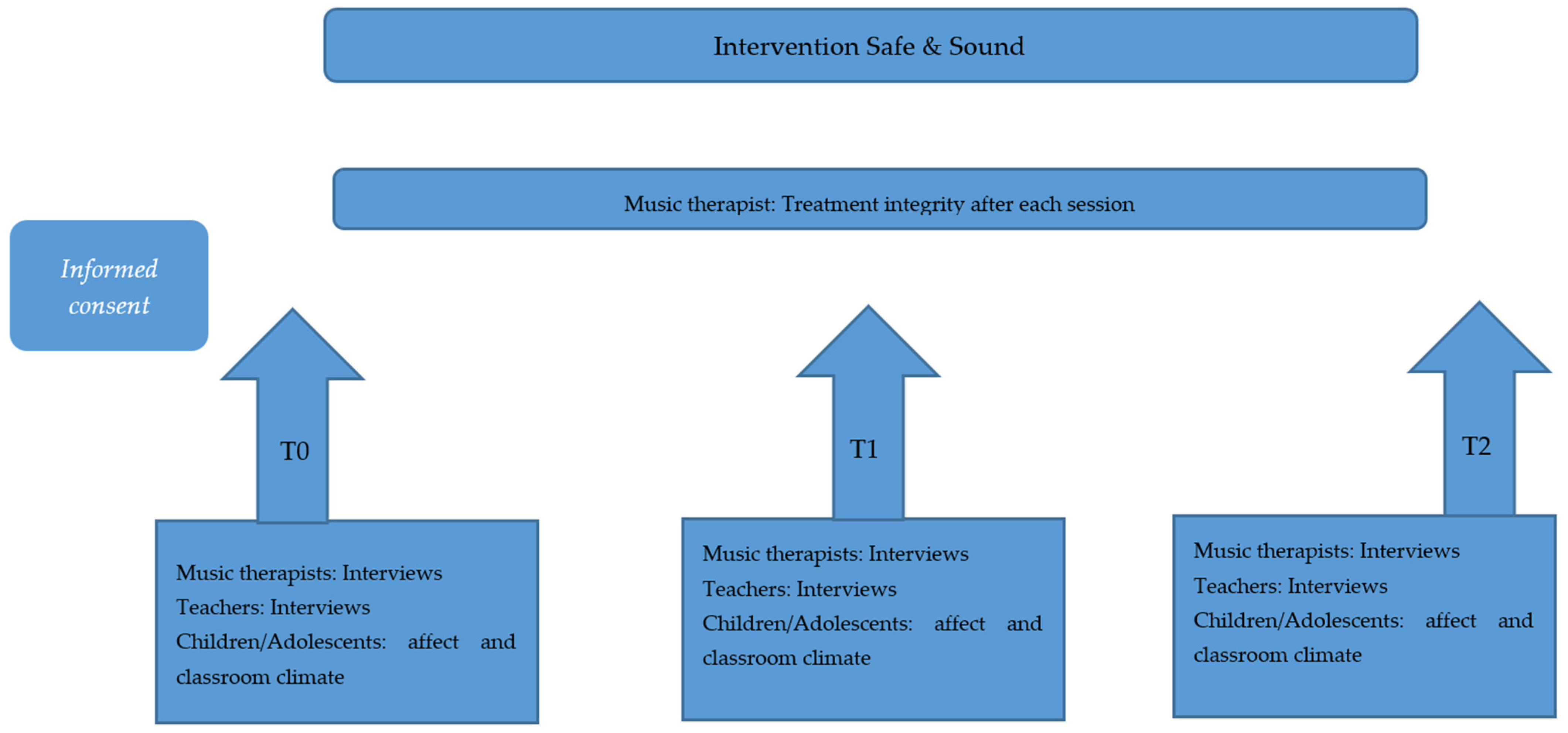
2.1. Design
2.2. Participants
2.3. Music Therapy Intervention “Safe & Sound”
2.4. Procedure
2.5. Data Collection Methods
2.5.1. Interviews
2.5.2. Measurement Instruments
- Visual analogue scale to measure positive and negative affect
- Special Education Classroom Climate Inventory
2.6. Treatment Integrity
2.7. Data Analyses
2.7.1. Qualitative Data Analysis
2.7.2. Quantitative Data Analysis
2.8. Trustworthiness
3. Results
3.1. Participants
3.2. Qualitative Results
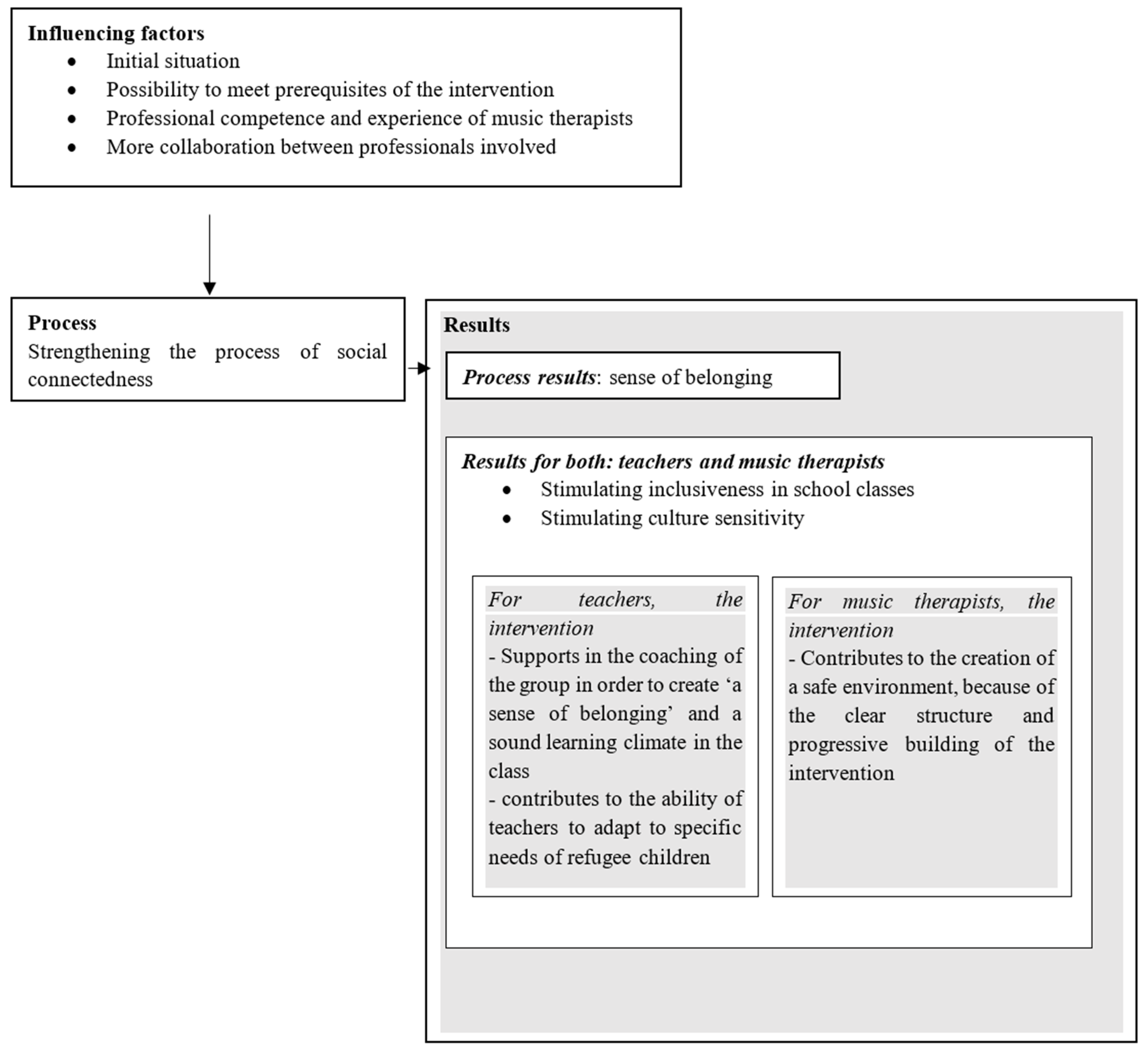
3.2.1. Strengthening the Process of Social Connectedness
3.2.2. Process Result: Sense of Belonging
3.2.3. Influencing Factors
- Initial situation
- Possibility to meet prerequisites of the intervention
- Professional competence and experience of musical therapist
- The collaboration between professionals involved
3.3. Quantative Results
3.3.1. Negative Affect
3.3.2. Classroom Climate
3.4. Treatment Integrity
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Visual Analogue Scale


Appendix B. Classroom Climate Questionnaire

References
- UNHCR. Global Trends. Forced Displacement in 2017; UNHCR: Geneva, Switzerland, 2018. [Google Scholar]
- Idemudia, E.S.; Williams, J.K.; Wyatt, G.E. Migration challenges among Zimbabwean refugees before, during and post arrival in South Africa. J. Inj. Violence Res. 2013, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- Solberg, Ø.; Nissen, A.; Vaez, M.; Cauley, P.; Eriksson, A.K.; Saboonchi, F. Children at risk: A nation-wide, cross-sectional study examining post-traumatic stress symptoms in refugee minors from Syria, Iraq and Afghanistan resettled in Sweden between 2014 and 2018. Confl. Health 2020, 14, 67. [Google Scholar] [CrossRef] [PubMed]
- Blackmore, R.; Boyle, J.A.; Fazel, M.; Ranasinha, S.; Gray, K.M.; Fitzgerald, G.; Misso, M.; Gibson-Helm, M. The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003337. [Google Scholar] [CrossRef] [PubMed]
- Crepet, A.; Rita, F.; Reid, A.; Van den Boogaard, W.; Deiana, P.; Quaranta, G.; Barbieri, A.; Bongiorno, F.; Di Carlo, S. Mental health and trauma in asylum seekers landing in Sicily in 2015: A descriptive study of neglected invisible wounds. Confl. Health 2017, 11, 1. [Google Scholar] [CrossRef]
- Priebe, S.; Giacco, D.; El-Nagib, R. Public Health Aspects of Mental Health among Migrants and Refugees: A Review of the Evidence on Mental Health Care for Refugees, Asylum Seekers and Irregular Migrants in the WHO European Region; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Sleijpen, M.; van der Aa, N.; Mooren, T.; Laban, C.J.; Kleber, R.J. The moderating role of individual resilience in refugee and Dutch adolescents after trauma. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 732. [Google Scholar] [CrossRef]
- UNICEF. Danger Every Step of the Way. A Harrowing Journey to EUROPE for Refugee and Migrant Children; UNICEF: Geneva, Switzerland, 2016; Available online: http://www.pharos.nl/documents/doc/psychische_problematiek_bij_vluchtelingkinderen_en-jongeren-handreiking.pdf (accessed on 1 September 2022).
- Bogic, M.; Njoku, A.; Priebe, S. Long-term mental health of war-refugees: A systematic literature review. BMC Int. Health Hum. Rights 2015, 15, 29. [Google Scholar] [CrossRef]
- Center for Substance Abuse Treatment. Understanding the impact of trauma. In Trauma-Informed Care in Behavioral Health Services; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014. [Google Scholar]
- Thomason, M.E.; Marusak, H.A. Toward understanding the impact of trauma on the early developing human brain. Neuroscience 2017, 342, 55–67. [Google Scholar] [CrossRef]
- De Vries, R.J.; van den Berg, W. Onderwijs aan vluchtelingenkinderen: Waar knelt het en wat gaat al goed? Verus: Amsterdam, The Netherlands, 2015; Available online: https://www.verus.nl/sites/www.verus.nl/files/documenten/rapportage_ledenpeiling_onderwijs_aan_vluchtelingenkinderen_2.pdf (accessed on 1 September 2022).
- Beld, M.H.M.; Van den Heuvel, E.G.; Van der Helm, G.H.P.; Kuiper, C.H.Z.; de Swart, J.J.W.; Roest, J.J.; Stams, G.J.J.M. The impact of classroom climate on students’ perception of social exclusion in secondary special education. Child. Youth Serv. Rev. 2019, 103, 127–134. [Google Scholar] [CrossRef]
- Haker, F.; van den Muijsenbergh, M.; Torensma, M.; van Berkum, M.; Smulders, E.; Looman, B.; van Wieringen, J.; Bloemen, E.; van Bokhoven, R. Kennissynthese Gezondheid van Nieuwkomende Vluchtelingen en Indicaties Voor Zorg, Preventie en Ondersteuning; Pharos: Utrecht, The Netherlands, 2016; Available online: https://www.pharos.nl/kennisbank/kennissynthese-gezondheid-van-nieuwkomende-vluchtelingen-en-indicaties-voor-zorg-preventie-en-ondersteuning/ (accessed on 1 September 2022).
- Peterson, C.; Poudel-Tandukar, K.; Sanger, K.; Jacelon, C.S. Improving mental health in refugee populations: A review of intervention studies conducted in the United States. Issues Ment. Health Nurs. 2020, 41, 271–282. [Google Scholar] [CrossRef]
- Reynolds, A.D.; Bacon, R. Interventions supporting the social integration of refugee children and youth in school communities: A review of the literature. Adv. Soc. Work 2018, 18, 745–766. [Google Scholar] [CrossRef]
- Nocon, A.; Eberle-Sejari, R.; Unterhitzenberger, J.; Rosner, R. The effectiveness of psychosocial interventions in war-traumatized refugee and internally displaced minors: Systematic review and meta-analysis. Eur. J. Psychotraumatology 2017, 8 (Suppl. 2), 1388709. [Google Scholar] [CrossRef] [PubMed]
- Van Goor & Toussaint Muziektherapie Voor Asielzoekerskinderen. Muziek als Traumaverwerking; Dagblad de Limburger: Maastricht, The Netherlands, 2016; Available online: https://libguides.studiecentra.han.nl/trauma/muziektherapie (accessed on 1 September 2022).
- Wiess, C.; Bensimon, M. Group music therapy with uprooted teenagers: The Importance of structure. Nord. J. Music. Ther. 2020, 29, 174–189. [Google Scholar] [CrossRef]
- Koelsch, S. Music-evoked emotions: Principles, brain correlates, and implications for therapy. Ann. N.Y. Acad. Sci. 2015, 1337, 193–201. [Google Scholar] [CrossRef] [PubMed]
- De Witte, M.; Pinho, A.D.S.; Stams, G.-J.; Moonen, X.; Bos, A.E.R.; van Hooren, S. Music Therapy for Stress Reduction: A Systematic Review and Meta-Analysis. Health Psychol. Rev. 2022, 16, 134–159. [Google Scholar] [CrossRef]
- Baker, F.; Jones, C. The effect of music therapy services on classroom behaviours of newly arrived refugee students in Australia—A pilot study. Emot. Behav. Difficulties 2006, 11, 249–260. [Google Scholar] [CrossRef]
- Jones, C.; Baker, F.; Day, T. From Healing Rituals to Music Therapy: Bridging the Cultur23al Divide Between Therapist and Young Sudanese Refugees. Arts Psychother. 2004, 31, 89–100. [Google Scholar] [CrossRef]
- Enge, K.E.A.; Stige, B. Musical pathways to the peer community: A collective case study of refugee children’s use of music therapy. Nord. J. Music. Ther. 2022, 31, 7–24. [Google Scholar] [CrossRef]
- De Haan, A.; Bloemen, E.; Beekman, J. Preventieve Interventies Voor Het Versterken Van de Psychische Gezondheid en Veerkracht van Statushouders. Pharos, Utrecht. 2018. Available online: https://www.pharos.nl/infosheets/asielzoekers-vluchtelingen-statushouders-kinderen-en-jongeren/ (accessed on 1 September 2022).
- Creswell, J.W.; Plano Clark, V.L.; Gutmann, M.L.; Hanson, W.E. Advanced mixed methods research designs. Handb. Mix. Methods Soc. Behav. Res. 2003, 209, 209–240. [Google Scholar]
- Movisie. Op Weg Naar Effectieve Sociale Interventies. Procesevaluatie Bij de Beoordeling van Interventies. 2020. Available online: https://www.movisie.nl/sites/movisie.nl/files/2020-04/informatieblad-procesevaluatie.pdf (accessed on 1 September 2022).
- Moonen, X. Easy language in the Netherlands. In Handbook of Easy Languages in Europe; Lindholm, C., Vanhatalo, U., Eds.; Frank & Timme: Berlin, Germany, 2021. [Google Scholar]
- Berghmans, J.M.; Poley, M.J.; van der Ende, J.; Weber, F.; Van de Velde, M.; Adriaenssens, P.; Himpe, D.; Verhulst, F.C.; Utens, E. A visual analog scale to assess anxiety in children during anesthesia induction (VAS-I): Results supporting its validity in a sample of day care surgery patients. Pediatric Anesth. 2017, 27, 955–961. [Google Scholar] [CrossRef]
- Rossi, V.; Pourtois, G. Transient state-dependent fluctuations in anxiety measured using STAI, POMS, PANAS or VAS: A comparative review. Anxiety Stress Coping 2012, 25, 603–645. [Google Scholar] [CrossRef]
- Rosseel, Y. lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Gold, C.; Solli, H.P.; Krüger, V.; Lie, S.A. Dose-response relationship in music therapy for people with serious mental disorders: Systematic review and meta-analysis. Clin. Psychol. Rev. 2009, 29, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Beld, M.H.M.; Van der Voort, D.; Van der Helm, G.H.P.; Kuiper, C.; De Swart, J.; Stams, G.J. Assessing classroom climate in special education: A validationStudy of the Special Education Classroom Climate Inventory. J. Psychoeduc. Assess. 2018, 36, 736–749. [Google Scholar] [CrossRef]
- Aalbers, S.; Vink, A.; de Witte, M.; Pattiselanno, K.; Spreen, M.; van Hooren, S. Feasibility of Emotion-regulating Improvisational Music Therapy for young adult students with depressive symptoms: A process evaluation. Nord. J. Music. Ther. 2022, 31, 133–152. [Google Scholar] [CrossRef]
- Cho, J.Y.; Lee, E. Reducing confusion about grounded theory and qualitative content analysis: Similarities and differences. Qual. Rep. 2014, 19, 1–20. [Google Scholar] [CrossRef]
- Strauss, A.; Corbin, J. Basics of Qualitative Research; Sage publications: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 1 September 2022).
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D.; R Core Team. Nlme: Linear and Nonlinear Mixed Effects Models R package version 3.1-153; R Package Version 3.1-153; The R Foundation: Vienna, Austria, 2021; Available online: https://CRAN.R-project.org/package=nlme (accessed on 1 September 2022).
- Guba, E.G.; Lincoln, Y.S. Naturalistic Inquiry; Sage: Newbury Park, CA, USA, 1985. [Google Scholar]
- Hurtado, S.; Carter, D.F. Effects of college transition and perceptions of the campus racial climate on Latino college students’ sense of belonging. Sociol. Educ. 1997, 70, 324–345. [Google Scholar] [CrossRef]
- Marley, C.; Mauki, B. Resilience and protective factors among refugee children post-migration to high-income countries: A systematic review. Eur. J. Public Health 2019, 29, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Jones, J.M. Discrimination, diversity, and sense of belonging: Experiences of students of color. J. Divers. High. Educ. 2021, 14, 63. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Nursing Research. In Principles and Methods, 7th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| χ2(df) | CFI | RMSEA | SRMR | ω Positive Affect | ω Negative Affect | ||
|---|---|---|---|---|---|---|---|
| Model 1 (all items) | T0 | 54.39(19) *** | 0.737 | 0.131 | 0.089 | 0.442 | 0.592 |
| T1 | 49.10(19) *** | 0.816 | 0.121 | 0.085 | 0.453 | 0.599 | |
| T2 | 68.64(19) *** | 0.715 | 0.156 | 0.100 | 0.438 | 0.605 | |
| Model 2 (without “easily angered”) | T0 | 45.76(13) *** | 0.754 | 0.153 | 0.088 | 0.450 | 0.663 |
| T1 | 39.84(13) *** | 0.832 | 0.138 | 0.083 | 0.444 | 0.683 | |
| T2 | 60.09(13) *** | 0.713 | 0.183 | 0.105 | 0.450 | 0.629 |
| T0 | T1 | T2 | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Negative Affect | 2.08 | 1.98 | 2.18 | 1.86 | 1.47 | 1.50 |
| Support | 9.32 | 1.09 | 8.82 | 1.71 | 8.99 | 1.46 |
| Growth | 9.15 | 1.25 | 9.13 | 1.15 | 9.12 | 1.20 |
| Atmosphere | 8.32 | 2.13 | 8.24 | 2.21 | 8.29 | 2.05 |
| Environment | 8.44 | 2.02 | 8.51 | 1.56 | 8.36 | 2.12 |
| Repression | 8.83 | 2.05 | 8.12 | 2.38 | 8.37 | 2.13 |
| Safety | 8.76 | 1.95 | 8.81 | 1.70 | 9.06 | 1.63 |
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | ||
| Negative Affect | Intercept | 1.911 | 0.133 | <0.001 | 2.522 | 0.233 | <0.001 | 2.522 | 0.253 | <0.001 | 2.599 | 0.256 | <0.001 |
| Time | −0.305 | 0.096 | 0.002 | −0.305 | 0.097 | 0.002 | −0.305 | 0.096 | 0.002 | ||||
| School-type | −0.2 | 0.272 | 0.464 | ||||||||||
| Deviance | −632.144 | −627.167 | −625.65 | −626.895 | |||||||||
| AIC | 1270.288 | 1262.334 | 1263.301 | 1263.789 | |||||||||
| p Δdeviance | 0.026 1 | 0.218 2 | 0.602 3 | ||||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | ||
| Support | Intercept | 9.045 | 0.106 | <0.001 | 9.383 | 0.189 | <0.001 | 9.383 | 0.167 | <0.001 | 9.475 | 0.187 | <0.001 |
| Time | −0.169 | 0.078 | 0.032 | −0.169 | 0.08 | 0.037 | −0.169 | 0.08 | 0.037 | ||||
| School-type | −0.238 | 0.209 | 0.258 | ||||||||||
| Deviance | −561.326 | −558.998 | −554.318 | −553.711 | |||||||||
| AIC | 1128.653 | 1125.996 | 1120.635 | 1121.422 | |||||||||
| p Δdeviance | 0.127 1 | 0.031 2 | 0.436 4 | ||||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | ||
| Growth | Intercept | 9.133 | 0.085 | <0.001 | 9.16 | 0.159 | <0.001 | 9.16 | 0.163 | <0.001 | 9.263 | 0.177 | <0.001 |
| Time | −0.014 | 0.067 | 0.837 | −0.014 | 0.07 | 0.842 | −0.014 | 0.07 | 0.842 | ||||
| School-type | −0.263 | 0.173 | 0.131 | ||||||||||
| Deviance | −502.511 | −502.489 | −502.232 | −501.081 | |||||||||
| AIC | 1011.021 | 1012.978 | 1016.464 | 1016.162 | |||||||||
| p Δdeviance | 0.884 1 | 0.612 2 | 0.235 3 | ||||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | ||
| Atmosphere | Intercept | 8.284 | 0.155 | <0.001 | 8.312 | 0.279 | <0.001 | 8.312 | 0.279 | <0.001 | 8.705 | 0.299 | <0.001 |
| Time | −0.014 | 0.116 | 0.905 | −0.014 | 0.116 | 0.905 | −0.014 | 0.116 | 0.905 | ||||
| School-type | −1.01 | 0.303 | 0.001 | ||||||||||
| Deviance | −684.236 | −684.229 | −684.228 | −678.881 | |||||||||
| AIC | 1374.472 | 1376.457 | 1380.455 | 1367.762 | |||||||||
| p Δdeviance | 0.932 1 | 0.973 2 | 0.021 3 | ||||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | ||
| Environment | Intercept | 8.438 | 0.135 | <0.001 | 8.522 | 0.254 | <0.001 | 8.522 | 0.25 | <0.001 | 8.693 | 0.273 | <0.001 |
| Time | −0.042 | 0.108 | 0.699 | −0.042 | 0.114 | 0.715 | −0.042 | 0.114 | 0.716 | ||||
| School-type | −0.44 | 0.273 | 0.111 | ||||||||||
| Deviance | −654.281 | −654.206 | −652.434 | −651.154 | |||||||||
| AIC | 1314.563 | 1316.412 | 1316.868 | 1316.307 | |||||||||
| p Δdeviance | 0.784 1 | 0.183 2 | 0.081 3 | ||||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | ||
| Repression | Intercept | 8.441 | 0.146 | <0.001 | 8.904 | 0.303 | <0.001 | 8.904 | 0.289 | <0.001 | 8.897 | 0.325 | <0.001 |
| Time | −0.231 | 0.133 | 0.082 | −0.231 | 0.134 | 0.085 | −0.231 | 0.133 | 0.083 | ||||
| School-type | 0.018 | 0.3 | 0.952 | ||||||||||
| Deviance | −708.66 | −707.136 | −706.333 | −707.134 | |||||||||
| AIC | 1423.319 | 1422.271 | 1424.666 | 1424.268 | |||||||||
| p Δdeviance | 0.217 1 | 0.370 2 | 0.966 3 | ||||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | ||
| Safety | Intercept | 8.877 | 0.118 | <0.001 | 8.58 | 0.243 | <0.001 | 8.58 | 0.255 | <0.001 | 8.588 | 0.273 | <0.001 |
| Time | 0.148 | 0.106 | 0.164 | 0.148 | 0.110 | 0.181 | 0.148 | 0.11 | 0.181 | ||||
| School-type | −0.019 | 0.242 | 0.937 | ||||||||||
| Deviance | −636.887 | −635.909 | −635.407 | −635.404 | |||||||||
| AIC | 1279.775 | 1279.818 | 1282.814 | 1284.807 | |||||||||
| p Δdeviance | 0.323 1 | 0.479 2 | 0.477 3 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heynen, E.; Bruls, V.; van Goor, S.; Pat-El, R.; Schoot, T.; van Hooren, S. A Music Therapy Intervention for Refugee Children and Adolescents in Schools: A Process Evaluation Using a Mixed Method Design. Children 2022, 9, 1434. https://doi.org/10.3390/children9101434
Heynen E, Bruls V, van Goor S, Pat-El R, Schoot T, van Hooren S. A Music Therapy Intervention for Refugee Children and Adolescents in Schools: A Process Evaluation Using a Mixed Method Design. Children. 2022; 9(10):1434. https://doi.org/10.3390/children9101434
Chicago/Turabian StyleHeynen, Evelyn, Vivian Bruls, Sander van Goor, Ron Pat-El, Tineke Schoot, and Susan van Hooren. 2022. "A Music Therapy Intervention for Refugee Children and Adolescents in Schools: A Process Evaluation Using a Mixed Method Design" Children 9, no. 10: 1434. https://doi.org/10.3390/children9101434