
Development of a Stress Scale for Siblings of Childhood Cancer Patients


Abstract
:1. Introduction
2. Materials and Methods
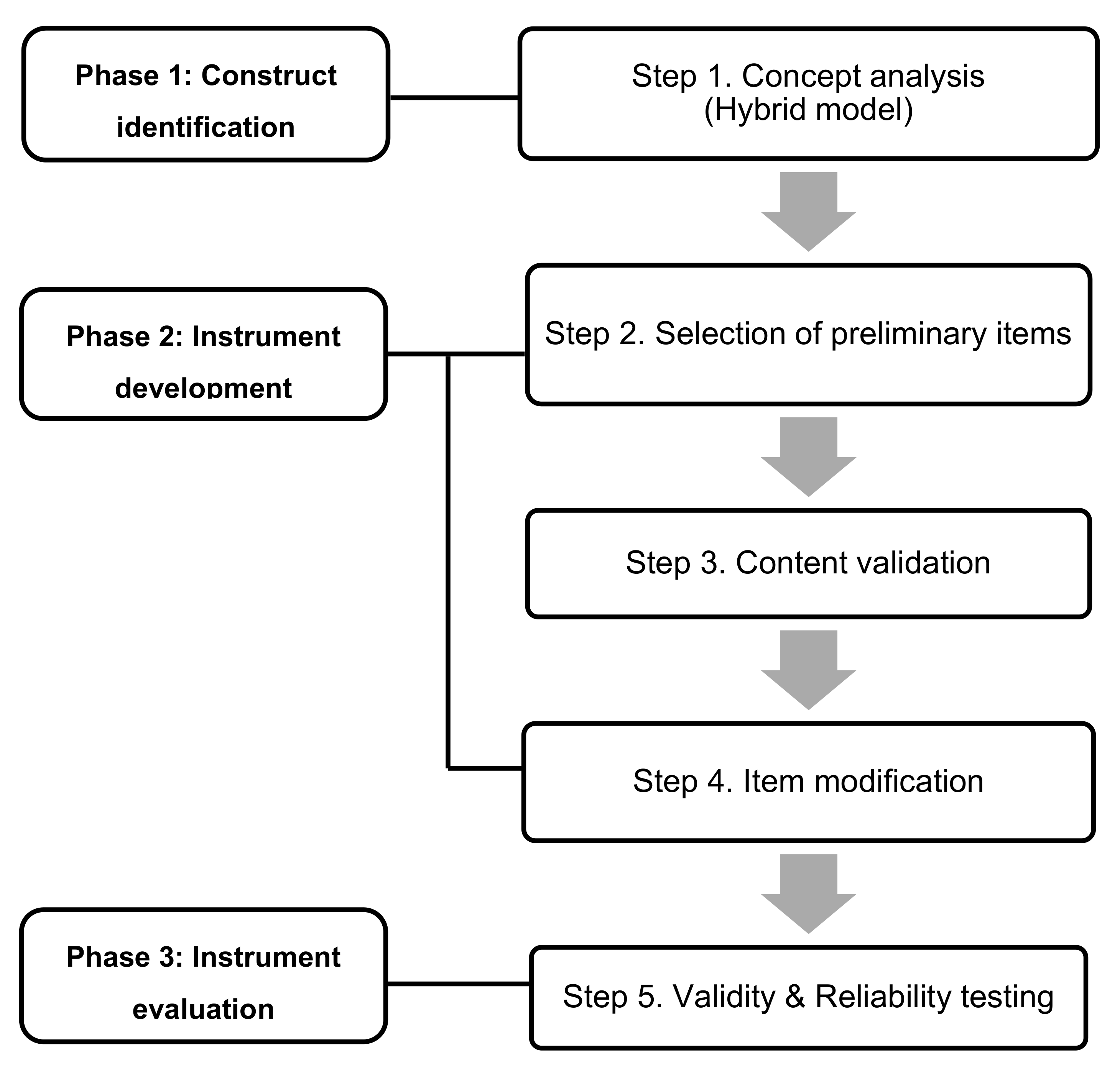
2.1. Process 1: Instrument Development
2.2. Process 2: Instrument Evaluation
2.2.1. Participants
2.2.2. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Item Analysis
3.3. Construct Validity
3.4. Criterion Validation
3.5. Reliability
3.6. Final Scale Design
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Statistics Korea. Available online: http://kostat.go.kr/assist/synap/preview/skin/doc.html?fn=synapview385219_2&rs=/assist/synap/preview (accessed on 20 September 2020).
- Alderfer, M.A.; Logan, B.A.; DiDonato, S.; Jackson, L.; Hayes, M.J.; Sigmon, S.T. Change across time in cancer-related traumatic stress symptoms of siblings of children with cancer: A preliminary investigation. J. Clin. Psychol. Med. Settings 2020, 27, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, L.M.; Kaal, K.J.; Bradley, L.; Alderfer, M.A. Cancer-related traumatic stress reactions in siblings of children with cancer. Fam. Syst. Health 2013, 31, 205–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, K.A.; Alderfer, M.A.; Ewing, L.J.; Marsland, A.L. The role of contextual threat in predicting self-reported distress among siblings of children with cancer. J. Clin. Psychol. Med. Settings 2013, 20, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Alderfer, M.A.; Long, K.A.; Lown, E.A.; Marsland, A.L.; Ostrowski, N.L.; Hock, J.M.; Ewing, L.J. Psychosocial adjustment of siblings of children with cancer: A systematic review. Psycho Oncol. 2010, 19, 789–805. [Google Scholar] [CrossRef]
- Toft, T.; Alfonsson, S.; Hovén, E.; Carlsson, T. Feeling excluded and not having anyone to talk to: Qualitative study of interpersonal relationships following a cancer diagnosis in a sibling. Eur. J. Oncol. Nurs. 2019, 42, 76–81. [Google Scholar] [CrossRef]
- Alderfer, M.A.; Stanley, C.; Conroy, R.; Long, K.A.; Fairclough, D.L.; Kazak, A.E.; Noll, R.B. The social functioning of siblings of children with cancer: A multi-informant investigation. J. Pediatr. Psychol. 2015, 40, 309–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houtzager, B.A.; Grootenhuis, M.A.; Last, B.F. Adjustment of siblings to childhood cancer: A literature review. Support. Care Cancer 1999, 7, 302–320. [Google Scholar] [CrossRef]
- Long, K.A.; Marsland, A.L.; Alderfer, M.A. Cumulative family risk predicts sibling adjustment to childhood cancer. Cancer 2013, 119, 2503–2510. [Google Scholar] [CrossRef] [Green Version]
- DeVellis, R.F. Scale development: Theory and Applications, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Yu, J.; Bang, K.S. Concept analysis of stress in siblings of patient with childhood cancer. Child. Health Nurs. Res. 2017, 23, 190–198. [Google Scholar] [CrossRef] [Green Version]
- Lynn, M.R. Determination and quantification of content validity. Nurs Res. 1986, 35, 382–386. [Google Scholar] [CrossRef]
- Kalkbrenner, M.T. A practical guide to instrument development and score validation in the social science: The measure approach. Pract Assess. Res. Eval. 2021, 26. Available online: https://scholarworks.umass.edu/pare/vol26/iss1/1/ (accessed on 29 March 2021).
- Polit, D.F.; Beck, C.T. Nursing Research, 9th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011. [Google Scholar]
- Min, H.Y.; Yoo, A.J. Development of a daily hassles scale for school age children. KJCS 1998, 19, 77–96. [Google Scholar]
- Park, J.O.; Seo, Y.S. Validation of the perceived stress scale (PSS) on samples of Korean university students. Kor. J. Psychol. Gen. 2010, 29, 611–629. [Google Scholar]
- Howard, M.C. A review of exploratory factor analysis decisions and overview of current practices: What we are doing and how can we improve? Int. J. Hum. Comput Interact. 2016, 32, 51–62. [Google Scholar] [CrossRef]
- Houtzager, B.A.; Oort, F.J.; Hoekstra-Weebers, J.E.H.M.; Caron, H.N.; Grootenhuis, M.A.; Last, B.F. Coping and family functioning predict longitudinal psychological adaptation of siblings of childhood cancer patients. J. Pediatr Psychol. 2004, 29, 591–605. [Google Scholar] [CrossRef] [Green Version]
- Woodgate, R.L. Siblings’ experiences with childhood cancer—A different way of being in the family. Cancer Nurs. 2006, 29, 406–414. [Google Scholar] [CrossRef]
- Wilkins, K.L.; Woodgate, R.L. Transition: A conceptual analysis in the context of siblings of children with cancer. J. Pediatr. Nurs. 2006, 21, 256–265. [Google Scholar] [CrossRef]
- Long, K.A.; Marsland, A.L.; Wright, A.; Hinds, P. Creating a tenuous balance: Siblings’ experience of a brother’s or sister’s childhood cancer diagnosis. J. Pediatr. Onco Nurs. 2015, 32, 21–31. [Google Scholar] [CrossRef]
- Lovgren, M.; Bylund-Grenklo, T.; Jalmsell, L.; Wallin, A.E.; Kreicbergs, U. Bereaved siblings’ advice to health care professionals working with children with cancer and their families. J. Pediatr. Onco Nurs. 2016, 33, 297–305. [Google Scholar] [CrossRef]
- Barrera, M.; Fleming, C.F.; Khan, F.S. The role of emotional social support in the psychological adjustment of siblings of children with cancer. Child. Care Hlth Dev. 2004, 30, 103–111. [Google Scholar] [CrossRef]
- Zegaczewski, T.; Chang, K.; Coddington, J.; Berg, A. Factors related to healthy siblings’ psychosocial adjustment to children with cancer: An integrative review. J. Pediatr. Onco Nurs. 2016, 33, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.S. Social support for school-aged siblings of children with cancer: A comparison between parent and sibling perceptions. J. Pediatr. Onco Nurs. 2001, 18, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Hamama, R.; Ronen, T.; Feigin, R. Self-control, anxiety, and loneliness in siblings of children with cancer. Soc. Work Health Care 2000, 31, 63–83. [Google Scholar] [CrossRef]
- McDonald, F.E.J.; Patterson, P.; White, K.J.; Butow, P.; Bell, M.L. Predictors of unmet needs and psychological distress in adolescent and young adult siblings of people diagnosed with cancer. Psycho Oncol. 2015, 24, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.; Millar, B.; Visser, A. The development of an instrument to assess the unmet needs of young people who have a sibling with cancer: Piloting the sibling cancer needs instrument (SCNI). J. Pediatr. Onco Nurs. 2011, 28, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, K.L.; Woodgate, R.L. A review of qualitative research on the childhood cancer experience from the perspective of siblings: A need to give them a voice. J. Pediatr. Onco Nurs. 2005, 22, 305–319. [Google Scholar] [CrossRef] [PubMed]
- Bendor, S.J. Anxiety and isolation in siblings of pediatric cancer patients: The need for prevention. Soc. Work Health Care 1990, 14, 17–35. [Google Scholar] [CrossRef] [PubMed]
- Rodebaugh, T.L.; Woods, C.M.; Thissen, D.M.; Heimberg, R.G.; Chambless, D.; Rapee, R.M. More information from fewer items: The factor structure and item properties of the original and brief fear of negative evaluation scale. Psychol. Assess. 2004, 16, 169. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Mean ± SD or n (%) | |
|---|---|---|
| Gender | Boy | 60 (48.0) |
| Girl | 65 (52.0) | |
| Age (year) | 13.89 ± 3.00 | |
| School | Elementary school | 60 (48.0) |
| Middle school | 65 (52.0) | |
| Birth order | First | 73 (58.4) |
| Middle | 23 (18.4) | |
| Last | 29 (23.2) | |
| Birth order of patient | First | 35 (28.0) |
| Middle | 18 (14.4) | |
| Last | 72 (57.6) | |
| Age of patient (year) | 11.90 ± 4.48 | |
| Duration since diagnosis (month) | 21.06 ± 23.73 | |
| <1 yr | 50 (40.0) | |
| 1–2 yrs | 47 (37.6) | |
| 2–5 yrs | 21 (16.8) | |
| >5 yrs | 7 (5.6) | |
| Perceived socioeconomic status | High | 3 (2.4) |
| Middle | 104 (83.2) | |
| Low | 18 (14.4) | |
| Item Contents | M ± SD | Skewness | Kurtosis | ITC * | Cronbach’s α If Item Deleted | |
|---|---|---|---|---|---|---|
| 1 | I feel upset because my parents do not pay attention to me as much as they used to. | 2.22 ± 0.93 | 0.387 | −0.663 | 0.507 | 0.903 |
| 2 | I feel upset about how my ill sibling looks now. | 2.59 ± 0.99 | −0.287 | −0.921 | 0.497 | 0.904 |
| 3 | I feel upset because my family spends less recreational time together now (e.g., family trip, dining, etc.). | 2.49 ± 0.98 | 0.034 | −0.988 | 0.505 | 0.903 |
| 4 | I do not want to follow my parents to the hospital because I am scared of hospitals. | 1.68 ± 0.78 | 0.942 | 0.286 | 0.451 | 0.904 |
| 5 | I feel upset because my family does not talk to each other as much as before. | 1.98 ± 0.85 | 0.508 | −0.432 | 0.552 | 0.903 |
| 6 | I feel upset because I can no longer hang out with my ill sibling. | 2.58 ± 0.97 | −0.052 | −0.961 | 0.303 | 0.907 |
| 7 | I am scared of getting cancer myself. | 2.01 ± 0.95 | 0.448 | −0.903 | 0.469 | 0.904 |
| 8 | I feel uncomfortable because I cannot eat the food I want because of my ill sibling. | 1.97 ± 0.98 | 0.701 | −0.531 | 0.625 | 0.901 |
| 9 | In difficult times, I end up doing nothing because I do not know what to do. | 2.04 ± 0.89 | 0.474 | −0.574 | 0.597 | 0.902 |
| 10 | I feel upset because my parents seem to be fighting about the ill sibling. | 1.70 ± 0.82 | 0.865 | −0.208 | 0.586 | 0.902 |
| 11 | I am careful around my ill sibling for the fear of accidentally hurting him/her. | 2.52 ± 0.95 | −0.348 | −0.859 | 0.521 | 0.903 |
| 12 | Sometimes, I feel sick for no reason (e.g., headache, stomachache, etc.). | 2.13 ± 0.89 | 0.235 | −0.849 | 0.374 | 0.906 |
| 13 | I feel upset because my family seems to be doing poorly financially due to the medical costs. | 1.94 ± 0.86 | 0.590 | −0.377 | 0.576 | 0.902 |
| 14 | Talking about a disease scares me. | 1.94 ± 0.88 | 0.682 | −0.229 | 0.559 | 0.902 |
| 15 | Sometimes, I feel angry toward my ill sibling. | 2.32 ± 0.97 | 0.066 | −1.035 | 0.406 | 0.905 |
| 16 | I feel annoyed because I keep comparing the current situation with the better days in the past. | 1.97 ± 0.90 | 0.608 | −0.435 | 0.721 | 0.899 |
| 17 | I do not want to talk about my ill sibling with my teacher. | 2.34 ± 0.88 | 0.127 | −0.679 | 0.371 | 0.906 |
| 18 | I feel frustrated because I do not have any friends who can understand and talk about my situation. | 1.83 ± 0.82 | 0.767 | 0.054 | 0.436 | 0.905 |
| 19 | I feel worried that something bad will happen to my ill sibling. | 2.82 ± 0.88 | −0.583 | −0.203 | 0.312 | 0.907 |
| 20 | I feel upset at myself for not being able to do anything for my ill sibling. | 2.26 ± 0.83 | 0.256 | −0.435 | 0.363 | 0.906 |
| 21 | Taking care of household chores often is becoming burdensome. | 1.90 ± 0.85 | 0.841 | 0.285 | 0.427 | 0.905 |
| 22 | I feel upset because my parents only give my ill sibling special treatment. | 1.96 ± 0.99 | 0.680 | −0.667 | 0.665 | 0.900 |
| 23 | I do not want my classmates to find out about my ill sibling. | 2.34 ± 0.98 | 0.234 | −0.910 | 0.383 | 0.906 |
| 24 | I feel upset because my living environments have changed due to my sibling’s treatment (e.g., room change, moving, etc.). | 1.62 ± 0.84 | 1.222 | 0.698 | 0.475 | 0.904 |
| 25 | I feel discontent because I cannot participate in my favorite activities (hobbies, school activities, etc.) as much as I used to because of my ill sibling. | 1.79 ± 0.88 | 0.780 | −0.408 | 0.538 | 0.903 |
| 26 | I feel isolated because people close to me (friends, relatives, teachers, neighbors, etc.) seem to only care about my ill sibling. | 1.73 ± 0.86 | 1.107 | 0.640 | 0.586 | 0.902 |
| 27 | I feel guilty when I get angry at my ill sibling. | 2.00 ± 0.93 | 0.498 | −0.734 | 0.449 | 0.904 |
| Factor | Items | F1 | F2 | F3 | F4 | F5 | F6 | |
|---|---|---|---|---|---|---|---|---|
| Factor 1. Changes in daily life | 21 | Taking care of household chores often is becoming burdensome. | 0.768 | 0.069 | 0.085 | 0.130 | −0.123 | 0.024 |
| 26 | I feel isolated because people close to me (friends, relatives, teachers, neighbors, etc.) seem to only care about my ill sibling. | 0.696 | 0.249 | 0.058 | 0.185 | 0.166 | 0.000 | |
| 25 | I feel discontent because I cannot participate in my favorite activities (hobbies, school activities, etc.) as much as I used to because of my ill sibling. | 0.670 | 0.386 | 0.027 | −0.102 | 0.140 | 0.156 | |
| 18 | I feel frustrated because I do not have any friends who can understand and talk about my situation. | 0.667 | −0.100 | 0.016 | 0.198 | 0.168 | 0.183 | |
| 24 | I feel upset because my living environments have changed due to my sibling’s treatment (e.g., room change, moving, etc.). | 0.556 | 0.064 | 0.090 | 0.016 | 0.400 | 0.076 | |
| 13 | I feel upset because my family seems to be doing poorly financially due to the medical costs. | 0.409 | 0.236 | 0.442 | 0.116 | 0.120 | 0.119 | |
| Factor 2. Ineffective coping | 15 | Sometimes, I feel angry toward my ill sibling. | 0.031 | 0.733 | 0.109 | −0.041 | 0.260 | −0.112 |
| 12 | Sometimes, I feel sick for no reason (e.g., headache, stomachache, etc.). | −0.018 | 0.678 | 0.095 | 0.086 | 0.050 | 0.069 | |
| 8 | I feel uncomfortable because I cannot eat the food I want because of my ill sibling. | 0.255 | 0.670 | 0.085 | 0.211 | 0.230 | 0.116 | |
| 10 | I feel upset because my parents seem to be fighting about the ill sibling. | 0.379 | 0.597 | 0.157 | 0.162 | 0.022 | 0.095 | |
| 16 | I feel annoyed because I keep comparing the current situation with the better days in the past. | 0.472 | 0.523 | 0.271 | 0.185 | 0.218 | 0.041 | |
| 9 | In difficult times, I end up doing nothing because I do not know what to do. | 0.351 | 0.399 | 0.276 | 0.223 | 0.173 | 0.058 | |
| Factor 3. Worries about ill sibling | 20 | I feel upset at myself for not being able to do anything for my ill sibling. | −0.076 | 0.135 | 0.784 | 0.165 | −0.118 | 0.132 |
| 19 | I feel worried that something bad will happen to my ill sibling. | −0.030 | 0.007 | 0.783 | 0.010 | 0.065 | 0.061 | |
| 11 | I am careful around my ill sibling for the fear of accidentally hurting him/her. | 0.182 | 0.127 | 0.635 | 0.049 | 0.328 | 0.070 | |
| 2 | I feel upset about how my ill sibling looks now. | −0.008 | 0.076 | 0.580 | 0.490 | 0.176 | 0.073 | |
| 27 | I feel guilty when I get angry at my ill sibling. | 0.261 | 0.180 | 0.534 | 0.106 | 0.112 | −0.152 | |
| Factor 4. Changes in relationships with family members | 3 | I feel upset because my family spends less recreational time together now (e.g., family trip, dining, etc.). | 0.153 | 0.214 | 0.157 | 0.714 | −0.030 | 0.148 |
| 6 | I feel upset because I can no longer hang out with my ill sibling. | 0.135 | −0.293 | 0.354 | 0.682 | 0.101 | −0.123 | |
| 5 | I feel upset because my family does not talk to each other as much as before. | 0.056 | 0.345 | 0.206 | 0.637 | 0.002 | 0.307 | |
| 1 | I feel upset because my parents do not pay attention to me as much as they used to. | 0.358 | 0.301 | −0.140 | 0.584 | 0.240 | −0.090 | |
| 22 | I feel upset because my parents only give my ill sibling special treatment. | 0.449 | 0.487 | −0.087 | 0.470 | 0.180 | 0.149 | |
| Factor 5. Fear about childhood cancer | 4 | I do not want to follow my parents to the hospital because I am scared of hospitals. | 0.040 | 0.230 | 0.028 | 0.151 | 0.786 | 0.131 |
| 14 | Talking about a disease scares me. | 0.222 | 0.105 | 0.421 | 0.027 | 0.594 | 0.228 | |
| 7 | I am scared of getting cancer myself. | 0.235 | 0.275 | 0.157 | 0.034 | 0.560 | −0.016 | |
| Factor 6. Concealing information | 17 | I do not want to talk about my ill sibling with my teacher. | 0.003 | 0.087 | 0.154 | 0.108 | 0.256 | 0.826 |
| 23 | I do not want my classmates to find out about my ill sibling. | 0.389 | 0.039 | 0.027 | 0.082 | −0.010 | 0.786 | |
| Eigen value | 3.741 | 3.320 | 3.117 | 2.544 | 2.086 | 1.707 | ||
| Variance | 13.854 | 12.295 | 11.545 | 9.422 | 7.726 | 6.322 | ||
| Cumulative variance | 13.854 | 26.149 | 37.694 | 47.115 | 54.841 | 61.163 | ||
| Variables | F1 | F2 | F3 | F4 | F5 | F6 | SSSCCP |
|---|---|---|---|---|---|---|---|
| DHSSAC | 0.580 (<0.001) | 0.450 (<0.001) | 0.172 (0.189) | 0.287 (0.026) | 0.177 (0.175) | 0.049 (0.710) | 0.466 (<0.001) |
| SSSCCP = Stress Scale for Siblings of Childhood Cancer Patient DHSSAC = Daily Hassles Scale for School Age Children | |||||||
| F1 = Changes in daily life F2 = Ineffective coping F3 = Worries about ill sibling | F4 = Changes in relationships with family members F5 = Fear about childhood cancer F6 = Concealing information | ||||||
| Variables | F1 | F2 | F3 | F4 | F5 | F6 | SSSCCP |
|---|---|---|---|---|---|---|---|
| PSS | 0.571 (<0.001) | 0.357 (0.003) | 0.242 (0.053) | 0.421 (<0.001) | 0.406 (0.001) | 0.393 (0.001) | 0.514 (<0.001) |
| SSSCCP = Stress Scale for Siblings of Childhood Cancer Patient PSS = Perceived Stress Scale | |||||||
| F1 = Changes in daily life F2 = Ineffective coping F3 = Worries about ill sibling | F4 = Changes in relationships with family members F5 = Fear about childhood cancer F6 = Concealing information | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, J.; Bang, K.-S.; Kang, H.J. Development of a Stress Scale for Siblings of Childhood Cancer Patients. Children 2021, 8, 265. https://doi.org/10.3390/children8040265
Yu J, Bang K-S, Kang HJ. Development of a Stress Scale for Siblings of Childhood Cancer Patients. Children. 2021; 8(4):265. https://doi.org/10.3390/children8040265
Chicago/Turabian StyleYu, Juyoun, Kyung-Sook Bang, and Hyoung Jin Kang. 2021. "Development of a Stress Scale for Siblings of Childhood Cancer Patients" Children 8, no. 4: 265. https://doi.org/10.3390/children8040265