
Developing Virtual Reality Head Mounted Display (HMD) Set-Up for Thoracoscopic Surgery of Complex Congenital Lung MalFormations in Children

 , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Three-Dimensional (3D) Models
2.3. Virtual Reality HMD Model
2.4. Preoperative Virtual Reality HMD Setup Evaluation
2.5. Surgical Technique
3. Results
3.1. Patient’s Data
3.2. Preoperative Planning
3.3. Surgical Procedure
3.4. Postoperative Navigation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stocker, J.T. Congenital pulmonary airway malformation: A new name and expanded classification of congenital cystic adenomatoid malformation of the lung. Histopathology 2002, 41, 424–431. [Google Scholar]
- Chitty, L.; Harcourt, J.; Hewitt, R.J.; Nicholson, A.G. Congenital Lung Disease. Kendigs Disord. Respir. Tract Child. 2019, 289–337.e8. [Google Scholar] [CrossRef]
- Andrade, C.F.; da Ferreira, H.P.C.; Fischer, G.B. Congenital lung malformations. J. Bras. Pneumol. 2011, 37, 259–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cass, D.L.; Quinn, T.M.; Yang, E.Y.; Liechty, K.W.; Crombleholme, T.M.; Flake, A.W.; Adzick, N.S. Increased cell proliferation and decreased apoptosis characterize congenital cystic adenomatoid malformation of the lung. J. Pediatr. Surg. 1998, 33, 1043–1046, discussion 1047. [Google Scholar] [CrossRef]
- Correia-Pinto, J.; Gonzaga, S.; Huang, Y.; Rottier, R. Congenital lung lesions-underlying molecular mechanisms. Semin. Pediatr. Surg. 2010, 19, 171–179. [Google Scholar] [CrossRef]
- Ho, U.Y.; Wainwright, B.J. Patched1 patterns Fibroblast growth factor 10 and Forkhead box F1 expression during pulmonary branch formation. Mech. Dev. 2017, 147, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Bird, A.D.; Flecknoe, S.J.; Tan, K.H.; Olsson, P.F.; Antony, N.; Mantamadiotis, T.; Hooper, S.B.; Cole, T.J. cAMP Response Element Binding Protein Is Required for Differentiation of Respiratory Epithelium during Murine Development. PLoS ONE 2011, 6, e17843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Prima, F.A.F.; Bellia, A.; Inclimona, G.; Grasso, F.; Teresa, M.; Cassaro, M.N. Antenatally diagnosed congenital cystic adenomatoid malformations (CCAM): Research Review. J. Prenat. Med. 2012, 6, 22–30. [Google Scholar] [PubMed]
- Chowdhury, M.M.; Chakraborty, S. Imaging of congenital lung malformations. Semin. Pediatr. Surg. 2015, 24, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Le Moal, J.; Peillon, C.; Dacher, J.-N.; Baste, J.-M. Three-dimensional computed tomography reconstruction for operative planning in robotic segmentectomy: A pilot study. J. Thorac. Dis. 2018, 10, 196–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Q.; Xie, B.; Hu, M.; Sun, X.; Huang, X.; Guo, M. Thoracoscopic anatomic pulmonary segmentectomy: A 3-dimensional guided imaging system for lung operations. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 183–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardari Nia, P.; Olsthoorn, J.R.; Heuts, S.; Maessen, J.G. Interactive 3D Reconstruction of Pulmonary Anatomy for Preoperative Planning, Virtual Simulation, and Intraoperative Guiding in Video-Assisted Thoracoscopic Lung Surgery. Innovations 2019, 14, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Oizumi, H.; Kanauchi, N.; Kato, H.; Endoh, M.; Suzuki, J.; Fukaya, K.; Sadahiro, M. Anatomic thoracoscopic pulmonary segmentectomy under 3-dimensional multidetector computed tomography simulation: A report of 52 consecutive cases. J. Thorac. Cardiovasc. Surg. 2011, 141, 678–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vertemati, M.; Cassin, S.; Rizzetto, F.; Vanzulli, A.; Elli, M.; Sampogna, G.; Gallieni, M. A Virtual Reality Environment to Visualize Three-Dimensional Patient-Specific Models by a Mobile Head-Mounted Display. Surg. Innov. 2019, 26, 359–370. [Google Scholar] [CrossRef]
- Vertemati, M.; Rizzetto, F.; Vezzulli, F.; Vanzulli, A.; Rantas, S.; Aseni, P.; Cassin, S. A mirroring virtual reality environment using mobile head mounted display for visualization of patient-specific anatomy. In Proceedings of the 2019 Inventions and Innovations: Medicine 2040, Tel Aviv-Yafo, Israel, 4–5 November 2019. [Google Scholar] [CrossRef]
- Peden, R.G.; Mercer, R.; Tatham, A.J. The use of head-mounted display eyeglasses for teaching surgical skills: A prospective randomised study. Int. J. Surg. 2016, 34, 169–173. [Google Scholar] [CrossRef]
- Solomon, B.; Bizekis, C.; Dellis, S.L.; Donington, J.S.; Oliker, A.; Balsam, L.B.; Zervos, M.; Galloway, A.C.; Pass, H.; Grossi, E.A. Simulating video-assisted thoracoscopic lobectomy: A virtual reality cognitive task simulation. J. Thorac. Cardiovasc. Surg. 2011, 141, 249–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, K.; Bjerrum, F.; Hansen, H.J.; Petersen, R.H.; Pedersen, J.H.; Konge, L. Using virtual reality simulation to assess competence in video-assisted thoracoscopic surgery (VATS) lobectomy. Surg. Endosc. 2017, 31, 2520–2528. [Google Scholar] [CrossRef]
- Sadeghi, A.H.; Maat, A.P.W.M.; Taverne, Y.J.H.J.; Cornelissen, R.; Dingemans, A.-M.C.; Bogers, A.J.J.C.; Mahtab, E.A.F. Virtual reality and artificial intelligence for 3-dimensional planning of lung segmentectomies. JTCVS Tech. 2021, 7, 309–321. [Google Scholar] [CrossRef]
- Timonen, T.; Iso-Mustajärvi, M.; Linder, P.; Lehtimäki, A.; Löppönen, H.; Elomaa, A.P.; Dietz, A. Virtual reality improves the accuracy of simulated preoperative planning in temporal bones: A feasibility and validation study. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. (EUFOS) Affil. Ger. Soc. Oto-Rhino-Laryngol.-Head Neck Surg. 2021, 278, 2795–2806. [Google Scholar] [CrossRef]
- Ujiie, H.; Yamaguchi, A.; Gregor, A.; Chan, H.; Kato, T.; Hida, Y.; Kaga, K.; Wakasa, S.; Eitel, C.; Clapp, T.R.; et al. Developing a virtual reality simulation system for preoperative planning of thoracoscopic thoracic surgery. J. Thorac. Dis. 2021, 13, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Jensen, K.; Bjerrum, F.; Hansen, H.J.; Petersen, R.H.; Pedersen, J.H.; Konge, L. A new possibility in thoracoscopic virtual reality simulation training: Development and testing of a novel virtual reality simulator for video-assisted thoracoscopic surgery lobectomy. Interact. Cardiovasc. Thorac. Surg. 2015, 21, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Kocyildirim, E.; Kanani, M.; Roebuck, D.; Wallis, C.; McLaren, C.; Noctor, C.; Pigott, N.; Mok, Q.; Hartley, B.; Dunne, C.; et al. Long-segment tracheal stenosis: Slide tracheoplasty and a multidisciplinary approach improve outcomes and reduce costs. J. Thorac. Cardiovasc. Surg. 2004, 128, 876–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadeghi, A.H.; Bakhuis, W.; Van Schaagen, F.; Oei, F.B.; Bekkers, J.A.; Maat, A.; Mahtab, E.A.; Bogers, A.; Taverne, Y. Immersive 3D virtual reality imaging in planning minimally invasive and complex adult cardiac surgery. Eur. Heart J.-Digit. Health 2020, 1, 62–70. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Features | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| Age at surgery | 4 months | 4 years | 3 years |
| Sex | F | F | F |
| Gestational age | term | term | term |
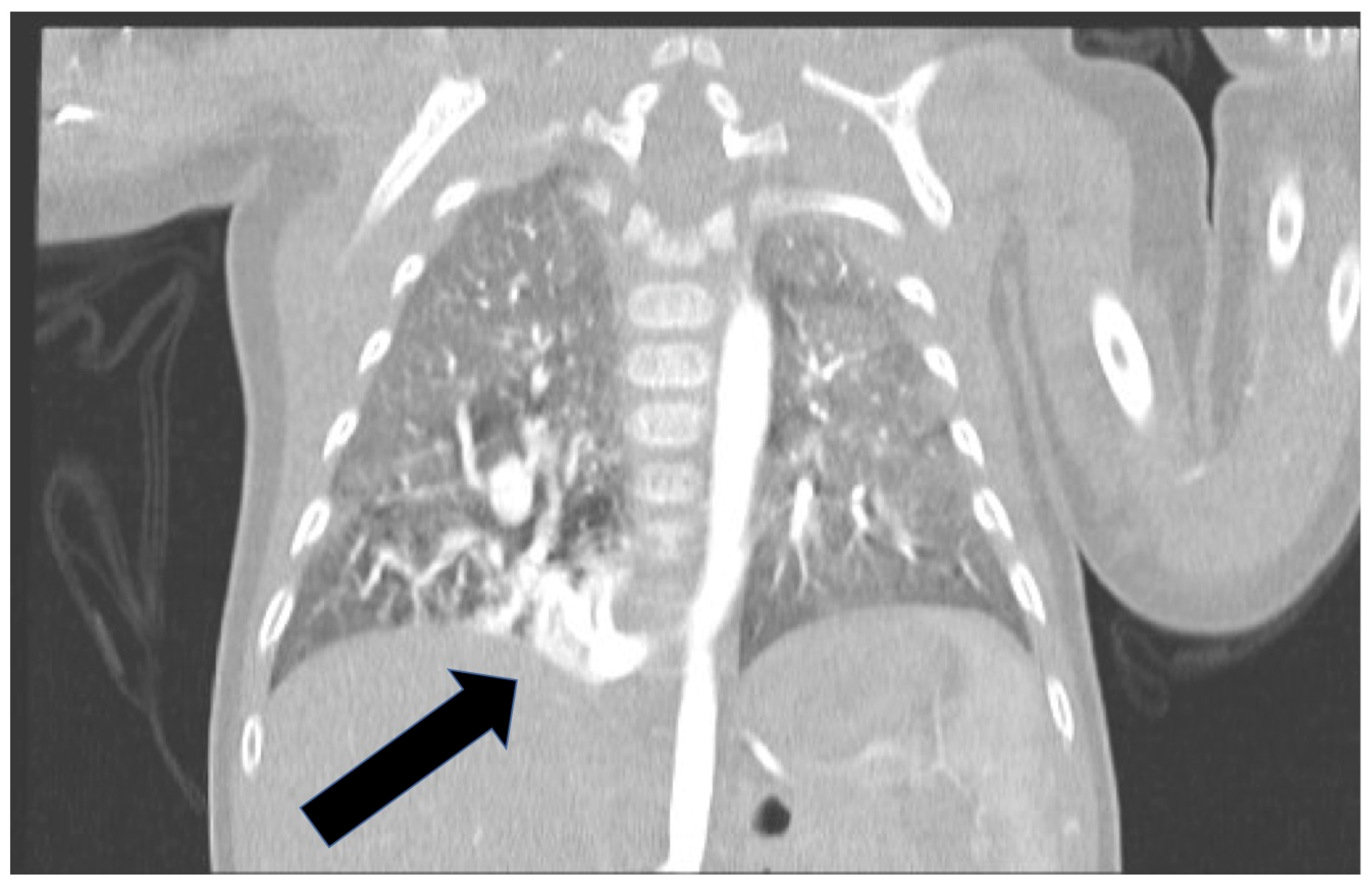
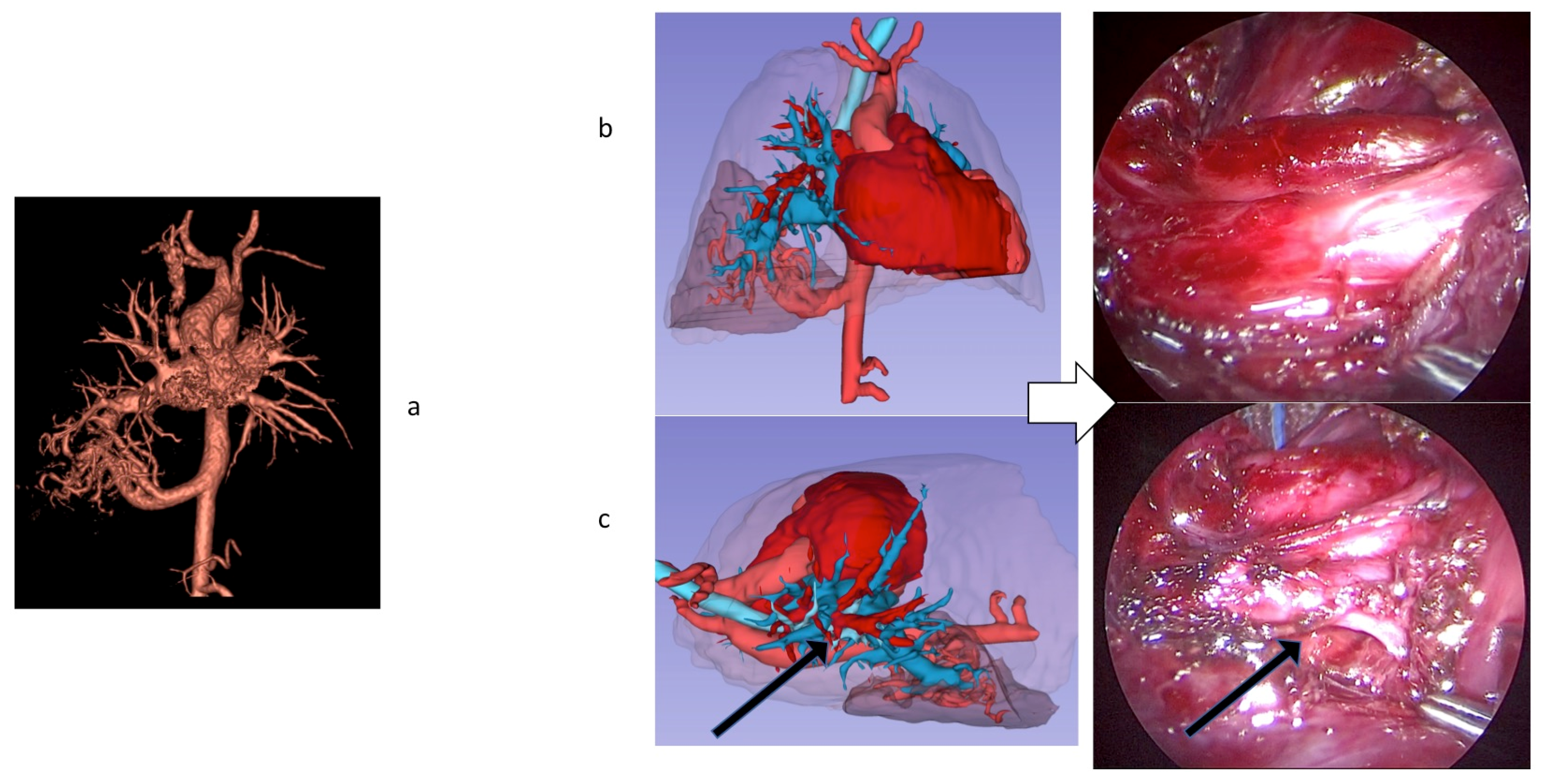
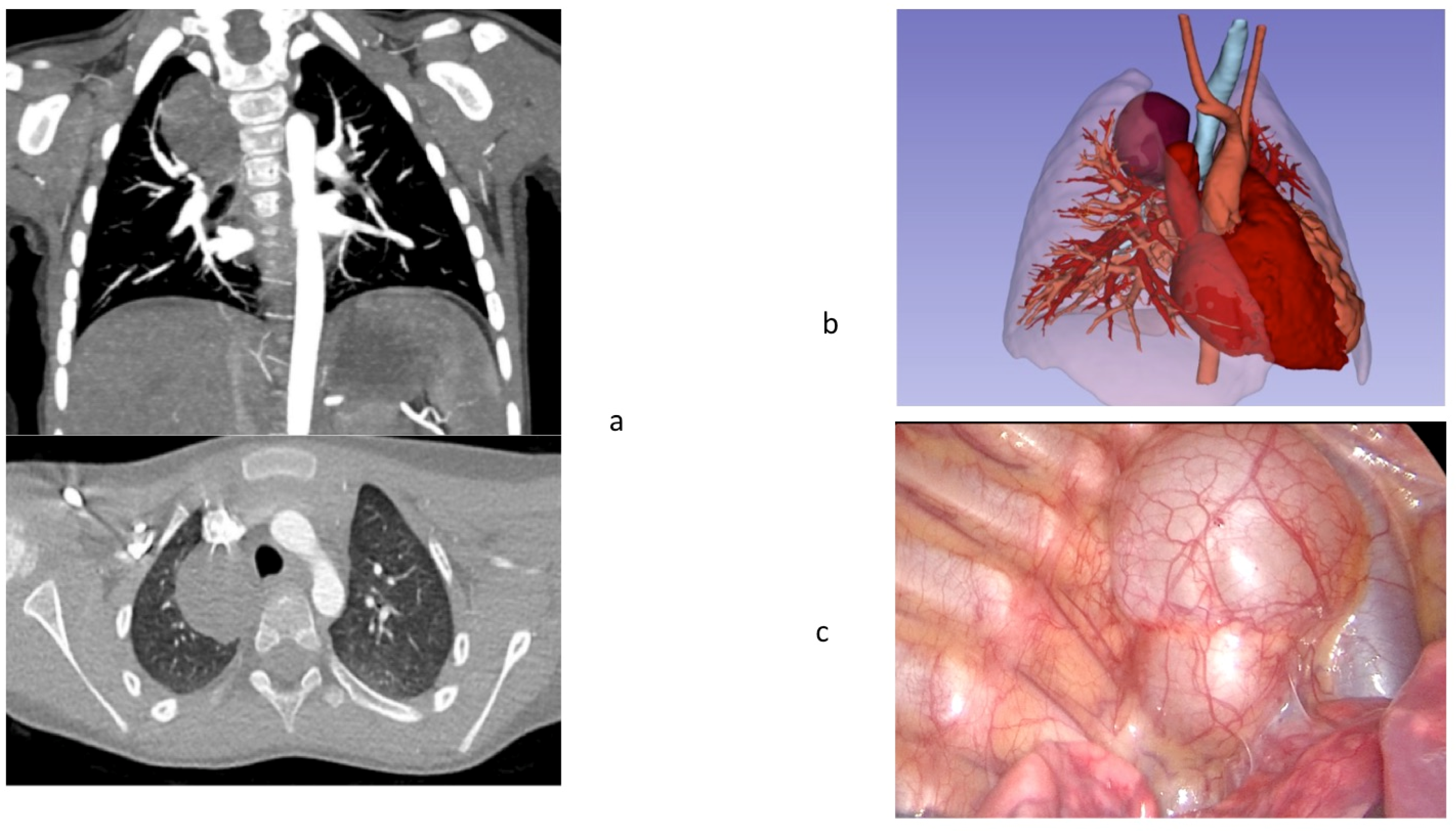
| Type of malformation | Right lobar bronchopulmonary sequestration Anomalous venous return | Right bronchogenic cyst | Left extralobar bronchopulmonary sequestration |
| Prenatal diagnosis | 20 weeks gestation | 22 weeks gestation | No prenatal diagnosis |
| Preoperative imaging | Intralobar pulmonary sequestration with surrounding areas of air trapping, possible hybrid malformation microcystic CPAM-pulmonary sequestration | Large Right bronchogenic cyst | Left extralobar sequestration |
| Symptoms at birth | Respiratory distress | No symptoms | Recurrent bronchopneumonia |
| Histology | Intralobar pulmonary sequestration and cystic adenomatoid malformation type 2 | Bronchogenic Cyst | Extralobar pulmonary sequestration and adenomatoid malformation type 3 |
| Surgery | Right Thoracoscopic lower lobectomy Dissection at the hilum | Thoracoscopic excision of bronchogenic cyst, dissection at the hilum | Thoracoscopic excision of pulmonary sequestration |
| Anatomical Structure | Virtual Reality HMD Set-Up | VATS |
|---|---|---|
| Visualization of hilum | -Excellent 3D view at the hilum of segmental structures | -2D = view |
| -Opportunity of rotation and evaluation of critical anatomy under different views 360° | ||
| Visualization of Bronchus and | ||
| -Excellent 3D view on segmental bronchi | -Poor orientation | |
| -Segmental bronchi -Bronchi orientation | -Excellent 3D orientation and relationship among structures | -Poor view on the bronchi 2D |
| Vessels | ||
| -Segmental artery and vein visualization | -Excellent 3d view on segmentation | -2D view |
| -Vessel orientation | -Excellent view on segmentation during orientation | |
| Approach to the pulmonary tissue | -realistic in-depth perception | -2D view, no depth perception |
| Pulmonary tissue | -No view on subsegmental structures | |
| -No advantages on tissue sparing | -Good control on tissue resection and manipulation | |
| -No tissue manipulation |
| Advantages | Debatable |
|---|---|
| Vessel anatomy variants detection | Sub-segmental artery, veins, bronchi division |
| Segmental artery, veins, bronchi division | Lack of simulation of lung inflation/deflation |
| Arteries, veins, bronchi orientation | Lack of simulation of virtual resection/transection and manipulation of pulmonary tissue |
| Realistic in-depth perception |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelizzo, G.; Costanzo, S.; Roveri, M.; Lanfranchi, G.; Vertemati, M.; Milani, P.; Zuccotti, G.; Cassin, S.; Panfili, S.; Rizzetto, F.; et al. Developing Virtual Reality Head Mounted Display (HMD) Set-Up for Thoracoscopic Surgery of Complex Congenital Lung MalFormations in Children. Children 2022, 9, 50. https://doi.org/10.3390/children9010050
Pelizzo G, Costanzo S, Roveri M, Lanfranchi G, Vertemati M, Milani P, Zuccotti G, Cassin S, Panfili S, Rizzetto F, et al. Developing Virtual Reality Head Mounted Display (HMD) Set-Up for Thoracoscopic Surgery of Complex Congenital Lung MalFormations in Children. Children. 2022; 9(1):50. https://doi.org/10.3390/children9010050
Chicago/Turabian StylePelizzo, Gloria, Sara Costanzo, Margherita Roveri, Giulia Lanfranchi, Maurizio Vertemati, Paolo Milani, Gianvincenzo Zuccotti, Simone Cassin, Sebastiano Panfili, Francesco Rizzetto, and et al. 2022. "Developing Virtual Reality Head Mounted Display (HMD) Set-Up for Thoracoscopic Surgery of Complex Congenital Lung MalFormations in Children" Children 9, no. 1: 50. https://doi.org/10.3390/children9010050