
Antibiotic Resistance Patterns of Uropathogens Causing Urinary Tract Infections in Children with Congenital Anomalies of Kidney and Urinary Tract

 , , , , , , and
, , , , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Urine Sampling
2.4. Antimicrobial Susceptibility
2.5. Data Collection
2.6. Statistical Analysis
3. Results
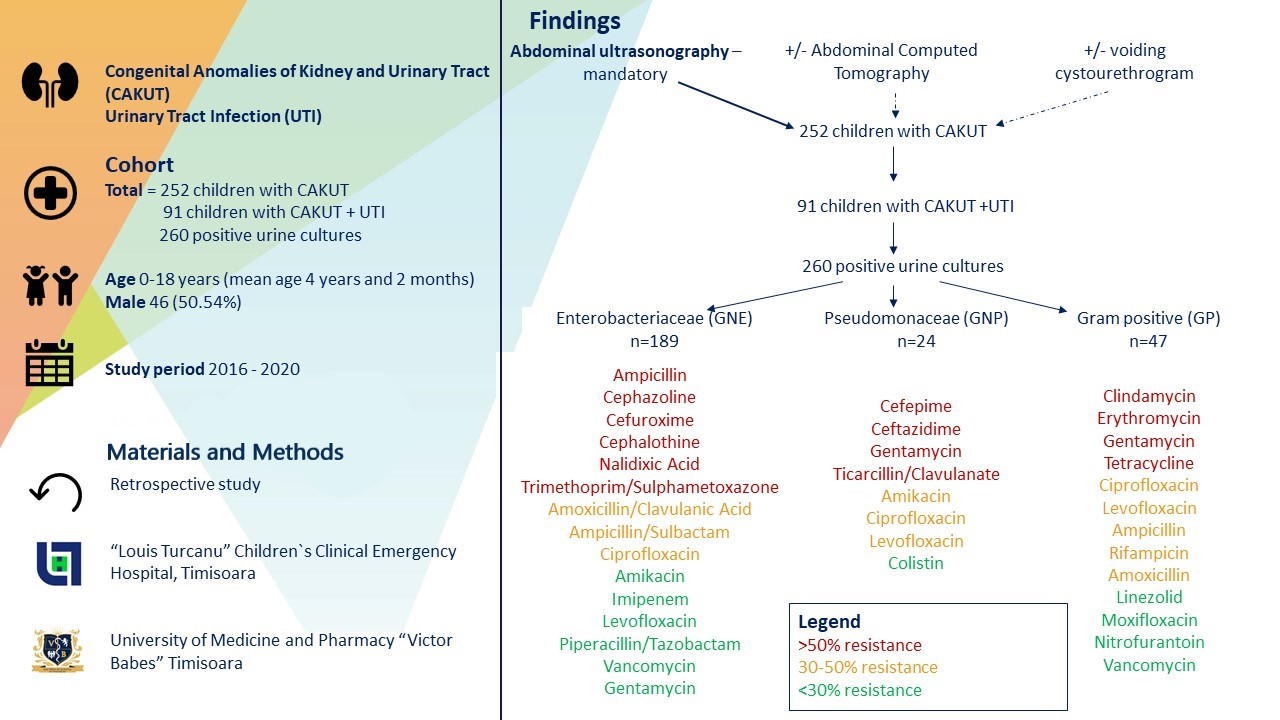
3.1. Type of CAKUT
3.2. Number of UTIs
3.3. Types of Uropathogens
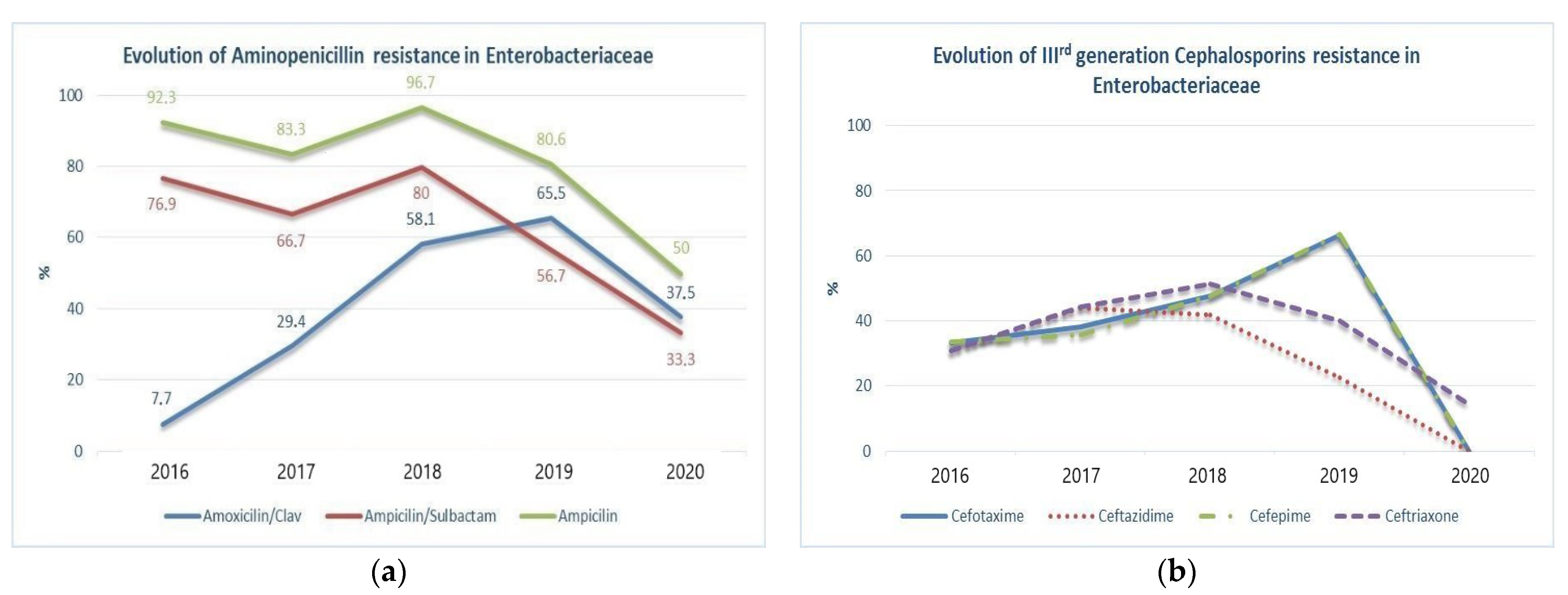
3.4. Uropathogens Antibiotic Resistance
4. Discussion
4.1. Uropathogens Antibiotic Resistance
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramos, N.L.; Dzung, D.T.N.; Stopsack, K.; Jankó, V.; Pourshafie, M.R.; Katouli, M.; Brauner, A. Characterisation of uropathogenic Escherichia coli from children with urinary tract infection in different countries. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 1587–1593. [Google Scholar] [CrossRef]
- Alper, B.S.; Curry, S.H. Urinary Tract Infection in Children. Am. Fam. Physician 2005, 72, 2483–2488. [Google Scholar]
- Stein, R.; Dogan, H.S.; Hoebeke, P.; Kočvara, R.; Nijman, R.J.; Radmayr, C.; Tekgül, S. Urinary tract infections in children: EAU/ESPU guidelines. Eur. Urol. 2015, 67, 546–558. [Google Scholar] [CrossRef]
- Twaij, M. Urinary tract infection in children: A review of its pathogenesis and risk factors. J. R. Soc. Promot. Health 2000, 120, 220–226. [Google Scholar] [CrossRef]
- Larkins, N.G.; Hewitt, I.K. Urinary Tract Infection in Children. Curr. Pediatr. Rep. 2018, 6, 259–268. [Google Scholar] [CrossRef]
- Alberici, I.; Bayazit, A.K.; Drozdz, D.; Emre, S.; Fischbach, M.; Harambat, J.; Jankauskiene, A.; Litwin, M.; Mir, S.; Morello, W.; et al. Pathogens causing urinary tract infections in infants: A European overview by the ESCAPE study group. Eur. J. Pediatr. 2015, 174, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Pendleton, J.N.; Gorman, S.P.; Gilmore, B.F. Clinical relevance of the ESKAPE pathogens. Expert Rev. Anti. Infect. Ther. 2013, 11, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Benkő, R.; Gajdács, M.; Matuz, M.; Bodó, G.; Lázár, A.; Hajdú, E.; Papfalvi, E.; Hannauer, P.; Erdélyi, P.; Pető, Z. Prevalence and antibiotic resistance of eskape pathogens isolated in the emergency department of a tertiary care teaching hospital in hungary: A 5-year retrospective survey. Antibiotics 2020, 9, 624. [Google Scholar] [CrossRef] [PubMed]
- A‘t Hoen, L.; Bogaert, G.; Radmayr, C.; Dogan, H.S.; Nijman, R.J.M.; Quaedackers, J.; Rawashdeh, Y.F.; Silay, M.S.; Tekgul, S.; Bhatt, N.R.; et al. Update of the EAU/ESPU guidelines on urinary tract infections in children. J. Pediatr. Urol. 2021, 17, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.B.; Downs, S.M.; Finnell, S.M.E.; Hellerstein, S.; Shortliffe, L.D.; Wald, E.R.; Zerin, J.M.; Davidson, C. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 2011, 128, 595–610. [Google Scholar] [PubMed] [Green Version]
- Shah, G.; Upadhyay, J. Controversies in the diagnosis and management of urinary tract infections in children. Paediatr. Drugs 2005, 7, 339–346. [Google Scholar] [CrossRef]
- Ammenti, A.; Alberici, I.; Brugnara, M.; Chimenz, R.; Guarino, S.; La Manna, A.; La Scola, C.; Maringhini, S.; Marra, G.; Materassi, M.; et al. Updated Italian recommendations for the diagnosis, treatment and follow-up of the first febrile urinary tract infection in young children. Acta Paediatr. 2020, 109, 236–247. [Google Scholar] [CrossRef]
- Korbel, L.; Howell, M.; Spencer, J.D. The clinical diagnosis and management of urinary tract infections in children and adolescents. Paediatr. Int. Child. Health 2017, 37, 273–279. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E. Comparative epidemiology and resistance trends of Proteae in urinary tract infections of inpatients and outpatients: A 10-year retrospective study. Antibiotics 2019, 8, 91. [Google Scholar] [CrossRef] [Green Version]
- Palleroni, N.J.; Bradbury, J.F. Stenotrophomonas, a new bacterial genus for Xanthomonas maltophilia (Hugh 1980) Swings et al. 1983. Int. J. Syst. Bacteriol. 1993, 43, 606–609. [Google Scholar] [CrossRef] [Green Version]
- Miyakita, H.; Hayashi, Y.; Mitsui, T.; Okawada, M.; Kinoshita, Y.; Kimata, T.; Koikawa, Y.; Sakai, K.; Satoh, H.; Tokunaga, M.; et al. Guidelines for the medical management of pediatric vesicoureteral reflux. Int. J. Urol. 2020, 27, 480–490. [Google Scholar] [CrossRef] [Green Version]
- Murugapoopathy, V.; Gupta, I.R. A primer on congenital anomalies of the kidneys and urinary tracts (CAKUT). Clin. J. Am. Soc. Nephrol. 2020, 15, 723–731. [Google Scholar] [CrossRef] [PubMed]
- Çetinkaya, P.G.; Gülhan, B.; Düzova, A.; Beşbaş, N.; Hayran, M.; Topaloğlu, R.; Özaltın, F. Clinical characteristics of children with congenital anomalies of the kidney and urinary tract and predictive factors of chronic kidney disease. Turk. J. Pediatr. 2020, 62, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Harambat, J.; Van Stralen, K.J.; Kim, J.J.; Tizard, E.J. Epidemiology of chronic kidney disease in children. Pediatr. Nephrol. 2012, 27, 363–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, D.; Wang, Q.; Shi, Z.; Sun, J. Congenital Anomalies of the Kidney and Urinary Tract in Children with Congenital Heart Defects. Kidney Blood Press. Res. 2020, 45, 307–313. [Google Scholar] [CrossRef]
- Ramayani, O.R.; Eyanoer, P.C.; Ritarwan, K.; Siregar, B.; Siregar, R.S. Prevalence of recurrent urinary tract infection in children with congenital anomalies of the kidney and urinary tract (CAKUT). IOP Conf. Ser. Earth Environ. Sci. 2018, 125. [Google Scholar] [CrossRef]
- Loukogeorgakis, S.P.; Burnand, K.; MacDonald, A.; Wessely, K.; De Caluwe’, D.; Rahman, N.; Farrugia, M.-K. Renal scarring is the most significant predictor of breakthrough febrile urinary tract infection in patients with simplex and duplex primary vesico-ureteral reflux. J. Pediatr. Urol. 2020, 16, 189.e1–189.e7. [Google Scholar] [CrossRef]
- Díaz Álvarez, M.; Acosta Batista, B.; Pérez Córdova, R.; Hernández Robledo, E. Urinary tract infection caused by Enterobacteriaceae and its relationship with vesicoureteral reflux. Bol. Med. Hosp. Infant. Mex. 2017, 74, 34–40. [Google Scholar] [CrossRef]
- Buettcher, M.; Trueck, J.; Niederer-Loher, A.; Heininger, U.; Agyeman, P.; Asner, S.; Berger, C.; Bielicki, J.; Kahlert, C.; Kottanattu, L.; et al. Swiss consensus recommendations on urinary tract infections in children. Eur. J. Pediatr. 2021, 180, 663–674. [Google Scholar] [CrossRef]
- Ladhani, S.; Gransden, W. Increasing antibiotic resistance among urinary tract isolates. Arch. Dis. Child. 2003, 88, 444–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashkenazi, S.; Even-Tov, S.; Samra, Z.; Dinari, G. Uropathogens of various childhood populations and their antibiotic susceptibility. Pediatr. Infect. Dis. J. 1991, 10, 742–746. [Google Scholar] [CrossRef]
- Kutasy, B.; Coyle, D.; Fossum, M. Urinary Tract Infection in Children: Management in the Era of Antibiotic Resistance-A Pediatric Urologist’s View. Eur. Urol. Focus 2017, 3, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Tratselas, A.; Iosifidis, E.; Ioannidou, M.; Saoulidis, S.; Kollios, K.; Antachopoulos, C.; Sofianou, D.; Roilides, E. Outcome of Urinary Tract Infections Caused by Extended Spectrum β-Lactamase-producing Enterobacteriaceae in Children. Pediatr. Infect. Dis. J. 2011, 30, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Okarska-Napierała, M.; Wasilewska, A.; Kuchar, E. Urinary tract infection in children: Diagnosis, treatment, imaging—Comparison of current guidelines. J. Pediatr. Urol. 2017, 13, 567–573. [Google Scholar] [CrossRef]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: Systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van De Sande-Bruinsma, N.; Grundmann, H.; Verloo, D.; Tiemersma, E.; Monen, J.; Goossens, H.; Ferech, M.; The European Antimicrobial Resistance Surveillance System and European Surveillance of Antimicrobial Consumption Project Groups. Antimicrobial drug use and resistance in Europe. Emerg. Infect. Dis. 2008, 14, 1722–1730. [Google Scholar] [CrossRef]
- Shaikh, N.; Hoberman, A.; Keren, R.; Ivanova, A.; Gotman, N.; Chesney, R.W.; Carpenter, M.A.; Moxey-Mims, M.; Wald, E.R. Predictors of Antimicrobial Resistance among Pathogens Causing Urinary Tract Infection in Children. J. Pediatr. 2016, 171, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Delbet, J.D.; Lorrot, M.; Ulinski, T. An update on new antibiotic prophylaxis and treatment for urinary tract infections in children. Expert Opin. Pharmacother. 2017, 18, 1619–1625. [Google Scholar] [CrossRef]
- Stultz, J.S.; Doern, C.D.; Godbout, E. Antibiotic Resistance in Pediatric Urinary Tract Infections. Curr. Infect. Dis. Rep. 2016, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Qader, A.; Hasan, J.; Hasan, Z. Bacteriuria in Children with Special Reference to Structural Abnormalities of Urinary Tract. J. Ped. Nephrol. 2020, 8. [Google Scholar] [CrossRef]
- Yilmaz, Y.; Tekkanat Tazegun, Z.; Aydin, E.; Dulger, M. Bacterial uropathogens causing urinary tract infection and their resistance patterns among children in Turkey. Iran. Red Crescent Med. J. 2016, 18, e26610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-Gil, T.; Martínez, J.L.; Blanco, P. Mechanisms of antimicrobial resistance in Stenotrophomonas maltophilia: A review of current knowledge. Expert Rev. Anti. Infect. Ther. 2020, 18, 335–347. [Google Scholar] [CrossRef]
- Parente, G.; Gargano, T.; Pavia, S.; Cordola, C.; Vastano, M.; Baccelli, F.; Gallotta, G.; Bruni, L.; Corvaglia, A.; Lima, M. Pyelonephritis in Pediatric Uropathic Patients: Differences from Community-Acquired Ones and Therapeutic Protocol Considerations. A 10-Year Single-Center Retrospective Study. Children 2021, 8, 436. [Google Scholar]
- Shaikh, N.; Craig, J.C.; Rovers, M.M.; Da Dalt, L.; Gardikis, S.; Hoberman, A.; Montini, G.; Rodrigo, C.; Taskinen, S.; Tuerlinckx, D.; et al. Identification of Children and Adolescents at Risk for Renal Scarring After a First Urinary Tract Infection: A Meta-analysis With Individual Patient Data. JAMA Pediatr. 2014, 168, 893–900. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Number (%) | <12 Months (n = 42) | 1–3 Years (n = 17) | 3–6 Years (n = 8) | Over 6 Years (n = 24) | Total (n = 91) |
|---|---|---|---|---|---|
| Age distribution | 46.15% | 18.68% | 8.79% | 26.37% | 100% |
| Male | 29 (69.04%) | 9 (52.94%) | 3 (37.5%) | 5 (20.83%) | 46 (50.54%) |
| CAKUT Type | |||||
| Renal malformation | 4 (9.52%) | 1 (5.88%) | 1 (12.5%) | 3 (12.5%) | 9 (9.89%) |
| Urethral malformation | 32 (76.19%) | 16 (94.11) | 6 (75%) | 19 (79.16%) | 73 (80.21%) |
| Vesical/subvesical malformation | 6 (14.28%) | - | 1 (12.5%) | 2 (8.33%) | 9 (9.89%) |
| Number of UTIs | |||||
| 1 to 4 UTIs | 36 (85.71) | 14 (82.35%) | 7 (87.5%) | 20 (83.33%) | 77 (84.61%) |
| 5 to 9 UTIs | 4 (9.52%) | 3 (17.64%) | 1 (12.5%) | 2 (8.3%) | 10 (10.98%) |
| Over 10 UTIs | 2 (4.76%) | - | - | 2 (8.3%) | 4 (4.39%) |
| Type of Uropathogens | Total N = 260 | Percentage (%) | 2016 n = 21 | 2017 n = 50 | 2018 n = 81 | 2019 n = 77 | 2020 n = 31 |
|---|---|---|---|---|---|---|---|
| GNE | 189 | 72.69 | 17 (80.95%) | 34 (68%) | 61 (75.30%) | 55 (71.42%) | 22 (70.96%) |
| E. coli | 101 | 38.84 | 13 | 18 | 31 | 31 | 8 |
| Klebsiella spp. | 55 | 21.15 | 3 | 10 | 17 | 21 | 4 |
| Proteus spp. | 21 | 8.07 | - | - | 9 | 2 | 10 |
| Enterobacter spp. | 6 | 2.30 | 1 | 1 | 3 | 1 | - |
| Serratia spp. | 3 | 1.15 | - | 3 | - | - | - |
| Citrobacter spp. | 2 | 0.76 | - | 2 | - | - | - |
| Morganella morganii | 1 | 0.38 | - | - | 1 | - | - |
| GNP | 24 | 9.23 | - | 5 (10%) | 12 (14.81%) | 3 (3.89%) | 4 (12.90%) |
| Pseudomonas spp. | 21 | 8.07 | - | 4 | 10 | 3 | 4 |
| Stenotrophomonas maltophilia | 2 | 0.76 | - | - | 2 | - | - |
| Ralstonia pickettii | 1 | 0.38 | - | 1 | - | - | - |
| GP | 47 | 18.07 | 4 (19.04%) | 11 (22%) | 8 (9.87%) | 19 (24.67%) | 5 (16.12%) |
| Enterococcus spp. | 41 | 15.76 | 4 | 11 | 7 | 15 | 4 |
| Staphylococcus aureus | 4 | 1.53 | - | - | - | 4 | - |
| Streptococcus agalactiae | 2 | 0.76 | - | - | 1 | - | 1 |
| Type of Uropathogens | UTI in Males (n = 151) | UTI in Females (n = 109) | p * |
| E. coli | 41 (27.2%) | 60 (55.0%) | <0.001 |
| Klebsiella spp. | 42 (27.8%) | 13 (11.9%) | <0.001 |
| Enterobacter spp. | 3 (2.0%) | 3 (2.8%) | 0.001 |
| Proteus spp. | 18 (11.9%) | 3 (2.8%) | 0.001 |
| Citrobacter amalonaticus | 2 (1.3%) | 0 (0.0%) | - |
| Serratia marcescens | 2 (1.3%) | 1 (0.9%) | 0.570 |
| Morganella morganii | 1 (0.7%) | 0 (0.0%) | - |
| Pseudomonas spp. | 8 (5.3%) | 13 (11.9%) | <0.001 |
| Stenotrophomonas maltophilia | 0 (0.0%) | 2 (1.8%) | - |
| Ralstonia pickettii | 1 (0.7%) | 0 (0.0%) | - |
| Enterococcus spp. | 28 (18.5%) | 13 (11.9%) | <0.001 |
| Staphylococcus aureus | 4 (2.6%) | 0 (0.0%) | - |
| Streptococcus agalactiae | 1 (0.7%) | 1 (0.9%) | - |
| Antibiotic | E. coli % | Klebsiella spp. % | p * |
|---|---|---|---|
| Ceftazidime | 14.9% | 42.6% | 0.002 |
| Ceftibuten | 0.0% | 87.5% | <0.001 |
| Ceftriaxone | 25.3% | 51.9% | 0.003 |
| Gentamycin | 27% | 64.8% | <0.001 |
| Netilmicin | 11.8% | 44% | 0.005 |
| Nitrofurantoin | 13.2% | 75.8% | <0.001 |
| Piperacillin/Tazobactam | 7.4% | 24.0% | 0.043 |
| Trimethoprim/Sulfamethoxazole | 56.6% | 73.5% | 0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isac, R.; Basaca, D.-G.; Olariu, I.-C.; Stroescu, R.F.; Ardelean, A.-M.; Steflea, R.M.; Gafencu, M.; Chirita-Emandi, A.; Bagiu, I.C.; Horhat, F.G.; et al. Antibiotic Resistance Patterns of Uropathogens Causing Urinary Tract Infections in Children with Congenital Anomalies of Kidney and Urinary Tract. Children 2021, 8, 585. https://doi.org/10.3390/children8070585
Isac R, Basaca D-G, Olariu I-C, Stroescu RF, Ardelean A-M, Steflea RM, Gafencu M, Chirita-Emandi A, Bagiu IC, Horhat FG, et al. Antibiotic Resistance Patterns of Uropathogens Causing Urinary Tract Infections in Children with Congenital Anomalies of Kidney and Urinary Tract. Children. 2021; 8(7):585. https://doi.org/10.3390/children8070585
Chicago/Turabian StyleIsac, Raluca, Diana-Georgiana Basaca, Ioana-Cristina Olariu, Ramona F. Stroescu, Andrada-Mara Ardelean, Ruxandra M. Steflea, Mihai Gafencu, Adela Chirita-Emandi, Iulia Cristina Bagiu, Florin George Horhat, and et al. 2021. "Antibiotic Resistance Patterns of Uropathogens Causing Urinary Tract Infections in Children with Congenital Anomalies of Kidney and Urinary Tract" Children 8, no. 7: 585. https://doi.org/10.3390/children8070585