
Cortisol Levels in Infants with Central Coordination Disorders during Vojta Therapy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Project
2.2. Ethical Approval
2.3. Physiotherapeutic Intervention
2.4. Subjects
2.5. The Analysis of Cortisol Concentration in Saliva
2.6. Statistical Analysis
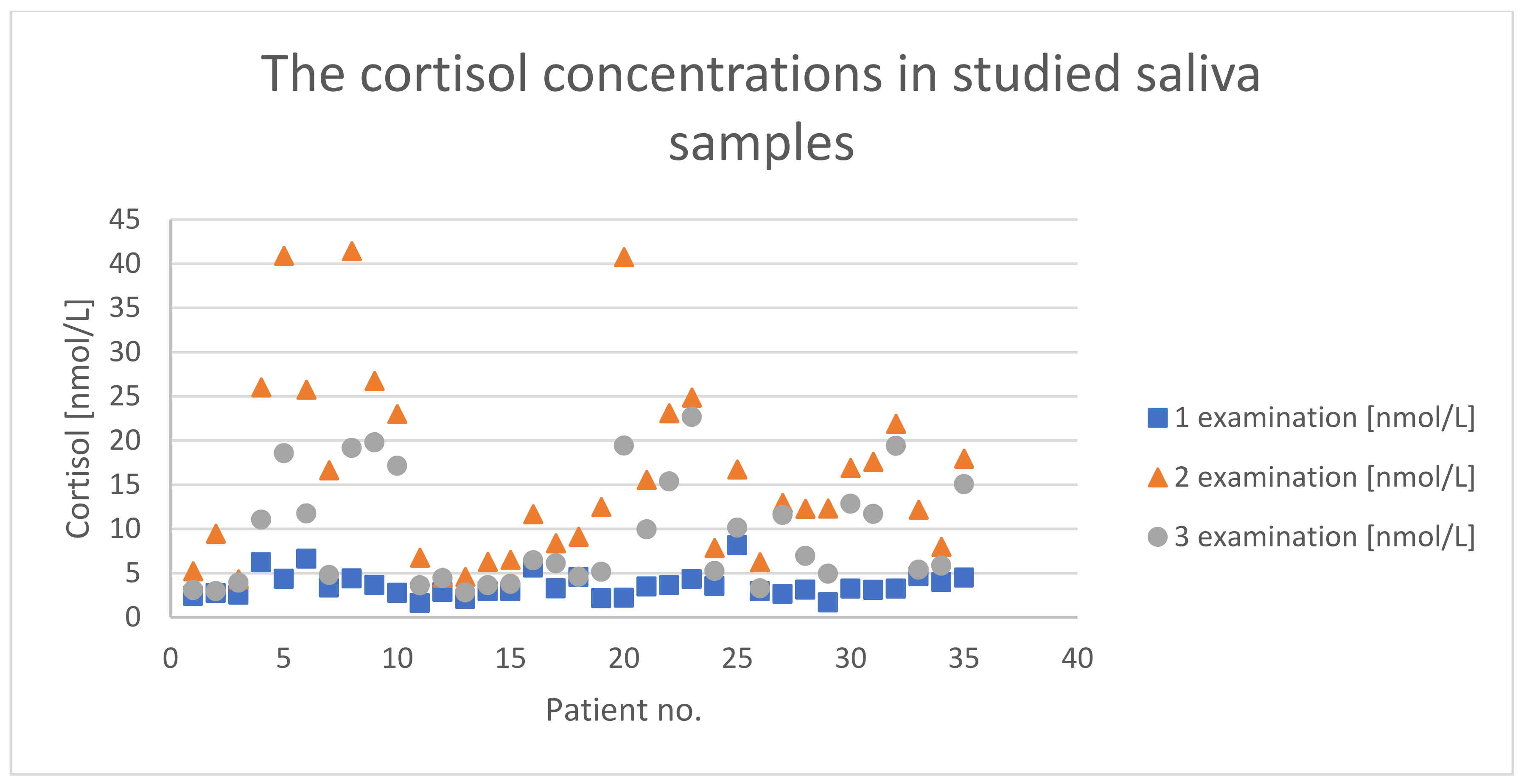
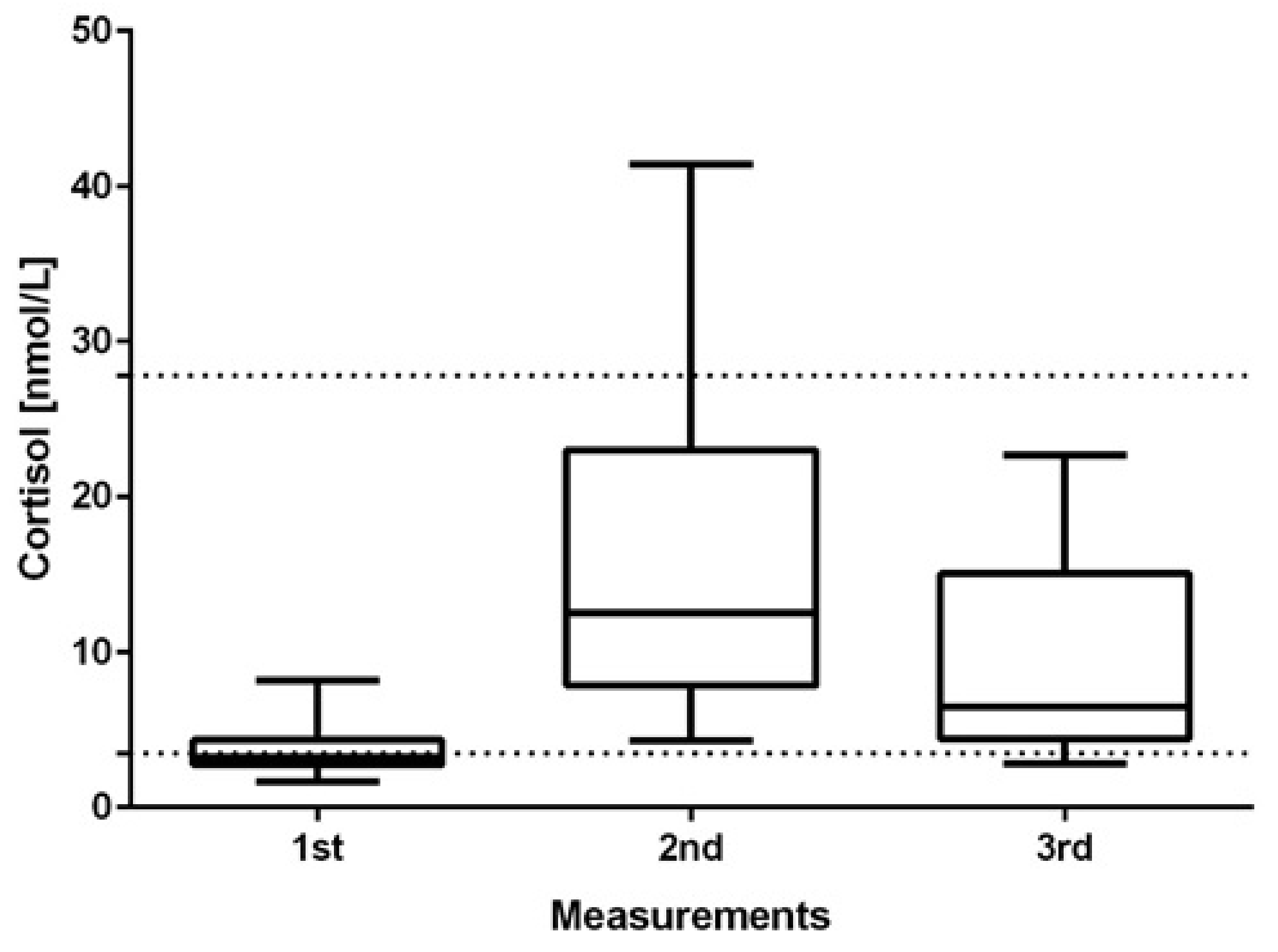
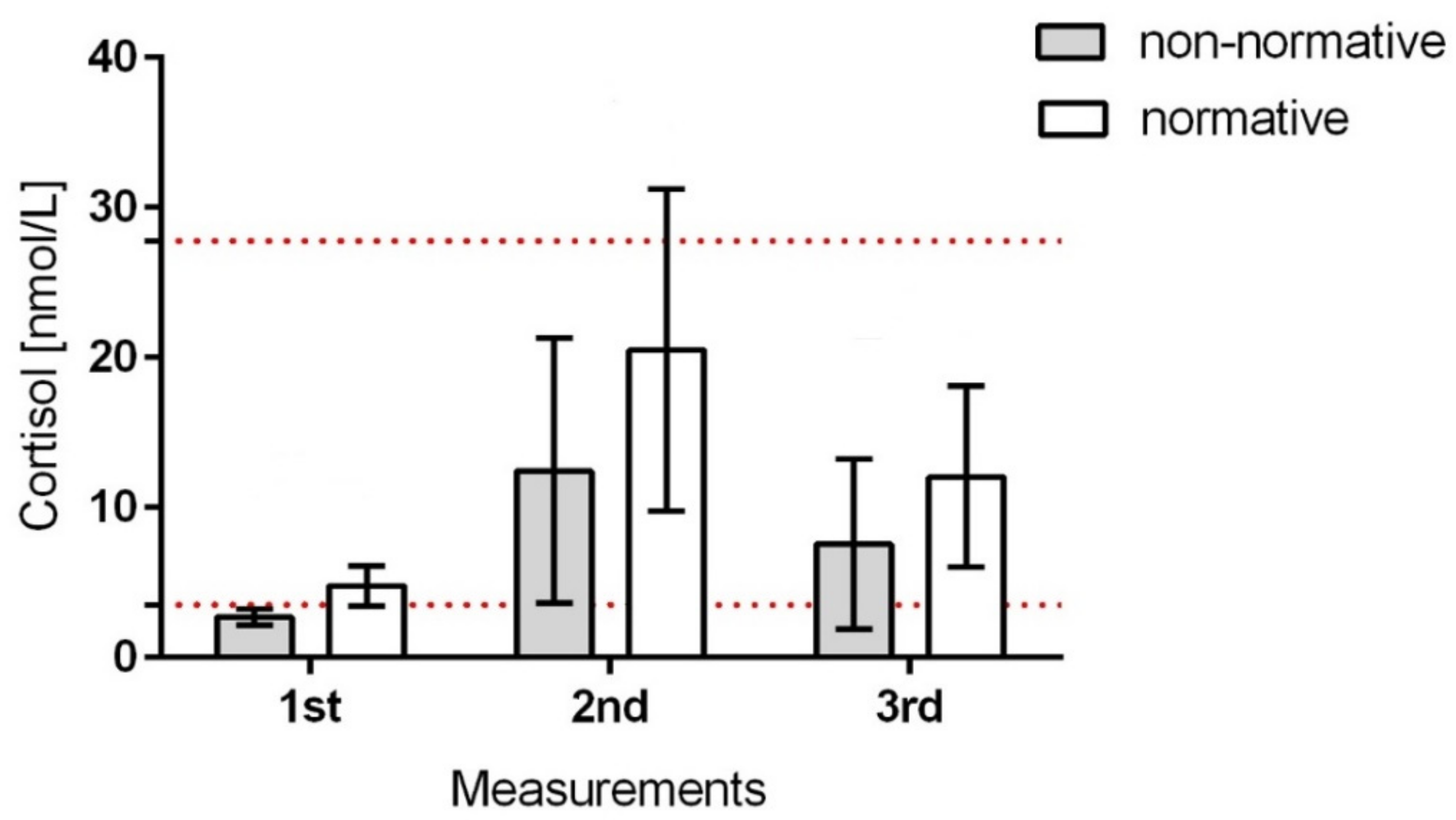
3. Results
4. Discussion
4.1. Limitations
4.2. Clinical Implications
5. Conclusions
- Vojta stimulation increased the level of free cortisol in saliva among infants with CCD, which, in 8.57% of children after therapy, exceeded normative values.
- After the Vojta intervention, the level of free cortisol in saliva decreased significantly, reaching reference values after 20 min.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blackburn, C.; Read, J.; Spencer, N. Children with Neurodevelopmental Disabilities; Annual report of the chief medical officer; Wiley: Hoboken, NJ, USA, 2012; pp. 1–13. [Google Scholar]
- Durkin, M. The epidemiology of developmental disabilities in low-income countries. Ment. Retard. Dev. Disabil. Res. Rev. 2002, 8, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Dessu, S.; Girum, T.; Geremew, M.; Zeleke, B. The burden of disease and cause of mortality in Ethiopia, 2000–2016: Findings from the Global Burden of Disease Study and Global Health Estimates. Med. Stud. Studia Med. 2020, 36, 246–256. [Google Scholar]
- Ding, S.; Lemyre, B.; Daboval, T.; Barrowman, N.; Moore, G.P. A meta-analysis of neurodevelopmental outcomes at 4–10 years in children born at 22–25 weeks gestation. Acta Paediatr. 2019, 108, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Hadders-Algra, M. General movements: A window for early identification of children at high risk for developmental disorders. J. Pediatr. 2004, 145, S8–S12. [Google Scholar] [CrossRef]
- Kiebzak, W.; Błaszczyk, B.; Szmigiel, C. Monitoring the proces of rehabilitation in children with disorders of central coordination. Pol. J. Physiother. Fizjoterapia Pol. 2003, 3, 243–249. [Google Scholar]
- Blauw-Hospers, C.; de Graaf-Peters, V.; Dirks, T.; Bos, A.; Hadders-Algra, M. Does early intervention in infants at high risk for a developmental motor disorder improve motor and cognitive development? Neurosci. Biobehav. Rev. 2007, 31, 1201–1212. [Google Scholar] [CrossRef]
- Blauw-Hospers, C.H.; Hadders-Algra, M. A systematic review of the effects of early intervention on motor development. Dev. Med. Child Neurol. 2005, 47, 421–432. [Google Scholar] [CrossRef] [Green Version]
- Spittle, A.; Orton, J.; Anderson, P.; Boyd, R.; Doyle, L.W. Early developmental intervention programmes post-hospital discharge to prevent motor and cognitive impairments in preterm infants. Cochrane Database Syst. Rev. 2012, 12, CD005495. [Google Scholar]
- Orton, J.; Spittle, A.; Doyle, L.; Anderson, P.; Boyd, R. Do early intervention programmes improve cognitive and motor outcomes for preterm infants after discharge? A systematic review. Dev. Med. Child. Neurol. 2009, 51, 851–859. [Google Scholar] [CrossRef]
- Kiebzak, W.; Kosztołowicz, M.; Zaborowska-Sapeta, K.; Kiebzak, M.; Dwornik, M. Application of T1 scale in evaluating effects of long-term therapy. Pol. Ann. Med. 2016, 23, 118–122. [Google Scholar] [CrossRef]
- Kiebzak, W.; Kowalski, I.M.; Domagalska, M.; Szopa, A.; Dwornik, M.; Kujawa, J.; Stępień, A.; Sliwiński, Z. Assessment of visual perception in adolescents with a history of central coordination disorder in early life–15-year follow-up study. Arch. Med. Sci. AMS 2012, 8, 879. [Google Scholar] [CrossRef] [Green Version]
- Vojta, V.; Peters, A. Das Vojta-Prinzip: Muskelspiele in Reflexfortbewegung und Motorischer Ontogenese; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Torrente-Rodríguez, R.M.; Tu, J.; Yang, Y.; Min, J.; Wang, M.; Song, Y.; Yu, Y.; Xu, C.; Ye, C.; IsHak, W.W.; et al. Investigation of cortisol dynamics in human sweat using a graphene-based wireless mHealth system. Matter 2020, 2, 921–937. [Google Scholar] [CrossRef]
- Veldhuis, J. Pulsatile hormone secretion: Mechanisms, significance and evaluation. In Ultradian Rhythms from Molecules to Mind; Springer: Berlin/Heidelberg, Germany, 2008; pp. 229–248. [Google Scholar]
- Faghih, R.T.; Dahleh, M.A.; Brown, E.N. An optimization formulation for characterization of pulsatile cortisol secretion. Front. Neurosci. 2015, 9, 228. [Google Scholar] [CrossRef] [Green Version]
- Casals, G.; Hanzu, F.A. Cortisol Measurements in Cushing’s Syndrome: Immunoassay or Mass Spectrometry? Ann. Lab. Med. 2020, 40, 285. [Google Scholar] [CrossRef]
- Kamin, H.S.; Kertes, D.A. Cortisol and DHEA in development and psychopathology. Horm. Behav. 2017, 89, 69–85. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Hoffman-Goetz, L. Exercise and the immune system: Regulation, integration, and adaptation. Physiol. Rev. 2000, 80, 1055–1081. [Google Scholar] [CrossRef] [Green Version]
- Hewagalamulage, S.D.; Lee, T.; Clarke, I.; Henry, B. Stress, cortisol, and obesity: A role for cortisol responsiveness in identifying individuals prone to obesity. Domest. Anim. Endocrinol. 2016, 56, S112–S120. [Google Scholar] [CrossRef]
- Szeszko, P.R.; Lehrner, A.; Yehuda, R. Glucocorticoids and hippocampal structure and function in PTSD. Harv. Rev. Psychiatry 2018, 26, 142–157. [Google Scholar] [CrossRef]
- Bae, Y.J.; Gaudl, A.; Jaeger, S.; Stadelmann, S.; Hiemisch, A.; Kiess, W.; Willenberg, A.; Schaab, M.; von Klitzing, K.; Thiery, J.; et al. Immunoassay or LC-MS/MS for the measurement of salivary cortisol in children? Clin. Chem. Lab. Med. 2016, 54, 811–822. [Google Scholar] [CrossRef]
- Tollenaar, M.S.; Jansen, J.; Beijers, R.; Riksen-Walraven, J.M.; de Weerth, C. Cortisol in the first year of life: Normative values and intra-individual variability. Early Hum. Dev. 2010, 86, 13–16. [Google Scholar] [CrossRef]
- Ivars, K.; Nelson, N.; Theodorsson, A.; Theodorsson, E.; Ström, J.O.; Mörelius, E. Development of salivary cortisol circadian rhythm and reference intervals in full-term infants. PLoS ONE 2015, 10, e0129502. [Google Scholar] [CrossRef]
- Wu, C.; Peng, X.; Li, X.; Niu, Q.; Guo, H.; Huang, H. Vojta and Bobath combined treatment for high risk infants with brain damage at early period. Neural. Regen. Res. 2007, 2, 121–125. [Google Scholar] [CrossRef]
- Buford, T.W.; Hsu, F.-C.; Brinkley, T.E.; Carter, C.S.; Church, T.S.; Dodson, J.A.; Goodpaster, B.H.; McDermott, M.M.; Nicklas, B.J.; Yank, V.; et al. Genetic influence on exercise-induced changes in physical function among mobility-limited older adults. Physiol. Genom. 2014, 46, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Lien, E.; Andersen, G.L.; Bao, Y.; Gordish-Dressman, H.; Skranes, J.S.; Vik, T.; Blackman, J.A. Apolipoprotein E polymorphisms and severity of cerebral palsy: A cross-sectional study in 255 children in N orway. Dev. Med. Child Neurol. 2013, 55, 372–377. [Google Scholar] [CrossRef] [Green Version]
- Van Eyk, C.; Corbett, M.; Maclennan, A. The emerging genetic landscape of cerebral palsy. Handb. Clin. Neurol. 2018, 147, 331–342. [Google Scholar]
- Pham, R.; Mol, B.W.; Gecz, J.; MacLennan, A.H.; MacLennan, S.C.; Corbett, M.A.; van Eyk, C.L.; Webber, D.L.; Palmer, L.J.; Berry, J.G. Definition and diagnosis of cerebral palsy in genetic studies: A systematic review. Dev. Med. Child Neurol. 2020, 62, 1024–1030. [Google Scholar] [CrossRef]
- Fleiss, B.; Gressens, P. Tertiary mechanisms of brain damage: A new hope for treatment of cerebral palsy? Lancet Neurol. 2012, 11, 556–566. [Google Scholar] [CrossRef]
- Damiano, D.L. Meaningfulness of mean group results for determining the optimal motor rehabilitation program for an individual child with cerebral palsy. Dev. Med. Child Neurol. 2014, 56, 1141–1146. [Google Scholar] [CrossRef]
- Smoczok, M.; Starszak, K.K.; Starszak, W. Paediatric care standards among wards in Poland from the perspective of staff, patients, and parents with particular emphasis on psychological care. Med. Stud. Studia Med. 2020, 36, 189–194. [Google Scholar] [CrossRef]
- Gunnar, M.R.; Talge, N.M.; Herrera, A. Stressor paradigms in developmental studies: What does and does not work to produce mean increases in salivary cortisol. Psychoneuroendocrinology 2009, 34, 953–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauli-Pott, U.; Schloß, S.; Skoluda, N.; Nater, U.M.; Becker, K. Low hair cortisol concentration predicts the development of attention deficit hyperactivity disorder. Psychoneuroendocrinology 2019, 110, 104442. [Google Scholar] [CrossRef] [PubMed]
- Baud, O.; Watterberg, K.L. Prophylactic postnatal corticosteroids: Early hydrocortisone. Semin. Fetal Neonatal Med. 2019, 24, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Zea, M.; Bellagambi, F.G.; Ben Halima, H.; Zine, N.; Jaffrezic-Renault, N.; Villa, R.; Gabriel, G.; Errachid, A. Electrochemical sensors for cortisol detections: Almost there. TrAC Trends Anal. Chem. 2020, 132, 116058. [Google Scholar] [CrossRef]
- Sezer Efe, Y.; Erdem, E.; Güneş, T. The Effect of Daily Exercise Program on Bone Mineral Density and Cortisol Level in Preterm Infants with Very Low Birth Weight: A Randomized Controlled Trial. J. Pediatr. Nurs. 2020, 51, e6–e12. [Google Scholar] [CrossRef]
- Boucher, P.; Plusquellec, P. Acute Stress Assessment From Excess Cortisol Secretion: Fundamentals and Perspectives. Front. Endocrinol. 2019, 10, 749. [Google Scholar] [CrossRef] [Green Version]
- Ponzi, D.; Flinn, M.V.; Muehlenbein, M.P.; Nepomnaschy, P.A. Hormones and human developmental plasticity. Mol. Cell. Endocrinol. 2020, 505, 110721. [Google Scholar] [CrossRef]
- Thau, L.; Gandhi, J.; Sharma, S. Physiology, Cortisol; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Federenko, I.S.; Nagamine, M.; Hellhammer, D.H.; Wadhwa, P.D.; Wüst, S. The Heritability of Hypothalamus Pituitary Adrenal Axis Responses to Psychosocial Stress Is Context Dependent. J. Clin. Endocrinol. Metab. 2004, 89, 6244–6250. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Diorio, J.; Tannenbaum, B.; Caldji, C.; Francis, D.; Freedman, A.; Sharma, S.; Pearson, D.; Plotsky, P.M.; Meaney, M.J. Maternal Care, Hippocampal Glucocorticoid Receptors, and Hypothalamic-Pituitary-Adrenal Responses to Stress. Science 1997, 277, 1659–1662. [Google Scholar] [CrossRef] [Green Version]
- Hall, F.S. Social Deprivation of Neonatal, Adolescent, and Adult Rats Has Distinct Neurochemical and Behavioral Consequences. Crit. Rev. Neurobiol. 1998, 12, 129–162. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| No guardian’s consent to participate in the study |
| Presence of disorders preventing the implementation of Vojta therapy [Vojta 2007] | |
| Up to 5 days from becoming vaccinated | |
| Feeding less than 30 min from the intervention |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiebzak, W.; Żurawski, A.; Głuszek, S.; Kosztołowicz, M.; Białek, W.A. Cortisol Levels in Infants with Central Coordination Disorders during Vojta Therapy. Children 2021, 8, 1113. https://doi.org/10.3390/children8121113
Kiebzak W, Żurawski A, Głuszek S, Kosztołowicz M, Białek WA. Cortisol Levels in Infants with Central Coordination Disorders during Vojta Therapy. Children. 2021; 8(12):1113. https://doi.org/10.3390/children8121113
Chicago/Turabian StyleKiebzak, Wojciech, Arkadiusz Żurawski, Stanisław Głuszek, Michał Kosztołowicz, and Wioletta Adamus Białek. 2021. "Cortisol Levels in Infants with Central Coordination Disorders during Vojta Therapy" Children 8, no. 12: 1113. https://doi.org/10.3390/children8121113