1. Introduction
Episodic vertigo in children is common but it frequently remains an underestimated symptom despite the fact that it could be detrimental to regular school attendance and leisure activities [
1]. The most common cause of episodic vertigo in children is vestibular migraine (VM) [
2], and headache can occur before, simultaneously or after vestibular symptoms; phonophobia, photophobia and motion sickness are often associated complaints.
The mechanisms that account for vestibular symptoms in adults with VM have been extensively investigated and a dysfunctional vestibulo–thalamo–cortical network [
3], the involvement of subclinical cerebellar–vestibular pathways [
4] and structural changes in the central vestibular cortex [
5,
6] have been proposed at different times. The debate over the mechanistic basis of VM in childhood is still open. Higher genetic susceptibility is suspected, given that most children with VM have a family history of migraines, but evidence to support heritability is limited [
7]. Once a correct diagnosis is established, medications are frequently effective in reducing symptoms [
8]. A careful examination of trigger symptoms is a prerequisite for successful non-pharmacological prophylaxis and rehabilitation [
9].
It is known that sensitivity to repeated, moving full-field visual scenes and motion is frequently reported in children with vestibular disorders and migraine [
10]. A previous case–control study in children with migraine without vestibular symptoms suggested abnormal visually-evoked postural responses (VEPRs) with respect to healthy subjects when exposed to a full-field horizontal optokinetic stimulation (OKN-S) [
11]. In addition, adult patients with both migraine (M) and VM exhibited a greater instability induced by OKN-S in the interictal period than healthy subjects [
12,
13]. Furman et al. stated that balance perturbation induced by OKN-S was greater in VM patients compared to subjects with M and suggested that this difference depends on a greater susceptibility of the former when exposed to large, moving scenes, such as traffic, crowded supermarkets, etc. [
14].
Dizziness and unsteadiness induced by optic flow, the so-called visually induced dizziness (ViD), is thought to depend on the inability of the central nervous system to process “conflicting” information from the vestibular and visual systems, such as those elicited in humans by standing still on the sidewalk and watching cars passing by. In such a situation, signals from the visual system suggest motion in contrast to vestibular and somatosensory information that indicates no head and body movement (visual–vestibular mismatch). Since ViD and balance disturbances can be improved by rehabilitation techniques that are based on OKN-S [
15], it is reasonable to suppose that children with VM could benefit from this approach. Unfortunately, there is currently no systematic study of VEPRs in this population, and it is not yet known if visual optic flow is an effective trigger of balance perturbation. Therefore, the aim of this study was to analyse VEPRs in children affected by VM.
2. Materials and Methods
This cross-sectional study was based on children referred to the Tertiary Centre for Vestibular and Balance Disorders of the University Hospital of Modena from the Centre for the Diagnosis and Treatment of Headaches of the same institution between 2013 and 2019.
The casuistry was composed of school-age children (6–12 years old) affected by vestibular migraine (group VM) and by migraine without aura (group M). Diagnosis has been defined according to the criteria proposed for adults recently reintroduced by the Committee for the Classification of Vestibular Disorders of the Bárány Society and the International Headache Society to define VM in childhood [
16,
17,
18]
Diagnostic criteria for VM were: at least 5 episodes with vestibular symptoms lasting between five minutes and 72 h; a history of migraine with\without aura; at least half of the episodes associated at with one of the following three migraine features: headache, (with at least two of the following four characteristics: One-sided location; Pulsating quality; Moderate or severe pain intensity; Aggravation by routine physical activity) photophobia and phonophobia; visual aura.
Children with middle and/or inner ear diseases were excluded. Parents were also asked to complete the Child Behaviour Checklist [
19] to rule out subclinical psychological disorders, such as anxiety, that could account for an impairment of vestibulo–spinal reflexes during OKN stimulation [
20]; subjects with psychological distress were excluded.
A group of children, well-matched for sex and age, selected from a database of healthy children, served as controls (group C).
2.1. Procedures
Preliminary Vestibular Tests
Subjects admitted to the study underwent a battery of preliminary vestibular tests, including videonystagmoscopy, electronystagmography with caloric tests (no specific test was performed to analyse pursuit gain and saccadic accuracy) and cervical vestibular evoked potentials (cVEMPs).
The tests were performed during symptom-free periods in order to detect spontaneous, positional and paroxysmal nystagmus and peripheral vestibular hyporeflexia/areflexia.
Nystagmus was considered pathological if the slow-phase velocity was greater than 3°/section in primary gaze. Caloric tests, performed according to the Fitzgerald–Hallpike technique, were considered pathological if the Jongkees’s formula was greater than 25%.
cVEMPs were considered abnormal if absent or with increased peak latencies or with large interaural amplitude asymmetry. Subsequently Children were Submitted to the Stabilometric Session
2.2. Stabilometric Session
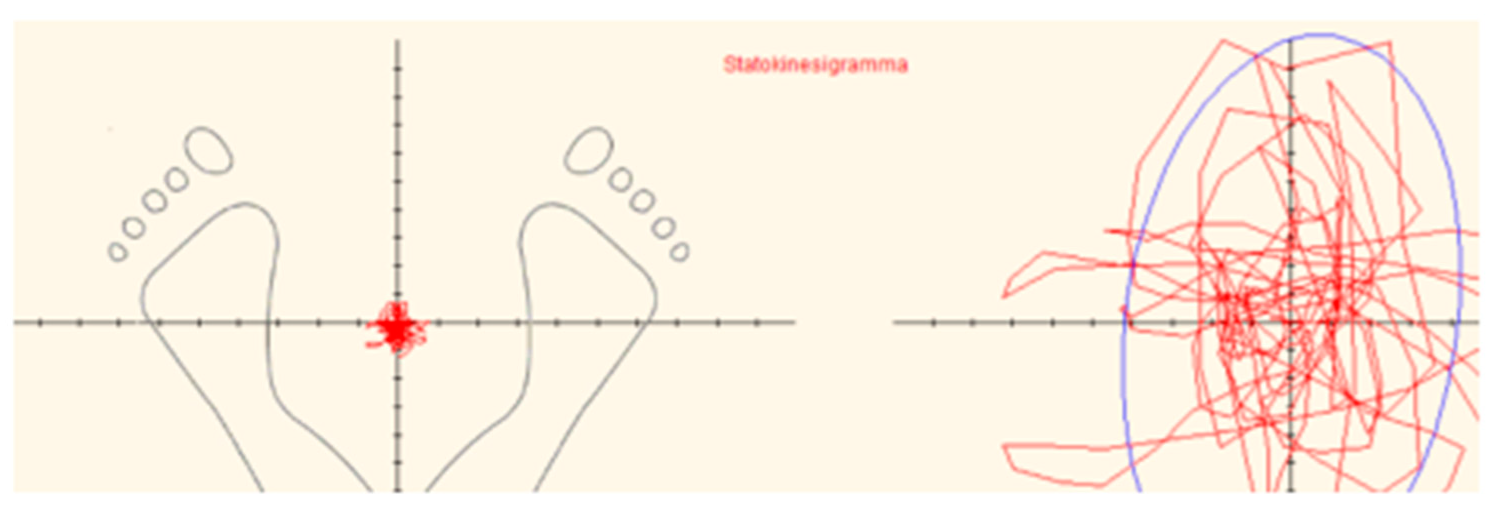
Static posturography was performed by a standardized stabilometric force platform (Svep-Politecnica). Technical data and procedure details are described in previous studies [
11,
20]. Briefly, the displacements of the centre of pressure (COP) that roughly correspond to the projection of the body centre of gravity to the ground were continuously registered during a period of 52 s with a sampling frequency of 50 Hz, and the resulting sway path, the so-called statokinesigram (SKG), was recorded (
Figure 1).
Four SKGs were obtained from all subjects while standing still on the stabilometric platform, under different visual conditions:
(1) With open eyes (OE) while gazing a vertical bar at a distance of 150 cm (cm) in front of them;
(2) Closed eyes (CE);
(3–4) During a full-field horizontal OKN-S that was delivered onto the wall in front of them at a 2 m distance, it was represented by vertical alternating white and dark bars rolling at a regular speed of 30° per second, from left to right and vice versa.
The sequence of the tests was randomly changed from one child to another, to avoid adaptation due to a possible learning effect.
The ratio of SKG-S measured under CE and OE conditions multiplied per 100, the so-called ‘stabilometric Romberg quotient’ (RI), was computed to assess the influence of static visual cues on the multisensory control of posture. Furthermore, the ratio between the sum of SKG-S recorded in the two tests during OKN-S and SKG-S in the OE condition was computed (OKN destabilizing index). This ratio is indicative of each subject’s sensitivity to moving visual surroundings with respect to static visual references [
21].
2.3. Electronystagmography Recordings
Electronystagmography was performed during the last two tests in order to record OKN reflex parameters: angular slow phase velocity (ASPV), number of saccades (NS), mean peak velocity of saccades (MPVS). ASPV and MPVS are expressed in degrees/second. Electronystagmographic recordings of OKN reflexes were executed over a period of 20 s (excluding the beginning and the final phase of the stimulation).
2.4. Statistical Analysis
Continuous variables were expressed as mean ± standard deviations (SD); continuous variables were compared between three groups (M, VM and C) with the one-way analysis of variance followed by the Tukey–Kramer post hoc comparison test. Fisher’s exact test was used to analyse gender homogeneity between patients and controls. p-values lower than 0.05 were considered significant. Statistical Package Software, version 16, was used for statistical analyses.
3. Results
Demographic characteristics of subjects and headache features are indicated in
Table 1.
The VM group was composed of 20 children, the M group of 19 and in the C group there were 20 children. Gender and age distribution among M, VM and C groups were not different. At this point, the participants of the groups were considered well-matched.
Furthermore, no difference was found between the VM and M groups with respect to the mean duration of illness and the time interval between the last headache attack and the day of examination. In no case was this interval shorter than 9 days or longer than 12 days with respect to the vertigo crisis. In all VM cases, headache was pulsatile and had one-side location features. In the M group, headache was unilateral in 15 children, pulsatile in 14. The number of headache attacks per month was lower in the VM than in the M group.
Concerning vestibular symptoms (VM group), in five subjects they preceded the crises (precritical), in eight subjects they accompanied the crises (critical) and in seven subjects they followed them (postcritical).
None of the participants developed headache during or after the stabilometric session, while nearly one half of children (nine cases) with VM complained of oncoming nausea and imbalance during OKN-S. Nevertheless, no subject had to discontinue either test.
3.1. Stabilometric Data
Stabilometric data are summarized in
Table 2, where the one-way analysis of variance and the Tukey–Kramer post hoc tests are reported. No significant difference between groups was observed concerning the value of SKG-S under the OE condition.
In the CE condition, SKG-S was significantly increased in both VM and M children compared to the C group, with no difference between the former two.
Stabilometric RI was increased only in the VM group with respect to healthy subjects, with no difference between the two pathological samples.
SKG-S induced by OKN-S to the right evidenced differences between groups: the M group did not exhibit an increased SKG-S with respect to controls, while a significant difference was shown between VM and M children and between the former and healthy controls.
SKG-S recorded with OKN-S to the left were different between groups. The tests did not induce statistically different SGK-S between healthy subjects and the M group. However, the VM group exhibited increased SKG-S with respect to both M and C children. As a consequence, the OKN destabilizing index was greater in the VM group compared to healthy subjects and M children, and no difference was evident between the latter two.
3.2. Electronystagmographic Recordings during Stabilometric Session
Electronystagmographic results are summarized in
Table 3 where one-way analyses of variance and Tukey–Kramer post hoc tests are reported.
Electronystagmographic recordings of OKN reflexes induced by horizontal optic flow delivered to the right revealed a reduced ASPV in VM with respect to both M and C groups, and no difference was found between M and C subjects. Total NS was also lower in the VM group than in M children and in controls it was found to be intermediate between the latter two. MPVS was reduced in VM with respect to both M and C groups, and no difference was revealed between these two latter groups.
Similarly, the optic flow delivered to the left induced a reduced ASPV in VM with respect to both M and C groups, and no difference was recorded between M and C subjects.
In the same session, NS was accordingly reduced in VM with respect to both M and C groups, and no difference was elicited between the latter two.
Finally, MPVS showed a significant reduction in children with VM compared to M children and healthy controls. This OKN reflex parameter did not significantly vary between M and C groups.
4. Discussion
This study investigated the postural control of children affected by migraine without aura and by VM in a juvenile population. In addition to base stabilometric conditions by static posturography, two further trials with horizontal OKN-S were performed to explore VEPRs.
A preliminary vestibular examination excluded the presence of peripheral vestibular disorders that could account for postural perturbations per se during both quiet stance and, above all, during OKN-S [
22]. At this stage, subjects with pathological ocular signs (spontaneous nystagmus and paroxysmal and persistent positional nystagmus), hyporeflexia as determined by caloric tests and altered vestibulo-collic reflexes were not included in this casuistry, in contrast to other studies on both children and adults [
23,
24,
25]. Postural stability in the OE condition was not different among groups, in contrast to CE, which disclosed a significant increase of SKG-S both in M and VM groups with respect to controls. Accordingly, stabilometric RI was increased in the former groups. It is therefore suggested that both M and VM in childhood entail a perturbation of the postural system due to a central vestibular dysfunction rather than a peripheral one. However, if static visual references are available, these postural perturbations become negligible. It is well-known that, among all sensory systems of the body, humans primarily use vision to enable the brain to integrate multisensory information regarding the relative position of the body in space and continuously adjust posture accordingly [
26]. Moreover, when vestibular information is defective, the central nervous system compensates for sensory deficiencies by further increasing the weight of visual cues to preserve upright posture [
27]. The reliance on static visual cues for postural control, so-called ‘visual dependency’, is not only present in adults with vestibular disorders [
28] but also in healthy children under 16 years and adolescents [
29]. This study documented the increase of ‘visual dependency’ in children with VM in accordance with previous studies of children with M [
11] and adults with VM [
13]. This study, however, showed that dynamic visual cues, such as those generated by OKN-S, are responsible for a destabilization of posture significantly greater in the two pathological groups than in controls and documented a further increase in children with VM relative to those with M.
Since these differences were present regardless of the direction of the OKN-S, the OKN destabilizing index behaved in accordance. A possible explanation for the difference of VEPRs between M and VM groups could be suggested by the difference of OKN reflex parameters recorded during optic flow with particular regard to ASPV and MPVS. It is generally accepted that the slow and fast phases of the OKN reflex consist of ocular pursuit and saccades, respectively, and abnormalities in both of these have been reported in children with vestibular migraine perhaps due to a central vestibular dysfunction [
25]. The increase of postural instability in children with M and VM in response to OKN-S recalls previous results both in children [
11] and adults [
12,
13,
14]. The exact mechanism of these abnormal VEPRs is not known bus some experiments suggested an altered interaction between visual and vestibular cortical networks [
12,
30]. It was also shown that healthy children may be more prone to ViD than adults because their ability to maintain adequate postural control in response to multisensory contradictory information is not complete before adolescence [
31]. Taken together, it is reasonable to suggest that large moving visual scenes, such as those commonly encountered in traffic or supermarkets, could be regarded as a trigger of balance disturbance in children with M and VM, even in vertigo- and pain-free intervals. This result closely resembles that of a recent investigation into adults with VM [
32]. This study concluded that recurrent attacks of dizziness are induced by routine moving visual stimuli in a high percentage of cases, so that visually busy environments can be considered as triggers.
The stabilometric results during optic flow reached an excellent significance level, so that the different behaviour of VEPRs in children suffering from vestibular migraine and in healthy controls has definitely been assessed.
The main limitation of the study is the small sample size, primarily due to the strict inclusion criteria. It should also be observed that electronystamographic tests for latency and the accuracy of horizontal and vertical saccades and pursuit gain were not executed in this study, so that the involvement of these ocular motor systems has only indirectly been analysed.
5. Conclusions
Postural strategies of children with migraine are different to those of healthy subjects, similarly to adults. These differences are even more relevant in children diagnosed as affected by VM. The stabilometric results of this study indicate a bimodal processing of visual information in the pain- and vertigo-free intervals: static visual references are effective in reducing body sway, and, in contrast, moving visual cues, such as those generated by OKN-S, are detrimental to postural control and a remarkable increase of body sway is clearly documented. This destabilization of posture is independent of the presence of peripheral vestibular disorders, and a reduced ability of the central nervous system to resolve the visual–vestibular mismatch induced by optic flow while standing still is postulated. For the first time, this study has shown that children with VM are critically destabilized by moving visual stimuli in the interictal period and this behavior could be interpreted as a marker of the disease. Finally, further studies are needed to verify if rehabilitation programs that incorporate OKN-S for balance disorders and motion sickness could be beneficial also for children with VM.
Author Contributions
Conceptualization, D.M., R.N. and C.B.; methodology, E.A. and D.M.; software, R.N.; validation, R.N., C.B., E.A., S.P. and A.C.; formal analysis, D.M.; investigation, D.M., E.A., R.N. and C.B.; resources, R.N., D.M. and C.B.; data curation, D.M.; writing—original draft preparation, D.M., E.A. and S.P.; writing—review and editing, D.M., S.P. and A.C.; supervision, S.P. and A.C.; project administration, D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. This study was approved by the Emilia Romagna region (AVEN) Ethical Committee (n: 1921, code NOC09 77/09, 10 June 2009). Written informed consent was obtained from parents of every participant, and the study was conducted according to the latest version of the declaration of Helsinki.
Institutional Review Board Statement
The study was approved by the provincial ethical committee of Modena (protocol number: 1921; study code: NOC09). All procedures in the study were in accordance with the ethical standards of the University of Modena and Reggio Emilia and with the latest version of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from the parents of all subjects involved in the study.
Data Availability Statement
The data presented in this study are available from the corresponding author on request due to privacy restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| C | Control |
| COP | Centre of pressure |
| CE | Closed eyes |
| OE | Open eyes |
| M | Migraine |
| VM | Vestibular migraine |
| VMC | Vestibular migraine in childhood |
| OKN | Optokinetic |
| RI | Romberg’s index |
| SKG | Statokinesigram |
| SKG-S | Statokinesiogram surface |
| ASPV | Angular slow phase velocity |
| MPVS | Mean peak velocity of saccades |
| VEPR | Visually evoked postural response |
| ViD | Visuall -induced Dizziness |
| cVEMPs | Cervical vestibular evoked potentials |
| Centimeters | cm |
| Millimeters | mm |
| Square millimeters | mm2 |
References
- Jahn, K. Vertigo and dizziness in children. Handb. Clin. Neurol. 2016, 137, 353–363. [Google Scholar] [PubMed]
- Langhagen, T.; Landgraf, M.N.; Huppert, D.; Heinen, F.; Jahn, K. Vestibular Migraine in Children and Adolescents. Curr. Pain Headache Rep. 2016, 20, 67. [Google Scholar] [CrossRef]
- Russo, A.; Marcelli, V.; Esposito, F.; Corvino, V.; Marcuccio, L.; Giannone, A.; Conforti, R.; Marciano, E.; Tedeschi, G.; Tessitore, A. Abnormal thalamic function in patients with vestibular migraine. Neurology 2014, 82, 2120–2126. [Google Scholar] [CrossRef] [Green Version]
- King, S.; Wang, J.; Priesol, A.J.; Lewis, R.F. Central Integration of Canal and Otolith Signals is Abnormal in Vestibular Migraine. Front. Neurol. 2014, 10, 233. [Google Scholar] [CrossRef] [Green Version]
- Messina, R.; Rocca, M.A.; Colombo, B.; Teggi, R.; Falini, A.; Comi, G.; Filippi, M. Structural brain abnormalities in patients with vestibular migraine. J. Neurol. 2017, 264, 295–303. [Google Scholar] [CrossRef]
- Zhe, X.; Zhang, X.; Chen, L.; Zhang, L.; Tang, M.; Zhang, D.; Li, L.; Lei, X.; Jin, C. Altered Gray Matter Volume and Functional Connectivity in Patients with Vestibular Migraine. Front. Neurosci. 2021, 15, 683802. [Google Scholar] [CrossRef] [PubMed]
- Paz-Tamayo, A.; Perez-Carpena, P.; Lopez-Escamez, J.A. Systematic Review of Prevalence Studies and Familial Aggregation in Vestibular Migraine. Front. Genet. 2020, 11, 954. [Google Scholar] [CrossRef]
- Brodsky, J.R.; Cusick, B.A.; Zhou, G. Evaluation and management of vestibular migraine in children: Experience from a pediatric vestibular clinic. Eur. J. Paediatr. Neurol. 2016, 20, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.D.; Herdman, S.J.; Whitney, S.L.; Cass, S.P.; Clendaniel, R.A.; Fife, T.D.; Furman, J.M.; Getchius, T.S.D.; Goebel, J.A.; Shepard, N.T.; et al. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Evidence-Based Clinical Practice Guideline. J. Neurol. Phys. Ther. 2016, 40, 124–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlou, M.; Whitney, S.L.; Alkathiry, A.A.; Huett, M.; Luxon, L.M.; Raglan, E.; Godfrey, E.L.; Bamiou, D.E. Visually Induced Dizziness in Children and Validation of the Pediatric Visually Induced Dizziness Questionnaire. Front. Neurol. 2017, 8, 656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baraldi, C.; Gherpelli, C.; Alicandri Ciufelli, M.; Monzani, D.; Pini, L.A.; Pani, L.; Guerzoni, S. A case-control study of visually evoked postural responses in childhood with primary headaches. Neurol. Sci. 2020, 41, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Rossi, C.; Alberti, A.; Sarchielli, P.; Mazzotta, G.; Capocchi, G.; Faralli, M.; Ricci, G.; Molini, E.; Altissimi, G. Balance disorders in headache patients: Evaluation by computerized static stabilometry. Acta Neurol. Scand. 2005, 111, 407–413. [Google Scholar] [CrossRef]
- Panichi, R.; Cipriani, L.; Sarchielli, P.; Di Mauro, M.; Pettorossi, V.; Ricci, G.; Faralli, M. Balance control impairment induced after OKS in patients with vestibular migraine: An intercritical marker. Eur. Arch. Otorhinolaryngol. 2015, 272, 2275–2282. [Google Scholar] [CrossRef] [PubMed]
- Furman, J.M.; Sparto, P.J.; Soso, M.; Marcus, D. Vestibular function in migraine-related dizziness: A pilot study. J. Vestib. Res. 2005, 15, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Pavlou, M.; Kanegaonkar, R.G.; Swapp, D.; Bamiou, D.E.; Slater, M.; Luxon, L.M. The effect of virtual reality on visual vertigo symptoms in patients with peripheral vestibular dysfunction: A pilot study. J. Vestib. Res. 2012, 22, 273–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lempert, T.; Olesen, J.; Furman, J.; Waterston, J.; Seemungal, B.; Carey, J.; Bisdorff, A.; Versino, M.; Evers, S.; Newman-Toker, D. Vestibular migraine: Diagnostic criteria. J. Vestib. Res. 2012, 22, 167–172. [Google Scholar] [CrossRef] [Green Version]
- van de Berg, R.; Widdershoven, J.; Bisdorff, A.; Evers, S.; Wiener-Vacher, S.; Cushing, S.L.; Mack, K.J.; Kim, J.S.; Jahn, K.; Strupp, M.; et al. Vestibular Migraine of Childhood and Recurrent Vertigo of Childhood: Diagnostic criteria Consensus document of the Committee for the Classification of Vestibular Disorders of the Bárány Society and the International Headache Society. J. Vestib. Res. 2021, 31, 1–9. [Google Scholar] [CrossRef]
- Tancredi, R.; Milone, A.; Floriani, C.; Marcheschi, M.; Muratori, F. La CBCL nella valutazione della psicopatologia in età evolutiva: Presentazione di una esperienza su un campione clinico di soggetti tra 4 e 16 anni. Riv. Ital. Pediatr. 2000, 26, 477–483. [Google Scholar]
- Monzani, D.; Marchioni, D.; Bonetti, S.; Pellacani, P.; Casolari, L.; Rigatelli, M.; Presutti, L. Anxiety affects vestibulospinal function of labyrinthine-defective patients during horizontal optokinetic stimulation. Acta Otorhinolaryngol. Ital. 2004, 24, 117–124. [Google Scholar]
- Bronstein, A.M. Visual vertigo syndrome: Clinical and posturography findings. J. Neurol. Neurosurg. Psychiatry 1995, 59, 472–476. [Google Scholar] [CrossRef]
- Van Ombergen, A.; Lubeck, A.J.; Van Rompaey, V.; Maes, L.K.; Stins, J.F.; Van de Heyning, P.H.; Wuyts, F.L.; Bos, J.E. The Effect of Optokinetic Stimulation on Perceptual and Postural Symptoms in Visual Vestibular Mismatch Patients. PLoS ONE 2016, 11, e0154528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Brevern, M.; Zeise, D.; Neuhauser, H.; Clarke, A.H.; Lempert, T. Acute migrainous vertigo: Clinical and oculographic findings. Brain 2005, 128, 365–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teggi, R.; Colombo, B.; Bernasconi, L.; Bellini, C.; Comi, G.; Bussi, M. Migrainous vertigo: Results of caloric testing and stabilometric findings. Headache 2009, 49, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Langhagen, T.; Lehrer, N.; Borggraefe, I.; Heinen, F.; Jahn, K. Vestibular migraine in children and adolescents: Clinical findings and laboratory tests. Front. Neurol. 2014, 5, 292. [Google Scholar] [CrossRef] [Green Version]
- Grace, G.M.; Alpert, P.T.; Cross, C.; Louis, M.; Kowalski, S. Postural balance in young adults: The role of visual, vestibular and somatosensory systems. J. Am. Acad. Nurse Pract. 2012, 24, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Voda, A.; Martin, O.; Naves, N.; Paulo, R.; Gascuel, J.D.; Schmerber, S. Visual-vestibular compensation in balance recovery: A transfer function model-based analysis. IFAC PapersOnLine 2019, 52, 88–93. [Google Scholar] [CrossRef]
- Cousins, S.; Cutfield, N.J.; Kaski, D.; Palla, A.; Seemungal, B.M.; Golding, J.F.; Staab, J.P.; Bronstein, A.M. Visual Dependency and Dizziness after Vestibular Neuritis. PLoS ONE 2014, 9, e105426. [Google Scholar] [CrossRef] [Green Version]
- Steindl, R.; Kunz, K.; Schrott-Fischer, A.; Scholtz, A.W. Effect of age and sex on maturation of sensory systems and balance control. Dev. Med. Child. Neurol. 2006, 48, 477–482. [Google Scholar] [CrossRef]
- Griebe, M.; Flux, F.; Wolf, M.E.; Hennerici, M.G.; Szabo, K. Multimodal assessment of optokinetic visual stimulation response in migraine with aura. Headache 2014, 54, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Bednarczuk, N.F.; Bonsu, A.; Ortega, M.C.; Fluri, A.S.; Chan, J.; Rust, H.; de Melo, F.; Sharif, M.; Seemungal, B.M.; Golding, J.F.; et al. Abnormal visuo-vestibular interactions in vestibular migraine: A cross sectional study. Brain 2019, 142, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Greffou, S.; Faubert, J. Life-span study of visually driven postural reactivity: A fully immersive virtual reality approach. J. Vis. 2008, 8, 426. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}