
Educational Pain Points for Pediatric Brain Tumor Survivors: Review of Risks and Remedies


Abstract
:1. Introduction
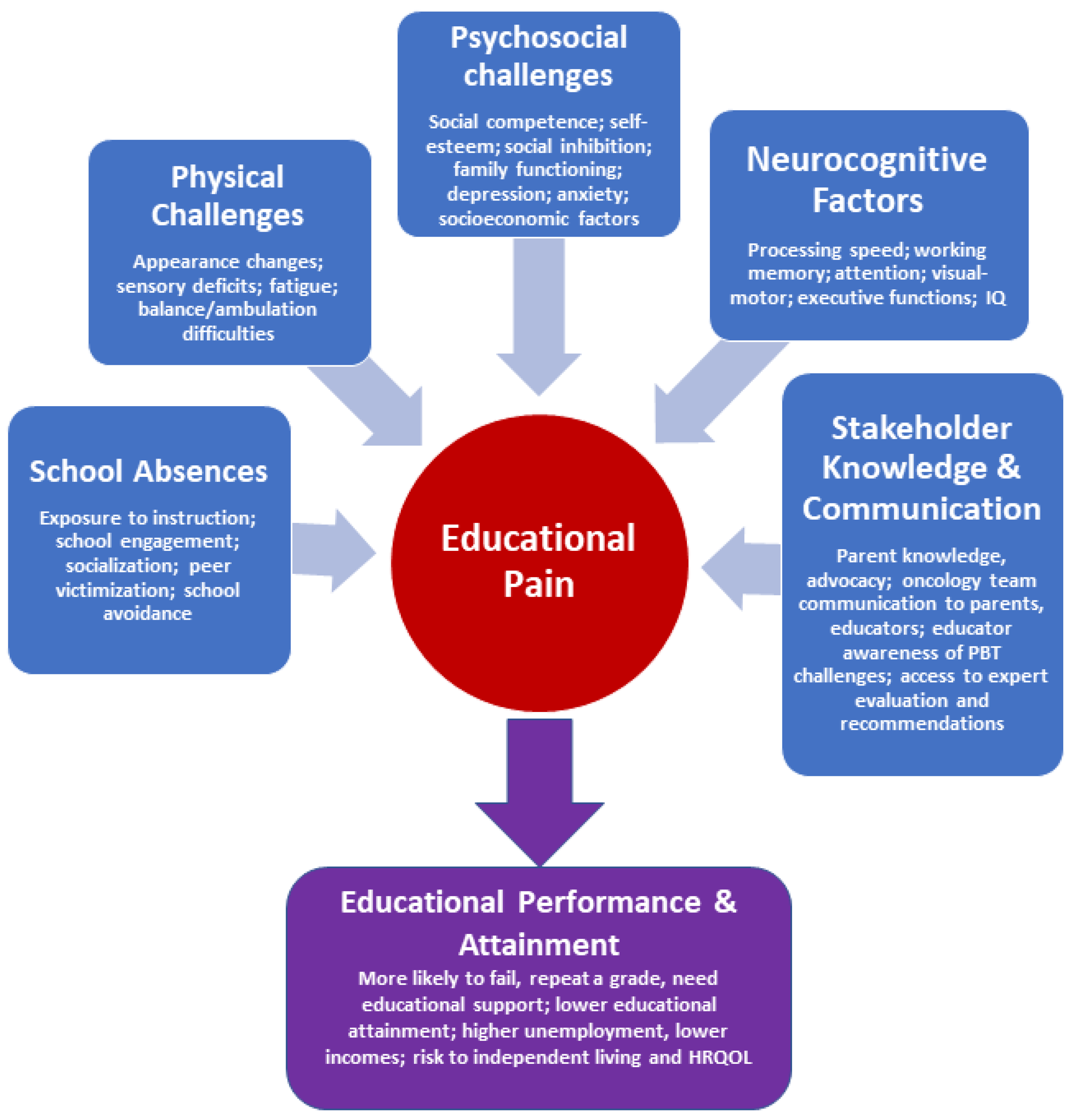
2. Educational Pain Points for Pediatric Brain Tumor Survivors
2.1. Neurocognitive Variables
2.2. School Absences and Limited School Engagement
2.3. Psychosocial Challenges
2.4. Stakeholder Knowledge and Communication
2.5. Physical Challenges
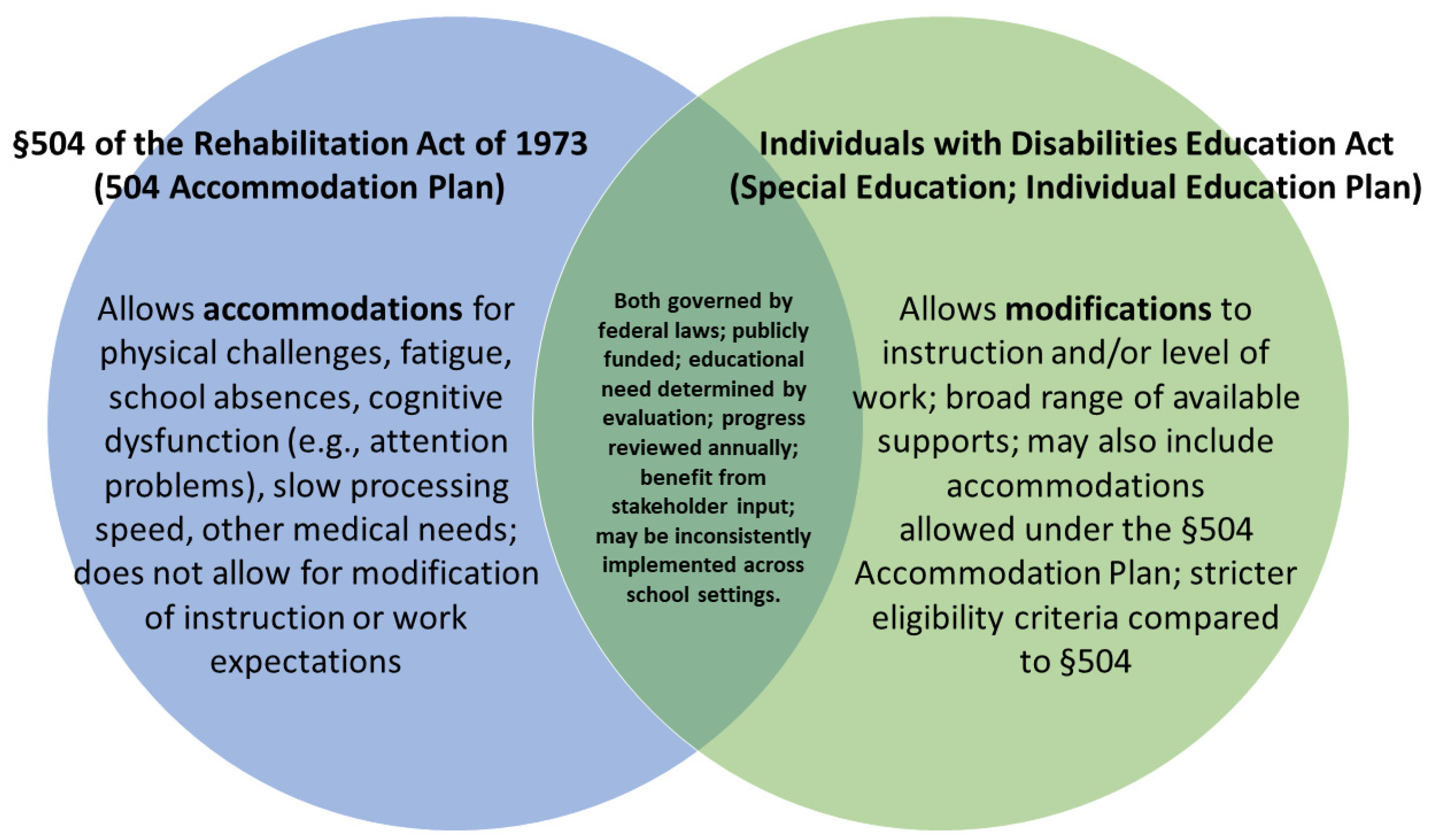
3. Educational Pain Management for Pediatric Brain Tumor Survivors
3.1. Targeted Intervention
3.2. Hospital-School Liaison and Reentry Programs and Professionals
4. Opportunities for Future Research
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, D.A.; Richardson, L.C.; Henley, S.J.; Wilson, R.J.; Dowling, N.F.; Weir, H.K.; Tai, E.W.; Buchanan Lunsford, N. Pediatric cancer mortality and survival in the United States, 2001–2016. Cancer 2020, 126, 4379–4389. [Google Scholar] [CrossRef]
- Stavinoha, P.L.; Askins, M.A.; Powell, S.K.; Pillay Smiley, N.; Robert, R.S. Neurocognitive and Psychosocial Outcomes in Pediatric Brain Tumor Survivors. Bioengineering 2018, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Schulte, F.; Russell, K.B.; Cullen, P.; Embry, L.; Fay-McClymont, T.; Johnston, D.; Rosenberg, A.R.; Sung, L. Systematic review and meta-analysis of health-related quality of life in pediatric CNS tumor survivors. Pediatr. Blood Cancer 2017, 64, e26442. [Google Scholar] [CrossRef]
- Vinchon, M.; Baroncini, M.; Leblond, P.; Delestret, I. Morbidity and tumor-related mortality among adult survivors of pediatric brain tumors: A review. Childs Nerv. Syst. 2011, 27, 697–704. [Google Scholar] [CrossRef]
- Barrera, M.; Atenafu, E.G.; Schulte, F.; Bartels, U.; Sung, L.; Janzen, L.; Chung, J.; Cataudella, D.; Hancock, K.; Saleh, A.; et al. Determinants of quality of life outcomes for survivors of pediatric brain tumors. Pediatr. Blood Cancer 2017, 64, e26481. [Google Scholar] [CrossRef]
- Lonnerblad, M.; Van’t Hooft, I.; Blomgren, K.; Berglund, E. A nationwide, population-based study of school grades, delayed graduation, and qualification for school years 10–12, in children with brain tumors in Sweden. Pediatr. Blood Cancer 2020, 67, e28014. [Google Scholar] [CrossRef] [Green Version]
- Bonneau, J.; Lebreton, J.; Taque, S.; Chappe, C. School performance of childhood cancer survivors: Mind the teenagers! J. Pediatr. 2011, 158, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L.A.; Pare-Blagoev, E.J.; Ruble, K. Barriers to Schooling in Survivorship: The Role of Neuropsychological Assessment. JCO Oncol. Pract. 2020, 16, e1516–e1523. [Google Scholar] [CrossRef] [PubMed]
- Lorenzi, M.; McMillan, A.J.; Siegel, L.S.; Zumbo, B.D.; Glickman, V.; Spinelli, J.J.; Goddard, K.J.; Pritchard, S.L.; Rogers, P.C.; McBride, M.L. Educational outcomes among survivors of childhood cancer in British Columbia, Canada: Report of the Childhood/Adolescent/Young adult cancer survivors (CAYACS) program. Cancer 2009, 115, 2234–2245. [Google Scholar] [CrossRef] [PubMed]
- Lönnerblad, M.; Lovio, R.; Berglund, E.; van’t Hooft, I. Affected aspects regarding literacy and numeracy in children treated for brain tumors. J. Pediatr. Oncol. Nurs. 2017, 34, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Maddrey, A.M.; Bergeron, J.A.; Lombardo, E.R.; McDonald, N.K.; Mulne, A.F.; Barenberg, P.D.; Bowers, D.C. Neuropsychological performance and quality of life of 10 year survivors of childhood medulloblastoma. J. Neurooncol. 2005, 72, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.M.; Robins, T.; Gannoni, A.F.; Tapp, H. Survivors of childhood cancer in South Australia attending a late-effects clinic: A descriptive report of psychological, cognitive, and academic late-effects. J. Psychosoc. Oncol. 2014, 32, 152–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saatci, D.; Thomas, A.; Botting, B.; Sutcliffe, A.G. Educational attainment in childhood cancer survivors: A meta-analysis. Arch. Dis. Child 2020, 105, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Ellenberg, L.; Liu, Q.; Gioia, G.; Yasui, Y.; Packer, R.J.; Mertens, A.; Donaldson, S.S.; Stovall, M.; Kadan-Lottick, N.; Armstrong, G.; et al. Neurocognitive status in long-term survivors of childhood CNS malignancies: A report from the Childhood Cancer Survivor Study. Neuropsychology 2009, 23, 705–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, J.W.Y.; Friedman, D.L.; Whitton, J.A.; Stovall, M.; Mertens, A.C.; Robison, L.L.; Weiss, N.S. Employment status among adult survivors in the childhood cancer survivor study. Pediatr. Blood Cancer 2008, 50, 104–110. [Google Scholar] [CrossRef]
- Torres, V.A.; Ashford, J.M.; Wright, E.; Xu, J.; Zhang, H.; Merchant, T.E.; Conklin, H.M. The impact of socioeconomic status (SES) on cognitive outcomes following radiotherapy for pediatric brain tumors: A prospective, longitudinal trial. Neuro-Oncology 2021, 23, 1173–1182. [Google Scholar] [CrossRef]
- Oyefiade, A.; Paltin, I.; De Luca, C.R.; Hardy, K.K.; Grosshans, D.R.; Chintagumpala, M.; Mabbott, D.J.; Kahalley, L.S. Cognitive Risk in Survivors of Pediatric Brain Tumors. J. Clin. Oncol. 2021, 39, 1718–1726. [Google Scholar] [CrossRef]
- Olsson, I.T.; Perrin, S.; Lundgren, J.; Hjorth, L.; Johanson, A. Long-Term Cognitive Sequelae After Pediatric Brain Tumor Related to Medical Risk Factors, Age, and Sex. Pediatr. Neurol. 2014, 51, 515–521. [Google Scholar] [CrossRef]
- Patel, S.K.; Mullins, W.A.; O’Neil, S.H.; Wilson, K. Neuropsychological differences between survivors of supratentorial and infratentorial brain tumours. J. Intellect. Disabil. Res. 2011, 55, 30–40. [Google Scholar] [CrossRef]
- Hardy, K.K.; Bonner, M.J.; Willard, V.W.; Watral, M.A.; Gururangan, S. Hydrocephalus as a possible additional contributor to cognitive outcome in survivors of pediatric medulloblastoma. Psycho-Oncology 2008, 17, 1157–1161. [Google Scholar] [CrossRef]
- Mahajan, A.; Stavinoha, P.L.; Rongthong, W.; Brodin, N.P.; McGovern, S.L.; El Naqa, I.; Palmer, J.D.; Vennarini, S.; Indelicato, D.J.; Aridgides, P.; et al. Neurocognitive Effects and Necrosis in Childhood Cancer Survivors Treated With Radiation Therapy: A PENTEC Comprehensive Review. Int. J. Radiat. Oncol. Biol. Phys. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, S.; Bode, U.; Deinlein, F.; Ottensmeier, H.; Warmuth-Metz, M.; Soerensen, N.; Graf, N.; Emser, A.; Pietsch, T.; Wolff, J.E.; et al. Treatment of early childhood medulloblastoma by postoperative chemotherapy alone. N. Engl. J. Med. 2005, 352, 978–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neil, S.H.; Whitaker, A.M.; Kayser, K.; Nelson, M.B.; Finlay, J.L.; Dhall, G.; Sands, S. Neuropsychological outcomes on Head Start III: A prospective, multi-institutional clinical trial for young children diagnosed with malignant brain tumors. Neuro-Oncol. Pract. 2020, 7, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Warrier, R.; Chauhan, A.; Davluri, M.; Tedesco, S.L.; Nadell, J.; Craver, R. Cisplatin and cranial irradiation-related hearing loss in children. Ochsner. J. 2012, 12, 191–196. [Google Scholar]
- Heitzer, A.M.; Raghubar, K.; Ris, M.D.; Minard, C.G.; Gragert, M.N.; Stancel, H.H.; Orobio, J.; Xue, J.; Whitehead, W.; Okcu, M.F.; et al. Neuropsychological functioning following surgery for pediatric low-grade glioma: A prospective longitudinal study. J. Neurosurg. Pediatr. 2019, 25, 251–259. [Google Scholar] [CrossRef]
- Ris, M.D.; Beebe, D.W.; Armstrong, F.D.; Fontanesi, J.; Holmes, E.; Sanford, R.A.; Wisoff, J.H.; Children’s Oncology, G. Cognitive and adaptive outcome in extracerebellar low-grade brain tumors in children: A report from the Children’s Oncology Group. J. Clin. Oncol. 2008, 26, 4765–4770. [Google Scholar] [CrossRef] [Green Version]
- Lanier, J.C.; Abrams, A.N. Posterior fossa syndrome: Review of the behavioral and emotional aspects in pediatric cancer patients. Cancer 2017, 123, 551–559. [Google Scholar] [CrossRef]
- Schreiber, J.E.; Palmer, S.L.; Conklin, H.M.; Mabbott, D.J.; Swain, M.A.; Bonner, M.J.; Chapieski, M.L.; Huang, L.; Zhang, H.; Gajjar, A. Posterior fossa syndrome and long-term neuropsychological outcomes among children treated for medulloblastoma on a multi-institutional, prospective study. Neuro-Oncol. 2017, 19, 1673–1682. [Google Scholar] [CrossRef]
- Jalali, R.; Mallick, I.; Dutta, D.; Goswami, S.; Gupta, T.; Munshi, A.; Deshpande, D.; Sarin, R. Factors influencing neurocognitive outcomes in young patients with benign and low-grade brain tumors treated with stereotactic conformal radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 974–979. [Google Scholar] [CrossRef]
- Merchant, T.E.; Conklin, H.M.; Wu, S.; Lustig, R.H.; Xiong, X. Late effects of conformal radiation therapy for pediatric patients with low-grade glioma: Prospective evaluation of cognitive, endocrine, and hearing deficits. J. Clin. Oncol. 2009, 27, 3691–3697. [Google Scholar] [CrossRef] [Green Version]
- Kahalley, L.S.; Winter-Greenberg, A.; Stancel, H.; Ris, M.D.; Gragert, M. Utility of the General Ability Index (GAI) and Cognitive Proficiency Index (CPI) with survivors of pediatric brain tumors: Comparison to Full Scale IQ and premorbid IQ estimates. J. Clin. Exp. Neuropsychol. 2016, 38, 1065–1076. [Google Scholar] [CrossRef] [Green Version]
- Palmer, S.L.; Armstrong, C.; Onar-Thomas, A.; Wu, S.; Wallace, D.; Bonner, M.J.; Schreiber, J.; Swain, M.; Chapieski, L.; Mabbott, D.; et al. Processing speed, attention, and working memory after treatment for medulloblastoma: An international, prospective, and longitudinal study. J. Clin. Oncol. 2013, 31, 3494–3500. [Google Scholar] [CrossRef] [Green Version]
- Chevignard, M.; Camara-Costa, H.; Doz, F.; Dellatolas, G. Core deficits and quality of survival after childhood medulloblastoma: A review. Neuro-Oncol. Pract. 2017, 4, 82–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, K.E.; Kuttesch, J.F.; Champion, J.E.; Andreotti, C.F.; Hipp, D.W.; Bettis, A.; Barnwell, A.; Compas, B.E. A quantitative meta-analysis of neurocognitive sequelae in survivors of pediatric brain tumors. Pediatr. Blood Cancer 2010, 55, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Conklin, H.M.; Ashford, J.M.; Howarth, R.A.; Merchant, T.E.; Ogg, R.J.; Santana, V.M.; Reddick, W.E.; Wu, S.J.; Xiong, X.P. Working Memory Performance among Childhood Brain Tumor Survivors. J. Int. Neuropsychol. Soc. 2012, 18, 996–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpentieri, S.C.; Meyer, E.A.; Delaney, B.L.; Victoria, M.L.; Gannon, B.K.; Doyle, J.M.; Kieran, M.W. Psychosocial and behavioral functioning among pediatric brain tumor survivors. J. Neuro-Oncol. 2003, 63, 279–287. [Google Scholar] [CrossRef]
- Robinson, K.E.; Pearson, M.M.; Cannistraci, C.J.; Anderson, A.W.; Kuttesch, J.F.; Wymer, K.; Smith, S.E.; Compas, B.E. Neuroimaging of executive function in survivors of pediatric brain tumors and healthy controls. Neuropsychology 2014, 28, 791–800. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, K.R.; Walsh, K.S.; Reynolds, N.C.; Mitchell, F.; Reddy, A.T.; Paltin, I.; Madan-Swain, A. Executive functions and social skills in survivors of pediatric brain tumor. Child Neuropsychol. 2013, 19, 370–384. [Google Scholar] [CrossRef] [Green Version]
- Winter, A.L.; Conklin, H.M.; Tyc, V.L.; Stancel, H.; Hinds, P.S.; Hudson, M.M.; Kahalley, L.S. Executive function late effects in survivors of pediatric brain tumors and acute lymphoblastic leukemia. J. Clin. Exp. Neuropsychol. 2014, 36, 818–830. [Google Scholar] [CrossRef]
- Wochos, G.C.; Semerjian, C.H.; Walsh, K.S. Differences in parent and teacher rating of everyday executive function in pediatric brain tumor survivors. Clin. Neuropsychol. 2014, 28, 1243–1257. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.A.; Hughes, C.W.; Stavinoha, P.L. School Competence and Fluent Academic Performance: Informing Assessment of Educational Outcomes in Survivors of Pediatric Medulloblastoma. Appl. Neuropsychol. Child. 2015, 4, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Mabbott, D.J.; Spiegler, B.J.; Greenberg, M.L.; Rutka, J.T.; Hyder, D.J.; Bouffet, E. Serial evaluation of academic and behavioral outcome after treatment with cranial radiation in childhood. J. Clin. Oncol. 2005, 23, 2256–2263. [Google Scholar] [CrossRef] [PubMed]
- Ris, M.D.; Walsh, K.; Wallace, D.; Armstrong, F.D.; Holmes, E.; Gajjar, A.; Zhou, T.; Packer, R.J. Intellectual and academic outcome following two chemotherapy regimens and radiotherapy for average-risk medulloblastoma: COG A9961. Pediatr. Blood Cancer 2013, 60, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, M.; Klerman, L.V.; Lamb, G.; Menary, J.; Alpert, J.J. School absence: A problem for the pediatrician. Pediatrics 1982, 69, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, L.K.; Kato, P.M. Psychosocial support for patients in pediatric oncology: The influences of parents, schools, peers, and technology. J. Pediatr. Oncol. Nurs. 2003, 20, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Katz, E.R.; Rubinstein, C.L.; Hubert, N.C.; Blew, A. School and social reintegration of children with cancer. J. Psychosoc. Oncol. 1988, 6, 123–140. [Google Scholar] [CrossRef]
- French, A.E.; Tsangaris, E.; Barrera, M.; Guger, S.; Brown, R.; Urbach, S.; Stephens, D.; Nathan, P.C. School attendance in childhood cancer survivors and their siblings. J. Pediatr. 2013, 162, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Park, H.J.; Lee, J.M.; Ju, H.Y.; Park, B.K.; Yu, E.S.; Yang, H.K.; Kim, J.Y.; Park, S.K.; Lee, Y.H.; et al. School performance of childhood cancer survivors in Korea: A multi-institutional study on behalf of the Korean Society of Pediatric Hematology and Oncology. Psychooncology 2018, 27, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Fredricks, J.A.; Blumenfeld, P.; Friedel, J.; Paris, A. School engagement. In What do Children Need to Flourish; Springer: Berlin/Heidelberg, Germany, 2005; pp. 305–321. [Google Scholar]
- Hocking, M.C.; Paltin, I.; Belasco, C.; Barakat, L.P. Parent perspectives on the educational barriers and unmet needs of children with cancer. Child Health Care 2018, 47, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, M.C.; Sari, H.Y.; Cetingul, N.; Kantar, M.; Erermis, S.; Aksoylar, S. Determination of school-related problems in children treated for cancer. J. Sch. Nurs. 2014, 30, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Abbott-Chapman, J.; Martin, K.; Ollington, N.; Venn, A.; Dwyer, T.; Gall, S. The longitudinal association of childhood school engagement with adult educational and occupational achievement: Findings from an Australian national study. Br. Educ. Res. J. 2014, 40, 102–120. [Google Scholar] [CrossRef]
- Bruce, B.S.; Chapman, A.; MacDonald, A.; Newcombe, J. School experiences of families of children with brain tumors. J. Pediatr. Oncol. Nurs. 2008, 25, 331–339. [Google Scholar] [CrossRef]
- Shiu, S. Issues in the education of students with chronic illness. Int. J. Disabil. Dev. Educ. 2001, 48, 269–281. [Google Scholar] [CrossRef]
- Maynard, B.R.; Heyne, D.; Brendel, K.E.; Bulanda, J.J.; Thompson, A.M.; Pigott, T.D. Treatment for School Refusal Among Children and Adolescents: A Systematic Review and Meta-Analysis. Res. Soc. Work. Pract. 2018, 28, 56–67. [Google Scholar] [CrossRef] [Green Version]
- Gurney, J.G.; Krull, K.R.; Kadan-Lottick, N.; Nicholson, H.S.; Nathan, P.C.; Zebrack, B.; Tersak, J.M.; Ness, K.K. Social outcomes in the Childhood Cancer Survivor Study cohort. J. Clin. Oncol. 2009, 27, 2390–2395. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.B.; Kaffenberger, C.; Goldberg, P.; Kyeung Mi, O.; Hudspeth, R. School reentry for children with cancer: Perceptions of nurses, school personnel, and parents. J. Pediatr. Oncol. Nurs. 2009, 26, 86–99. [Google Scholar] [CrossRef]
- Wakefield, C.E.; McLoone, J.; Goodenough, B.; Lenthen, K.; Cairns, D.R.; Cohn, R.J. The Psychosocial Impact of Completing Childhood Cancer Treatment: A Systematic Review of the Literature. J. Pediatric Psychol. 2009, 35, 262–274. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.S.; Dellarole, A.; Peterson, E.C.; Bregy, A.; Komotar, R.; Harvey, P.D.; Elhammady, M.S. Long-term psychiatric outcomes in pediatric brain tumor survivors. Childs Nerv. Syst. 2015, 31, 653–663. [Google Scholar] [CrossRef]
- Salley, C.G.; Hewitt, L.L.; Patenaude, A.F.; Vasey, M.W.; Yeates, K.O.; Gerhardt, C.A.; Vannatta, K. Temperament and social behavior in pediatric brain tumor survivors and comparison peers. J. Pediatr. Psychol. 2015, 40, 297–308. [Google Scholar] [CrossRef] [Green Version]
- Emond, A.; Edwards, L.; Peacock, S.; Norman, C.; Evangeli, M. Social competence in children and young people treated for a brain tumour. Support Care Cancer 2016, 24, 4587–4595. [Google Scholar] [CrossRef]
- Boydell, K.M.; Stasiulis, E.; Greenberg, M.; Greenberg, C.; Spiegler, B. I’ll show them: The social construction of (in)competence in survivors of childhood brain tumors. J. Pediatr. Oncol. Nurs. 2008, 25, 164–174. [Google Scholar] [CrossRef]
- Upton, P.; Eiser, C. School experiences after treatment for a brain tumour. Child Care Health Dev. 2006, 32, 9–17. [Google Scholar] [CrossRef]
- Vanclooster, S.; Bilsen, J.; Peremans, L.; Van der Werff Ten Bosch, J.; Laureys, G.; Willems, E.; Genin, S.; Van Bogaert, P.; Paquier, P.; Jansen, A. Attending school after treatment for a brain tumor: Experiences of children and key figures. J. Health Psychol. 2019, 24, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Quast, L.F.; Phillips, P.C.; Li, Y.; Kazak, A.E.; Barakat, L.P.; Hocking, M.C. A prospective study of family predictors of health-related quality of life in pediatric brain tumor survivors. Pediatr. Blood Cancer 2018, 65, e26976. [Google Scholar] [CrossRef]
- Ach, E.; Gerhardt, C.A.; Barrera, M.; Kupst, M.J.; Meyer, E.A.; Patenaude, A.F.; Vannatta, K. Family factors associated with academic achievement deficits in pediatric brain tumor survivors. Psychooncology 2013, 22, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson-Green, B.; Morris, R.D.; Krawiecki, N. Family and illness predictors of outcome in pediatric brain tumors. J. Pediatr. Psychol. 1995, 20, 769–784. [Google Scholar] [CrossRef] [PubMed]
- Van Schoors, M.; Caes, L.; Knoble, N.B.; Goubert, L.; Verhofstadt, L.L.; Alderfer, M.A. Systematic review: Associations between family functioning and child adjustment after pediatric cancer diagnosis: A meta-analysis. J. Pediatr. Psychol. 2017, 42, 6–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hocking, M.C.; Hobbie, W.L.; Deatrick, J.A.; Hardie, T.L.; Barakat, L.P. Family Functioning Mediates the Association Between Neurocognitive Functioning and Health-Related Quality of Life in Young Adult Survivors of Childhood Brain Tumors. J. Adolesc. Young Adult Oncol. 2015, 4, 18–25. [Google Scholar] [CrossRef]
- Ruble, K.; Pare-Blagoev, J.; Cooper, S.; Martin, A.; Jacobson, L.A. Parent perspectives on oncology team communication regarding neurocognitive impacts of cancer therapy and school reentry. Pediatr. Blood Cancer 2019, 66, e27427. [Google Scholar] [CrossRef]
- Ruble, K.; Pare-Blagoev, J.; Cooper, S.; Jacobson, L.A. Pediatric oncology provider perspectives and practices: Supporting patients and families in schooling after cancer diagnosis. Pediatr. Blood Cancer 2020, 67, e28166. [Google Scholar] [CrossRef] [PubMed]
- Greenzang, K.A.; Cronin, A.M.; Kang, T.; Mack, J.W. Parent understanding of the risk of future limitations secondary to pediatric cancer treatment. Pediatr. Blood Cancer 2018, 65, e27020. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.L.; Christiansen, H.L.; Elam, M.; Hoag, J.; Irwin, M.K.; Pao, M.; Voll, M.; Noll, R.B.; Kelly, K.P. Academic Continuity and School Reentry Support as a Standard of Care in Pediatric Oncology. Pediatr. Blood Cancer 2015, 62, S805–S817. [Google Scholar] [CrossRef] [Green Version]
- Nabors, L.A.; Little, S.G.; Akin-Little, A.; Iobst, E.A. Teacher knowledge of and confidence in meeting the needs of children with chronic medical conditions: Pediatric psychology’s contribution to education. Psychol. Sch. 2008, 45, 217–226. [Google Scholar] [CrossRef]
- Tresman, R.; Brown, M.; Fraser, F.; Skinner, R.; Bailey, S. A School Passport as Part of a Protocol to Assist Educational Reintegration After Medulloblastoma Treatment in Childhood. Pediatr. Blood Cancer 2016, 63, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Hocking, M.C.; Walsh, K.S.; Hardy, K.K.; Conklin, H.M. Addressing Neurocognitive Late Effects in Pediatric Cancer Survivors: Current Approaches and Future Opportunities. J. Clin. Oncol. 2021, 39, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Summers, K. An evaluation of the educational support for teachers who teach children with life-limiting illness in schools. Pastor. Care Educ. 2012, 30, 191–207. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, M.C.; Mulrooney, D.A.; Steinberger, J.; Lee, J.; Baker, K.S.; Ness, K.K. Deficits in Physical Function Among Young Childhood Cancer Survivors. J. Clin. Oncol. 2013, 31, 2799–2805. [Google Scholar] [CrossRef] [Green Version]
- Lassaletta, A.; Bouffet, E.; Mabbott, D.; Kulkarni, A.V. Functional and neuropsychological late outcomes in posterior fossa tumors in children. Childs Nerv. Syst. 2015, 31, 1877–1890. [Google Scholar] [CrossRef]
- Roddy, E.; Mueller, S. Late Effects of Treatment of Pediatric Central Nervous System Tumors. J. Child Neurol. 2016, 31, 237–254. [Google Scholar] [CrossRef]
- Goldenberg-Cohen, N.; Ehrenberg, M.; Toledano, H.; Kornreich, L.; Snir, M.; Cohen, I.J.; Michowiz, S. Preoperative visual loss is the main cause of irreversible poor vision in children with a brain tumor. Front. Neurol. 2011, 2, 62. [Google Scholar] [CrossRef] [Green Version]
- Hornquist, L.; Rickardsson, J.; Lannering, B.; Gustafsson, G.; Boman, K.K. Altered self-perception in adult survivors treated for a CNS tumor in childhood or adolescence: Population-based outcomes compared with the general population. Neuro-Oncology 2015, 17, 733–740. [Google Scholar] [CrossRef]
- Krull, K.R.; Hardy, K.K.; Kahalley, L.S.; Schuitema, I.; Kesler, S.R. Neurocognitive outcomes and interventions in long-term survivors of childhood cancer. J. Clin. Oncol. 2018, 36, 2181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conklin, H.M.; Ogg, R.J.; Ashford, J.M.; Scoggins, M.A.; Zou, P.; Clark, K.N.; Martin-Elbahesh, K.; Hardy, K.K.; Merchant, T.E.; Jeha, S.; et al. Computerized Cognitive Training for Amelioration of Cognitive Late Effects Among Childhood Cancer Survivors: A Randomized Controlled Trial. J. Clin. Oncol. 2015, 33, 3894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kesler, S.R.; Lacayo, N.J.; Jo, B. A pilot study of an online cognitive rehabilitation program for executive function skills in children with cancer-related brain injury. Brain Inj. 2011, 25, 101–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, K.K.; Willard, V.W.; Bonner, M.J. Computerized cognitive training in survivors of childhood cancer: A pilot study. J. Pediatr. Oncol. Nurs. 2011, 28, 27–33. [Google Scholar] [CrossRef]
- Cox, L.E.; Ashford, J.M.; Clark, K.N.; Martin-Elbahesh, K.; Hardy, K.K.; Merchant, T.E.; Ogg, R.J.; Jeha, S.; Willard, V.W.; Huang, L.; et al. Feasibility and acceptability of a remotely administered computerized intervention to address cognitive late effects among childhood cancer survivors. Neuro-Oncol. Pract. 2015, 2, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Carlson-Green, B.; Puig, J.; Bendel, A. Feasibility and efficacy of an extended trial of home-based working memory training for pediatric brain tumor survivors: A pilot study. Neuro-Oncol. Pract. 2017, 4, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.L.; Leigh, L.; Ellison, S.C.; Onar-Thomas, A.; Wu, S.J.; Qaddoumi, I.; Armstrong, G.T.; Wright, K.; Wetmore, C.; Broniscer, A.; et al. Feasibility and Efficacy of a Computer-Based Intervention Aimed at Preventing Reading Decoding Deficits Among Children Undergoing Active Treatment for Medulloblastoma: Results of a Randomized Trial. J. Pediatr. Psychol. 2014, 39, 450–458. [Google Scholar] [CrossRef] [Green Version]
- Butler, R.W.; Copeland, D.R. Attentional processes and their remediation in children treated for cancer: A literature review and the development of a therapeutic approach. J. Int. Neuropsychol. Soc. 2002, 8, 115–124. [Google Scholar] [CrossRef]
- Butler, R.W.; Copeland, D.R.; Fairclough, D.L.; Mulhern, R.K.; Katz, E.R.; Kazak, A.E.; Noll, R.B.; Patel, S.K.; Sahler, O.J. A multicenter, randomized clinical trial of a cognitive remediation program for childhood survivors of a pediatric malignancy. J. Consult. Clin. Psychol. 2008, 76, 367–378. [Google Scholar] [CrossRef]
- Patel, S.K.; Ross, P.; Cuevas, M.; Turk, A.; Kim, H.; Lo, T.T.; Wong, L.F.; Bhatia, S. Parent-directed intervention for children with cancer-related neurobehavioral late effects: A randomized pilot study. J. Pediatr. Psychol. 2014, 39, 1013–1027. [Google Scholar] [CrossRef]
- Holland, A.A.; Hughes, C.W.; Harder, L.; Silver, C.; Bowers, D.C.; Stavinoha, P.L. Effect of motivation on academic fluency performance in survivors of pediatric medulloblastoma. Child Neuropsychol. 2016, 22, 570–586. [Google Scholar] [CrossRef] [PubMed]
- Barrera, M.; Atenafu, E.G.; Sung, L.; Bartels, U.; Schulte, F.; Chung, J.; Cataudella, D.; Hancock, K.; Janzen, L.; Saleh, A.; et al. A randomized control intervention trial to improve social skills and quality of life in pediatric brain tumor survivors. Psychooncology 2018, 27, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Poggi, G.; Liscio, M.; Pastore, V.; Adduci, A.; Galbiati, S.; Spreafico, F.; Gandola, L.; Massimino, M. Psychological intervention in young brain tumor survivors: The efficacy of the cognitive behavioural approach. Disabil. Rehabil. 2009, 31, 1066–1073. [Google Scholar] [CrossRef]
- Annett, R.D.; Patel, S.K.; Phipps, S. Monitoring and Assessment of Neuropsychological Outcomes as a Standard of Care in Pediatric Oncology. Pediatr. Blood Cancer 2015, 62, S460–S513. [Google Scholar] [CrossRef] [Green Version]
- Cheung, L.L.T.; Wakefield, C.E.; Ellis, S.J.; Mandalis, A.; Frow, E.; Cohn, R.J. Neuropsychology Reports for Childhood Brain Tumor Survivors: Implementation of Recommendations at Home and School. Pediatr. Blood Cancer 2014, 61, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.S.; Noll, R.B.; Annett, R.D.; Patel, S.K.; Patenaude, A.F.; Embry, L. Standard of Care for Neuropsychological Monitoring in Pediatric Neuro-Oncology: Lessons From the Children’s Oncology Group (COG). Pediatr. Blood Cancer 2016, 63, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Northman, L.; Ross, S.; Morris, M.; Tarquini, S. Supporting pediatric cancer survivors with neurocognitive late effects: A model of care. J. Pediatr. Oncol. Nurs. 2015, 32, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Bruce, B.S.; Newcombe, J.; Chapman, A. School liaison program for children with brain tumors. J. Pediatr. Oncol. Nurs. 2012, 29, 45–54. [Google Scholar] [CrossRef]
- Northman, L.; Morris, M.; Loucas, C.; Ross, S.; Muriel, A.C.; Guo, D.; London, W.B.; Manley, P.; Ullrich, N.J. The Effectiveness of a Hospital-Based School Liaison Program: A Comparative Study of Parental Perception of School Supports for Children With Pediatric Cancer and Neurofibromatosis Type 1. J. Pediatr. Oncol. Nurs. 2018, 35, 276–286. [Google Scholar] [CrossRef]
- Dubowy, R.L.; Rieger, B.P.; Songer, N.S.; Kleinmann, A.E.; Lewandowski, L.J.; Rogers, C.L.; Silber, J.M. Teaching teachers about childhood cancer—The effects of a web-based training program. J. Pediatr. Hematol. Oncol. 2006, 28, 729–733. [Google Scholar] [CrossRef] [PubMed]
- Helms, A.S.; Schmiegelow, K.; Brok, J.; Johansen, C.; Thorsteinsson, T.; Simovska, V.; Larsen, H.B. Facilitation of school re-entry and peer acceptance of children with cancer: A review and meta-analysis of intervention studies. Eur. J. Cancer Care 2016, 25, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Hay, G.H.; Nabors, M.L.; Sullivan, A.; Zygmund, A. Students with Pediatric Cancer: A Prescription for School Success. Phys. Disabil. Educ. Relat. Serv. 2015, 34, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Mitby, P.A.; Robison, L.L.; Whitton, J.A.; Zevon, M.A.; Gibbs, I.C.; Tersak, J.M.; Meadows, A.T.; Stovall, M.; Zeltzer, L.K.; Mertens, A.C. Utilization of special education services and educational attainment among long-term survivors of childhood cancer—A report from the Childhood Cancer Survivor Study. Cancer 2003, 97, 1115–1126. [Google Scholar] [CrossRef] [PubMed]
- APHOES. Practice Recommendations for Managing the Educational Needs of Pediatric Hematology and Oncology Patients; APHOES, 2015; Available online: https://www.healassociation.org/wp-content/uploads/2019/03/APHOES-Practice-Recommendations-No-Password-Book-Baby-Revised-Version2015-1.pdf (accessed on 23 October 2021).
- Lum, A.; Donnan, B.; Wakefield, C.E.; Fardell, J.E.; Marshall, G.M. Establishing Australian school re-entry service guidelines for children diagnosed with cancer. J. Paediatr. Child Health 2017, 53, 529–533. [Google Scholar] [CrossRef] [Green Version]
- Marchak, J.G.; Devine, K.A.; Hudson, M.M.; Jacobson, L.A.; Michel, G.; Peterson, S.R.; Schulte, F.; Wakefield, C.E.; Sands, S.A. Systematic review of educational supports of pediatric cancer survivors: Current approaches and future directions. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.C. Preliminary empirical model of crucial determinants of best practice for peer tutoring on academic achievement. J. Educ. Psychol. 2015, 107, 558. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Common Educational Supports for PBT Survivors |
|---|
| Academic Needs |
|
| Psychosocial Needs |
|
| Physical Needs |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stavinoha, P.L.; Trinh-Wong, T.; Rodriguez, L.N.; Stewart, C.M.; Frost, K. Educational Pain Points for Pediatric Brain Tumor Survivors: Review of Risks and Remedies. Children 2021, 8, 1125. https://doi.org/10.3390/children8121125
Stavinoha PL, Trinh-Wong T, Rodriguez LN, Stewart CM, Frost K. Educational Pain Points for Pediatric Brain Tumor Survivors: Review of Risks and Remedies. Children. 2021; 8(12):1125. https://doi.org/10.3390/children8121125
Chicago/Turabian StyleStavinoha, Peter L., Thuy Trinh-Wong, Laura N. Rodriguez, Chawncey M. Stewart, and Kris Frost. 2021. "Educational Pain Points for Pediatric Brain Tumor Survivors: Review of Risks and Remedies" Children 8, no. 12: 1125. https://doi.org/10.3390/children8121125