
Regulation of Serum Sodium Levels during Chemotherapy Using Selective Arginine Vasopressin V2-Receptor Antagonist Tolvaptan in a Four-Year-Old Girl with a Suprasellar Germ Cell Tumor


Abstract
:
1. Introduction
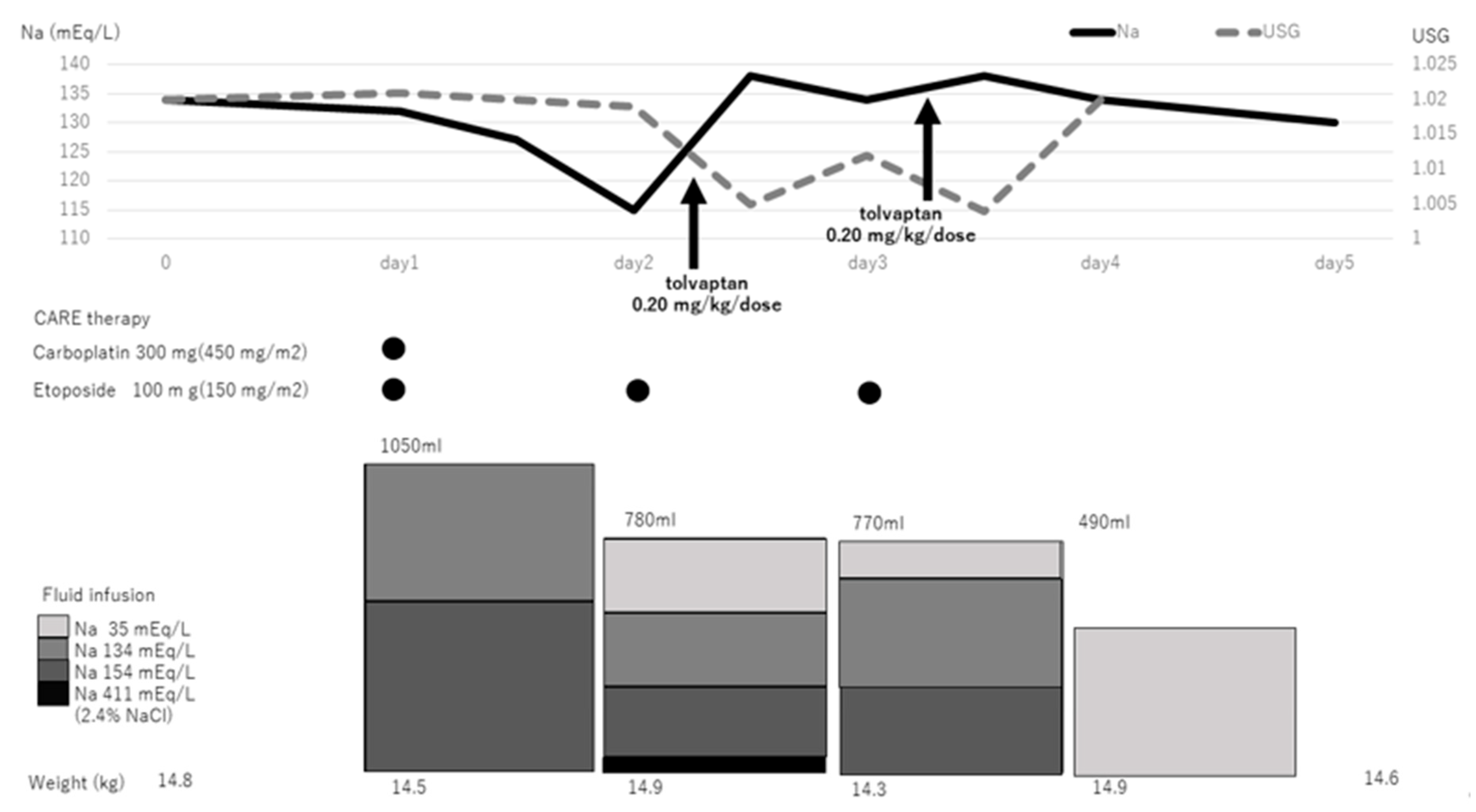
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berl, T. Vasopressin antagonists. N. Engl. J. Med. 2015, 372, 2207–2216. [Google Scholar] [CrossRef] [PubMed]
- Aditya, S.; Rattan, A. Vaptans: A new option in the management of hyponatremia. Int. J. Appl. Basic Med. Res. 2012, 2, 77–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuesta, M.; Thompson, C.J. The syndrome of inappropriate antidiuresis (SIAD). Best. Pract. Res. Clin. Endocrinol. Metab. 2016, 30, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Rondon-Berrios, H. Urea for Chronic Hyponatremia. Blood Purif. 2020, 49, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Arima, H.; Goto, K.; Motozawa, T.; Mouri, M.; Watanabe, R.; Hirano, T.; Ishikawa, S.E. Open-label, multicenter, dose-titration study to determine the efficacy and safety of tolvaptan in Japanese patients with hyponatremia secondary to syndrome of inappropriate secretion of antidiuretic hormone. Endocr. J. 2021, 68, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Willemsen, R.H.; Delgado-Carballar, V.; Elleri, D.; Thankamony, A.; Burke, G.A.; Nicholson, J.C.; Dunger, D.B. Tolvaptan use during hyperhydration in paediatric intracranial lymphoma with SIADH. Endocrinol. Diabetes Metab. Case Rep. 2016, 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Tuli, G.; Tessaris, D.; Einaudi, S.; De Sanctis, L.; Matarazzo, P. Tolvaptan Treatment in Children with Chronic Hyponatremia due to Inappropriate Antidiuretic Hormone Secretion: A Report of Three Cases. J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Gürbüz, F.; Taştan, M.; Turan, İ.; Yüksel, B. Efficiency of Single Dose of Tolvaptan Treatment During the Triphasic Episode After Surgery for Craniopharyngioma. J. Clin. Res. Pediatr. Endocrinol. 2019, 11, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Marx-Berger, D.; Milford, D.V.; Bandhakavi, M.; Van’t Hoff, W.; Kleta, R.; Dattani, M.; Bockenhauer, D. Tolvaptan is successful in treating inappropriate antidiuretic hormone secretion in infants. Acta Paediatr. 2016, 105, 334–337. [Google Scholar] [CrossRef] [PubMed]
- Koksoy, A.Y.; Kurtul, M.; Ozsahin, A.K.; Cayci, F.S.; Tayfun, M.; Bayrakci, U.S. Tolvaptan Use to Treat SIADH in a Child. J. Pediatr. Pharmacol. Ther. 2018, 23, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Kraayvanger, L.; Latza, J.; Vockelmann, C.; Berlit, P.; Weber, R. Tolvaptan treatment of severe stroke-like symptoms and bilateral subcortical diffusion restriction due to syndrome of inappropriate secretion of ADH after polytrauma. J. Neurol. 2014, 261, 1436–1438. [Google Scholar] [CrossRef] [PubMed]
- Verbalis, J.G.; Goldsmith, S.R.; Greenberg, A.; Korzelius, C.; Schrier, R.W.; Sterns, R.H.; Thompson, C.J. Diagnosis, evaluation, and treatment of hyponatremia: Expert panel recommendations. Am. J. Med. 2013, 126, S1–S42. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Blood Chemistry | Endocrine Tests | (Reference Values) | ||||
|---|---|---|---|---|---|---|
| TP | 6.5 | g/dL | ADH | 1.1 | pg/mL | <0.5 |
| BUN | 8.0 | mg/dL | BNP | <5.8 | pg/mL | <18.4 |
| UA | 3.9 | mg/dL | Aldosterone | 6.0 | ng/mL | 3.6–24.0 |
| Cre | 0.19 | mg/dL | PRA | 1.0 | ng/mL/h | 0.2–2.7 |
| Na | 121 | mEq/L | ACTH | 8.9 | pg/mL | 7.2–21.0 |
| K | 3.6 | mEq/L | Cortisol | 5.5 | μg/dL | 6.4–21.0 |
| Cl | 93 | mEq/L | ||||
| TG | 198 | mg/dL | ||||
| BG | 106 | mg/dL | ||||
| Plasma Osm | 252 | mOsm/kg | ||||
| Urinalysis | ||||||
| Urine specific gravity | 1.024 | |||||
| Na | 194 | mEq/L | ||||
| Cre | 48 | mEq/L | ||||
| Urine Osm | 708 | mOsm/kg |
| Authors | Age (Years) | Cause of SIADH | Initial Dose of Tolvaptan (mg/kg/dose) | Change in s-Na (mEq/L) * | Maximum UV (mL/kg/h) * | References |
|---|---|---|---|---|---|---|
| Koksoy, et al. | 16 | Idiopathic | 0.28 | 115 to 122 in 16 h | 9 | [10] |
| Marx-Berger, et al. | 0.2 | Idiopathic | 0.8 | 138 to 153 in 2 days | No data | [9] |
| Marx-Berger, et al. | 0.3 | Idiopathic | 0.6 | No data | No data | [9] |
| Willemsen, et al. | 11 | Intracranial B-cell lymphoma | 0.14 | 119 to 130 in 2 days | 8 | [6] |
| Tuli, et al. | 7 | ROHHAD syndrome | 0.06 | No data | No data | [7] |
| Tuli, et al. | 4 | A large sellar and suprasellar tumor | 0.1 | No data | No data | [7] |
| Tuli, et al. | 5 | Hypothalamic astrocytoma | 0.05 | No data | No data | [7] |
| Gürbüz, et al. | 13 | Craniopharyngioma | 0.13 | 117 to 126 in 4 h | 8.1 | [8] |
| Kraayvanger, et al. | 17 | Severe polytrauma | 15 mg/day | 116 to 139 in 24 h | No data | [11] |
| Hiroshima, et al. | 4 | Suprasellar germ cell tumor | 0.2 | 126 to 138 mEq/L in 10 h | 15 at 4 h | This study |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hiroshima, S.; Nyuzuki, H.; Sasaki, S.; Ogawa, Y.; Nagasaki, K. Regulation of Serum Sodium Levels during Chemotherapy Using Selective Arginine Vasopressin V2-Receptor Antagonist Tolvaptan in a Four-Year-Old Girl with a Suprasellar Germ Cell Tumor. Children 2021, 8, 293. https://doi.org/10.3390/children8040293
Hiroshima S, Nyuzuki H, Sasaki S, Ogawa Y, Nagasaki K. Regulation of Serum Sodium Levels during Chemotherapy Using Selective Arginine Vasopressin V2-Receptor Antagonist Tolvaptan in a Four-Year-Old Girl with a Suprasellar Germ Cell Tumor. Children. 2021; 8(4):293. https://doi.org/10.3390/children8040293
Chicago/Turabian StyleHiroshima, Shota, Hiromi Nyuzuki, Sunao Sasaki, Yohei Ogawa, and Keisuke Nagasaki. 2021. "Regulation of Serum Sodium Levels during Chemotherapy Using Selective Arginine Vasopressin V2-Receptor Antagonist Tolvaptan in a Four-Year-Old Girl with a Suprasellar Germ Cell Tumor" Children 8, no. 4: 293. https://doi.org/10.3390/children8040293